

Translate this page into:
The bite-type malocclusion classification – An extended Angle-method. Is the new classification reliable?

*Corresponding author: Hans Pancherz, Dresdener Str. 5a, Wettenberg -35435, Hessen, Germany. h.pancherz@hotmail.de
-
Received: ,
Accepted: ,
How to cite this article: Pancherz H, Bondemark L. The bite-type malocclusion classification – An extended Angle-method. Is the new classification reliable? APOS Trends Orthod 2021;11(2):100-5.
Abstract
Objectives:
As part in appraising the usefulness of the new bite-type method, a reliability assessment of the classification system was performed.
Materials and Methods:
Eighty-five selected dental casts were appraised by six operators and compared to a “Gold Standard.” The reliability of the bite-type method was assessed by double registrations of each of the nine bite-type classes by every operator.
Results:
An overall acceptable bite-type classification of all examiners existed. Correct assessments were found in 75–90% of the dental casts. Thus, the bite-type classification is a reliable method for categorizing sagittal malocclusions.
Conclusion:
The procedure could favorably replace the angle classification as it is more precise and detailed, without losing the strength of the basic angle system as an uncomplicated communication tool.
Keywords
Bite-type malocclusion classification
Angle classification
Reliability assessment

INTRODUCTION
The angle classification of sagittal malocclusions was introduced in orthodontics by Edward Angle in 1899[1] and modified in 1900[2] and 1907.[3] The angle classification [Figure 1] is worldwide the most well-known system for the assessment of sagittal malocclusions. The method has been the standard for more than 100 years.

- The angle classification.
The great advantage of the procedure is that it is easy to use and facilitates the communication between orthodontists as well as between teachers and students.
The disadvantage of the angle method is that the relation of the front-teeth is considered only in Class II subjects but not in Class I and Class III cases. Thus, the precision of the angle procedure is limited to the occlusion of the molars, not regularly taking account of the front teeth which are of utmost importance in the assessment of sagittal malocclusions.
Due to the limitations of the angle method, a new classification of malocclusions, the bite-type,[4] was introduced in the literature in 2018 [Figure 2]. The bite-type is an extended angle classification that will improve the categorization of sagittal malocclusions by including the incisors in all the three molar-classes of angle. At the Department of Orthodontics, University of Giessen in Germany the bite-type classification has been the standard method for the assessment of sagittal malocclusions since 1995 and has completely replaced the angle system.
![The bite-type classification. Revised from Pancherz.[4]](/content/9/2021/11/2/img/APOS-11-100-g002.png)
- The bite-type classification. Revised from Pancherz.[4]
However, when proposing a new classification system, it is important to consider the reliability or consistency of the method. Therefore, the aim of the present study was to perform a reliability assessment of the bite-type classification. Operators representing different levels of experience in orthodontics were used in this reliability study.
MATERIALS AND METHODS
The study was carried out on pretreatment dental casts from the archives of the Faculty of Orthodontics, Malmö University, Sweden.
Patient data were handled according to the guidelines and requirements of the Declaration of Helsinki. Due to the design of this study no approval from an accredited research ethics committee was needed. All parents/legal guardians gave their written informed consent regarding the use of the dental casts of their children.
Bite-type classification
Molar relation
Like the angle classification from 1907,[3] the bite-type classification [Figure 2] assesses the sagittal relation of the occluding permanent first molars. Equivalent to angle, molar occlusion is given in three classes (I, II, and III):
Class I (neutral occlusion) = The mesiobuccal cusp of the maxillary first molar fits into the main buccal grove of the mandibular first molar (+½ cusp width) on both sides
Class II (distal occlusion) = The mesiobuccal cusp of the maxillary first molar occludes mesial (>½ cusp width) to the main buccal grove of the lower first molar on at least one side
Class III (mesial occlusion) = The mesiobuccal cusp of the maxillary first molar occludes distal (>½ cusp width) to the main buccal grove of the mandibular first molar on at least one side.
Incisor relation
In the bite-type classification also the sagittal relation of the incisors, expressed by the overjet, is considered, and given in four incisor classes (0, 1, 2, and 3):
0 = Normal overjet (2.0–3.5 mm). The maxillary incisors have a normal angulation
1 = Large overjet (>3.5 mm). The maxillary incisors are proclined or have a normal angulation. The central incisor with the largest overjet is considered
2 = Small overjet (<2.0 mm). The maxillary incisors are retroclined and the bite is deep, that is, the overbite is more than 5 mm. At least two central incisors must be affected
3 = Negative overjet (anterior cross bite) ranging to an incisor edge-to-edge incisor position. At least the two central incisors must be affected.
