

Translate this page into:
Ethnical evaluation of Bangladeshi young adults in terms of morphometrically-analyzed craniofacial skeleton
This article was originally published by Wolters Kluwer and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Md. Rizvi H, Hossain M, Tanee K. Ethnical evaluation of Bangladeshi young adults in terms of morphometrically- analyzed craniofacial skeleton. APOS Trends Orthod 2013;3:15-22.
Abstract
Morphometric study for the craniofacial relations and variations in humans have long been used to differentiate various racial groups in physical anthropology. The objective of this study was to describe the morphological features of craniofacial skeleton in Bangladeshi young adults and to compare it with already reported standards for the Caucasian population as well as cephalometric values of other Indian races using Steiner’s reference norms. The study was conducted for 52 Bangladeshi young adults (27 male and 25 females), aged 21-27 years, having balanced and harmonious facial profiles, clinically acceptable occlusion with permanent dentition and no history of orthodontic treatment. Lateral cephalograms taken of these subjects were used for a series of morphometric analyses. Bangladeshi subjects were more protrusive skeletally and dentally than Caucasians. Furthermore, the mandibular plane angle was smaller in Bangladeshi subjects than in the Caucasians. Present results also suggest that the Astrics, Dravidians, and Armenoid who penetrated into Bengal in the early ages may have contributed substantially to the morphogenesis of craniofacial skeleton in the present Bengalis. The results of this study support the idea that a single standard of facial esthetics should not be applied to all racial and ethnic groups.
Keywords
Craniofacial morphology
racial group
cephalometric analysis
Steiner analysis

INTRODUCTION
Populations differ in their character, size, growth, and shape. These differences are due to a complicated interaction of genetic and environmental factors.[1] Distinctions between races by geographical location, historical origins, culture, and language were usually subsumed into three major racial groups, that is , Asiatic (or Mongoloid), Black (or Negroid), and White (or Caucasian).[2,3] Such classification into three groups provided each group with its own characteristics, which in general serve to distinguish one from others. However, morphological and anthropological findings indicate not only do each racial group have its own standards[4-7] but within the same race, each subgroup has its own standards.[8-10] It is assumed unreasonable to apply the standards of one racial group to another, or to apply the standards of one subgroup to another even in the same race.[11-13]
Cephalometric measurements may be available for reducing subjectivity in the assessment of aesthetically acceptable face, or indication for orthodontic and surgical intervention. Interventions on the jaws and facial skeleton can alter the facial appearance. With an increase in the number of Bangladeshis seeking professional treatment from orthodontists, maxillofacial surgeons or plastic and reconstructive surgeons, it has become apparent that there is an absolute need to determine what constitutes a normal or acceptable face for the Bangladeshi population. Treatment plans and clinical procedure should be determined after consideration of the racial group involved and thorough understanding of the morphological differences between races and their normal ranges.[14]
Cephalometric studies on different ethnic groups, including those of Chan’s[15] on Chinese, Garcia’s[16] on Mexican Americans, Drummond’s[5] on Negroes and Park’s[17] on Korean adults, have indicated that norms in one racial group cannot be regarded or accepted as normal for other racial groups.
The first morphometrical study for Bangladeshi subjects with use of cephalograms was done by Sajedeen et al.[18] to obtain cephalometric norms of Bangladeshi children. Meanwhile, up to present, no studies have been conducted for the adult population of Bangladesh. This study was thus designed to elucidate morphological features of Bangladeshi young adults by means of Steiner’s analysis with an aim of clinical application of the findings.
MATERIALS AND METHODS
The material for this study consisted of standardized lateral cephalograms of 27 Bangladeshi young males and 25 young females. They were selected according to the following criteria. A normal and acceptable lateral soft tissue profile, 21-27 years of age, Angle Class I molar relationship with full complement of permanent dentition up to the second molar in the proper intercuspal position. No history of orthodontic treatment, no gross dental caries or periodontal disease, and no history of facial trauma were also defined as the inclusion criteria.
