Translate this page into:
Palatally displaced and impacted canines – What is taught during postgraduate orthodontics training in Europe?


-
Received: ,
Accepted: ,
How to cite this article: Muslim H, Naoumova J. Palatally displaced and impacted canines – What is taught during postgraduate orthodontics training in Europe? APOS Trends Orthod 2021;11(1):62-73.
Abstract
Objectives:
One of the most challenging orthodontic treatments is displaced and impacted canines palatally displaced canines (PDC/PIC). The aim of this study was, therefore, to assess what postgraduate students are taught about PDC and PIC during their postgraduate orthodontic training (POT) in Europe.
Materials and Methods:
A digital survey containing 22 questions was sent to 164 POT programs in 28 European countries. Questions were asked about which interceptive and surgical treatments are taught, the advantages of different surgical procedures, and what dressing materials and X-rays are used for PIC therapy planning. Reminders were sent 4 times.
Results:
About 43% (71 POT programs) responded. Extraction of deciduous canines (76%) was the most favored interceptive treatment. A closed technique with a gingival margin flap and a gold plated chain was the most commonly taught surgical technique (69%), even though both open and closed exposure of PICs were performed in 54 postgraduate programs. Coe-Pak™ with sutures was one of the preferred dressing materials in open exposure. Active treatment was started before the canine erupted, that is, spontaneous eruption of the tooth following open exposure was not awaited by 1/3 of the respondents and 1/3 left the question unanswered. Closed exposure was more often preferred than open exposure for post-surgical, periodontal, and esthetic reasons. The most common radiographs before surgery were panoramic and intraoral radiographs. Cone-beam computed tomography was taken by half of the respondents when resorption of adjacent teeth was suspected.
Conclusion:
Extraction of deciduous canines as an interceptive approach to PDC and closed exposure of PIC were taught in most of the POT programs.
Keywords
Impacted canines
Displaced canines
Postgraduate education
Orthodontics

INTRODUCTION
In approximately 1–3% of the population, one or both permanent canines fail to erupt.[1] If the displaced canine is left, it may lead to permanent impaction or even to resorption of adjacent teeth. This means that early interceptive treatment is important to attempt to reduce the need for complicated and lengthy orthodontic treatment. Interceptive treatment of palatally displaced canines (PDCs) includes either extraction of the deciduous canine,[2] or extraction in combination with the use of cervical pull headgear,[3] a space maintainer or transpalatal expansion.[4] If eruption of a PDC is not achieved despite interceptive treatment, the canine is most often treated with surgical exposure followed by a fixed appliance. There is a variety of mucosal flap designs to expose the canine, along with a range of different dressings and packing materials.[5] To date, there is no evidence suggesting that one of the two major techniques, open or closed exposure, is superior with regard to operating time, periodontal status, and esthetic assessment, or in patient-reported outcomes.[6,7] A recent study conducted by Naoumova et al. concluded that the choice of exposure technique often depends on the clinician’s personal preferences.[8]
Orthodontic specialty education in Europe was first offered in 1935, and many years later, in the 1950s, the first postgraduate orthodontic training (POT) programs were developed in the Netherlands, the Scandinavian countries, and Switzerland.[9] In 1977, the European Federation of Orthodontic Specialists Associations (EFOSA) was founded, with the aim to improve the quality of education by coordinating the teaching of orthodontics at university and post-university level and to standardize examinations in the specialist training programs in orthodontics.[10] The majority of European countries are active EFOSA members. Similar to EFOSA, the Network of Erasmus Based European Orthodontic Postgraduate Programmes (NEBEOP), founded in 2008, aimed to advance orthodontic postgraduate training in Europe and their guidelines serve as a stamp of quality.[11] Their guidelines dictate that POT should be a minimum of 3 years of full-time education under the supervision of orthodontic specialists in an institute or university with a nationally recognized academic standard. Other criteria for membership include treatment of at least 50 new cases with a variety of malocclusions, a structured theoretical education program, including weekly sessions of lectures, seminars, and treatment planning. A final examination at the end of the 3-year program is also a prerequisite for membership of the NEBEOP. Eighteen countries are listed as members of NEBEOP.[12] The Council of Europe, on the other hand, includes 47 sovereign states; thus, a clear majority of countries in Europe lack a standardized specialist training program that complies with the guidelines set by NEBEOP.
For the past two decades, evidence-based research has increasingly emphasized that health-care decisions should be based on the best available evidence. Decisions about how to treat malocclusions and tooth eruption disturbances may also be affected by the clinician’s knowledge from their POT.
To the best of our knowledge, no studies have investigated what is taught at POT programs about PDC and PIC, two of the most challenging orthodontic problems. The aim of this study was, therefore, to evaluate which interceptive treatments, surgical exposure techniques, and roentgenological examinations postgraduate orthodontics students in Europe are taught to use when diagnosing and treating PDC and PIC.
MATERIALS AND METHODS
A digital questionnaire (esMaker NX3-V3.0 Entergate) was sent to program directors responsible for the POT programs at universities or university clinics in Europe. The POT programs were either member of EFOSA and/ or NEBEOP [Figure 1]. Addresses were obtained from the website of the European Orthodontic Society (EOS) (https://www.eoseurope.org/useful_links/dental_schools). If addresses were missing from the EOS website, the individual orthodontic programs were contacted.

- The map shows all the countries and cities that the survey was sent to. The blue dots indicate post-orthodontic training programs that replied to the survey, red dots indicate places that did not answer, and red dots with a black ring indicate that several programs from the same city did not answer the survey.