Consequently, in the bite-type classification the molar relations (I, II, and III) are combined with four incisor relations (0, 1, 2, and 3) resulting in the following nine bite-types [Figure 2]: I:0, I:1, I:2, I:3, II:0, II:1, II:2, III:0, and III:3.
Selection of dental casts – “Gold Standard”
Based on the overjet and molar relation (Angle classification), all pretreatment dental casts from the archives of the Department of Orthodontics in Malmö were screened. Only casts displaying a complete permanent dentition, except for the third molars, were selected.
After the screening, the two authors of this study evaluated the dental casts on two different occasions and independently of each other. The casts were appraised according to the bite-type classification. In case of disagreement, between the authors, which occurred in 4%, consensus was reached after discussion.
Finally, a total of 85 dental casts were selected and found suitable for this study. The casts represented the nine bite-types with about an equal number (7–10 casts) in each bite-type. These dental casts constituted the “Gold Standard” (= a predetermined diagnostic truth for each case based on consensus) for the later assessments by six operators. Each cast was randomly coded in a sequence from 1 to 85. This order was used in the later assessments by the operators.
Operators
Six operators participated to assess the intra- and inter-examiner reliability in classifying the nine bite-types. The operators were:
Two orthodontic specialists (Spec A and B) who both had more than 5 years of experience in clinical orthodontics
Two postgraduate orthodontic students (PG A and B) who both had more than 1 year of experience in clinical orthodontics
Two general dental practitioners (GP A and B) who both had over 15 years of experience in basic orthodontic diagnostics.
None of the operators had any previous knowledge of the new bite-type classification. However, before the classification of the 85 bite-types, the six operators were trained using [Figure 2] together with nine special dental casts corresponding to the nine bite-types. These nine casts were not included in the main study.
In the final assessment of the 85 dental casts the six operators had access to [Figure 2] as a help. The operators had to fill out a protocol based on the numerical coded list of the casts 1 to 85. After an interval of 4 weeks, the 85 dental casts were reevaluated by the six operators.
Statistical analysis
For the six operators, the intra-individual and inter-individual variability in categorizing each of the 85 dental casts was calculated by the McNemar’s test[5] for binomial distribution.
Differences between the nine bite-types were assessed by the Fisher’s exact test.[6] The test was performed in each of the six operators.
For all statistical analyses, differences with P < 5% (P < 0.05) were considered statistically significant.
RESULTS
The success rate of the six operators, all together, in correctly assessing the nine bite-types is shown in [Figure 3]. The results revealed an overall acceptable bite-type classification in each operator. No significant inter-operator (P-values between 0.078 and 1.000) or intra-operator (P-values between 0.082 and 1.000) differences were found.
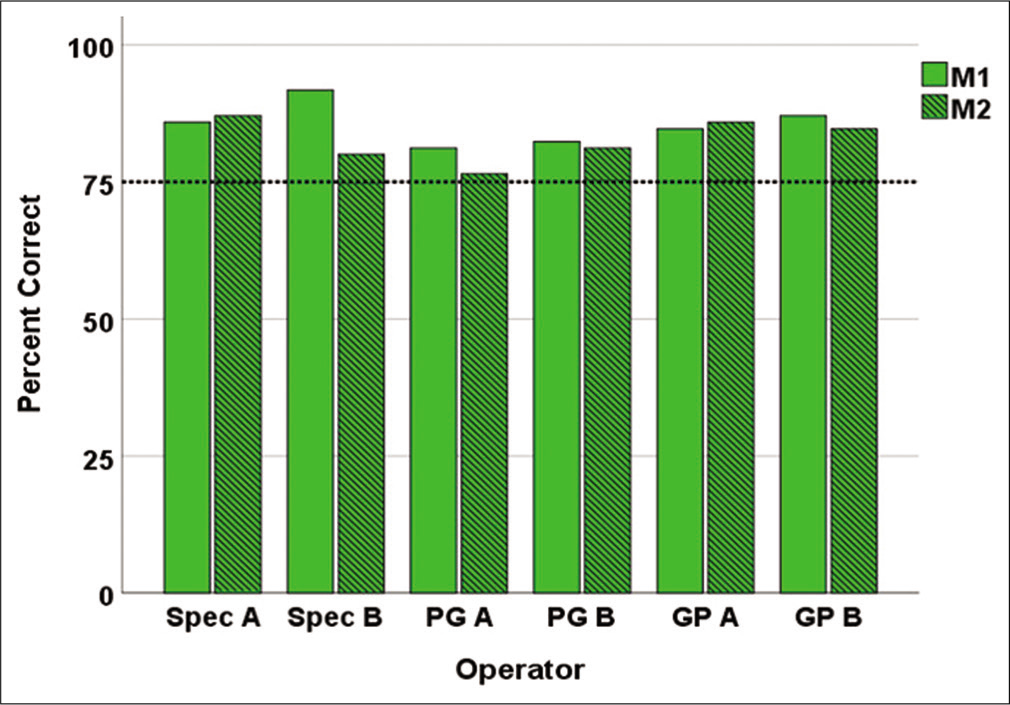
- Reliability of the sum of all nine bite-types: I:0, I:1, I:2, I:3, II:0, II:1, II:2, III:0, and III:3. Distribution of the number (%) of correct double measurements (M1 and M2) by six operators: Two orthodontic specialists (Spec A and B), two postgraduate orthodontic students (PG A and B) and two general practitioners (GP A and B). The dotted line in the graph represents an arbitrary acceptance level (75%) of correct classifications.