The subject’s head was positioned in the Pantos 16 xp roentgenographic cephalostat maintaining an object-film distance of 15.0 cm and an X-ray object distance of 152.4 cm. The photo stimulable phosphor plate (PSP) that is enclosed in a light tight cassette was positioned parallel to the midsagittal plane of the subject such that the X-ray beam was directed perpendicular to it. The ear rods were used to stabilize the head in a vertical plane. The subject’s head was positioned so that the Frankfort horizontal plane would be parallel to the floor. Each subject was instructed to look straight and maintain a relaxed posture with teeth in centric occlusion and lips relaxed during X-ray exposure. X-ray films were exposed to an electric current of 61-85 Kvp and 4-10 mA for 1.2 s.
Lateral cephalogram was traced upon an A4 size acetate paper with a 2B hard lead pencil over a well-illuminated viewing screen. Each cephalogram was traced twice at least at 1-week interval and the average measurement taken into account to minimize the error. The midline of the double contour bilateral structures was drawn to minimize error caused by head positioning. The linear measurements were recorded with a measuring scale up to a precision of 0.5 mm. The angular measurements were analyzed with a protractor up to a precision of 0.5°. A print out of results was then prepared for each tracing that reproduced the traced points according to Steiner analysis [Figure 1]. Written informed consent was obtained from each subject prior to taking cephalogram. Ethical clearance for the study was reviewed and approved by the National Research Ethics Committee of Bangladesh Medical Research Council (Ref: BMRC/NREC/2010-2013/901 dated: 28/10/2010).
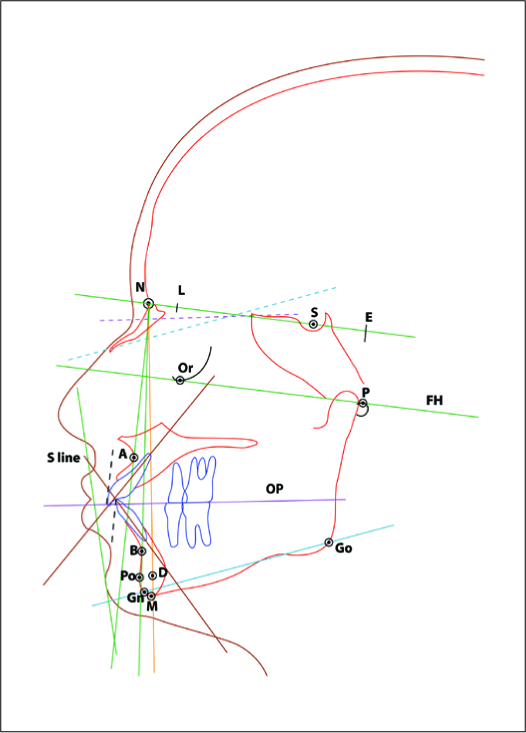
- Steiner’s analysis with the reference points identified. 1. SNA; 2. SNB; 3. ANB; 4. SND; 5.U I TO NA (MM); 6.U I TO NA (ANGLE); 7.L I TO NB (MM); 8.L I TO NB (ANGLE); 9. INTERINCISAL; 10. OP TO SN; 11. GOGN TO SN.12. SE(MM) 13. SL(MM)
A one sample t test was used to compare the Bangladeshi means with Steiner’s ideal values. This is because the Steiner values are based upon those of one individual. Steiner began with 20 ideal cases selected at the University of Illinois and used by Downs. He then considered 18 ideal and beautiful cases that had been selected at the University of Washington. Subsequently, he selected several cases from his practice that he thought met most of the qualifications he was seeking. Among these was one that he thought best met the desirable qualities of the group of patients. This single case compared favorably with the standards initially proposed by Downs. It was from this case that the measurements of the Steiner’s analysis were taken.[19,20] Similar methods of statistical comparision were used by Sharma[21] for determinig Steiner’s norms of Nepalese population ranging in age from 16 to 21 years. Steiner’s data on Caucasian samples were taken from an original article of Steiner published in 1953.[22] On the basis of these data, a complete chart of Steiner’s analysis was also depicted for Bangladeshi young adult population. For a series of statistical treatment, a statistical package “STATA” (version 8.0 International versions, StataCorp, College Station, Texas, USA) was used.