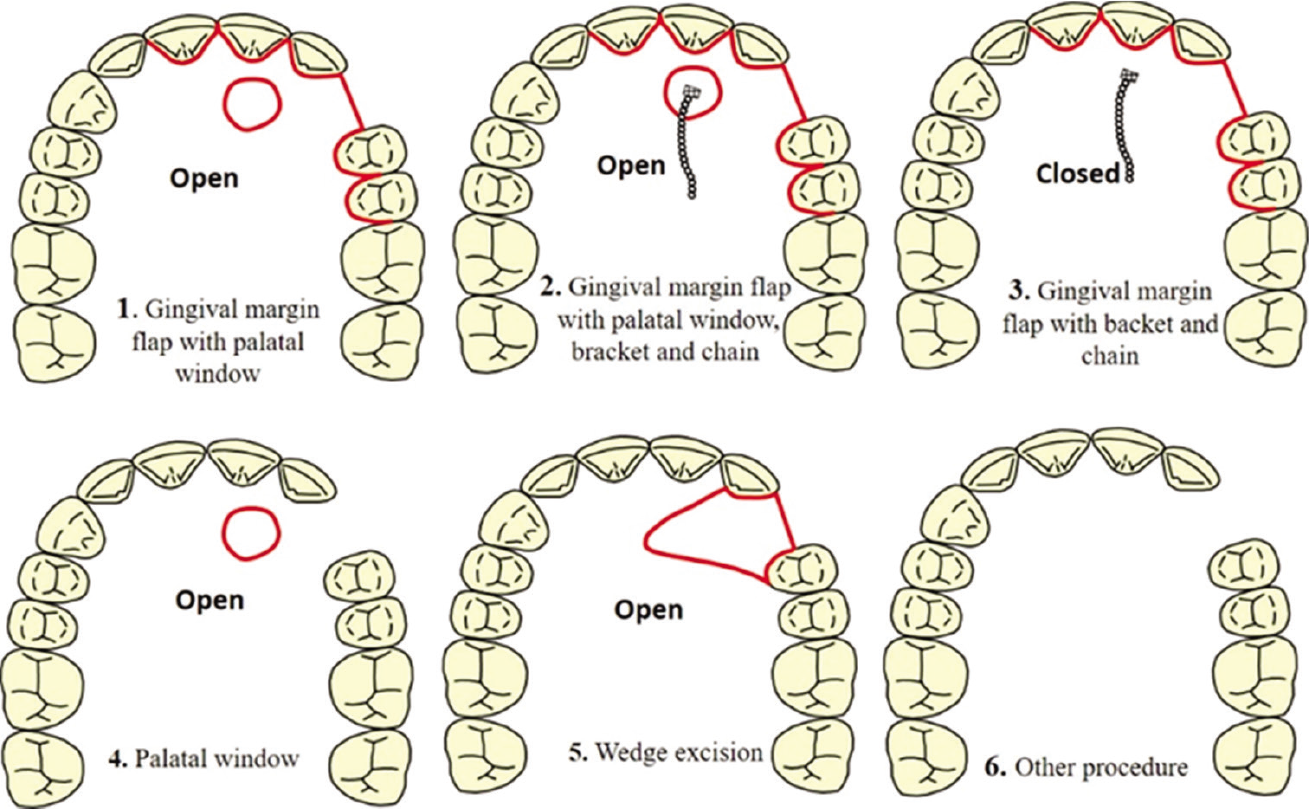
The questionnaire included 22 questions about the treatment and diagnosis of PDC and PIC [Appendix 1] and was not anonymous, as the respondents were asked to report which county and university they represented. The questionnaire was divided into two categories: Open and multiple-choice questions. The multiple-choice questions asked which interceptive approaches are taught and at what age the procedures are performed, as well as the number of PICs that are treated annually. If surgical exposure was not included in the POT program, the participants did not need to continue with the questionnaire, as all the remaining questions related to exposure of PICs: The age of the patient at the time of exposure, who decides and performs the surgical exposure procedure and what the advantages are of different surgical procedures. The participants were also asked which radiographs were taken before the exposure, what kind of dressing was chosen for open exposure and whether spontaneous eruption of the canine was required before starting treatment. An image containing different surgical designs was included in the questionnaire as a visual aid to answering which exposure techniques were taught in their POT program. If techniques other than the images shown were taught, the respondents were given the opportunity to explain their own procedure.
Reminders were sent 4 times. If the questionnaire remained unanswered, it was sent to a second person involved in the POT program and if the survey still remained unanswered, no further attempts were made to obtain an answer. The following members of the NEBEOP, Austria, Belgium, Bosnia and Herzegovina, Czech Republic, Denmark, Finland, Germany, Greece, Italy, Latvia, the Netherlands, Norway, Poland, Portugal, Spain, Sweden, Switzerland, and the United Kingdom, received two additional reminders, on top of the previous four reminders.
The study protocol was approved by the Swedish Ethical Review Authority (2020-04365).
Statistics
Descriptive values of all collected numerical data were calculated using Microsoft Office Excel.
RESULTS
The questionnaire was sent to 164 cities in 28 countries. Out of these, 71 postgraduate programs, 43%, responded [Figure 1]. About 100% response rate was obtained from the Nordic countries, except for Iceland, which does not have a POT program. Malta, Bosnia and Herzegovina, Slovenia, and Estonia also had 100% response rate, although each of these countries only has one or two cities responsible for POT. Cities in the Netherlands, the United Kingdom, and Switzerland returned 70% response rate, while Greece, Hungary, and Slovakia had 50% response rate. Many countries had a poor response rate of 30% or less, including Belgium, Bulgaria, the Czech Republic, France, Germany, Italy, Portugal, and Spain [Figure 1]. Most of the NEBEOP members had a response rate of at least 50% or more.
A clear majority of the universities/university clinics had a 3-year training program in orthodontics (80%).
Extraction of the deciduous canine (76%) was the most commonly taught interceptive treatment approach followed by extraction of the deciduous canine in combination with extraoral traction (41%) or rapid maxillary expansion (RME) (41%) [Figure 2]. In most POT programs, interceptive treatment was performed on individuals 10–13 years of age (64%) and in 33% at age 9 or below.
