

Translate this page into:
Prevalence evaluation of sleep-related breathing disorders in patients with class II malocclusion and mandibular deficiency using SRBD-PSQ


*Corresponding author: Fatemeh Kahnemuee, Department of Orthodontics, Dental Faculty, Zahedan University of Medical Sciences, Zahedan, Iran. fh.kahnamuee@yahoo.com
-
Received: ,
Accepted: ,
How to cite this article: Lal Alizadeh F, Abtahi M, Sekandari F, Kahnemuee F. Prevalence evaluation of sleep-related breathing disorders in patients with class II malocclusion and mandibular deficiency using SRBD-PSQ. APOS Trends Orthod. doi: 10.25259/APOS_88_2024
Abstract
Objectives:
Sleep-related breathing disorders (SRBDs) are a group of pathological conditions characterized by dysfunction in the upper airways, ranging from primary snoring to obstructive sleep apnea. The purpose of this study is to determine the prevalence of SRBD using the SRDB Scale of the Pediatric Sleep Questionnaire (SRBDPSQ) among children and adolescents with class II malocclusion and mandibular deficiency. In addition, it seeks to identify any correlations between SRBD and the mentioned malocclusion.
Material and Methods:
A census was conducted among potential candidates for mandibular advancement treatment who were referred to the orthodontic ward of Mashhad Dental School. The parents of 90 children aged 7 to 14 completed the Persian version of the SRBD-PSQ after clinical examination and confirmation of the need for mandibular advancement by an orthodontist.
Results:
Ninety questionnaires were collected for the study, with 37.8% being boys and 62.2% being girls. The overall prevalence of SRBD was found to be 15.6%. During the general examination, the questionnaire’s total score and behavioral differences were significantly higher in boys (P = 0.001, P = 0.004, respectively). Age displayed an inverse and significant relationship with behavioral disorders and SRBD (P = 0.023, P = 0.031, respectively), indicating a decrease in SRBD and behavioral disorders with increasing age. Individuals who answered positively to the questionnaire had significantly higher rates of snoring (P = 0.025) and behavioral disorders (P < 0.001) compared to others.
Conclusion:
SRDBs are more prevalent among children who meet the criteria for mandibular advancement treatment compared to the general population of children. Boys with attention deficit hyperactivity disorder require special attention. Snoring and behavioral disorders are key symptoms for diagnosing SRBD.
Keywords
Obstructive sleep apnea
Sleep disorders
Mandibular deficiency

INTRODUCTION
Sleep-related breathing disorders (SRDBs) encompass a range of conditions characterized by frequent episodes of reduced or obstructed respiratory airflow. These disorders present with various symptoms, including snoring, upper airway resistance syndrome, and the most severe manifestation, obstructive sleep apnea (OSA) syndrome.[1] OSA refers to the recurrent and chronic partial or complete collapse of the upper airway, occurring predominantly during the rapid eye movement stage but can also happen in other sleep stages.[2] The reported prevalence of OSA is 14% among males and 5% among females, with parent-reported apnea events during sleep ranging from 0.2% to 4%.[3] OSA peaks between the ages of 3 and 8 years in children, and snoring is a prevalent symptom of SRDBs, affecting approximately 1.5% to 27.6% of children.[2,4]
The management of OSA depends on factors such as the child’s age, symptom severity, clinical findings, presence of comorbidities, and polysomnography (PSG) results.[5] Large tonsils and lymph nodes are common risk factors for pediatric OSA, making adenotonsillectomy the primary treatment option.[6] Adenotonsillectomy has shown significant clinical efficacy in non-obese children, resulting in improved oximetry readings. Evidence-based guidelines recommend continuous positive airway pressure (CPAP) therapy as the first-line treatment for improving OSA in children without adenotonsillar hypertrophy, although its effectiveness may be limited by low compliance or patient refusal. A substantial proportion of children with OSA do not respond well to initial adenotonsillectomy or experience difficulties tolerating CPAP therapy. In comparison, mobile functional orthodontic appliances offer a less invasive and more tolerable alternative.[7] The multifactorial nature of OSA complicates its management, with craniofacial abnormalities and neuromuscular tone disorders during sleep emerging as significant etiological factors influencing disease development and exacerbation. In addition, lymphoid hyperplasia and growth-related changes in the upper airway size contribute to the severity of pediatric OSA.[3,5]
