

Translate this page into:
Comparison of the Changes in Hyoid Bone Position in Subjects with Normodivergent and Hyperdivergent Growth Patterns: A Cephalometric Study
Address for correspondence: Dr. Faisal Arshad, Senior Lecturer, Department of Orthodontics, Rajarajeswari Dental College and Hospital, Bengaluru, India. E-mail: faisalking1335@yahoo. in
This article was originally published by Wolters Kluwer and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Objective
The aim of this study is to test the hypothesis that there is no difference in hyoid bone position among individuals with different growth patterns before and after treatment.
Materials and Methods
Pre- and post-treatment lateral cephalogram of forty Class I adults in the age group of 20–27 years were grouped. All the cases were treated with the first premolar extraction in all quadrants. Based on the growth pattern of the face, individuals were divided into: (1) Group 1 (n = 20): Normodivergent, i.e., FH/MP angle smaller than 30.5° (20 patients). (2) Group 2 (n = 20): Hyperdivergent, i.e., FH/MP angle larger than 30.5° (20 patients). Lateral cephalograms were traced and analyzed manually for evaluation of hyoid bone position. Patients in both groups were treated with preadjusted appliances. Pre- and post-treatment lateral cephalograms were traced, and variables were compared using paired t-test, and the relationship between dentofacial variables, growth pattern, and the hyoid bone position was analyzed using Karl Pearson’s correlation coefficient method. The changes of hyoid position after treatment were compared using t-test.
Results
The data were analyzed by Kolmogorov–Smirnov and paired t-test. Karl Pearson’s correlation coefficient test was performed to determine whether there was an association between the changes of hyoid and growth pattern. Following retraction of incisors, statistically significant correlation was observed in the pre- and post-treatment values of dentofacial structures and hyoid bone, but no significant correlation was found in position of the hyoid bone in the normodivergent and hyperdivergent groups. In both the groups, hyoid bone moved in an inferior and posterior direction after orthodontic treatment.
Conclusion
No change was seen in position of the hyoid bone in normodivergent and hyperdivergent groups.
Keywords
Hyoid bone
hyperdivergent
normodivergent

Introduction
Brodie[1] points out that as man assumed an upright posture, the head had to be balanced on the vertebral column. This was attained by equal anterior and posterior muscle tension relative to the occipital condyles. In the accomplishment of this delicate cranial balance and posture, the hyoid bone plays an important and active part. According to Gray,[2] the omohyoid muscles are concerned, “especially in prolonged inspiratory efforts, since by tensing the lower part of the cervical fascia it lessens the inward suction of the soft parts which would otherwise compress the great vessels and the lung apices.” The importance of the hyoid bone should now be self-evident. Without it, our facility of maintaining an airway, swallowing and preventing regurgitation, and maintaining the upright postural position of the head could not be as well controlled.
In general, considerations of the cervicofacial skeleton, the hyoid bone tends to be overlooked or given scant attention. However, it is a unique structure in man in that, unlike all other bones of the head and neck, it has no bony articulations. There are two major groups of muscles – the suprahyoid and the infrahyoid attached to this bone. These muscles rely on the hyoid bone for their actions and have certain very important functions. The digastric muscles increase the anteroposterior dimension and the oropharynx during deglutition while the posterior belly of the digastric and the stylohyoid muscle act to prevent regurgitation of food after swallowing. The suprahyoid muscles depress the mandible by contracting against a fixed hyoid platform, the absence of which may seriously impair mandibular opening.