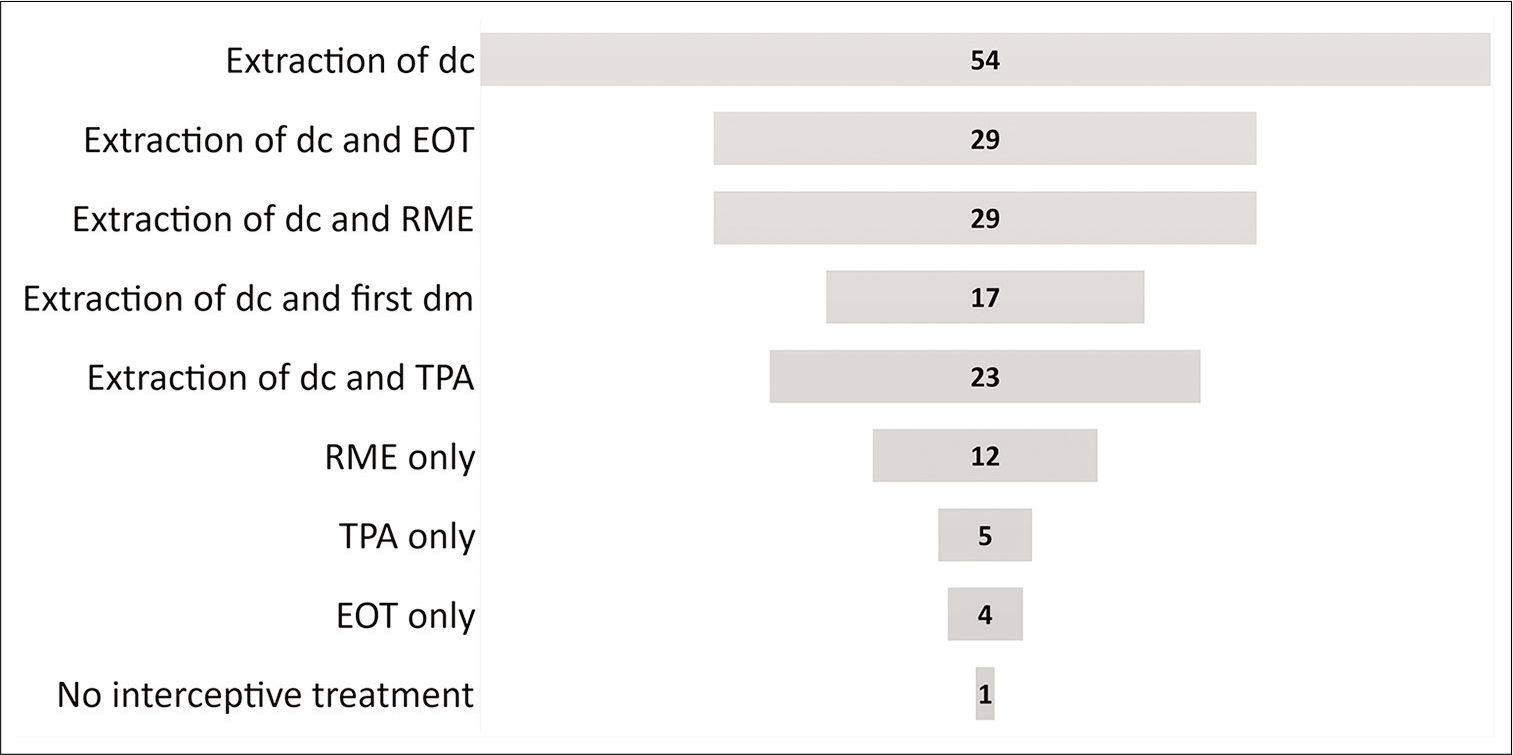
- Interceptive treatment approaches that are taught in postgraduate orthodontics programs, specified in numbers of educational center. EOT: Extraoral traction, TPA: Transpalatal arch, RME: Rapid maxillary expansion, dc: Deciduous canine, dm: Deciduous molar.
Thirty POT programs performed more than 20 surgical exposures every year, the rest had approximately 10–20 exposures yearly. Surgical exposure of PICs was mostly performed (68%) in patients 12–15 years of age, but in 16% of the POT programs, the patients were 12 years old, and in the remaining programs, the patients were 16–20 old.
The oral and maxillofacial surgeon usually performed the surgical exposures (71%) followed by the pedodontist (13%) and the orthodontist (8%). The surgical technique was most often chosen by the orthodontist in collaboration with the oral surgeon (56%). In 20%, it was decided by the orthodontist alone and a similar percentage by the performing surgeon alone.
Both open and closed surgical exposure of PICs was taught in 54 of the POT programs (76%) that responded to the survey. Closed exposure as the only surgical technique was taught in 13 POT programs, while open exposure as the only surgical method was preferred in three places. A closed technique with a gingival margin flap, bracket, and chain was the surgical technique taught in most places (69%). Other procedures included open procedures with a gingival flap with a palatal window, with or without a bracket and chain (21% and 16%, respectively) [Figure 3].
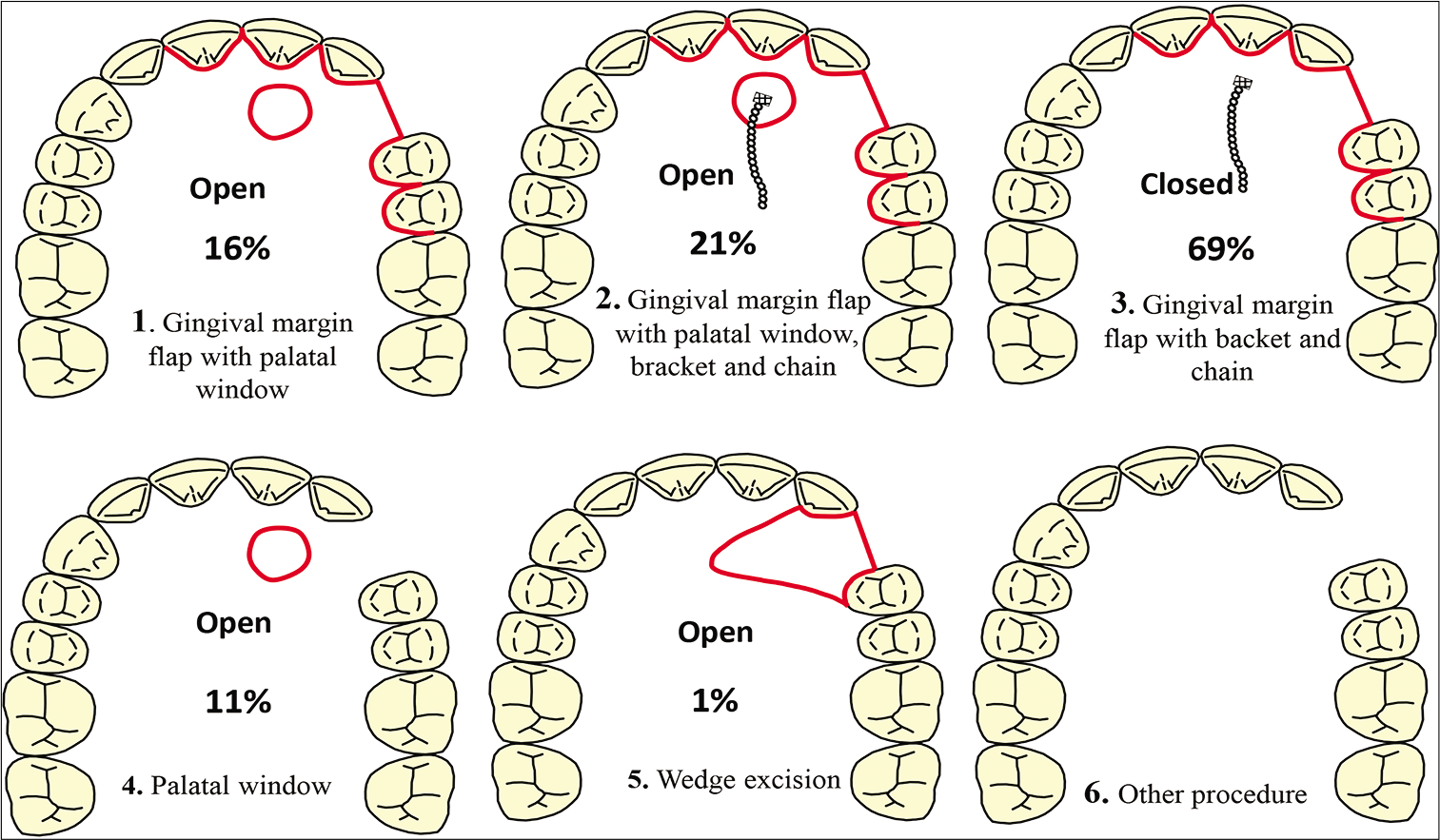
- Different surgical techniques to expose palatally impacted canines. The percentage below each image indicates how often a certain technique was selected by the respondents.