Children’s facial growth has a profound impact on the shape and size of the upper airway. The hard tissue boundaries of the upper airway encompass the maxillary and mandible incisors, the piriform rim in the front, the cervical vertebrae in the back, the skull floor above, and the hyoid bone below. Transversely, it is interconnected with the width of the palate, the middle fossa of the skull, and the distance between the rami. In addition, the soft tissue that forms the upper airway includes pharyngeal muscles, tongue, soft palate, nasal conchae, tonsils, lymph nodes, and nostrils.[8] The natural growth of the bony structures significantly amplifies the dimensions of the bone boundaries. Meanwhile, it concurrently reduces the size of the major lymphatic tissues in the upper airway, such as the tonsils and lymph nodes. Consequently, this process enlarges the airway.[9] The predominance of oral breathing, primarily caused by increased resistance in nasal breathing or hypertrophy of the adenoids and tonsils, results in a shift in the use of nasal and oral cavity muscles. This alteration affects the craniofacial development of growing children, modifies the position of the tongue, increases oropharyngeal volume, and ultimately heightens the risk of apnea.[10]
The diagnosis of pediatric OSA is exclusively confirmed through PSG, which is considered the gold standard. This diagnostic method entails various physiological measurements such as electroencephalogram, electrocardiogram, airflow measurement, and observation of body position during sleep.[5] A comprehensive PSG typically involves the examination of sleep stages, hand and leg movements, airflow patterns, respiratory system activity, heart rate, blood oxygen saturation levels, and body position. These examinations are conducted in sleep clinics under the expertise of sleep specialists.[11] Finally, the apnea/hypopnea index serves as the most commonly used metric for reporting OSA. This index differentiates between individuals with and without the disorder and aids in assessing its severity.[2,12]
The diagnostic evaluation of childhood OSA has undergone advancements in recent years. At present, all pediatric PSGs include carbon dioxide (CO2) monitoring. This can be done through end-tidal CO2 measurement or CO2 monitoring through the skin.[3] Children with OSA and craniofacial risk factors should be referred to an orthodontist who is part of a multidisciplinary sleep medicine team.[7]
Orthodontic treatment for patients with OSA is based on correcting dental and bone defects associated with this condition. Two common orthodontic procedures used to increase the size of the upper airway are mandibular advancement appliances and rapid maxillary expansion for treating class II malocclusion. The initial effect of these appliances is to improve occlusion and reduce bone defects.[13] It is worth noting that a patient with OSA may be recommended for maxillary expansion without a transverse discrepancy or for mandibular (or maxillary) advancement without a sagittal discrepancy. In such cases, treatment alternatives should be considered by the relevant physicians and dentists based on the patient’s specific needs.[3]
Numerous studies have investigated the mechanisms and effects of functional appliances. The short-term use of functional appliances has shown no evidence of contraindications or significant side effects due to their temporary nature.[14] Recent systematic reviews and meta-analyses indicate that when functional appliances are used during puberty, they have greater skeletal effects on the mandible in the short term.[15] Studies on growing adolescents with class II skeletal malocclusion treated with functional appliances have demonstrated an increase in the dimensions of the pharyngeal respiratory tract in the oropharynx region. These changes persist even after growth completion.[16] However, in patients treated before puberty, the significant effects are primarily limited to the dental and alveolar surfaces.[17] Therefore, the age of the child plays a crucial role in OSA treatment. Some children who are unresponsive to CPAP therapy may require airway support during sleep. In these cases, the prescribing physician may recommend the use of mandibular advancement appliances. The prescription is not solely based on occlusion classification but primarily focuses on supporting and maintaining the airway while considering orthopedic and dentofacial control. Accurate monitoring of facial growth is essential during this period.[18]
As early diagnosis of OSA leads to more effective treatment and has a significant impact on people’s quality of life, it is crucial to identify OSA in its early stages. OSA can result in serious complications, such as developmental delay, memory loss, mental illnesses, metabolic disorders, cardiovascular diseases, and even premature death, if left untreated.[7,19,20] While numerous studies have investigated the effects of treating class II malocclusion with mandibular deficiency on patients with OSA, none have specifically focused on OSA in children who are candidates for this treatment. Therefore, this study aimed to investigate the incidence of OSA in children who require mandibular advancement treatment with functional appliances.