Several studies have reported significant relationship between pharyngeal structures and both dentofacial and craniofacial structures.[3,4] Numerous researchers reported the interaction between pharyngeal dimensions and various sagittal and vertical facial growth patterns at varying degrees.[5,6] Skeletal features such as retrusion of the maxilla and mandible and vertical maxillary excess in hyperdivergent patients may lead to narrower anteroposterior dimensions of the airway.[7]
Sagittal facial growth is seen as downward and forward growth.[8,9] A study indicated that vertical growth of condyles is lesser than vertical growth of facial sutures and alveolar processes, resulting in backward mandibular rotation and bite opening. On the contrary, if vertical growth of condyles is greater than vertical growth of facial sutures and molar areas, forward mandibular rotation and bite closing are seen. Therefore, the ultimate vector of mandibular growth is a consequence of the competition between horizontal and vertical growth.[10] An interaction occurs between respiratory function and the maxillary and mandibular growth pattern.[11]
The correlation between hyoid bone position and the vertical growth pattern of the face is controversial. Opdebeeck et al.[12] compared the position of the hyoid bone in individuals with short face and long face syndrome and noted movement of the hyoid bone in concert with movement of the mandible, tongue, pharynx, and cervical spine. Thus, the positions of the hyoid bone and the tongue can be considered as indicators of pharyngeal airway passage. Hence, it is necessary to determine whether any difference is evident in the hyoid bone position among patients with different growth patterns. To investigate this assumption, the main aim of this study was to compare changes in position of the hyoid bone in healthy Class I individuals with two different growth patterns (Group I: Normodivergent and Group II: Hyperdivergent). For this purpose, the null hypothesis assumed was that no significant differences were present in the hyoid bone position of Class I individuals with different growth patterns. Furthermore, the pre- and post-treatment dentofacial parameters in normodivergent and hyperdivergent group were compared.
Materials and Methods
Pre- and post-treatment lateral cephalogram: of forty, Class I adults in age group of 20–27 years were grouped. All the cases were treated with the first premolar extractions in all quadrants. Based on the growth pattern of the face, patients were divided into:
Group I (n = 20): Normodivergent, i.e., FH/MP angle smaller than 30.5°
Group II (n = 20): Hyperdivergent, i.e., FH/MP angle larger than 30.5°.
Pre- and post-lateral cephalograms were traced and analyzed manually for evaluation of hyoid bone position and variables were compared. Individuals in both groups were treated with preadjusted appliances. The inclusion criteria included: Skeletal Class I, Class I molar, canine, and premolar relationship; well-aligned arches with no or minimal crowding; increased UL-E line, LL-E line, U1/SN, and L1/M P value greater than standard deviation (SD) above the mean. Maximum anchorage and maximal retraction of anterior teeth, no obvious hyperplasia of tonsils or adenoids on cephalograms, no history of previous orthodontic/orthopedic treatment or any cleft lip/palate, patients with chronic mouth breathing, permanent snoring and tonsillectomy, or adenoidectomy were excluded from the study.
All patients were treated with 0.022 × 0.028 inch preadjusted appliances. All pre- and post-treatment cephalograms were taken from the same machine by the same operator. Hyoid bone position was evaluated. The cephalometric landmarks and analyses [Table 1 and Figures 1, 2] were based on the methods described previously by Lowe et al.,[13] Liu et al.,[14] and Zhong et al.[15] Two serial cephalograms from each individual were traced by the same investigator.