Lin’s concordance method[23] was used to calculate the intrainvestigator reproducibility. The descriptive statistics for Bangladesh sample were calculated using “STATA” (version 8.0 International versions, StataCorp). The Lin’s concordance correlation coefficients (pc) ranged (0.950-0.985) for linear measurements and (0.944-0.981) for the angular measurements indicating minimal intrainvestigator random error.
To check the normality of data and to demonstrate if these two-group data (male and female Bangladeshis) show normal distribution or not, “STATA” (version 8.0 International versions, StataCorp) software was used. It was found that the histograms of the data used in the study tend to be around a central value with no bias to left or right resembling the “Bell Curve” of normal distribution, although some data did follow it closely but not perfectly, as is the usual case.
RESULTS
Overall morphological features of craniofacial skeleton in Bangladeshi young adults Table 1 shows the means of linear and angular measurements for Bangladeshi young adults. On comparison between the male and female subjects, no significant differences were found for all the measurement items excluding both SL and SE distances, which exhibited a statistically significant difference between male and female subjects with a confidence level of P < 0.05.
| Parameters | Male n=27 | Female n=25 | Significance | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Average | SD | SE | Average | SD | SE | T value | P value | ||
| SNA | 83.3 | 3.45 | 0.66 | 84.4 | 4.57 | 0.91 | 0.9544 | 0.3445 | |
| SNB | 81.3 | 3.46 | 0.66 | 81.6 | 3.65 | 0.73 | 0.2340 | 0.8159 | |
| ANB | 1.9 | 2.6 | 0.50 | 2.8 | 2.7 | 0.55 | 1.1162 | 0.2697 | |
| SND | 79.2 | 3.39 | 0.65 | 79.3 | 3.85 | 0.77 | 0.1669 | 0.8681 | |
| U_1 to NA | 30.2 | 6.23 | 1.19 | 29.4 | 7.09 | 1.41 | 0.4690 | 0.6411 | |
| U_1 to NA_mm | 8.0 | 2.42 | 0.46 | 7.9 | 1.94 | 0.38 | 0.2352 | 0.8150 | |
| L_1 to NB | 29.2 | 7.73 | 1.48 | 32.2 | 8.32 | 1.66 | 1.3444 | 0.1849 | |
| L_1 to NB_mm | 7.8 | 3.38 | 0.65 | 8.21 | 2.77 | 0.55 | 0.4686 | 0.8631 | |
| Interincisal | 119.2 | 10.62 | 2.04 | 116.1 | 10.03 | 2.00 | 1.0627 | 0.2930 | |
| SN_to_OP | 12.8 | 3.37 | 0.64 | 13.3 | 4.42 | 0.61 | 0.8784 | 0.3839 | |
| SN_to_GoGn | 25.0 | 6.34 | 1.22 | 26.6 | 6.3 | 1.26 | 0.9103 | 0.3670 | |
| SE_mm_ | 24.3 | 2.49 | 0.48 | 21.6 | 3.09 | 0.61 | 3.5367 | 0.0009* | |
| SL_mm_ | 62.7 | 8.31 | 1.59 | 56.7 | 10.09 | 2.01 | 2.3583 | 0.0223* | |
When Bangladeshi subjects were compared with Caucasians, most measurement items exhibited a significant difference from the means of the Caucasians excluding ANB and SN to OP angles that depicted no statistically significant differences between Bangladeshi and Caucasian subjects [Table 2].
| Parameters | Caucasian norm[22] | Bangladeshi norm total N=52 | Significance P value | |||
|---|---|---|---|---|---|---|
| Mean | SD | Mean difference | ||||
| SNA | 82 | 83.8 | 4.02 | −1.8 | 0.002* | |
| SNB | 80 | 81.5 | 3.52 | −1.5 | 0.003* | |
| ANB | 2 | 2.3 | 2.70 | −0.3 | 0.348 | |
| SND | 76 | 79.3 | 3.58 | −3.3 | 0.001* | |
| U_1 to NA | 22 | 29.8 | 6.60 | −7.8 | 0.001* | |
| U_1 to NA_mm | 4 | 8.0 | 2.18 | −4.0 | 0.001* | |
| L_1 to NB | 25 | 30.6 | 8.08 | −5.6 | 0.001* | |
| L_1 to NB_mm | 4 | 8.0 | 3.08 | −4.0 | 0.001* | |
| Interincisal | 131 | 117.7 | 10.3 | 13.3 | 0.001* | |
| SN_to_OP | 14 | 13.3 | 4.42 | 0.7 | 0.258 | |
| SN_to_GoGn | 32 | 25.8 | 6.33 | 6.2 | 0.001* | |
| SE_mm_ | 22 | 23.0 | 3.10 | −1.0 | 0.024* | |
| SL_mm_ | 51 | 59.8 | 9.61 | −8.8 | 0.001* | |
Figure 2 shows a clear difference in the polygonic portrayal of Caucasian and Bangladeshi dento-facial patterns.