The open surgical technique was favored due to the reduced risk of reoperation (35%) and the fewer post-surgical complications (23%), compared with closed exposure. Smaller post-surgical mucosal defects (49%) and faster immediate post-surgical recovery (32%) were the supposed benefits of choosing a closed technique over an open technique. Concerning orthodontic treatment, 48% of the respondents responded that the open surgical technique allowed for a better view of the tooth position and the direction of traction, while a majority of those who favored the closed technique pointed out the possibility to immediately distalize the canines as being an advantage of closed exposure. Thirty-nine POT programs (55%) replied that the closed surgical exposure technique would result in better periodontal attachment and less gingival recession (45%). In contrast, 12 POT programs answered that open exposure results in better periodontal attachment and 10 POT programs thought that open exposure would lead to less gingival recession [Table 1]. Thirty respondents failed to answer why they chose one exposure technique over another. However, 25% of all respondents stated that they chose the closed exposure when the canine is in a deep position, while a superficially positioned canine would be exposed by open exposure.
| Surgery and post-surgery recovery | Open exposure (%) | Closed exposure (%) |
|---|---|---|
| Less pain during surgery Less complications with the surgery Shorter surgical time Faster immediate post-surgery recovery Fewer reoperations Less risk of mucosa healing Smaller mucosa defects post-surgery |
n=2 (3) n=16 (23) n=11 (16) n=10 (14) n=25 (35) |
n=5 (7) n=10 (14) n=5 (7) n=23 (32) n=13 (18) n=21 (30) n=35 (49) |
| Orthodontic treatment | Open exposure | Closed exposure |
| Less pain during active orthodontic treatment Better view of the tooth position and the direction of traction Shorter duration of active orthodontic treatment Easier orthodontic mechanics No lost chain Possibility to distalize immediately |
n=9 (13) n=34 (48) n=14 (20) n=17 (24) n=19 (27) |
n=10 (14) n=6 (9) n=34 (48) |
| Periodontal health and esthetic post-orthodontic treatment | Open exposure | Closed exposure |
| Better periodontal attachment levels Better alveolar bone level Less gingival recession Less difference in crown height between the impacted and the normally erupting side |
n=12 (17) n=1 (1) n=10 (14) n=10 (14) |
n=39 (55) n=19 (27) n=32 (45) n=14 (20) |
A deeply positioned palatal canine was defined as the tooth being in proximity to the apices or apical third of neighboring teeth (17%) or when it was covered by a substantial amount of bone (10%). A deeply positioned palatal canine could also be defined as not being present on palpation, being significantly displaced, located close to the midline or close to the nasal floor. Two universities mentioned using sector measurement as described by Ericson and Kurol[13] to define the impaction. In most cases, a deeply positioned PIC was diagnosed with cone-beam computed tomography (CBCT) (40%), while a few POT programs used panoramic radiographs (PAN) (4%) or parallax radiographs (4%) to diagnose a deeply positioned palatal canine. A superficial PIC was defined as such when it was palpable (34%) or having little or no bone covering (10%). Other definitions included being superficially located in relation to neighboring teeth (4%) and minimal displacement (1%), and one university used sector measurements.[13] CBCT was used in 14% of the POT programs to diagnose superficially located impacted canines. About 8% of the questionnaires mentioned diagnosis by PAN and by intraoral radiographs. Other diagnostic radiographs included parallax radiograph (3%) and computed tomography (CT) (1%). Approximately one-fifth of the respondents did not answer how they define and diagnose deeply and superficially positioned PICs.
Coe-Pak with sutures was the most commonly used dressing material (23%); however, 23 POT programs did not reply. Glass ionomer cement was the dressing material of choice in seven places, and in nine programs, no dressing material was used [Figure 4]. Almost half of the respondents failed to answer how long they would leave the dressing material in place. There was a variety of answers to this question as it was an open question. Because of the many alternatives, the answers were divided into three different subgroups. One questionnaire stated that they were unsure of how long they recommended that the dressing be left in place. Of the remaining 35 that replied, only five said that they would leave the dressing material in place until eruption of the tooth. Fifteen POT programs taught their students to wait 1 week before removing the dressing material (21%), while 12 told their students to leave the dressing material more than 2 weeks (17%). About 34% of the respondents did not wait for spontaneous eruption of the canine following open exposure, while one-fifth (18%) waited 3–6 months before applying any orthodontic traction to the exposed canine. One-third of the respondents left this question unanswered [Figure 5].