| Variable | Defnition |
|---|---|
| Landmarks | |
| C3 | The most anteroinferior point of the third vertebra |
| H | The most superior and anterior point of hyoid bone |
| RGN | The most protrusive point of retrognathion |
| H1 | Foot point of perpendicular line from RGN to C3 |
| Hyoid position | |
| HRGN, mm | Distance between H and RGN |
| HH1, mm | Distance between H and H1 |
| C3H, mm | Distance between C3 and H |
| SH, mm | Distance between S and H |
| Dentofacial measurements | |
| ANB, degrees | Angle between point A and B at nasion |
| FH/MP, degrees | Angle between the mandibular plane and the FH plane |
| U1/FH, degrees | Angle between the FH plane and long axis of upper incisors |
| L1/MP, degrees | Angle between the mandibular plane and long axis of lower incisors |
| UL-E line, mm | Horizontal distance from the most protrusive point of upper lip to E line |
| LL-E line, mm | Horizontal distance from the most protrusive point of lower lip to E line |
| U1FHp, mm | Horizontal distance from the tip of the upper incisor crown to constructed FH plane vertical |
| L1FHp, mm | Horizontal distance from the tip of the lower incisor crown to constructed FH plane vertical |
| U6FHp, mm | Horizontal distance from the distal point of the upper first molar crown to constructed FH plane vertical |
| L6FHp, mm | Horizontal distance from the distal point of the lower first molar crown to constructed FH plane vertical |
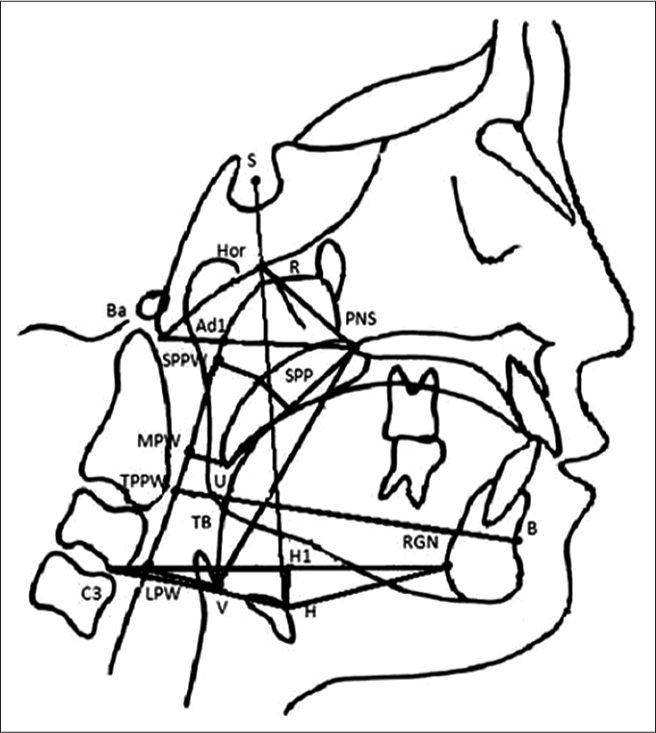
- The cephalometric landmarks and analyses of pharyngeal airway

- The cephalometric landmarks and analyses of dentofacial complex
Statistical analysis
All statistical analyses were performed with software package SPSS (for Windows 7, version 16.0, SPSS). Data were expressed as the mean and SD. Kolmogorov–Smirnov test was applied to pre- and post-operative measurements and showed a normally distributed population. Therefore, pre- versus post-treatment values were analyzed with paired t-test. The changes of hyoid position before and after treatment were compared using Kolmogorov–Smirnov and paired t-test. Karl Pearson’s correlation coefficient test was performed to determine whether there was an association between the changes of hyoid measurements and those of dentofacial structures.
Results
No statistically significant differences were observed in the retraction distance of the upper and lower lips and the tip of upper and lower incisor, ANB angle, FH/MP angle, and the hyoid bone position between the normodivergent and hyperdivergent groups after the treatment as shown in Table 2. However, Tables 2 and 3, Graph 1 and 2 show statistically significant changes in the pre and post operative values of Groups I and II for dentofacial parameters and change in position of hyoid bone respectively. Table 4 and Graph 3 show the pre and post treatment changes in the dentofacial parameters. After treatment, the hyoid bone tends to move in a posterior and inferior direction in both Groups (I and II), respectively. Table 5 and Graph 4 show the changes of the hyoid bone position after the treatment. The results displayed a significant decrease in C3H (P < 0.001) and SH (P < 0.001) whereas changes in HRGN and HH1 showed no significant differences. However, no significant changes in the position of hyoid bone were seen when both the groups were compared to each other.