- Polygonic portrayal of Bangladeshi dentofacial patterns from Steiner analysis
In Figure 3, the percentages of Bangladeshi young adults with protrusive, normal, and retrusive facial profiles according to Steiner “S” line are shown. The most prevalent lateral soft tissue profile in Bangladeshi subjects is protrusive.

- Percentages of facial profile types in this study according to Steiner 'S' LINE
Skeletal measurements
Evaluating SNA and SNB angles, it is interesting to note that both exhibited a significantly greater value in Bangladeshi subjects than in the Caucasians. It is thus indicated that the maxillary and mandibular apical bases were more prognathic (P < 0.05) in the Bangladeshi population when compared to the Caucasians [Table 2]. Meanwhile, no statistically significant differences in the antero–posterior position of the maxillary and mandibular apical bases to the cranial base were found between male and female subjects [Table 1].
ANB angle indicates an antero–posterior relationship between the maxillary and mandibular apical bases relative to the cranial base. The value of this angle for Bangladeshi population was almost similar to the mean reported by Steiner without any significant difference [Table 2]. Polygon also shows that the ANB angle is very close to that of the Caucasians [Figure 2]. In addition, there was no significant difference in ANB angle between male and female Bangladeshi subjects [Table 1].
The mean of SND angle was significantly larger in Bangladeshi subjects, indicating that the centre of mandibular symphysis is placed more anteriorly (P < 0.05) than in the Caucasians [Table 2]. When compared between male and female Bangladeshi subjects, no significant difference was found between them [Table 1].
Mandibular plane angle to the cranial base (SN_to_ GoGn angle) of Bangladeshi adults was significantly smaller (P < 0.001) than that of the Steiner’s norm [Table 2]. From this result, it may be a reasonable assumption that Bangladeshi people have a more prominent horizontal growth than the Caucasians. Meanwhile, there was no significant difference in the means between the males and females [Table 1].
Bangladeshi population showed a smaller inclination of occlusal plane (SN_to_Op angle) than the Caucasians, although this difference was not statistically significant (P = 0.258) [Table 2]. This study also exhibited no significant difference in SN-to-OP angle between male and female subjects [Table 1].
Dentoalveolar measurements
U_I to NA (both angular and linear) experienced a significantly greater value in the Bangladeshi subjects. L_1 to NB (both angular and linear) also exhibited a significantly greater value in the Bangladeshi subjects than in the Caucasians [Table 2]. These findings along with a significantly smaller interincisal angle [Table 2] of the Bangladeshi young adults demonstrated a fact that the upper and lower incisors of Bangladeshi subjects were more procumbent and protracted when compared with those of Caucasian subjects. As far as the comparison between male and female subjects was concerned, U_ I to NA, (both angular and linear), L_1 to NB (both angular and linear) and interincisal angle did not show any statistically significant differences [Table 1].
This study revealed a wide divergence in the SE and SL distances in the Bangladeshi population. Mean of SE distance was significantly greater than that of Caucasians (P < 0.05) [Table 2]. In addition, the SL distance in relation to the cranial base was significantly larger in Bangladeshi sample than in the Caucasians (P < 0.001) [Table 2]. Both SL and SE distances depicted a statistically significant difference (P < 0.05) between male and female subjects with a smaller value in the females than in the male subjects, suggesting that anteroposterior length of the mandible in relation to the cranial base was significantly larger in Bangladeshi males than in the females [Table 1].
Soft tissue measurement
According to Steiner, the lips in well balanced faces should touch a line extending from the soft tissue contour of the chin to the middle of an S formed by the lower border of nose. Lips located beyond and behind this line tend to be protrusive and retrusive, respectively.
