

Translate this page into:
An innovative approach for correction of pseudo class III malocclusion with the use of “Planas direct tracks”
Address for correspondence: Dr. Ketan Vora, Vora Dental Clinic and Orthodontic Centre, 567/4A, Shivam Apartment, Near Zala Complex, Bibwewadi-Kondhwa Road, Pune - 411 037, Maharashtra, India. E-mail: drk10vora@gmail.com
How to cite this article: Vora KS, Misal A, Toshniwal NG. An innovative approach for correction of pseudo class III malocclusion with the use of “Planas direct tracks”. APOS Trends Orthod 2013;3:190-6.
Abstract
Anterior cross bite due to a pseudo Class III is a kind of malocclusion, which has a potential to turn into a facial deformity. This orthodontic emergency should be treated as soon as it is observed. A case of pseudo Class III was treated with Planas direct tracks (PDT). The PDT was designed such that the distal incline of the upper block occludes with mesial incline of the lower block such that the mandible will have a posterior path of closure with condyles in centric relation. Significant clinical change was seen in the subject. There was a significant reduction in mesial step and a considerable improvement in the facial profile. Cephalometrically, there was a significant increase seen in the lower anterior facial height. PDT is an efficient solution for the correction of early pseudo Class III malocclusion.
Keywords
Anterior cross bite
Planas direct tracks
pseudo Class III malocclusion

INTRODUCTION
The fundamentals of biology, growth and development supported by current research dictate that most of the malocclusions and facial deformities begin mild in nature and become severe as age advances. The understanding of this developing deformity or malocclusion is crucial for the clinician involved in early orthodontic treatment. The capability of cells, tissues and organs to adapt through normal growth processes is greatest, early in development and diminishes as maturation progresses.[1]
Several studies[2,3] have revealed that anterior cross bite if not treated has a functional appliance like effect causing excess growth of the mandible, restricting the growth of the maxilla. Changing the path of closure by forcing the patient to function with the mandible forced backwards and condyles in centric relation (CR) could correct the anterior cross bite problems. Literature reveals many different appliances and philosophies, including the use of Planas direct tracks (PDT) by Pedro Planas of Spain in the year 1971.[4] According to Planas, “Cross bites are very easy to correct, whenever diagnosed early. If not treated, they can produce severe difficulties in the future, due to skeletal modifications that may occur and might be irreversible.”
PDT are prism shaped blocks incorporating inclined planes made up of composite resin directly built or cemented on the occlusal surfaces of deciduous molars. The PDT are designed such that the distal incline of the upper block occlude with the mesial incline of the lower block such that the mandible will have a posterior path of closure with condyles in CR.[5]
In this case, we have used photo activated composite resin (3M™ ESPE™ Filtek™ P60 Posterior Restorative System), which is easily bonded to primary teeth. There is no specific indication for particular composite resin brand, but it must have some resistance to withstand occlusal forces during the swallowing and mastication.
CASE REPORT
This is a case report of a 4-year-old female patient who reported to the dental clinic with the chief complaint of malaligned teeth. On clinical examination, it was observed that:
The facial profile of the patient was concave suggesting anterior divergence. [Figures 1 and 2]
Patient had anterior cross-bite and mesial step not more than 3 mm [Figures 3-5].
Patient was able to position her mandible in edge-to- edge bite suggesting of centric occlusion-CR (CO-CR) deviation.
The growth pattern of the patient was horizontal.
Patient was having healthy or properly restored set of teeth and almost well-aligned individual dental arches.
There was no transverse problem or any skeletal discrepancy in the maxillary arch.
No family history of mandibular prognathism.
Patient had not undergone any orthodontic treatment before.
Patient was free from temporomandibular joint dysfunction disorders.