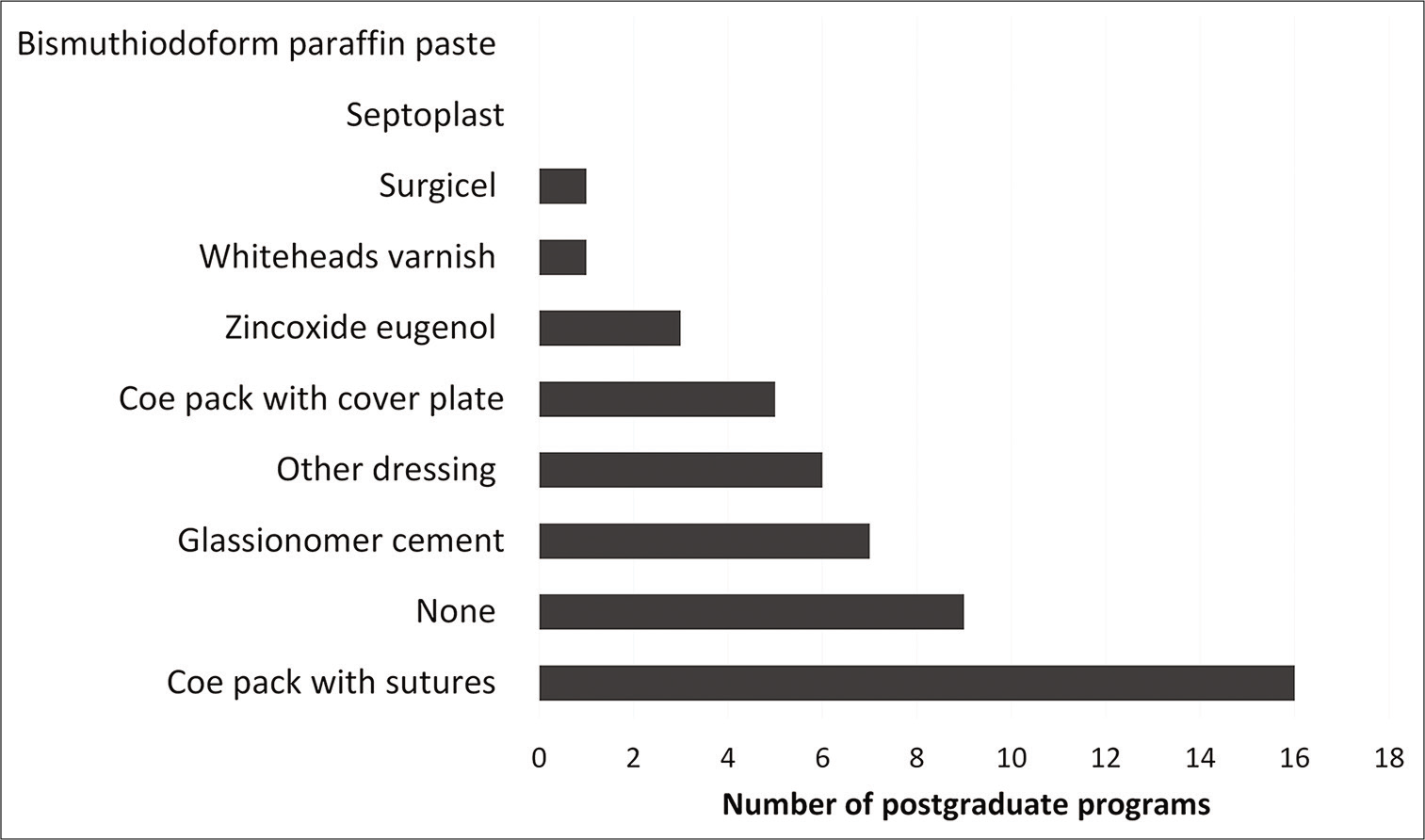
- Type of dressing preferred for use in open exposure.
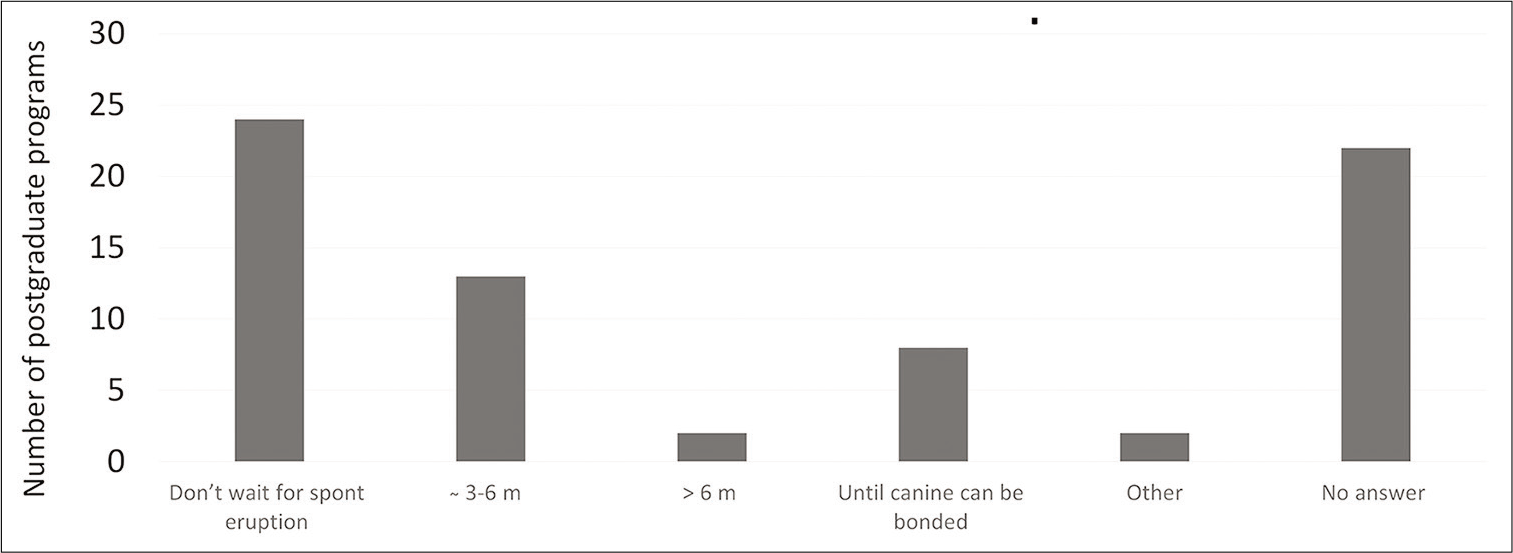
- The time allowed for the canine to erupt spontaneously before starting active orthodontic movement, after open exposure.