| Variables | Group | Group I Normodivergent (n=20) | Group II Hyperdivergent (n=20) | t | P | ||
|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | ||||
| ANB (°) | 0.41 | 0.09 | 0.39 | 0.09 | 0.5108 | 0.6157 | |
| FH/MP (°) | 0.80 | 0.28 | 0.56 | 0.20 | 2.1868 | 0.0422* | |
| U1/FH (°) | 15.34 | 0.59 | 15.56 | 1.28 | −0.4929 | 0.6280 | |
| L1/MP (°) | 4.99 | 0.73 | 5.45 | 0.90 | −1.2528 | 0.2263 | |
| UL-E line (mm) | 3.33 | 1.10 | 3.36 | 0.98 | −0.0622 | 0.9511 | |
| LL-E line (mm) | 3.28 | 0.47 | 2.96 | 0.56 | 1.3915 | 0.1810 | |
| U1FHp (mm) | 6.20 | 0.48 | 5.93 | 0.81 | 0.9078 | 0.3760 | |
| L1FHp (mm) | 5.07 | 0.95 | 4.68 | 1.72 | 0.6281 | 0.5378 | |
| U6FHp (mm) | 0.98 | 0.54 | 1.12 | 0.42 | −0.6441 | 0.5276 | |
| L6FHp (mm) | 0.42 | 0.40 | 0.51 | 0.22 | −0.6286 | 0.5375 | |
*P<0.05. SD – Standard deviation
| Variables | Time points | Group I (n=20) | Group II (n=20) | t | P | ||
|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | ||||
| HRGN (mm) | Changes | 0.41 | 0.18 | 0.33 | 0.15 | 1.0639 | 0.3015 |
| C3H (mm) | Changes | 0.86 | 0.38 | 1.18 | 0.83 | −1.1070 | 0.2829 |
| HH1 (mm) | hanges | 0.35 | 0.11 | 0.30 | 0.30 | 0.4986 | 0.6241 |
| SH (mm) | Changes | 0.76 | 0.46 | 0.54 | 0.28 | 1.2924 | 0.2126 |
SD – Standard deviation
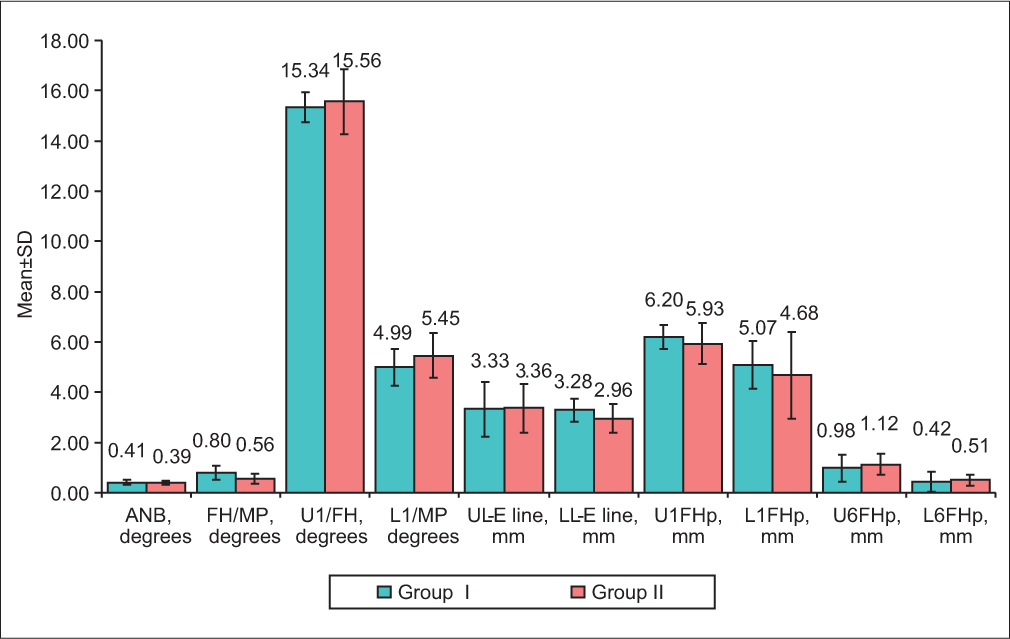
- Comparison of the changes in dentofacial parameters preoperatively and postoperatively in Groups I and II
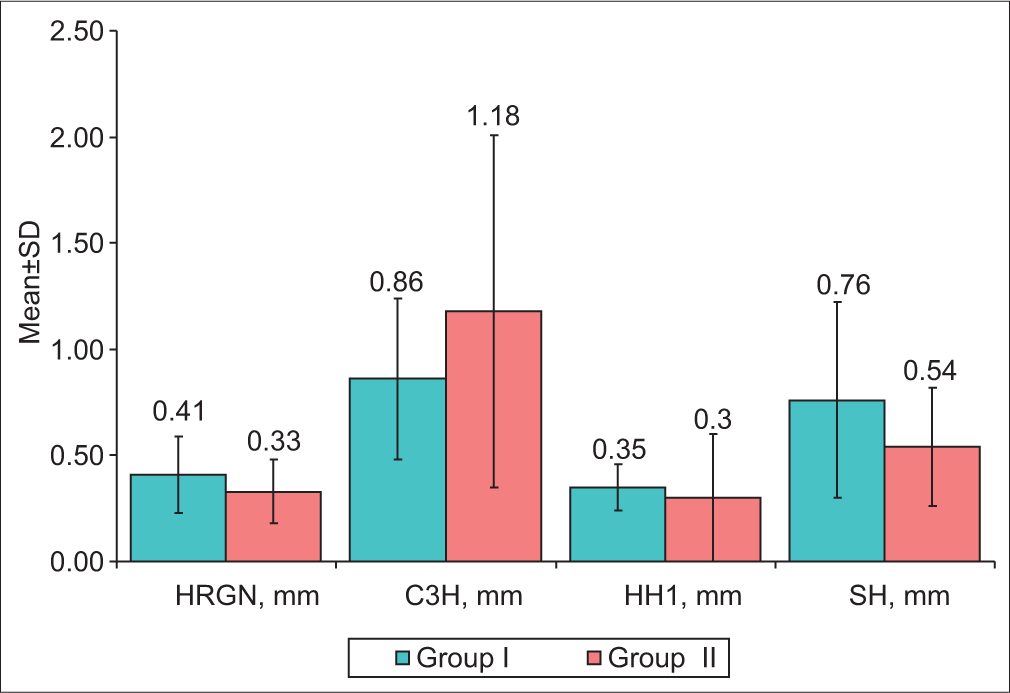
- Comparison of the changes in position of hyoid bone preoperatively and postoperatively in Groups I and II
| Variables | Time | Mean | SD | Mean difference | SD difference | Percentage of change | Paired t | P |
|---|---|---|---|---|---|---|---|---|
| ANB (°) | Pretreatment | 3.82 | 0.69 | −0.40 | 0.09 | −10.47 | −20.8395 | <0.001 |
| Posttreatment | 4.22 | 0.67 | ||||||
| FH/MP (°) | Pretreatment | 34.19 | 2.93 | −0.68 | 0.27 | −1.99 | −11.3168 | <0.001 |
