

Translate this page into:
A systematic review of mandibular advancement using clear aligners in patients with sleep apnea

*Corresponding author: Fatimah Mohammed Abdu Samater, Department of Orthodontics, Dammam Medical Complex, Dammam, Saudi Arabia. dr.fatimah.sam@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Samater FM, Aldomiaty DT, Alqahtani RF, Alzahrani AM, Alharthi DS. A systematic review of mandibular advancement using clear aligners in patients with sleep apnea. APOS Trends Orthod. 2025;15:1-11. doi: 10.25259/APOS_152_2024
Abstract
Objectives:
Aligners are one of the orthodontic appliances that are rarely touched upon by orthodontists when they talk about obstructive sleep apnea (OSA) and its treatment modalities. This systematic review was aimed at understanding the effectiveness of the mandibular advancement (MA) technique using aligners in managing OSA and its associated impact on nasal airway volume, morphology, and the position of the hyoid bone.
Material and Methods:
A standardized data extraction form was devised to extract relevant variables from the studies that were identified through an extensive online search across multiple databases, with the whole process being conducted in accordance with the preferred reporting items for systematic reviews and meta-analysis guidelines.
Results:
The four papers selected for this review were quite heterogeneous in their treatment approaches. The use of MA devices (MADs) in conjunction with orthodontic aligners was successful in managing snoring and mild sleep apnea and allowed the continuation of orthodontic treatment. Clear aligners for upper arch expansion increase nasal airway volume and intermolar distance, particularly in pediatric patients. The treatment protocol of maxillomandibular advancement (MMA), followed by post-operative surgical treatment, also resulted in successful post-operative outcomes and resolution of OSA. The use of aligners improved the upper airway morphology and hyoid bone position, with MA using aligners being more effective in improving the narrowest part of the hypopharynx.
Conclusion:
The study found that moving the lower jaw forward with aligners could help some people with OSA, make their nasal airways bigger, improve the shape of their upper airways, and put the hyoid bone in the best place. These findings could inform future therapeutic strategies and patient management protocols in orthodontic practice.
Keywords
Mandibular advancement device
Clear aligners
Invisalign mandibular advancement
Maxillomandibular advancement
Obstructive sleep apnea
Orthodontic treatment
Post-operative care