The ability of the six operators, separately, to correctly classify the nine bite-types is shown in [Figure 4a-i]. For the bite-types I:1, II:1, II:2, there were no classification problems for any of the operators [Figure 4b, f and g]. For the bite-types I:0, I;2, I:3, III:0, and III:3, some operators had classification problems [Figures 4a, c, d, h, and i]. Especially difficult to make correct assessments were found in two operators for bite-type II:0 [Figure 4e].
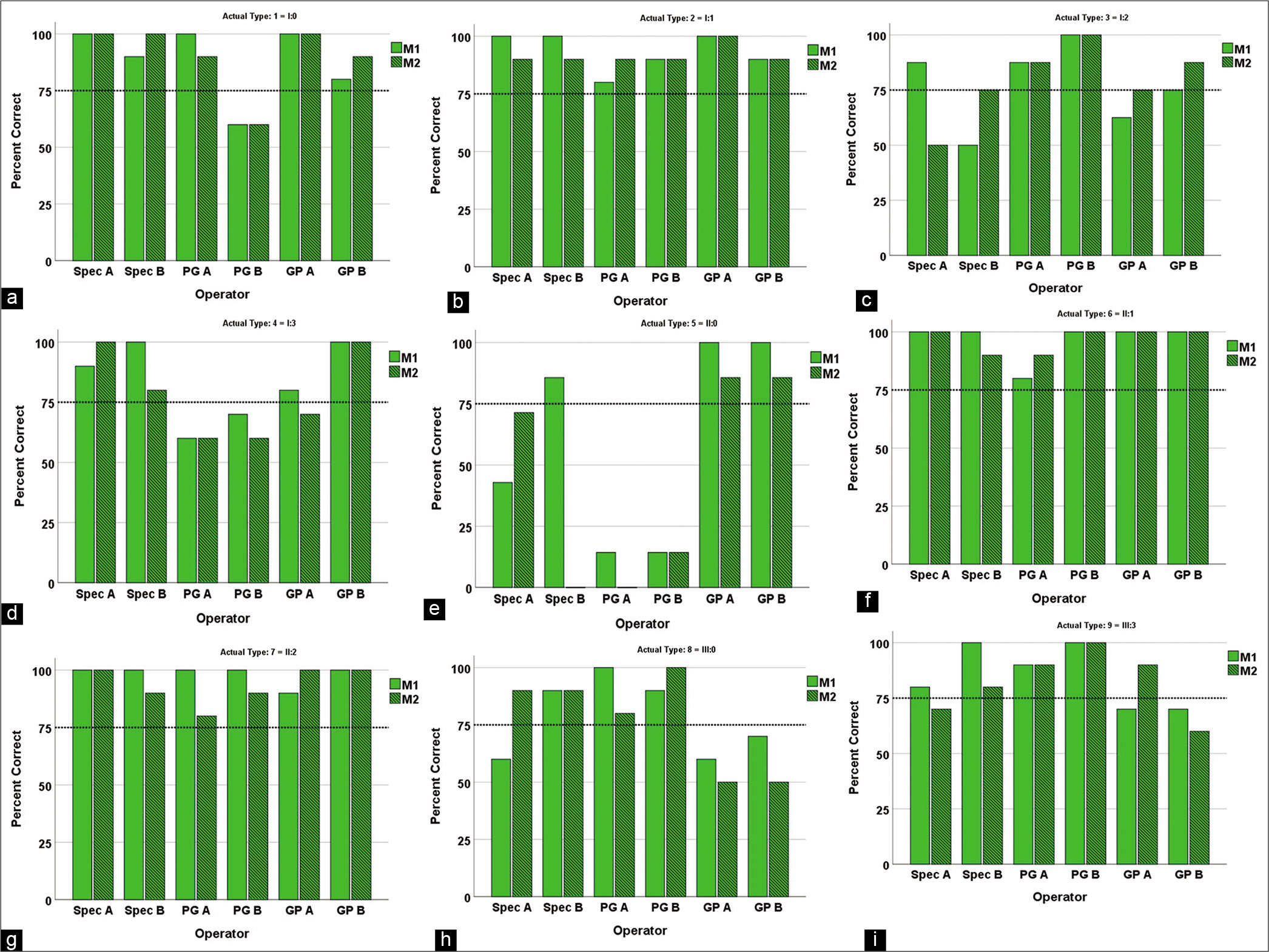
- Reliability of the 9 bite-types. Distribution of the number (%) of correct double measurements (M1 and M2) by six operators: Two orthodontic specialists (Spec A and B), two postgraduate orthodontic students (PG A and B) and two general practitioners (GP A and B). The dotted line in the 9 graphs represent an arbitrary acceptance level (75%) of correct classifications. Reliability of bite-type I:0 (a), in (b) bite-type I:1, in (c) bite-type I:2, in (d) bite-type I:3, in (e) bite-type II:0, in (f) bite-type II:1, in (g) bite-type II:2, in (h) bite-type III:0, and in (i) bite-type III:3.