| Posttreatment | 34.87 | 2.98 | ||||||
| U1/FH (°) | Pretreatment | 120.70 | 2.84 | 15.45 | 0.98 | 12.80 | 70.6550 | <0.001 |
| Posttreatment | 105.25 | 2.75 | ||||||
| L1/MP (°) | Pretreatment | 97.42 | 3.41 | 5.22 | 0.83 | 5.36 | 28.0161 | <0.001 |
| Posttreatment | 92.20 | 3.49 | ||||||
| UL-E line (mm) | Pretreatment | 2.76 | 0.74 | 3.35 | 1.02 | 121.47 | 14.7399 | <0.001 |
| Posttreatment | −0.59 | 0.46 | ||||||
| LL-E line (mm) | Pretreatment | 5.70 | 1.13 | 3.12 | 0.53 | 54.74 | 26.4886 | <0.001 |
| Posttreatment | 2.58 | 1.30 | ||||||
| U1FHp (mm) | Pretreatment | 72.02 | 3.00 | 6.07 | 0.66 | 8.42 | 40.9749 | <0.001 |
| Posttreatment | 65.95 | 3.07 | ||||||
| L1FHp (mm) | Pretreatment | 67.83 | 2.51 | 4.88 | 1.37 | 7.19 | 15.9592 | <0.001 |
| Posttreatment | 62.96 | 2.57 | ||||||
| U6FHp (mm) | Pretreatment | 31.46 | 1.43 | −1.05 | 0.48 | −3.34 | −9.8138 | <0.001 |
| Posttreatment | 32.51 | 1.43 | ||||||
| L6FHp (mm) | Pretreatment | 32.34 | 2.41 | −0.46 | 0.32 | −1.44 | −6.6013 | <0.001 |
| Posttreatment | 32.81 | 2.35 |
SD – Standard deviation
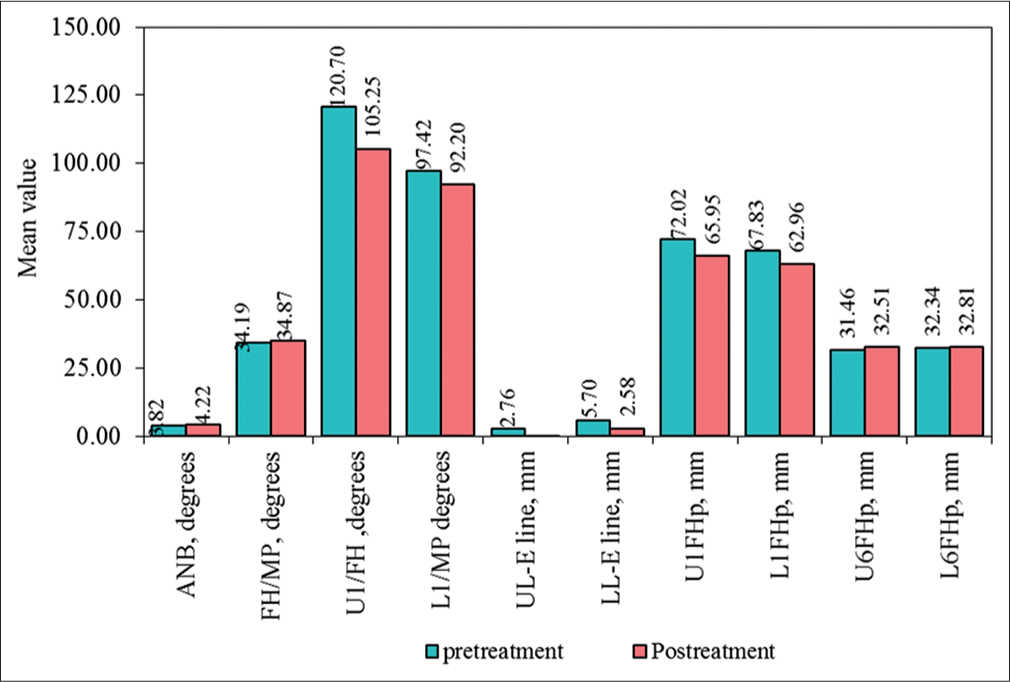
- Comparison of changes in pre- and post-treatment values of dentofacial parameters
| Variables | Time | Mean | SD | Mean difference | SD difference | Percentage of change | Paired t | P |
|---|---|---|---|---|---|---|---|---|
| HRGN (mm) | Pretreatment | 33.81 | 3.16 | −0.37 | 0.17 | −1.09 | −9.9174 | <0.001 |
| Posttreatment | 34.17 | 3.15 | ||||||
| C3H (mm) | Pretreatment | 32.69 | 1.38 | 1.02 | 0.65 | 3.12 | 7.0158 | <0.001 |
| Posttreatment | 31.67 | 1.42 | ||||||
| HH1 (mm) | Pretreatment | 4.14 | 1.37 | −0.33 | 0.22 | −7.85 | −6.6141 | <0.001 |
| Posttreatment | 4.47 | 1.33 | ||||||
| SH (mm) | Pretreatment | 98.40 | 3.34 | −0.65 | 0.39 | −0.66 | −7.5056 | <0.001 |
| Posttreatment | 99.05 | 3.18 |
SD – Standard deviation

