

Translate this page into:
Management of root resorption of anterior teeth caused by impacted canines with emergency traction for replacement of central incisors
*Corresponding author: Tomonari Matsumura, Private Orthodontic Practice, LIV Orthodontics, Tokyo, Japan. matsumura.orts@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Matsumura T, Kanno Z, Kawabe A, Ono T. Management of root resorption of anterior teeth caused by impacted canines with emergency traction for replacement of central incisors. APOS Trends Orthod. 2024;14:282-6. doi: 10.25259/APOS_118_2023
Abstract
Impacted maxillary canines occasionally incline mesially and cause severe root resorption of the maxillary incisors. Here, we describe a case of severe root resorption of the maxillary central incisors caused by impacted canines and the successful alignment of the maxillary arch with the replacement of the central incisors by the canines using a super-elastic Ni-Ti alloy. Furthermore, we successfully managed the patient’s psychological distress using this approach. In the future, if the lateral incisors cannot be conserved, the retracted canines will be available as abutment teeth for prosthodontic treatment.
Keywords
Impacted canines
Maxillary incisors
Root resorption
Emergency traction
Orthodontic treatment

INTRODUCTION
Orthodontic patients commonly request improved facial esthetics. Satisfactory appearance and alignment of the maxillary incisors are critical factors for both facial esthetics and maxillofacial functions.[1]
However, the maxillary canines frequently erupt in a high and buccal position in patients with crowding of the anterior teeth. Furthermore, the prevalence of impacted maxillary canines is 2–3%.[2] Impacted maxillary canines occasionally incline mesially.[3] Moreover, approximately 50% of impacted canines cause root resorption of the maxillary lateral incisors, and root resorptions of the maxillary incisors occur most frequently at 11–12 years of age.[2] Various etiological factors have been suggested, including high lip pressure, mesial migration of the maxillary molars due to early loss of the deciduous teeth, and mesial localization of the canine tooth germ. Managing the psychological distress of losing anterior teeth in patients with root resorption is a crucial part of the treatment.[4]