A majority used a gold plated chain when teaching the closed technique (63%), while 31% used a variety of materials, including steel or stainless steel ligatures or chains, titanium chains, and solid gold chains.
CT/CBCT machines were available in 55 POT programs, and 31% of the respondents claimed that CBCT images were always used [Table 2]. About 57% taught their postgraduate students to use CBCT in connection with PIC if there was a risk of resorption of the neighboring teeth. Other reasons for using CT/CBCT were if other radiographic evaluation was unsatisfactory (6%), or if there were no clinical signs of the canine position (3%). Five universities failed to report their reasoning behind the use of CT/CBCT. Many of the respondents always used PAN during therapy planning of PDC and PIC (82%), while a substantial number of universities claimed also to use intraoral radiographs (48%) [Table 2].
| Types of radiograph | No answer | Always | Sometimes | Never |
|---|---|---|---|---|
| Intraoral radiograph | 15 | 48 | 27 | 10 |
| Panoramic radiograph | 7 | 82 | 10 | 1 |
| CBCT | 3 | 31 | 66 | 0 |
| CT | 37 | 1 | 13 | 49 |
DISCUSSION
Postgraduate education in orthodontics, one of the first specialist fields in dentistry, is highly challenging not only for the postgraduate students but also for the educators who need to keep themselves updated with the latest evidence-based knowledge. The scope of the present study was, therefore, to investigate if POT programs in different European countries are teaching similar approaches to handling some of the most challenging problems in orthodontics, PDC, and PIC. The main important finding was that extraction of a deciduous canine was the most frequently taught interceptive treatment [Figure 2]. Previous RCT studies and systematic reviews have shown that early extraction is both effective and the preferable approach to intercepting PDCs.[2-3,14-16] Open or closed exposure of PICs is two commonly used surgical techniques; yet, there is little evidence that supports one method over the other,[6] leaving the choice of surgical technique to the preference of the surgeon and/or the orthodontist.[8] This was reflected in the present survey by the wide distribution of advantages mentioned for each surgical method by the respondents [Table 1]. A survey from the UK[17] found that half of the 325 orthodontists favored open exposure, in contrast to another survey, where closed exposure was the preferred choice of oral and maxillofacial surgeons.[18] Our results show that both surgical techniques were performed in two-thirds of the POT programs. On the other hand, closed exposure with a gingival margin flap was the surgical technique taught in most places [Figure 3]. Other preferred procedures included open exposure with a gingival flap with a palatal window, with or without a bracket and chain. The considerable variation in the design of mucosal flaps noted in the present study is in line with other reports.[5]
Many respondents favored a closed exposure because it was thought to result in better periodontal attachment, less gingival recession, faster immediate post-surgical recovery, and smaller post-surgical defects [Table 1]. On the other hand, the reduced risk of reoperation and shorter post-surgical recovery were attributed to open surgical exposure by the advocates of that procedure [Table 1]. There is, however, no evidence in the literature to support differences in either periodontal health or in post-operative pain.[7,18] Even though closed exposure was preferred for deeply positioned canines and open exposure for superficial canines, most respondents resorted to their preferred surgical technique, regardless of the tooth position. To the extent of our knowledge, there are no studies evaluating the treatment outcome of different surgical exposures of deeply versus superficially located canines, nor are there any studies on the orthodontic benefits of different surgical techniques. Half of the respondents in our study mentioned the feasibility of the tooth position and direction of traction as orthodontic benefits with open exposure, while the possibility to distalize the canine immediately after surgery was stated as a benefit of closed exposure. Thirty out of 78 respondents failed to answer why they chose one surgical procedure over the other.
Numerous surgical dressings are used in open exposure.[5] Coe-Pak™ with sutures was the preferred dressing material in the present study, even though many other alternatives were mentioned [Figure 4]. Instead of conventional packs, glass ionomer cement bonded to the canine crown may be used, allowing the canine to self-erupt for several months before orthodontic traction is applied.[8] Glass ionomer cement contains a biocompatible material, known not to cause postoperative discomfort or complications.[19] As there are no guidelines on which surgical dressing should be used when exposing PICs or when they should be removed, the answers in our study were divergent and many respondents did not reply [Figure 4]. Despite a variety of answers, a clear majority of the respondents did not teach their residents to wait for spontaneous eruption of the canine post-surgery [Figure 5]. A gold plated chain was bonded to the exposed canine when the closed exposure technique was taught in a majority of the training programs, which is in line with previous reports.[5,8]
In most POT programs, surgical exposures were performed on patients between 12 and 15 years of age. Interceptive treatment of PDCs is recommended before the age of 13, especially in cases that benefit from deciduous canine extraction.[20] In a prospective longitudinal study on delayed diagnosis of PIC, Brorsson and Naoumova[21] found that most patients who had surgical exposure of a PIC were between 12 and 15 years, a result can be applied to countries with regular dental examinations. In accordance with the previous studies, the oral and maxillofacial surgeon performed the exposure in 70% of the POT programs.[5,18] The surgical technique was most often chosen by the orthodontist in collaboration with the oral surgeon, which is in line with a previous study.[8]
Two-dimensional images, PAN, followed by intraoral radiographs were the first-hand choice for treatment planning of PDC/PIC, in contrast to an earlier study.[8] An interesting finding was that 1/3 of the respondents taught their students to “always” use CBCT, while half of the POT programs taught their students to use CBCT if the canine posed a threat to the apices of the neighboring teeth.
The present study had a low response rate (43%), despite multiple reminders. In general, electronic surveys have a lower response rate compared with paper-based questionnaires. On the other hand, there are many advantages to electronic mail surveys, such as cost efficiency, ease of administration, and immediacy of results.[22] A possible reason for our low response rate could be the amount of questions in the survey covering both multiple-choice questions and several open-ended questions, which may take longer to complete. According to Kittleson,[23] surveys should be short and non-invasive, including follow-up reminders. Another possible reason for the present survey being left unanswered could be poor English language proficiency. Difficulty of understanding the questions would make it harder to reply. Program directors may also have been reluctant to answer questionnaires, or not fully complete a questionnaire, to avoid feeling exposed if they thought their answers might differ from the norm. A higher response rate was received from North Europe, which could tie in with the fact that most of the countries where we had an overall medium to high response rate where members of NEBEOP. To improve the response rate, personalized contacts and pre-contacts could be used in future studies.