MATERIAL AND METHODS
This cross-sectional analytical study was conducted between September 2021 and August 2022 at the Faculty of Dentistry at Mashhad University of Medical Sciences. The study population included patients referred to the orthodontic department who were candidates for mandibular advancement treatment due to suspected OSA. The sample size calculation was based on a previous similar study conducted by Ghonim et al.,[21] assuming a 20% prevalence of OSA in the population. With an alpha error of 0.05 and a beta error of 0.9, the required sample size was determined to be 90 patients.[21]
Participants were recruited using the following inclusion criteria: (1) provision of informed consent, (2) absence of physical or mental disabilities, (3) no craniofacial syndromes, (4) no current use of sleeping pills, and (5) no neurological disorders, including attention-deficit hyperactivity disorder or related medications. Patients who met these criteria were enrolled consecutively until the required sample size was reached.
All participants completed the SRDB Pediatric Sleep Questionnaire (SRBD-PSQ), which consists of 22 items across three domains: snoring, sleepiness, and behavior. The questionnaire was distributed to participants in written form and completed independently by the patients. Responses were coded as “yes” (scored 1), “no” (scored 0), or “I don’t know” (treated as missing data). The final score was calculated by averaging non-missing responses, with scores ranging from 0 to 1. A cutoff value of ≥0.33 indicated a higher risk of OSA. The Persian version of the SRBD-PSQ used in this study demonstrated acceptable internal consistency, with a Cronbach’s alpha ranging between 0.56 and 0.76.
For missing questionnaire responses, participants with fewer than 20% missing answers were included in the analysis, with the average score of non-missing items used for final score calculation. If more than 20% of responses were missing, the participant’s data was excluded from the analysis.
Data were analyzed using the Statistical Package for the Social Sciences 22 software, and the Shapiro–Wilk test was conducted to determine the normality of the data distribution for quantitative variables. Mann–Whitney and independent t-tests were performed to compare snoring, sleepiness, behavior disorder, and total scores in male and female participants with breathing disorders. In addition, Chi-square and Fisher’s exact tests were used to examine the relationship between snoring, sleepiness, behavioral disorders, and breathing disorders.
RESULTS
In this study, the SRBD-PSQ questionnaire was completed by the parents of 90 participants. The questionnaire assessed three areas: snoring, sleepiness, and behavioral characteristics. The variables studied in this research are described in [Table 1].
| Variable | n | % | SD±Mean | (Min–Max) |
|---|---|---|---|---|
| Gender | ||||
| Female | 56 | 62.2 | ||
| Male | 34 | 37.8 | ||
| Age (year) | 1.54±10.56 | (7–14) | ||
| Snoring | 33.0±0.65 | (0–3) | ||
| Sleepiness | 74±0.94 | (0–3) | ||
| Behavioral disorder | 1.80±1.76 | (0–6) | ||
| Total score | 4.21±73.2 | (0–11) |
SD: Standard deviation
Frequency of participants with breathing disorders and their areas: [Figure 1] presents the number and percentage of subjects with breathing disorders, snoring disorders, sleep disorders, and behavioral disorders. Among the subjects, 15.6% (n = 14) were identified to have breathing disorders, 5.6% (n = 5) exhibited snoring disorders, 23.3% (n = 21) had sleep disorders, and 47.8% (n = 43) displayed behavioral disorders.