Here, we describe a case of severe root resorption of the maxillary incisors caused by impacted canines and the successful alignment of the maxillary teeth with the replacement of the canines through the central incisors using a superelastic Ni-Ti alloy archwire.[5]
CASE REPORT
An 11-year-old female presented with the chief complaint of mobility of the bilateral maxillary central incisors. She had no notable medical history and a straight soft-tissue profile [Figure 1a-c]. The intraoral photographs and cephalograms revealed a skeletal Class II malocclusion [Table 1 and Figure 1d and e].
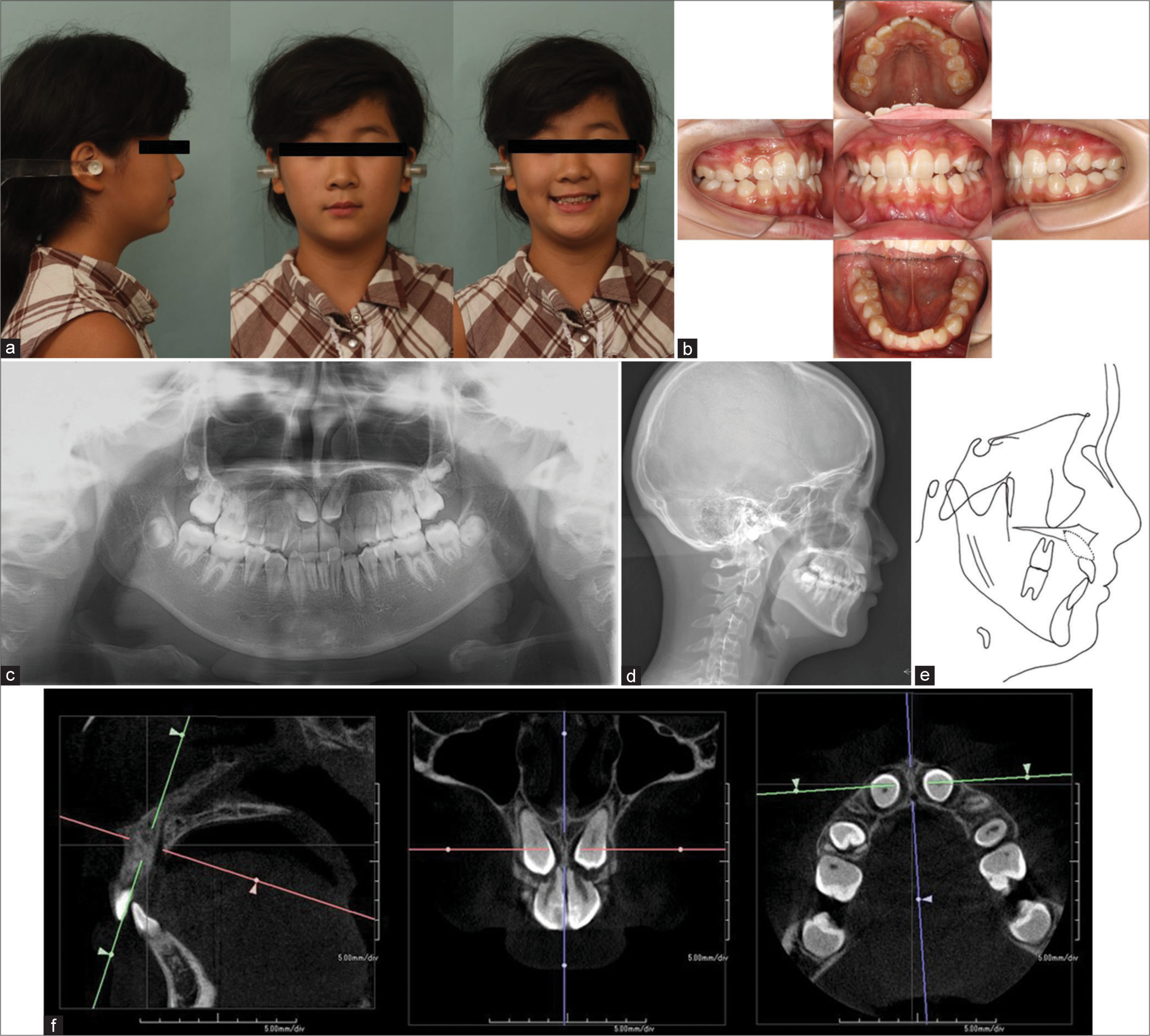
- Pre-treatment (a) Pre-treatment facial photographs. (b) Pre-treatment intraoral photographs. (c) Pre-treatment panoramic radiographs. (d) Pre-treatment cephalometric radiographs. (e) Pre-treatment cephalometric tracing. (f) Pre-treatment cone beam computed tomography images.
| Variables | Japanese Norm* | Pre-treatment | Post-treatment |
|---|---|---|---|
| Skeletal (degree) | |||
| SNA | 82.3±3.5 | 83.6 | 83.5 |
| SNB | 78.9±3.5 | 78.8 | 79.6 |
| ANB | 3.4±1.8 | 4.8 | 3.9 |
| FMA | 28.8±5.2 | 31.6 | 31.5 |
| Dental (degree) | |||
| IMPA | 96.3±5.8 | 87.7 | 88.3 |
| U1 to SN | 104.5±5.6 | 102.9 | 104.3 |
| Interincisal angle | 124.1±7.6 | 132.5 | 131.3 |
| Soft tissue (mm) | |||
| Upper lip to E-line | −1.0±2.0 | −2.0 | −2.0 |
| Lower lip to E-line | 1.0±2.0 | −2.0 | −1.0 |
*:Means and standard deviations (SDs) are depicted. SNA: Sella nasion point A, SNB: Sella nasion point B, ANB: A point, nasion, B point, FMA: Frankfort mandibular plane angle, IMPA: Angle between mandibular plane and long axis of the lower incisor. U1-SN: Angle between long axis of upper incisor and sella nasion.