This study, however, showed that among the study population, 73% of the Bangladeshi samples had protrusive lip, 19% had normal lip, and only 8% had retrusive lip [Figure 3]. Thus, this study suggests that the Bangladeshi young adults have a high tendency to have a protrusive lip profile when compared to Caucasian samples.
DISCUSSION
There is little information available for the emergence of the racial features of Bengali population. There has been no significant research for this subject and available data extracted from the past are not even reliable. Indian educationist Mitra[24] compiled information on the emergence of racial features of Bengali population from the linguistic and ethnological evidence and has elaborately discussed in his book “Tribes and castes of West Bengal.” According to him, the earliest inhabitants of India as well as of Bengal were a long-headed, dark-skinned, and broad-nosed race whom the modern anthropologists called Proto-Australoid or Austro-Asiatic or Nisadic type. These people spoke the Austric whereas a modern type of the Austric through modification in India became Munda that is spoken by many tribes and castes. This race contributes largely to the so-called lower castes of Bengal, namely, the Bagdis, the Bauris, the Chandals and others. Moreover, there are many Austric words in the vocabularies of Bengali language.
Chronologically, the next race migrated to India from the west belonged to Matrilineal Mediterranean stock. The present specimen of long-headed, tall-, and sharp-nosed population is the Tamils of south India and most Dravidian languages at present have been derived from those originally spoken by this race. In India, the Mediterraneans are well known as Dravidians. In a migration of the Mediterraneans, the round-headed Armenoid came to India from Asia Minor and Mesopotamia via Persia, in course of time when the Mediterranean and the Armenoid penetrated into Bengal. People having long head, fine nose, and tall stature came to India and belonged to the same race as the Nordics of Europe. Their penetration into Bengal was not only slow but also late in the history. They were the Aryans, the creators of the Vedic Civilization.
Kharbanda[25] reported that bimaxillary protrusion, a variation in the facial profile, exists among ethnic groups from the southern parts of India mostly Dravidians, Nigroid, and certain races from Indonesia. The findings of this study highly support that the Bengalis have an increased tendency toward bimaxillary protrusion possibly due to a contribution from their predominant Dravidian ancestry.
The State of Assam lies in close geographic proximity to Bangladesh and thus results of the study conducted by Nabanita and Mitali[26] [Table 3] on Assamese young adults appear to be quite similar to those of this study. State of Kerala is located in the most southern part of India. Results of the study by John[27] [Table 3] on adult population of Kerala were almost the same as the findings in this study. Another city, Bangalore, located in the eastern and southern part of India and the findings of the study conducted by Rajendran et al.[28] [Table 3] on adult Bangaloreans appear to be quite similar to those of this study. This may be due to the common ethnic background that the Bengalis, the Keralaties and Bangaloreans share. These areas are the eastern and southern parts of India that were once predominantly inhibited by the Astrics (Austro Asiatic), the Dravidians and the Armenoid who penetrated into Bengal. Thus, it may be assumed that these three races may have contributed a lot to the craniofacial morphology of the present Bengalis.