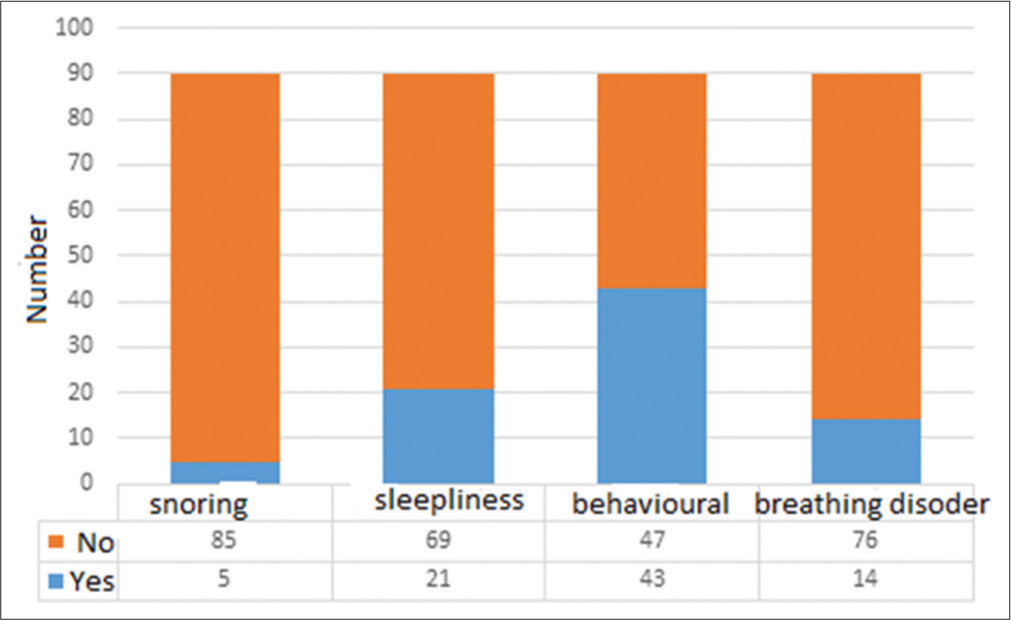
- Subjects with breathing disorders in their sleep.
Investigating the relationship between different areas of the questionnaire and breathing disorders: [Table 2] depicts the relationship between snoring, sleepiness, and behavioral variables in individuals with and without breathing disorders. The data show that 21.4% (n = 3) of subjects with breathing disorders and 2.6% (n = 2) of subjects without breathing disorders experienced snoring. This difference was statistically significant (P = 0.025). Regarding sleepiness, 35.7% (n = 5) of subjects with breathing disorders and 21.1% (n = 16) of subjects without breathing disorders reported sleepiness. However, this difference was not statistically significant (P = 0.302). In terms of behavioral disorders, 100% (n = 14) of subjects with breathing disorders and 38.2% (n = 29) of subjects without breathing disorders indicated behavioral issues. This difference was statistically significant (P < 0.001).
| Breathing disorder | Snoring | Sleepiness | Behavioral disorder | |||
|---|---|---|---|---|---|---|
| No | Yes | No | Yes | No | Yes | |
| No | 74 (97.4) | 2 (2.6) | 60 (78.9) | 16 (21.1) | 47 (61.8) | 29 (38.2) |
| Yes | 11 (78.6) | 3 (21.4) | 9 (64.3) | 5 (35.7) | 0 (0) | 14 (100) |
| Total score | 85 (94.4) | 5 (5.6) | 69 (76.7) | 21 (23.3) | 47 (52.2) | 43 (47.8) |
| Chi-square test result | P*=0.025 | P*=0.302 | χ2=18.12 p<0.001 | |||
The relationship between snoring, sleepiness, behavioral disorder, total score, and age is analyzed in [Table 3]. The data reveal an inverse relationship between age and the variables of snoring, sleepiness, behavioral disorder, and total score. However, this relationship was not significant for any of the variables. Snoring showed a direct relationship with sleepiness, behavioral disorder, and total score, but its significant relationship was only observed with the total score (P = 0.002). Sleepiness demonstrated a significant direct relationship with behavioral disorder and total score (P = 0.017 and P < 0.001, respectively). The area of behavioral disorder also displayed a significant direct relationship with the total score (P < 0.001).