- Comparison of the changes in pre- and post-treatment values of hyoid bone position
Discussion
Precise measurement of hyoid position by cephalometric means is considered difficult. Graber[16] states that slight variations in head position in the cephalostat, the postural position of the spine, and the state of function; all affect the position of the hyoid bone. However, he points out that within these limitations, definite conclusions concerning the normal hyoid position may be made. Stepovich[17] reports that when roentgenograms of the same person were taken at different time intervals; the hyoid bone was found to be positioned differently in each film. Ingervall et al.[18] believe that Stepovich exaggerates the lack of precision in recording the hyoid bone position, although they admit that the hyoid position will vary even under standard conditions. King[19] noted that the changes in head position lead to changes in the position of the hyoid bone in the same person. If the head is extended back, then the hyoid bone moves back; if the head is tipped forward, then the hyoid bone moves forward. Grant[20] studied the position of the hyoid bone in Class I, II, and III malocclusions. He concludes that the hyoid bone position is constant in all three classes and that the position of the hyoid bone is determined by the musculature and not by the occlusion of the teeth.
The possibility of some tie-up between the hyoid bone position and mandibular morphology led to a consideration of skeletal types which, according to Graber[16] and gives disparate results since some of the investigations find positive correlations between hyoid bone position and skeletal type while others find no correlation at all.[21]