| Cephalometric parameters | Caucasian norm[22] | Present study (Bangladeshis) | Assamese (Nabanita et al.)[26] | Kerala (John)[27] | Bangalore (Rajendran et al.)[28] | Kashmiris (Mengi)[29] | Bombay (Kamalamma)[30] |
|---|---|---|---|---|---|---|---|
| SNA | 82 | 83.8 | 84.5 | 84.14 | 83.45 | 81.30 | 81.40 |
| SNB | 80 | 81.5 | 81.41 | 81.85 | 80.50 | 78.0 | 79.18 |
| ANB | 2 | 2.3 | 3.01 | 2.27 | 2.95 | 3.30 | 2.22 |
| SND | 76 | 79.3 | 78.67 | 79.36 | 77.85 | 76.0 | 76.22 |
| U_1 to NA | 22 | 29.8 | 25.04 | 27.44 | 25.85 | 18.0 | 27.26 |
| U_1 to NA_mm | 4 | 8.0 | 4.11 | 7.46 | 6.65 | 5.20 | 9.19 |
| L_1 to NB | 25 | 30.6 | 29.25 | 30.75 | 28.45 | 24.10 | 30.21 |
| L_1 to NB_mm | 4 | 8.0 | 4.63 | 7.5 | 6.85 | 5.70 | 8.89 |
| Interincisal | 131 | 117.7 | 122.71 | 119.69 | 122.95 | 134.60 | 120.79 |
| SN_to_Op | 14 | 13.3 | 13.63 | 11.79 | - | 15.00 | 15.65 |
| SN_to_GoGn | 32 | 25.8 | 26.6 | 27.91 | 29.01 | 30.00 | 28.75 |
| SE_mm_ | 22 | 23.0 | 20.97 | 21.46 | 21.40 | - | 22.78 |
| SL_mm | 51 | 59.8 | 53.17 | 59.66 | 57.40 | - | 53.92 |
SNA = Sella-Nasion-Point A angle; SNB = Sella-Nasion-Point B angle; ANB = Point A-Nasion-Point B angle; SND = Sella-Nasion-Point D angle; SN = Sella Nasion plane; OP = Occlusal plane; GoGn = Gonion-Gnathion ; SE_mm = Sella-E point distance, SL_mm = Sella-L point distance,U_1 =long axis of upper central incisor,L_1= long axis of lower central incisor,NA= Nasion to point A plane, NB= Nasion to point B plane
On the other hand, Kashmir and Bombay (Mumbai) are located in the northern and western parts of India. Previous studies of Mengi[29] [Table 3] on Kashmiri sample and Kamala et al.[30] [Table 3] on Bombay sample revealed that the maxillary and the mandibular apical base (SNA and SNB) were less prognathic in the samples than in the Bangladeshis. Thus, the present findings are consistent with data from other studies on populations of close geographic proximity and ethnic background [Table 3]. The data of studies of Steiner’s analysis of different Indian ethnic groups (except for Assamese) were obtained from compilation by Kumar.[31]
Mohammad et al.[32] [Table 4] found in the Malaysian Malay people that the maxilla and mandible were located more forward than Caucasian. They also demonstrated bimaxillary dental protrusion when compared to the Caucasian. In fact the Malaysian Malay has more protrusive upper and lower lips. This study reveals that Bangladeshis also have an increased tendency toward bimaxillary protrusion. Malaysian Malay has higher cant of both the occlusal and mandibular planes, and posterior rotation of the mandible when compared to the Caucasian. In contrast, the Bangladeshis exhibit a more prominent horizontal growth pattern with lesser cant of both the occlusal and mandibular planes.
| Cephalometric parameters | Caucasian norm[22] | Present study (Bangladeshis) | Malaysian (Mohammad H. A et al.) [32] | Japanese (Miura et al.)[4] | Korean (In-Chool park. et al.)[17] |
|---|---|---|---|---|---|
| SNA | 82 | 83.8 | 83.7 | 81.3 | 81.15 |
| SNB | 80 | 81.5 | 81.2 | 76.8 | 78.7 |
| ANB | 2 | 2.3 | 2.5 | 4.5 | 2.5 |
| SND | 76 | 79.3 | 77.5 | 73.4 | 75.8 |
| U_1 to NA | 22 | 29.8 | 24.1 | 24.1 | 23.4 |
| U_1 to NA_mm | 4 | 8.0 | 11.6 | 5.9 | 7 |
| L_1 to NB | 25 | 30.6 | 32.3 | 31.2 | 27.4 |
| L_1 to NB_mm | 4 | 8.0 | 11.0 | 7.8 | 7.2 |
| Interincisal | 131 | 117.7 | 121.0 | 120.3 | 126.55 |
| SN_to_Op | 14 | 13.3 | 16.7 | 20 | 16.9 |
| SN_to_GoGn | 32 | 25.8 | 34.5 | 36.2 | 33.4 |
| SE_mm_ | 22 | 23.0 | - | 21 | - |
| SL_mm | 51 | 59.8 | - | 41.1 | - |
SNA = Sella-Nasion-Point A angle; SNB = Sella-Nasion-Point B angle; ANB = Point A-Nasion-Point B angle; SND = Sella-Nasion-Point D angle; SN = Sella Nasion plane; OP = Occlusal plane; GoGn = Gonion-Gnathion ; SE_mm = Sella-E point distance, SL_mm = Sella-L point distance,U_1 =long axis of upper central incisor,L_1= long axis of lower central incisor,NA= Nasion to point A plane, NB= Nasion to point B plane
Miura et al.[4] [Table 4] revealed that Japanese people were not protrusive skeletally relative to the Caucasians but did exhibit dentoalveolar protrusion resulting in an acute interincisal angle. Japanese had higher cant of both the occlusal and mandibular planes exhibiting larger vertical growth pattern than the Caucasians. In contrast, the Bangladeshis exhibit larger horizontal growth. With respect to Korean craniofacial morphology, Park et al.[17] [Table 4] reported dentoalveolar protrusion, higher cant of both the occlusal and mandibular planes compared to the Caucasians.