| Variable | Snoring | Sleepiness | Behavioral disorder | Total score |
|---|---|---|---|---|
| Age | Rsp=−0.021 p=0.842 | Rsp=−0.034 p=0.749 | Rsp=−0.126 p=0.237 | Rsp=−0.018 p=0.864 |
| Snoring | - | Rsp=0.110 p=0.303 | Rsp=0.084 p=0.433 | Rsp=0.328 p=0.002 |
| Sleepiness | - | Rsp=0.252 p=0.017 | Rsp=0.616 p<0.001 | |
| Behavioral disorder | - | Rsp=0.743 p<0.001 |
Rsp: Spearman correlation coefficient, P:P-value
The number, mean, standard deviation, median, interquartile range, minimum, and maximum scores of snoring, sleepiness, behavioral disorder, and total score based on gender, along with the results of statistical tests, are presented in [Table 4]. The data show that although males had higher mean scores than females in all areas and the total score, a significant difference was observed only in the behavioral score and total score (P = 0.004 and P = 0.001, respectively).
| Variable | n | SD±Mean | (Interquartile range) Median | Range (Min–Max) | Mann–Whitney U test result |
|---|---|---|---|---|---|
| Snoring | |||||
| Female | 56 | 0.30±0.69 | 0.0 (0.0) | 0.0–3.0 | Z=1.07 |
| Male | 34 | 0.38±0.60 | 0.0 (1.0) | 0.0–2.0 | p=0.286 |
| Sleepiness | |||||
| Female | 56 | 0.66±0.98 | 0/0 (1.0) | 0.0–3.0 | Z=1.44 |
| p=0.151 | |||||
| Behavioral disorder | |||||
| Male | 56 | 1.39±1.60 | 1.0 (2.0) | 0.0–6.0 | Z=2.86 |
| Female | 34 | 2.47±1.81 | 3.0 (3.0) | 0.0–6.0 | p=0.004 |
| Total score | |||||
| Male | 56 | 3.54±2.68 | 3.0 (4.0) | 0.0–10.0 | Z=3.19 |
| Female | 34 | 5.32±2.47 | 5.0 (3.3) | 1.0–11.0 | p=0.001 |
SD: Standard deviation
DISCUSSION
SRDBs, classified as the second category in the International Classification of Sleep Disorders-3, 2015, encompass a wide range of symptoms, including snoring, OSA, and airway resistance.[1,20] Snoring and OSA are particularly prominent symptoms observed in children with SRDBs.[22] Untreated SRBD can lead to neurological and behavioral disorders, developmental deficits, attention deficit/hyperactivity, as well as cardiac and metabolic problems.[20] The primary risk factors exacerbating this condition in children often include tonsil hypertrophy and craniofacial anomalies.[3]
At present, orthodontics plays a significant role in the diagnosis and treatment of SRDB-related syndromes. Studies have reported a correlation between malocclusion, posterior cross-bite, changes in overjet and overbite, and OSA in children.[23] Maxillary stenosis and a class II skeletal relationship with mandibular deficiency have been widely accepted as dominant risk factors.[7] This study utilizes the Persian version of the SRBD-PSQ to investigate the prevalence of SRDBs in patients with class II malocclusion and mandibular deficiency who visited the orthodontic department of Mashhad Faculty of Dentistry in 2021. Ninety questionnaires were completed and collected from parents of children aged 7 to 14 years, with 37.8% of the respondents being male and 62.2% being female.
Analysis of all children included in the study revealed a direct and significant relationship between all areas of the questionnaire and the total score. There was a positive and significant correlation between the sleepiness area and the behavioral disorder area. Boys exhibited significantly higher total scores and scores for behavioral disorders. There were no significant differences between fathers and mothers with academic and non-academic education levels across all areas and total scores. The prevalence of SRDBs in the studied population was 15.6%, highlighting the need for further investigation and referrals to sleep clinics. Among children who answered positively on the questionnaire, age showed an inverse and significant relationship with the total score and behavioral disorder area. The behavioral disorder area had a direct and significant correlation with the total score. There were no significant differences between male and female subjects in all areas and the total score, except for a higher rate of snoring and behavioral disorder among subjects with positive answers compared to healthy subjects.