A panoramic radiograph showed severe root resorption in the bilateral maxillary central incisors caused by the mesially inclined impacted canines, as well as congenital absence of the mandibular right lateral incisor. In addition, cone beam computed tomography revealed that the impacted canines were located apical to the respective central incisors [Figure 1f]. All four maxillary incisors were vital and exhibited mild-to-moderate mobility.
Treatment objectives
The treatment objectives for this patient were to (1) eliminate crowding; (2) establish an ideal overjet and overbite and to achieve a functional and stable occlusion in a Class I molar relationship; (3) achieve ideal esthetical and functional maxillary incisors; and (4) create an easy to maintain oral environment while saving as many healthy teeth as possible.
Treatment alternatives
Conventional bilateral maxillary first premolar extraction to align the teeth was considered in this case. However, due to their location, traction of the impacted canines to the original positions of the first premolars without damaging the lateral incisors was considered difficult; therefore, this option was excluded. Moreover, the extraction of the impacted canines was also considered. This option was also excluded due to their location and the mobility of the damaged maxillary central incisors. Another treatment option considered was to observe the impacted canines and delayed extraction of the central incisors followed by prosthodontic treatment (for example, dental implants or partial dentures). However, this option was also excluded due to the patient’s age and psychological distress due to the loss of the anterior teeth and further prosthodontic treatment.
Treatment progress
The mandibular left first premolar and bilateral maxillary central incisors were extracted. Next, the bone overlying the bilateral impacted maxillary canines was fenestrated, and traction was applied to move the canines to the original positions of the bilateral central incisors using a multi-bracket appliance. A lingual arch was placed for anchorage during traction. Dummy teeth for the central incisors were placed over the gingiva throughout the active treatment period, considering the esthetics. Finally, the canines were recontoured to imitate the central incisors using composite resin as a temporary restoration to prevent cutting natural teeth as much as possible. If necessary, prosthodontic treatment will be performed in the future [Figure 2a-c].

- Treatment progress. (a) Traction of the impacted canines. (b) After 5 months of traction. The contour of the canines can be observed. (c) After 12 months of traction. Beginning of the mandibular alignment.
Treatment results
The duration of active treatment was 31 months [Figure 3a-c]. At the end of active treatment, mobility of the bilateral maxillary central incisors (formerly canines) was unchanged and within the physiological range. Moreover, the periodontal condition was normal. Regarding the bilateral maxillary lateral incisors, mobility and other vitality reactions were unchanged. The difference between the maxillary central incisors and canines caused anterior tooth-size ratio discrepancy. Therefore, we used composite resin to recontour the canines as central incisors after orthodontic treatment [Table 1 and Figure 3d and e].