It is interesting to note that the Malaysian Malay people have higher cant of both the occlusal and mandibular planes similarly to the Japanese and Korean people and the feature of skeletal and dentoalveolar bimaxillary protrusion is also similar to Bangladeshi and south Indians. More extensive and detail studies are highly anticipated to be carried out to find out what could be the cause of such diverse craniofacial morphology commonly observed in different racial groups in southeast Asian countries.
CONCLUSIONS
In line with the present findings, it is evident that, in the Bangladeshi population with well-balanced faces, there are some fundamental variations in the craniofacial structure when compared to Steiner’s norms in the Caucasians. These results would be beneficial for appropriate diagnosis and orthodontic treatment planning for Bangladeshi young adult patients. The results of this study also support the idea that a single standard of facial esthetics should not be applied to other racial and ethnic groups. The following differences and similarities have been demonstrated in the Bangladeshi samples as compared to the Caucasian samples.
The maxillary and mandibular apical bases in relation to the anterior cranial base were located more anteriorly or prognathic as compared to the Caucasian samples
The mandibular plane angle to the cranial base plane (SN-GoGn angle) was smaller, suggesting a more prominent horizontal growth pattern in Bangladeshis
Bangladeshi young adults had a protrusive dentoalveolar structure when compared to the Caucasians
Significant differences in the SE and SL distances were found between Bangladeshi population and the Caucasians
No significant differences were found in most craniofacial features between Bangladeshi male and female.
Thus, it is concluded that most cephalometric measurements in the Bangladeshi subjects were significantly different from the Steiner’s Caucasian norms. The results of this study have clinical implications in the diagnosis and treatment planning of Bangladeshi young adult patients. In the skeletal and dentoalveolar systems, adult Bangladeshis demonstrated more bimaxillary protrusion with a tendency to the smaller mandibular plane angle. Therefore, in the diagnosis and treatment planning, it seems that more maxillary skeletal protrusion is more acceptable than in the Caucasians. This study also depicts that the Astrics (Austro Asiatic), Dravidians, and Armenoid who penetrated into Bengal in the early ages may have contributed a lot to the craniofacial morphology of the present Bengalis. To draw a decisive conclusion of the Steiner‘s analysis on Bangladeshi population for diagnosis, treatment planning and prognosis, further studies are needed with a larger study population after proper screening of facial types.
Source of Support:
Nil.
Conflict of Interest:
None declared.
Author Help: Online submission of the manuscripts
Articles can be submitted online from http://www.journalonweb.com. For online submission, the articles should be prepared in two files (first page file and article file). Images should be submitted separately.
First Page File: Prepare the title page, covering letter, acknowledgement etc. using a word processor program. All information related to your identity should be included here. Use text/rtf/doc/pdf files. Do not zip the files. Article File: The main text of the article, beginning with the Abstract to References (including tables) should be in this file. Do not include any information (such as acknowledgement, your names in page headers etc.) in this file. Use text/rtf/doc/pdf files. Do not zip the files. Limit the file size to 1024 kb. Do not incorporate images in the file. If file size is large, graphs can be submitted separately as images, without their being incorporated in the article file. This will reduce the size of the file. Images: Submit good quality color images. Each image should be less than 4096 kb (4 MB) in size. The size of the image can be reduced by decreasing the actual height and width of the images (keep up to about 6 inches and up to about 1800 x 1200 pixels). JPEG is the most suitable file format. The image quality should be good enough to judge the scientific value of the image. For the purpose of printing, always retain a good quality, high resolution image. This high resolution image should be sent to the editorial office at the time of sending a revised article. Legends: Legends for the figures/images should be included at the end of the article file.