A study by Galeotti et al.[23] aimed to examine the prevalence of malocclusion in children aged 2–10 years with OSA and evaluate the relationship between occlusal variables and OSA. In this study, all patients underwent clinical orthodontic examinations to record occlusal variables, including milk-canine relation, presence of posterior cross-bite, overjet, and overbite. For children whose parents reported snoring and common symptoms of OSA, the diagnosis was confirmed through pulse oximetry and cardiorespiratory polygraphy conducted at home. The study revealed a high prevalence of malocclusion in children with OSA compared to the control group. The prevalence of malocclusion was higher in children with OSA (89.9%) compared to the control group (60.6%) (P > 0.001).
Posterior cross-bite and deviations in overjet and overbite (reduced overbite, increased overbite, and increased overjet) are significantly associated with OSA, as shown in our study. Among class I patients, a milk-canine relationship was observed in a higher number of cases,[24] while studies on patients with class II malocclusion and open bite have shown larger overjet and smaller overbite to be more commonly observed.[22] Our study, as well as others, has shown a link between malocclusion and OSA.
In a 2018 study in America, DaRocha et al.[25] investigated the relationship between SRDB symptoms and specific oral health indicators in children. The study used the SRBDPSQ to screen for SRDBs. Angle classification, the molar relationship of the first permanent molar, attention-deficit/hyperactivity disorder, and dental crowding were not found to be associated with the SRBD-PSQ score. However, in our study, a positive and significant relationship was found between the questionnaire score and behavioral disorder, which may be due to age differences and different populations studied. The mean age of our study was younger at 7 years compared to DaRocha et al.’s[25] study, where children started from age 7. One-third of sleep problems remained unnoticed when parents completed questionnaires in a study by Paavonen et al.,[26] which was also observed in our study.
A 2019 study in Canada examined the prevalence of SRBD among children aged 5–16 receiving orthodontic treatment using the Pediatric Sleep Questionnaire (PSQ). The prevalence of positive risk of SRDB among the children receiving orthodontic treatment was significantly higher than in the general population of children (average 5%), which was similar to our study. Attention-deficit/hyperactivity disorder was more prevalent in orthodontic patients with a higher risk of SRDB in both our study and the Canadian study, as the PSQ was used in both studies.[27]
Di Carlo et al.[28] studied the prevalence of SRDB using the PSQ on 668 patients from the Department of Oral and Maxillofacial Sciences, Sapienza University of Rome, Italy, and the Department of Pediatric Dentistry, University of Murcia, Spain. The prevalence of SRBD for the whole sample was 7.9%, with a positive correlation between snoring, bad habits, and anxiety with SRDB. Our study also found a direct and positive association between all areas and SRBD, likely due to the use of the PSQ in both studies. However, only sleepiness and behavioral disorder showed a significant relationship, which may be due to our much smaller population size (n = 90) compared to Di Carlo et al.’s study (n = 668).[28] The prevalence of SRBD in our study was higher than that in a study by Constanze Sauer, possibly due to the difference in our population demographics, as our study was conducted among patients who needed orthodontic treatment with class II malocclusion and mandibular deficiency.
A study by Vázquez-Casas et al.[20] investigated the prevalence of SRBD in patients with craniofacial abnormalities and compared the results before and after treatment using the PSQ and SRBD-PSQ completed by parents. The study found a higher prevalence of SRBD (22.8%) compared to our study, which may be attributed to the inclusion of all types of craniofacial abnormalities in their population.
In India, a study by Metgud et al.[29] investigated the correlation between orofacial disorders and SRDBs in primary school children using the Nordic Orofacial Test-Screening and PSQ. The study found a positive relationship between the two disorders, with 8.58% of children at risk for SRDBs and 32.6% of children having symptoms of orofacial disorders. The lower prevalence of SRDBs in this study may be due to the general population studied and the larger sample size compared to our study. In addition, females had a higher risk of SRDBs in this study, unlike our study where gender did not show a significant association.