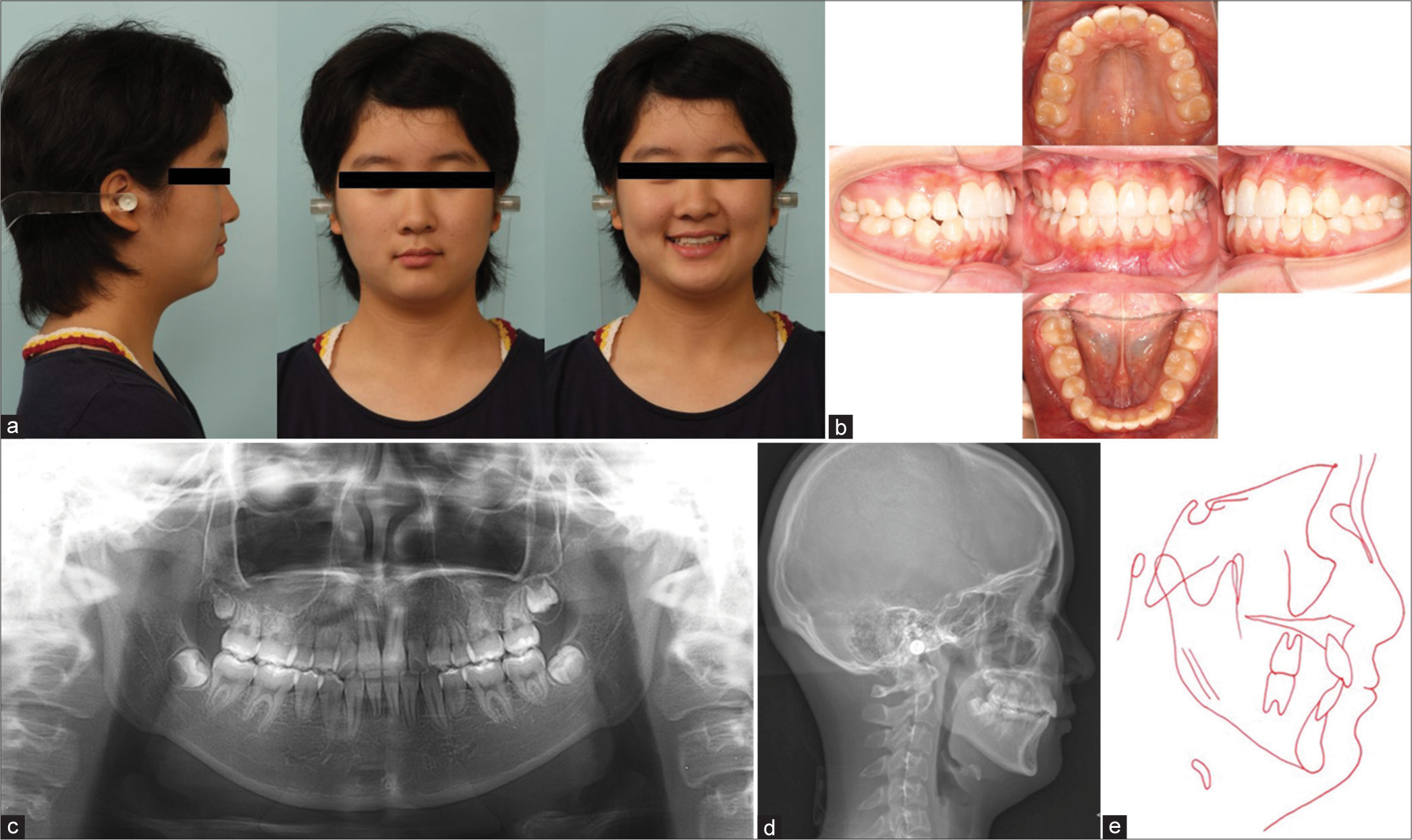
- Post-treatment. After 31 months of the active treatment: (a) Post-treatment facial photographs. (b) Post-treatment intraoral photographs. (c) Post-treatment panoramic radiographs. (d) Post-treatment cephalometric radiographs, (e) Post-treatment cephalometric tracing.
Superimposition of pre-and post-treatment cephalometric tracings revealed that alignment of the impacted canines had been achieved [Figure 4].