- Pre-treatment lateral view

- Pre-treatment front view

- Pre-treatment intra-oral front view

- Pre-treatment intra-oral right lateral view

- Pre-treatment intra-oral left lateral view
Pre-treatment cephalometric analysis revealed decreased or negative ANB angle.
Treatment objective
To correct the CO-CR shift by guiding the mandible in a downward and backward position, increase the lower facial height.
Treatment alternatives
Some appliances like tongue blade therapy achieve the above stated objective by correcting the incisal inclinations of upper and lower teeth. Whereas, other appliances correct the cross bite by opening the bite e.g. reverse Twin Block appliance.
Most of these traditional appliances are removable in nature; with some exerting excess force, while others require banding of molars that greatly increases the chair side time, visits and treatment cost. Very few of the appliances that are used today for early treatment of anterior cross bite or pseudo Class III solve both problems: That of compliance and increased treatment cost at the same time. PDT was selected keeping into consideration all these factors.
Protocol followed
Pre-treatment study models, one in CO, i.e., habitual occlusion and the second in CR with the help of wax bite showing that there was CO-CR shift present along with cephalograms were taken.
Patient was immediately taken up for placement of PDT in the oral cavity by indirect method.
Indirect technique for fabrication of PDT
Bite registration
Construction bite was recorded in the most retruded position possible. The bite was slightly opened creating 2 mm of interincisal space. Bite registration was based on Planas minimum vertical dimension law,[4] which states that when mandible moves to achieve maximum intercuspal position it always does so by approximating the mandible and maxilla as much as possible.
Fabrication of tracks made in dental plaster on the articulator
The working models of the patient along with the registered wax bite were mounted on a three point articulator. Tracks resembling the PDT to be placed intra-orally were fabricated using dental plaster on the occlusal surfaces of the second deciduous molars of the models mounted on the articulator. The height of these tracks was adjusted in accordance with the vertical clearance obtained through the construction bite. The width was kept equal to the buccolingual width of the molar.
The tracks for the maxillary arch were made with the apex roughly lying straight above the mesial marginal ridge of the maxillary second deciduous molars. The inclines of the tracks slope downwards toward the distal side where it meets the tooth at its distal marginal ridge.
The tracks for the mandibular arch were made with the apex roughly lying straight above the distal marginal ridge of the mandibular second deciduous molars. The inclines of the tracks slope downwards toward the mesial side where it meets the tooth at its mesial marginal ridge [Figures 6-8].

- Intra-oral front view with Planas direct tracks

- Right lateral view with Planas direct tracks

- Left lateral view with Planas direct tracks
Once the plaster tracks are formed, the vacuum formed clear templates were formed using a 0.5 mm thick clear acrylic sheet Copyplast (SCHEU-Dental, Burgberg, Germany. This clear acrylic mold later served as a template for intraoral placement of the PDT using a high load bearing posterior composite resin 3M™ ESPE™ Filtek™ P60 Posterior Restorative System:
Treatment progress
Progress of the treatment was analyzed after 6 months by
Assessment of pre- and post-treatment study models
Assessment of pre- and post-treatment lateral cephalograms (Figures 9-11)
Assessment of pre- and post-treatment intra oral and extra oral photographs [Figures 1-5 and 12-16].
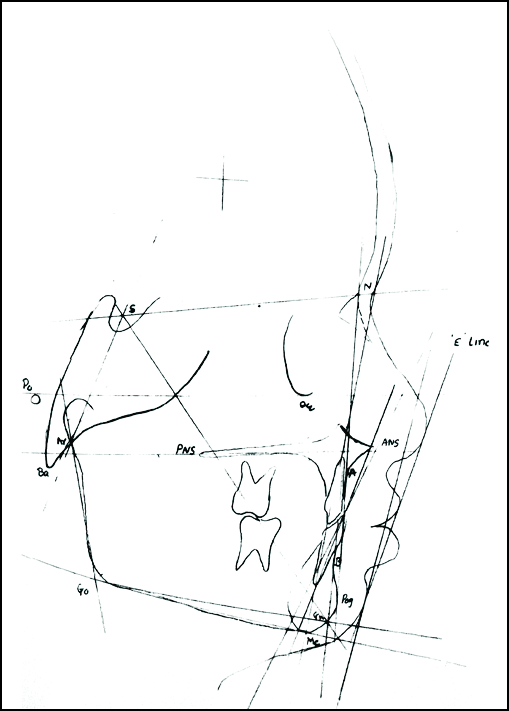
- Pre-treatment cephalometric tracing
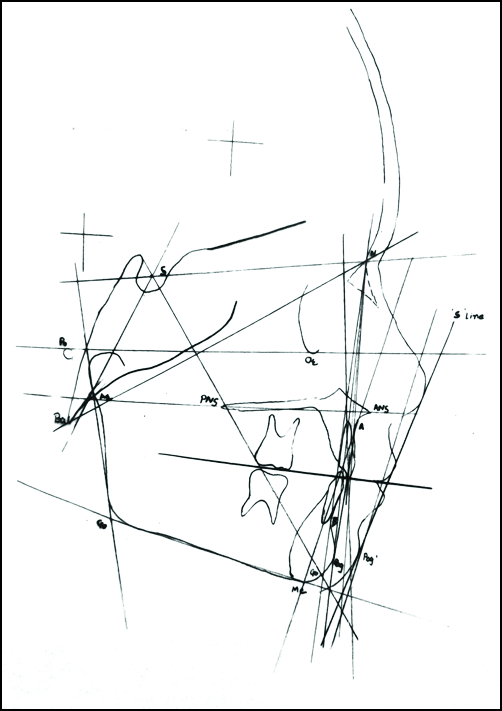
- Post-treatment cephalometric tracing
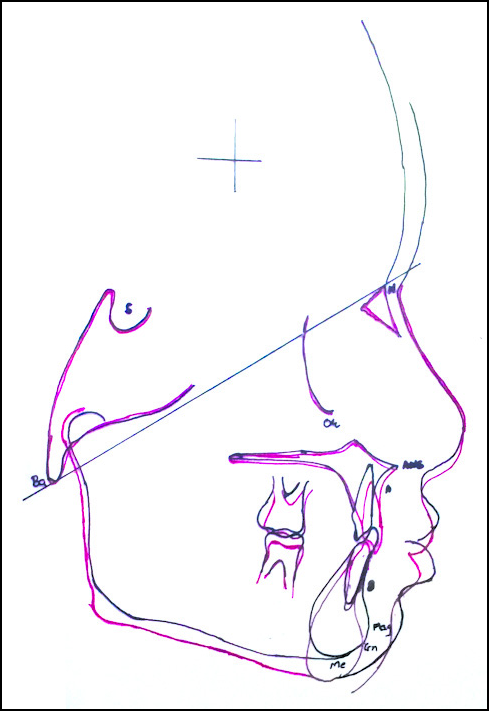
- Superimposition