Previous reports have shown varying prevalence rates of SRBD between males and females. Our study, as well as others, has found higher prevalence rates in males. However, some studies have found no association between gender and the prevalence of OSAS. Age has also been suggested as a factor in the prevalence of SRBD, with lymphoid tissue development being complete at a certain age. However, a review article reported no significant differences in the severity of SRBD among different age groups.
The lower prevalence rate found in the Indian study can be attributed to the general population being studied. In contrast to our study, females had a higher risk than males, possibly due to the larger sample size in the Indian study (482 people, with almost equal numbers of males and females). Published reports have shown that similar to our findings, the prevalence range of SRBD in males is between 6.5% and 13.6%, while in females, it is lower at 3.3–7.4%. However, other studies did not find any significant association between gender and the prevalence of OSAS.[30]
It is generally assumed that the prevalence of SRBD would decrease with age once lymphoid tissue development is complete. However, a review article[2] reported the opposite result, showing no significant differences in the severity of SRBD among subjects aged 4–11 years and 2–13 years.
CONCLUSION
The prevalence of SRDBs is higher among children who are potential candidates for mandibular advancement appliances compared to the general pediatric population. This suggests a possible association between SRBD, class II malocclusion, and mandibular deficiency, although further comprehensive research is needed to validate these findings.
In addition, special attention should be given to males with attention-deficit/hyperactivity disorder, as they may have a higher risk for SRBD. Snoring and behavioral disorders emerged as significant symptoms associated with the diagnosis of SRBD in this study.
Given that children with craniofacial abnormalities, including those with class II malocclusions, are frequently referred to orthodontic specialists, these specialists are well-suited to screen for SRBD using the SRBD-PSQ questionnaire. The early detection of SRBD through questionnaires like the SRBD-PSQ is particularly important in pediatric and orthodontic clinics, where patients with craniofacial abnormalities, known risk factors for SRBD, are often seen.
While our study suggests important relationships between mandibular advancement, class II malocclusion, and SRBD, more detailed longitudinal studies are needed to confirm these results and explore the mechanisms behind these associations.
Ethical approval
The research/study was approved by the Institutional Review Board at IR.MUMS.DENTISTRY.REC, number 1400.065, dated August 4, 2021.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- Obstructive sleep apnea, metabolic dysfunction, and periodontitis-machine learning and statistical analyses of the dental, oral, medical epidemiological (DOME) big data study. Metabolites. 2023;13:595.
- [CrossRef] [PubMed] [Google Scholar]
- Epidemiology of pediatric obstructive sleep apnea. Proc Am Thorac Soc. 2008;5:242-52.
- [CrossRef] [PubMed] [Google Scholar]
- Obstructive sleep apnea and orthodontics: An American Association of Orthodontists White Paper. Am J Orthod Dentofacial Orthop. 2019;156:13-28.e1.
- [CrossRef] [PubMed] [Google Scholar]
- Diagnosis and treatment of sleep apnea in children: A future perspective is needed. Biomedicines. 2023;11:1708.
- [CrossRef] [PubMed] [Google Scholar]
- Multidisciplinary clinic for care of children with complex obstructive sleep apnea. Int J Pediatr Otorhinolaryngol. 2020;138:110384.
- [CrossRef] [PubMed] [Google Scholar]
- Relationships among and predictive values of obesity, inflammation markers, and disease severity in pediatric patients with obstructive sleep apnea before and after adenotonsillectomy. J Clin Med. 2020;9:579.
- [CrossRef] [PubMed] [Google Scholar]
- Effectiveness of functional orthodontic appliances in obstructive sleep apnea treatment in children: Literature review. Brazilian J Otorhinolaryngol. 2022;88:263-78.
- [CrossRef] [PubMed] [Google Scholar]
- Anatomy and pathophysiology of upper airway obstructive sleep apnoea: Review of the current literature. Sleep Med Res. 2021;12:1-8.
- [CrossRef] [Google Scholar]
- Evaluation of an individualized facial growth prediction model based on the multivariate partial least squares method. Angle Orthod. 2022;92:705-13.