References
- The organization of the growth process. In: Fetus into Man: Physical Growth from Conception to Maturity (2nd ed). Ware, England: Castlemead Publications; 1989. p. :165-77.
- [Google Scholar]
- Man’s Most Dangerous Myth, The Fallacy of Races. New York: Columbia University Press; 1942.
- Races: A study of the problems of race formation in man. Springfield: Charles C.Thomas; 1950. p. :65-71.
- Cephalometric standards for Japanese according to the Steiner analysis. Am J Orthod. 1965;51:288-95.
- [Google Scholar]
- A determination of cephalometric norms for the Negro race. Am J Orthod. 1968;54:670-82.
- [Google Scholar]
- Cephalometric standards of Steiner analysis established on Chinese children. J Formosa Med Assoc. 1971;70:97-102.
- [Google Scholar]
- A comparison of cephalometric norms for the African Bantu and Caucasoid population. Eur J Orthod. 1983;5:223-4.
- [Google Scholar]
- A soft tissue cephalometric analysis and its use in orthodontic treatment planning. Am J Orthod. 1983;84:1-28.
- [Google Scholar]
- Differential diagnosis of American adult male black and white populations using Steiner analysis. Angle Orthod. 1974;44:346-50.
- [Google Scholar]
- A Textbook of Orthodontics. Bristol: Wright; 1986. p. :188-91.
- Cephalometric evaluation of craniofacial variation in normal Saudi population according to Steiner analysis. Saudi Med J. 2000;21:746-50.
- [Google Scholar]
- Cephalometric evaluation of Mexican Americans using the Downs and Steiner analyses. Am J Orthod. 1975;68:67-74.
- [Google Scholar]
- A cephalometric study of Korean adults. Am J Orthod Dentofacial Orthop. 1989;96:54-9.
- [Google Scholar]
- Estimation of cephalometric norm for Bangladeshi children (Steiner method) Bangladesh Journal Of Orthodontics and Dentofacial Orthopedics. 2010;1:1-4.
- [Google Scholar]
- The influence of different facial components on facial aesthetics. Eur J Othhod. 2002;24:1-7.
- [Google Scholar]
- A measuring system for facial aesthetics in Caucasianadolescents: Reproducibility and validity. Eur J Orthod. 2005;27:579-84.
- [Google Scholar]
- Steiner›s cephalometric norms for the Nepalese population. J Orthod. 2011;38:21-31.
- [Google Scholar]
- A concordance correlation coefficient to evaluate reproducibility. Biometrics. 1989;45:255-68.
- [Google Scholar]
- Tribes and castes of west Bengal. Alipore: West Bengal Government Press; 1953. p. :378.
- Diagnosis and Management of Malocculusion and Dentofacial Deformities (1st ed). Haryana: Elsevier; 2009. p. :109.
- Cephalometric evaluation based on Steiner analysis on young adults of Assam. J Indian Orthod Soc. 2009;43:17-22.
- [Google Scholar]
- A cephalometric comparison of the Dento-Skeletal-Facial patterns of adults from Kerala with Normal, class II, and class III malocclusions. MDS thesis. University of Kerala
- [Google Scholar]
- Cephalometric evaluation of young Kashmiri male adults. Data furnished for compilation by Kumar KJ. Cephalometric norms for use with Indian population. Indian Orthodontic Society. Vellore: Samraj; 1987. p. :23.
- Roentgnographic Cephalometric study of craniofacial–dental relationship among Indians exhibiting normal occlusion. J Indian Orthod Soc. 1973;5:43-51.
- [Google Scholar]
- Cephalometric norms for use with Indian population; Indian Orthodontic Society. Vellor: Samraj; 1987. p. :14-23.
- Cephalometric evaluation for Malaysian Malay by Steiner analysis. Sci Res Essays. 2011;6:627-34.
- [Google Scholar]