- Post-treatment front view

- Post-treatment lateral view

- Post-treatment intra-oral front view

- Post-treatment intra-oral right lateral view

- Post-treatment intra-oral left lateral view
Treatment results
Assessment of pre and post study model
It was observed that, after 6 months, there was a significant decrease in the negative overjet. There was slight decrease in overbite. The linear distance of the mesial step of deciduous second molar was also decreased during the course of the treatment [Table 1].
| No. | 0 months | 6 months | ||||||
|---|---|---|---|---|---|---|---|---|
| Overjet | Overbite | Terminal plane (mesial) | Overjet | Overbite | Terminal plane (mesial) | |||
| Rt. | Lt. | Rt. | Lt. | |||||
| 1 | −2 | 2 | 3 | 3 | 2 | 1 | 1 | 2 |
Assessment of pre- and post-treatment cephalograms
During the course of treatment, there was a decrease in SNB angle. There was an increase in both the anterior and posterior facial height. The values of mandibular plane and Y axis were also increased. There was a slight increase in saddle angle, articular angle and gonial angle. The value of the upper incisor to SN was also increased over a period of 6 months. The value of lower incisor to mandibular plane angle was decreased. The linear distance of upper lip to S line was slightly increased. The linear distance of the lower lip to S line was increased significantly [Table 2].
| Cephalometric parameters | Pre-treatment | Post-treatment |
|---|---|---|
| A-P skeletal measurement | ||
| SNA | 82 | 82 |
| SNB | 81.5 | 79 |
| ANB | 0.5 | 3 |
| SN-Pog | 82 | 80 |
| Vertical skeletal measurement | ||
| N-Me | 90 | 94 |
| S-Go | 68 | 69 |
| SN-Go-Gn | 22 | 25 |
| Y-Axis | 57 | 60 |
| Cranial base measurement | ||
| N-S-Ar | 118 | 119 |
| S-Ar-Go | 145 | 147 |
| Ar-Go-Me | 115 | 116 |
| Incisor measurement | ||
| U1-SN | 75 | 85 |
| U1-Nper | −4 | 2 |
| L1-A-Pog | 0 | 2 |
| L1-Go-Gn | 98 | 93 |
| Soft tissue measurement | ||
| Relation of upper lip to E line | −2 | −2 |
| Relation of lower lip to E line | −6 | −2 |
DISCUSSION
There is always a very strong skeletal component in anterior cross-bites. Vast majority of 10-year-old patients with Class III malocclusions grow that way through time from “pseudo” 3-year-old occlusions.[6] This strengthens the argument toward early treatment of a full anterior crossbite.[6]
The pattern of development in each facial form is established at a very early age, even before the eruption of the first permanent molars and long before the adolescent growth spurt.[7]
Pseudo Class III is one such anomaly which deviates the growth pattern of both the maxilla and mandible. There is a definite discrepancy in CR and CO. As the PDT is based on philosophy of the inclined plane, it corrects the CO-CR shift by guiding the mandible in a downward and backward position and is indicated in late primary and early mixed dentition.
There are many appliances which can correct the cross-bite. Some correct it by change in the inclination of upper and lower incisors such as tongue blade, whereas the other appliances correct cross bite by opening the bite. E.g. reverse twin block.[8-16]
These traditional appliances are bulky, exert excess pressure and require patient compliance. Keeping this in mind, PDT was selected because of its compliance, simplicity and ability to provide long-term retention, which is very essential in the treatment of Class III malocclusion. All the diagnostic records were taken and maintained, after taking consent [Figure 17].