In the present study, there was no significant difference found in the position of the hyoid bone in individuals with normodivergent and hyperdivergent growth patterns. In both groups, the hyoid bone is displaced in posterior and inferior direction. However, Haralabakis et al.[22] also found no difference in anteroposterior position of the hyoid bone in adult individuals with anterior open bite compared with individuals with normal bite when its position was evaluated from near reference structures such as the cervical spine, pharynx, and mandibular plane. This observation supported the concept that the hyoid bone moved in conjunction with adjacent anatomic structures when rotating backward in patients with long face syndrome. However, the previous study done by Opdebeeck et al.[12] also showed no significant difference in the anteroposterior position of the hyoid bone in individuals with different vertical jaw dysplasias when its position was evaluated from very near reference planes.
The hyoid position depends on the relative balance of muscle attachment from the base of the cranium bilaterally and the region of the mandibular symphysis. The inferior movement of the hyoid bone seen in the present study is consistent with the findings of other studies,[17,18] showing that this movement is an adaptation preventing an encroachment of the tongue into the pharyngeal airway.
The limitation of the current study is that two-dimensional imaging was used to evaluate three dimensional structures. However, there is a high correlation between lateral radiographs and three-dimensional magnetic resonance imaging scans.[23] Moreover, Miles et al.[24] reported a high reliability of cephalometric landmarks and measurements. Thus, cephalograms are still widely used. The other limitation of the present study was that the gender of the patient was not taken into consideration. Further studies should be aimed at long-term effects of orthodontic treatment on hyoid bone position with three-dimensional imaging.