In 1992, van der Linden[9] developed a 3-year curriculum for postgraduate education in orthodontics. However, later published surveys show that various POT programs in Europe have very dissimilar preconditions with regard to all aspects of orthodontic training and registration within different countries. Several programs only have a theoretical program, with very little clinical training. Some programs may send their students to clinics other than their educational institutions for clinical training.[24] A survey of perceived problems in orthodontic education in 23 European countries at undergraduate, postgraduate, and continuing professional education level showed that funding at postgraduate level was a very common problem for most of the participating countries. A lack of qualified teachers was reported as being worst at postgraduate level and frequently by countries from West, Central, and East Europe. Lack of equipment was a larger problem at all levels of education in Central and East Europe.[25]
Earlier studies have assessed the postgraduate students’ satisfaction with their education, in relation to the length of training and the content of the education program.[22,26] On the other hand, the lack of studies into evidence-based approaches to education programs emphasizes the need for such studies. Education programs need to have a structured curriculum that observes a certain global standard and it is, therefore, vital to evaluate residents and the education curriculum to maintain the quality of a program. In 2006, the World Federation of Orthodontics established a committee[27] whose task was to create guidelines for postgraduate orthodontic education programs. Future studies should evaluate how these guidelines are being followed. In addition, more studies are needed to compare different parts of the POT programs to ensure that the quality of orthodontic education remains high.
CONCLUSION
Extraction of deciduous canines as an interceptive treatment of PDC was taught in most POT programs. Both open and closed exposure of PICs was taught in the majority of the POT programs; however, closed exposure was the preferred technique, for post-surgical, periodontal, and esthetic reasons. Many programs failed to respond and divergent replies were obtained about dressing material, when it should be removed and if the canine should erupt spontaneously following open exposure. 2D images: PAN followed by intraoral radiographs was the first-hand choice before surgery. CBCT was taken by half of the respondents when root resorption of adjacent teeth was suspected, while it was always taken by 1/3 of the POT programs.
Acknowledgments
The authors wish to thank all postgraduate directors for responding to the survey and Birgitta Ahlström for her help with the digital questionnaire.
Declaration of patient consent
Patient’s consent not required as patients identity is not disclosed or compromised.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- The prevalence of malocclusion in Swedish schoolchildren. Scand J Dent Res. 1973;81:12-21.
- [CrossRef] [PubMed] [Google Scholar]
- Extraction of the deciduous canine as an interceptive treatment in children with palatal displaced canines-Part I: Shall we extract the deciduous canine or not? Eur J Orthod. 2015;37:209-18.
- [CrossRef] [PubMed] [Google Scholar]
- Two interceptive approaches to palatally displaced canines: A prospective longitudinal study. Angle Orthod. 2004;74:581-6.
- [Google Scholar]
- An RCT on treatment of palatally displaced canines with RME and/or a transpalatal arch. Eur J Orthod. 2011;33:601-7.
- [CrossRef] [PubMed] [Google Scholar]
- Exposure of unerupted palatal canines: A survey of current practice in the United Kingdom, and experience of a gingival-sparing procedure. Br J Oral Maxillofac Surg. 2010;48:641-4.
- [CrossRef] [PubMed] [Google Scholar]
- Open versus closed surgical exposure of canine teeth that are displaced in the roof of the mouth. Cochrane Database Syst Rev. 2017;8:CD006966.
- [CrossRef] [PubMed] [Google Scholar]
- Periodontal health of palatally displaced canines treated with open or closed surgical technique: A multicenter, randomized controlled trial. Am J Orthod Dentofacial Orthop. 2013;144:176-84.
- [CrossRef] [PubMed] [Google Scholar]
- Glass-ionomer open exposure (GOPEX) versus closed exposure of palatally impacted canines: A retrospective study of treatment outcome and orthodontists' preferences. Eur J Orthod. 2018;40:617-25.
- [CrossRef] [PubMed] [Google Scholar]
- Orthodontic specialists education in Europe: past, present and future. Prog Orthod. 2005;6:14-35.
- [Google Scholar]
- EFOSA History. 2020. Available from: http://www.efosa.eu/content/aboutus/history/history.asp#top. [Last accessed on 2020 Jan 10]
- [Google Scholar]
- Network of Erasmus Based European Orthodontic Postgraduate Programmes. 2018. Bylaws. Available from: http://www.nebeop.org/content/nebeop/nebeop%20bylaws_vs2018.pdf [Last accessed on 2020 Mar 11]
- [Google Scholar]
- Network of Erasmus Based European Orthodontic Postgraduate Programmes. 2020. Full Members. Available from: http://www.nebeop.org/content/members/fullmembers.asp. [Last accessed on 2020 Mar 12]
- [Google Scholar]
- Resorption of maxillary lateral incisors caused by ectopic eruption of the canines. A clinical and radiographic analysis of predisposing factors. Am J Orthod Dentofacial Orthop. 1988;94:503-13.
- [CrossRef] [Google Scholar]
- Effect of interceptive extraction of deciduous canine on palatally displaced maxillary canine: A prospective randomized controlled study. Angle Orthod. 2013;84:3-10.
- [CrossRef] [PubMed] [Google Scholar]
- Effectiveness of extraction of primary canines for interceptive management of palatally displaced permanent canines: A systematic review and meta-analysis. Eur J Orthod. 2018;40:149-56.
- [CrossRef] [PubMed] [Google Scholar]
- Extraction of primary canines for interceptive orthodontic treatment of palatally displaced permanent canines: A systematic review. Angle Orthod. 2017;87:878-85.
- [CrossRef] [PubMed] [Google Scholar]
- Cases-Clinical audit; scenarios for evaluation and study. Br Dent J. 1997;183:108-11.
- [CrossRef] [PubMed] [Google Scholar]
- No difference in surgical outcomes between open and closed exposure of palatally displaced maxillary canines. J Oral Maxillofac Surg. 2012;70:2026-34.
- [CrossRef] [PubMed] [Google Scholar]
- Glass ionomer cement used as surgical dressing after radical surgical exposure of impacted teeth. Swed Dent J. 1992;16:87-92.