- Patient consent
Vertical skeletal changes
Increase in anterior facial height was due to supra eruption of teeth anterior to the deciduous second molars. Mandibular plane angle and Y axis were slightly increased due to downward and backward rotation of mandible. Therefore, patients with the horizontal growth pattern should be selected with the minimal bite opening during bite registration. Furthermore, the PDT with less steep inclined planes should be fabricated and hence that the increase in the vertical dimension of the face height can be kept minimum and in control.
Dentoalveolar change
The angular measurement between upper incisors and SN plane was increased. The linear measurement of upper incisors from N.Pog line was also increased. This change is due to release of crossbite and tongue pressure [Table 2].
The change in linear distance from the upper lip to S line over a period of 6 months indicates that there is not much skeletal and dental change in the maxillary arch (but the dental changes in terms of maxillary incisor proclination was compensated by downward and backward rotation of mandible).
The linear distance from the lower lip to S line reduced, which indicates drastic change in the lower lip posture along with skeletal and dental changes in the mandible.
After evaluating all these values, it can be stated that the net increase in ANB angle or correction of anterior cross bite was due to backward and downward position of mandible and increase in inclination of maxillary incisors and decrease in inclination of mandibular incisors thus relieving displacement of mandible due to premature contact of upper and lower incisors.
The main objective of pseudo Class III treatment is a correction of CO-CR shift. From the superimposition at Ba-N plane it can be concluded that slight backward and upward shift of condylar head has taken place [Figure 11].
As the PDT is glued on occlusal surfaces of deciduous molars they even work during the functional movements such as mastication, swallowing etc. These functional movements act as bio-mechanic stimulus, which may influence the shape, size and proportion of masticatory bones. As the tracks are bonded on to deciduous second molars, they can be retained in place until molar exfoliation, providing long-term retention. In this case, the blocks were removed to see the changes and these blocks were again placed. These will be left there until the exfoliation of deciduous second molars, thus it will provide dual retention by guiding the path of closure as well as the positive overjet will also help in retention.
However, there are certain limitations for the use of PDTs. They are not suitable for patients with vertical growth pattern. Furthermore their use requires healthy set of deciduous dentition.
CONCLUSION
PDT is efficient in correcting anterior crossbite in pseudo Class III malocclusion at an early age. Long-term studies with more number of patients are needed to observe the effect of Tracks on the bone morphology and soft-tissue. Sometimes it becomes necessary to complement PDT action with myotherapy to improve the lip, cheek and facial muscle activity. Further studies involving symptomatologic, gnathostatic diagnosis for case evaluation is advised.
Source of Support:
Nil.
Conflict of Interest:
None declared.
References
- Biological rationale for early treatment of dentofacial deformities. Am J Orthod Dentofacial Orthop. 2002;121:554-8.
- [Google Scholar]
- Treatment of anterior crossbite caused by occlusal interferences. Quintessence Int Dent Dig. 1979;10:57-60.
- [Google Scholar]
- Rehabilitation Neuro Occlusal (RNO). Spain: Masson- Salvat Odontologia Barcelona; 1994.
- Selective grinding and Planas’ direct tracks as a source of prevention. J Pedod. 1981;5:298-314.
- [Google Scholar]
- Anterior crossbite correction in the early deciduous dentition. Am J Orthod Dentofacial Orthop. 1992;102:160-2.
- [Google Scholar]
- Patterns of vertical growth in the face. Am J Orthod Dentofacial Orthop. 1988;93:103-16.
- [Google Scholar]
- Treatment effect of combined maxillary protraction and chincap appliance in severe skeletal Class III cases. Am J Orthod Dentofacial Orthop. 1987;92:304-12.
- [Google Scholar]
- The effect of chin cup therapy on the growth and development of the cranial base and midface. Am J Orthod Dentofacial Orthop. 1986;90:475-83.
- [Google Scholar]
- Early treatment of Class III incisor relationship using the chincap appliance. Eur J Orthod. 1993;15:371-6.
- [Google Scholar]
- Long-term effects of chincap therapy on skeletal profile in mandibular prognathism. Am J Orthod Dentofacial Orthop. 1990;98:127-33.
- [Google Scholar]
- A possibility for physiologic orthodontic movement. Am J Orthod Oral Surg. 1944;30:227-328.:345-328.
- [Google Scholar]
- Palatal expansion: Just the beginning of dentofacial orthopedics. Am J Orthod. 1970;57:219-55.
- [Google Scholar]
- Biomechanical and clinical considerations of a modified protraction headgear. Am J Orthod. 1980;78:125-39.
- [Google Scholar]
- An orthopedic approach to the treatment of Class III malocclusion in young patients. J Clin Orthod. 1987;21:598-608.
- [Google Scholar]
- Orthopedic correction of Class III malocclusion with palatal expansion and custom protraction headgear. J Clin Orthod. 1988;22:314-25.
- [Google Scholar]