Conclusion
The values of the dentofacial parameters and hyoid bone position showed no difference between the normodivergent (Group I) and hyperdivergent (Group II). However, in each group, the hyoid bone tends to move in a posterior and inferior direction.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Anatomy and physiology of head and neck musculature. Am J Orthod. 1950;36:831-44.
- [CrossRef] [Google Scholar]
- Anatomy, Descriptive and Applied. London: Longmans, Green & Company; 1977.
- A longitudinal study of the development of the posterior nasopharyngeal wall between 3 and 16 years of age. Eur J Orthod. 1983;5:47-58.
- [CrossRef] [PubMed] [Google Scholar]
- A study on the pharyngeal size in different skeletal patterns. Am J Orthod Dentofacial Orthop. 1995;108:69-75.
- [Google Scholar]
- Upper airway dimensions in Class II malocclusion. Effects of headgear treatment. Angle Orthod. 2007;77:1046-53.
- [Google Scholar]
- The long face syndrome and impairment of the nasopharyngeal airway. Angle Orthod. 1990;60:167-76.
- [Google Scholar]
- A cephalometric comparative study of the soft tissue airway dimensions in persons with hyperdivergent and normodivergent facial patterns. J Oral Maxillofac Surg. 1998;56:135-9.
- [Google Scholar]
- Inhibition or stimulation of the vertical growth of the facial complex, its significance to treatment. Angle Orthod. 1967;37:285-97.
- [Google Scholar]
- Extreme variation in vertical facial growth and associated variation in skeletal and dental relations. Angle Orthod. 1971;41:219-29.
- [Google Scholar]
- Craniofacial growth in untreated skeletal Class I subjects with low, average, and high MP-SN angles: A longitudinal study. Am J Orthod Dentofacial Orthop. 2003;124:670-8.
- [CrossRef] [PubMed] [Google Scholar]
- Sagittal mandibular development effects on the dimensions of the awake pharyngeal airway passage. Angle Orthod. 2010;80:1061-7.
- [CrossRef] [PubMed] [Google Scholar]
- Comparative study between the SFS and LFS rotation as a possible morphogenic mechanism. Am J Orthod. 1978;74:509-21.
- [CrossRef] [Google Scholar]
- Cephalometric comparisons of craniofacial and upper airway structure by skeletal subtype and gender in patients with obstructive sleep apnea. Am J Orthod Dentofacial Orthop. 1996;110:653-64.
- [Google Scholar]
- Effects of a mandibular repositioner on obstructive sleep apnea. Am J Orthod Dentofacial Orthop. 2000;118:248-56.
- [Google Scholar]
- A comparison study of upper airway among different skeletal craniofacial patterns in nonsnoring Chinese children. Angle Orthod. 2010;80:267-74.
- [CrossRef] [PubMed] [Google Scholar]
- Hyoid changes following orthopedic treatment of mandibular prognathism. Angle Orthod. 1978;48:33-8.
- [Google Scholar]
- A cephalometric positional study of the hyoid bone. Am J Orthod. 1965;51:882-900.
- [CrossRef] [Google Scholar]
- Change in location of hyoid bone with mandibular positions. Acta Odontol Scand. 1970;28:337-61.
- [Google Scholar]
- A roentgenographic study of pharyngeal growth. Angle Orthod. 1952;22:23.
- [CrossRef] [Google Scholar]
- A Radiographic Study of Hyoid Bone Position in Angle’s Class I, II, and Ill Malocclusions. Master’s Thesis thesis
- [Google Scholar]
- The hyoid bone position in adult individuals with open bite and normal occlusion. Eur J Orthod. 1993;15:265-71.
- [CrossRef] [Google Scholar]
- Validity of upper airway assessment in children: A clinical, cephalometric, and MRI study. Angle Orthod. 2011;81:433-9.
- [Google Scholar]
- The reliability of upper airway landmark identification. Aust Orthod J. 1995;14:3-6.
- [Google Scholar]