DISCUSSION
The angle method has often been criticized:[7-11] “Angle is too limited and imprecise;” “Angle is not detailed enough;” “The method does not indicate the complexity of the problem;” “What about the incisors in Class I and Class III malocclusions?” “What to do in case of missing molars?” and “Molar rotation affects the classification.” The above critique points will certainly also apply for the molar area of the bite-type classification. However, as the front teeth always are included in the bite-type assessments, the method is more precise and more detailed than the angle procedure. Furthermore, in comparison to the angle classification the bite-type method permits a better intraand inter-class differentiation by combining the molar relation in each class with adequate overjet relations. Thus, bite-type I includes four overjet classes (0–3) while bite-type II includes three (0–2) and bite-type III two overjet classes (0 and 3). The reason for the exclusion of the overjet Class 3 in bite-type 2 and the overjet Classes 1 and 2 in Bite Type III is that they are not found clinically; at least we (the authors) have not seen any of them during our active time as orthodontists. This is also logical since no one would expect a negative overjet in a Class II (distal) occlusion case or a large overjet in a Class III (mesial) occlusion case.
The vertical incisor relation (overbite) is only considered in the bite-types I:2 and II:2. This, because retroclined maxillary incisors, as in these two bite-types, usually are combined with a deep bite.[12]
To the knowledge of the authors, only one study exists trying to evaluate the reliability of the angle classification.[8] In the present reliability investigation of the bite-type method, the consistency in classifying the different types of bite-types was found to be acceptable high. Hence, the percentage number of consistent assessments in the six operators, when summarizing the nine bite-types, exceeded 75% (75–92%) in the six operators. Furthermore, for individual bite-types and in individual operators correct assessments could be seen even in 100% of the dental casts analyzed.
Inconsistent registrations were especially found in postgraduate orthodontic students for the bite-types I:0 [Figure 4a] and II:0 [Figure 4e]. Obviously, a normal overjet, (0) as in these two bite-types, was difficult to assess consistently. Surprisingly, the general practitioners showed better results than the postgraduates. In relation to the amount of training in orthodontics, the opposite would have been expected.
CONCLUSION
The bite-type classification is a reliable method for the assessment of sagittal malocclusions. The procedure could favorably replace the angle classification as it is more precise and detailed without losing the strength of the angle system being an uncomplicated communication tool.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
None.
Conflicts of interest
There are no conflicts of interest.
References
- Treatment of Malocclusion of the Teeth and Fractures of the Maxillae In: Angle System (6th ed). Philadelphia, PA: SS White Manufacturing; 1900. p. 6-8, 77-144
- [Google Scholar]
- Treatment of Malocclusion of the Teeth and Fractures of the Maxillae In: Angle System (7th ed). Philadelphia, PA: SS White Manufacturing; 1907. p. :44-59.
- [Google Scholar]
- The bite type-an extended angle classification. Presentation of a new method. Kieferorthopädie. 2018;32:31-6.
- [Google Scholar]
- Note on the sampling error of the difference between correlated proportions or percentages. Psychometrika. 1947;12:153-7.
- [CrossRef] [PubMed] [Google Scholar]
- The characteristics of malocclusion: A modern approach to classification and diagnosis. Am J Orthod. 1969;56:443-54.
- [CrossRef] [Google Scholar]
- Angle classification revisited 1. Is current use reliable? Am J Orthod Dentofacial Orthop. 1992;102:173-9.
- [CrossRef] [Google Scholar]
- Dentoskeletal morphology in children with deckbiss. J Orofac Orthop. 1998;59:274-85.
- [CrossRef] [PubMed] [Google Scholar]