- [CrossRef] [PubMed] [Google Scholar]
- Orthodontics treatments for managing obstructive sleep apnea syndrome in children: A systematic review and meta-analysis. Sleep Med Rev. 2016;25:84-94.
- [CrossRef] [PubMed] [Google Scholar]
- Clinical guideline for the evaluation, management and long-term care of obstructive sleep apnea in adults. J Clin Sleep Med. 2009;5:263-76.
- [CrossRef] [PubMed] [Google Scholar]
- Effect of orthopedic and functional orthodontic treatment in children with obstructive sleep apnea: A systematic review and meta-analysis. Sleep med Rev. 2023;67:101730.
- [CrossRef] [PubMed] [Google Scholar]
- Treatment effects of removable functional appliances in patients with Class II malocclusion: A systematic review and meta-analysis. Eur J Orthod. 2015;37:418-34.
- [CrossRef] [PubMed] [Google Scholar]
- Treatment effects of removable functional appliances in pre-pubertal and pubertal class II patients: A systematic review and meta-analysis of controlled studies. PLoS One. 2015;10:e0141198.
- [CrossRef] [PubMed] [Google Scholar]
- Treatment and post-treatment effects of functional therapy on the sagittal pharyngeal dimensions in Class II subjects. Int J Pediatr Otorhinolaryngol. 2017;101:47-50.
- [CrossRef] [PubMed] [Google Scholar]
- Treatment timing for functional jaw orthopaedics followed by fixed appliances: A controlled long-term study. Eur J Orthod. 2018;40:430-6.
- [CrossRef] [PubMed] [Google Scholar]
- Craniofacial, dental arch morphology, and characteristics in preschool children with mild obstructive sleep apnea. J Dent Sci. 2020;15:193-9.
- [CrossRef] [PubMed] [Google Scholar]
- Obstructive sleep apnea in adults. Dent Press J Orthod. 2019;24:99-109.
- [CrossRef] [PubMed] [Google Scholar]
- Prevalence of sleep-related breathing disorders in children with malocclusion. J Clin Exp Dent. 2020;12:e555-60.
- [CrossRef] [PubMed] [Google Scholar]
- Prevalence of obstructive sleep apnea in orthodontic patients with different skeletal classes using STOP-BANG questionnaire: An observational study. Open Access Maced J Med Sci. 2021;9:87-91.
- [CrossRef] [Google Scholar]
- Sleep-disordered breathing in children. Pediatr Rev. 2019;40:3-13.
- [CrossRef] [PubMed] [Google Scholar]
- Prevalence of malocclusion in children with obstructive sleep apnoea. Orthod Craniofac Res. 2018;21:242-7.
- [CrossRef] [PubMed] [Google Scholar]
- Prevalence of sleep-disordered breathing and associations with malocclusion in children. J Clin Sleep Med. 2020;16:1007-12.
- [CrossRef] [PubMed] [Google Scholar]
- Association of sleep disordered breathing with oral health findings in children. J Dent Sleep Med. 2022;9:3-11.
- [CrossRef] [Google Scholar]
- Sleep problems of school-aged children: A complementary view. Acta Paediatr (Oslo, Norway 1992). 2000;89:223-8.
- [CrossRef] [Google Scholar]
- Pediatric sleep-disordered breathing in the orthodontic population: Prevalence of positive risk and associations. Am J Orthod Dentofacial Orthop. 2020;157:466-73.e1.
- [CrossRef] [PubMed] [Google Scholar]
- Prevalence of sleep-disordered breathing in children referring for first dental examination. A multicenter cross-sectional study using pediatric sleep questionnaire. Int J Environ Res Public Health. 2020;17:8460.
- [CrossRef] [PubMed] [Google Scholar]
- Association of orofacial dysfunction and sleep disordered breathing among Indian primary school children. J Oral Biol Craniofac Res. 2022;12:639-44.
- [CrossRef] [PubMed] [Google Scholar]
- Prevalence of obstructive sleep apnea syndrome and associated symptoms in 3--11-year-old Turkish children. Pediatr Pulmonol. 2005;39:251-6.
- [CrossRef] [PubMed] [Google Scholar]