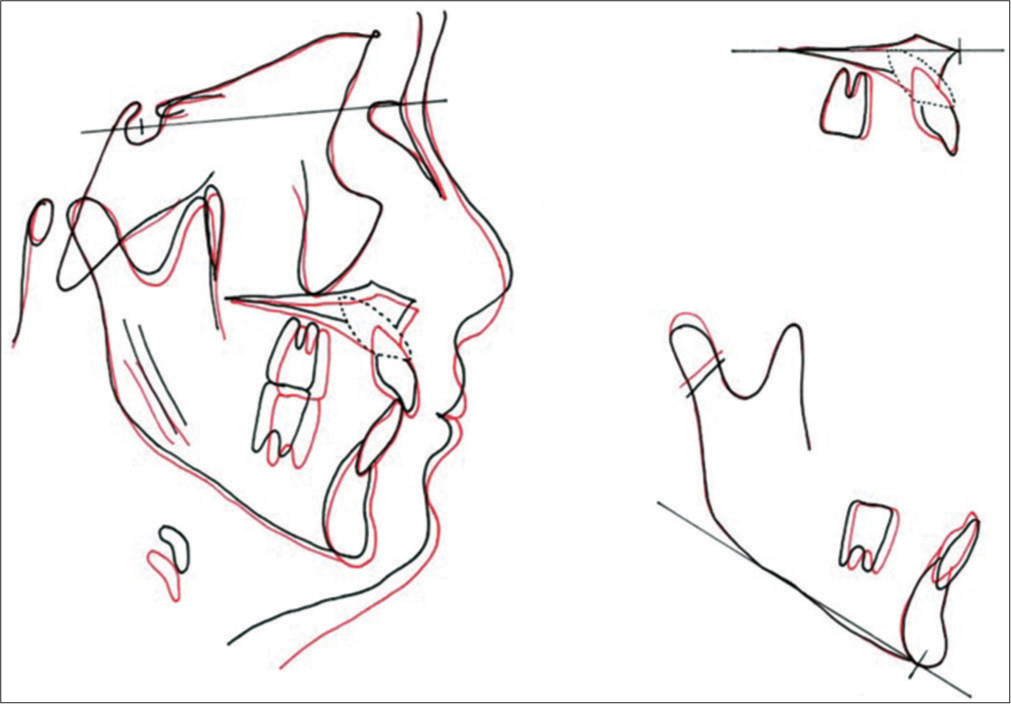
- Superimpositions, pre-treatment cephalometric tracing (black line), post-treatment cephalometric tracing (red line).
The patient and her parents were initially anxious about the treatment; however, they were satisfied with the result, as an esthetically pleasing smile was achieved.
DISCUSSION
In this case, we successfully aligned the maxillary arch by replacing the central incisors with the canines and conserved the bilateral lateral incisors. In the future, if the lateral incisors cannot be conserved, the retracted canines will be available as abutment teeth for prosthodontic treatment. Considering that the patient will be 14 years old at the end of treatment, it is necessary to observe the stability of the treatment results, including the late mandibular growth and the presence of wisdom teeth.
The prognosis of vital incisors showing root resorption should be determined through continuous observation and indefinite maintenance. Intensive and careful examination of the degree of the resorption, mobility, and vitality of the maxillary incisors and the location and inclination of the impacted canines are necessary and can be aided by cone beam computed tomography. Following this, comprehensive treatment planning should be discussed and selected. Managing the patients’ psychological distress associated with the loss of anterior teeth should be a crucial part of the treatment plan.
CONCLUSION
To avoid future complications, orthodontists should consider methods to manage root resorption of the anterior teeth due to impacted canines in children, even in the absence of symptoms.
Ethical approval
Institutional Review Board approval is not required.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- The importance of incisor positioning in the esthetic smile: The smile arc. Am J Orthod Dentofacial Orthop. 2001;120:98-111.
- [CrossRef] [PubMed] [Google Scholar]
- Orthodontic management of impacted maxillary canines. APOS Trends Orthod. 2020;10:64-71.
- [CrossRef] [Google Scholar]
- Outcomes of the surgical exposure, bonding and eruption of 82 impacted maxillary canines. J Can Dent Assoc. 1998;64:572-4.
- [Google Scholar]
- Multidisciplinary management of an impacted maxillary central incisor associated with supernumerary teeth: A case report. Gen Dent. 2018;66:46-50.
- [Google Scholar]
- The super-elastic property of the Japanese NiTi alloy for use in orthodontics. Am J Orthod Dentofacial Orthop. 1986;90:1-10.
- [CrossRef] [PubMed] [Google Scholar]