- [Google Scholar]
- The use of panoramic radiographs to decide when interceptive extraction is beneficial in children with palatally displaced canines based on a randomized clinical trial. Eur J Orthod. 2018;40:565-74.
- [CrossRef] [PubMed] [Google Scholar]
- Delayed diagnosis of displaced and impacted canines-a prospective longitudinal study. Acta Odontol Scand. 2020;78:165-72.
- [CrossRef] [PubMed] [Google Scholar]
- Perceptions of orthodontic specialist training in the United Kingdom: A national survey of postgraduate orthodontic student opinion. J Orthod. 2016;43:202-17.
- [CrossRef] [PubMed] [Google Scholar]
- Determining effective follow-up of E-mail surveys. Am J Health Behav. 1997;2:193-6.
- [Google Scholar]
- A survey of postgraduate (specialist) orthodontic education in 23 European countries. J Orthod. 2000;27:92-8.
- [CrossRef] [PubMed] [Google Scholar]
- A survey of perceived problems in orthodontic education in 23 European countries. J Orthod. 2000;27:343-8.
- [CrossRef] [PubMed] [Google Scholar]
- Orthodontic training: The residents' perspective. Am J Orthod Dentofacial Orthop. 1994;106:649-53.
- [CrossRef] [Google Scholar]
- World federation of orthodontists (WFO) guidelines for postgraduate orthodontic education. World J Orthod. 2009;10:153-66.
- [Google Scholar]
Appendix 1: The questionnaire that was sent to the POT programs
Treatment of palatally displaced and impacted canines
In which country and city are you responsible for the specialist training program in orthodontics? Country City University or university clinic. How long is your postgraduate program in orthodontics?…………….years Which interceptive treatment approach do you teach in your program when patients have palatally displaced canine? (Several alternatives may be chosen.) Extraction of the deciduous canine Extraction of the deciduous canine and the first deciduous molar Extraction of the deciduous canine + Extraoral traction Extraction of the deciduous canine + Transpalatal bar Extraction of the deciduous canine + Rapid maxillary expansion Transpalatal bar, only Rapid maxillary expansion, only Extraoral traction, only Do not perform any interceptive treatment Other; if so, what. At what age do you prefer that interceptive treatment is performed? (Several alternatives may be chosen.) ≤9 10–13 13–15 ≥16. Approximately, how many surgical exposures of palatally impacted canines are performed in your dental hospital each year? 0 Reason (no need to reply to the rest of the questionnaire) 1–5 6–10 11–15 16–20 >20. What age is the majority of your patients when they have surgical exposure of the palatally impacted canines? <12 12–15 16–20 20–25 >25. Who performs the surgical exposure? (Several alternatives may be chosen.) The orthodontist The pedodontist The periodontologist The oral (and maxillofacial) surgeon Someone else; in that case, who? Who chooses which technique should be used when exposing the palatally impacted canine? The orthodontist The performing dentist/surgeon The orthodontist in collaboration with the dentist/ surgeon Someone else; in that case, who? Which surgical technique or techniques do you teach in your university/dental hospital when a palatally impacted canine is to be exposed? Open exposure Closed exposure Both techniques depending on the specific case Other technique/s; in that case, which one/ones? Which of these surgical procedures resembles most those that you teach or recommend in your university/ dental hospital when a palatally impacted canine is to be exposed? 1 2 3 4 5 6, please explain your procedure. If you teach the open technique, what are the benefits of that technique compared with other techniques (several alternatives may be chosen). Concerning surgery and post-surgery recovery Less pain during surgery Fewer complications with the surgery Shorter surgical time Faster immediate post-surgery recovery Less reoperation Other; in that case, what? Concerning orthodontic treatment Less pain during active orthodontic treatment Better view of the tooth position and the direction of traction Shorter duration of active orthodontic treatment Easier orthodontic mechanics No lost chain Other; in that case, what? Concerning periodontal health and esthetics after orthodontic treatment. Better periodontal attachment levels Better alveolar bone level Less gingival recession Less difference in crown height between the impacted and the normally erupting side Other; in that case, what? If you teach the closed technique, which are the benefits of that technique compared with other techniques (several alternatives may be chosen). Concerning surgery and post-surgery recovery Less pain during the surgery Fewer complications with the surgery Less risk of mucosa healing and tooth re-impaction Shorter surgical time Faster immediate post-surgery recovery Less reoperation Smaller mucosa defects post-surgery Other; in that case, what? Concerning orthodontic treatment Possibility to distalize immediately after surgery Less pain during active orthodontic treatment Shorter duration of active orthodontic treatment Other; in that case, what? Concerning periodontal health and esthetics after orthodontic treatment. Better periodontal attachment levels Better alveolar bone level Less gingival recession Less difference in crown height between the impacted and the normally erupting side Other; in that case, what? If you teach several surgical techniques, when do you choose one technique over the other; for instance, deeply versus superficially positioned? How do you define and diagnose a deeply positioned palatally impacted canine? How do you define and diagnose a superficially positioned palatally impacted canine? If you teach the open technique, what kind of dressing material do you use to prevent the gingiva from healing and covering the impacted canine? Glass ionomer cement Coe-Pak™ with sutures Coe-Pak™ with cover plate Whitehead’s varnish Surgicel™ Septoplasty™ Bismuth iodoform paraffin paste (BIPP) Zinc oxide eugenol (ZOE) None Other dressing; in that case, which? For how long do you leave the dressing in place? If you teach the open technique, how long time do you allow for the canine to erupt spontaneously before you start active orthodontic treatment? Do not wait for a spontaneous eruption, start treatment at once Approximately 3–6 months >6 months Until the canine can be bonded Other; in that case, what? If you teach the closed technique, do you use:
Gold plated chain Other; in that case, what? Do you have access to, and use CT (computed tomography)/CBCT (cone-beam computed tomography) in connection with palatally impacted canines? Yes No. Which radiographic technique do you teach your postgraduate students to use when making therapy plans for surgical exposure of palatally impacted canines? (Several alternatives may be chosen.) Intraoral radiographs Always Sometimes Never. Panoramic radiographs Always Sometimes Never. CBCT. Always Sometimes Never. In which cases do you teach your postgraduate students to use CT/CBCT in connection with palatally impacted canines?