INTRODUCTION
Obstructive sleep apnea (OSA) is a prevalent sleep disorder characterized by repeated episodes of partial or complete upper airway obstruction during sleep, resulting in disrupted sleep and oxygen desaturation.[1] This condition is associated with numerous health consequences, including daytime sleepiness, cognitive dysfunction, and an increased risk of cardiovascular disease.[1] Sleep apnea is a significant sleep disorder marked by repeated breathing interruptions during sleep, known as “apneas.” These can last anywhere from a few seconds to minutes and may occur over 30 times/h, resulting in poor sleep quality and leading to excessive daytime sleepiness and other health-related issues.[2] It is a common condition, affecting around 3–7% of men and 2–5% of women in the general population. However, it is believed that many cases go undiagnosed, suggesting that the actual prevalence could be even higher.[3]
The primary cause of sleep apnea is often the excessive relaxation of the muscles in the back of the throat, which support structures such as the tonsils, the side walls of the throat, and the tongue.[4] This over-relaxation can impede normal breathing, causing the brain to briefly wake the person to reopen their airway. These awakenings are typically so short that they are not remembered. Symptoms of sleep apnea commonly include loud snoring, episodes of breathing cessation during sleep, abrupt awakenings with shortness of breath, waking up with a dry mouth or a sore throat, morning headaches, difficulty staying asleep, excessive daytime sleepiness, attention problems, and irritability. If not treated, sleep apnea can lead to various health problems, including high blood pressure, stroke, heart failure, irregular heartbeats, heart attacks, diabetes, depression, the worsening of attention deficit hyperactivity disorder (ADHD), and headaches.[1-3] The treatment for sleep apnea generally involves lifestyle changes, devices to facilitate breathing, mouthpieces, medication, or even surgery.[4] These lifestyle changes may include weight loss, smoking cessation, avoiding alcohol and sedatives, sleeping on one’s side, and regular physical activity.[4]
Skeletal Class II malocclusion is a dentofacial anomaly typified by a retrognathic mandible, a prognathic maxilla, or a simultaneous manifestation of both of these conditions.[1,2] This malformation, essentially a product of irregular maxillary and mandibular growth patterns, is known to catalyze alterations in craniofacial and upper airway morphologies.[3] Consequently, these alterations can reciprocally affect modifications in craniofacial tissues’ growth and development. Because of this interaction, it is very important to think about the shape of the upper airway when planning early treatment for skeletal Class II malocclusion. It is also noteworthy that the sagittal and vertical dimensions of the mandible and its relative positioning can influence the position of the hyoid bone.[4] For example, mandibular retrognathism can cause the hyoid bone to move backward, and turning the jaw clockwise can cause the hyoid bone to move inferiorly and posteriorly.[5]
The pathophysiology of OSA underscores the paramount importance of upper airway patency, with narrow airways being a key contributor to this disorder.[6] OSA, known to afflict over 2% of the pediatric population, can have long-term detrimental effects on health. Hence, a full check of the upper airway and the position of the hyoid bone is necessary for planning orthodontic treatment and judging how well it worked in cases of malocclusion.[7]
Among the various treatment modalities, continuous positive airway pressure (CPAP) remains the gold standard for OSA.[2] However, patient compliance with CPAP is often suboptimal due to discomfort, noise, and inconvenience.[8] Consequently, there is a growing interest in alternative treatment strategies, among which mandibular advancement devices (MADs) have emerged as a promising option.[9] By moving the lower jaw forward, MADs make the upper airway bigger and less likely to collapse, which helps people with OSA.[10] In addition to these, surgical treatment options for OSA are typically considered when non-surgical options such as lifestyle modifications, CPAP therapy, or oral appliances do not work well enough or the patient does not tolerate them. The goal of surgical treatment is to remove the obstruction in the airway that leads to sleep interruptions. There are several types of surgical procedures, each targeting different areas of the airway. One of the most common is uvulopalatopharyngoplasty,[5] which involves the removal of excess tissue from the throat, including the uvula, part of the soft palate, and, in some cases, the tonsils and adenoids. This surgery widens the airway and facilitates unobstructed breathing. In cases where large tonsils are the primary cause of OSA, particularly in children, a tonsillectomy can significantly improve or even cure the condition.[11] Various nasal surgeries can also rectify obstructions in the nasal passage, such as a deviated septum or turbinate hypertrophy. For severe cases of OSA, maxillomandibular advancement (MMA) might be considered.[1,7] This procedure, which involves moving the upper and lower parts of the jaw forward to increase the size of the airway, is invasive but is among the most effective surgical treatments for OSA. Another option is genioglossus advancement, a surgery that moves the base of the tongue forward. This enlargement of the airway reduces the chances of airway obstruction.[12] A relatively new treatment, hypoglossal nerve stimulation, involves the implantation of a device that stimulates the hypoglossal nerve, which controls the movement of the tongue. The stimulation keeps the tongue in a position that prevents it from blocking the airway.[8]
The twin-block (TB) functional appliance, traditionally employed in managing Class II skeletal patterns due to retrognathic mandible, has demonstrated efficacy in enhancing upper airway morphology and optimally repositioning the hyoid bone in pediatric and adolescent patients with retrognathic mandibular.[11] Furthermore, Invisalign mandibular advancement (MA), a new, clear functional appliance, is mostly used for people who have skeletal Class II malocclusion and mandibular retrusion.[12] Although the operational principle of the MA appliance bears resemblance to that of the TB appliance, their mechanisms of action are not identical.
In recent years, aligners, clear removable appliances, have been increasingly used for MA in OSA patients.[10,12] Aligners offer several advantages over traditional appliances, including better comfort, less oral dryness, and improved esthetics.[9,10] However, the clinical effectiveness and safety of aligners for MA in OSA patients remain uncertain, with very few studies that exist reporting mixed results. This systematic review aims to consolidate the existing literature on the use of aligners for MA in patients with OSA. Specifically, we aimed to evaluate the effectiveness of aligners in reducing OSA symptoms.
MATERIAL AND METHODS
Review protocol
The preferred reporting items for systematic reviews and meta-analysis guidelines[13] were followed in the process of making this systematic review, with the search strategy, selection criteria, bias assessment, and variable extraction all done in accordance with the stated guidelines. The study selection process for this review is represented in [Figure 1] is a representation of the study selection process for this review.
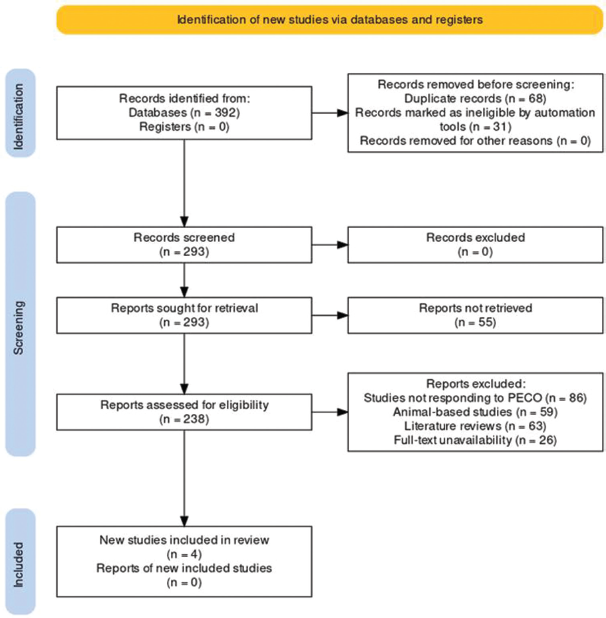
- Preferred reporting items for systematic reviews and meta-analysis protocol utilized for this review. PECO; P: patient E: exposure C: comparison O: outcome
The PECO protocol for the review “MA using aligners in patients with sleep apnea” was as follows:
Patient
Individuals diagnosed with sleep apnea of varying demographics and health backgrounds.
Exposure
The use of aligners for MA as a non-surgical orthodontic intervention to alleviate symptoms of sleep apnea.
Comparison
Although not the primary focus, a comparison was made with patients receiving alternative treatments or no treatment when such data were available.
Outcome
Effectiveness and safety of the aligner-based treatment, focusing on reduction of sleep apnea symptoms, improvement in sleep quality, and any associated adverse events.
Database search protocol
This systematic review utilized a comprehensive search strategy across eight databases: PubMed, Embase, Web of Science, Scopus, PsycINFO, CINAHL, Cochrane Library, and Google Scholar. The search strategy was designed to be exhaustive and incorporated both medical subject heading keywords and the use of Boolean operators to optimize the retrieval of relevant articles, as shown in [Table 1].
| Database | Search string |
|---|---|
| PubMed | (“Sleep Apnea, Obstructive” [MeSH] OR “sleep apnea”) AND (“Orthodontic Appliance Design” [MeSH] OR “aligners”) AND (“Mandibular Advancement” [MeSH] OR “mandibular advancement”) |
| Embase | (“Sleep apnea, obstructive”/exp OR “sleep apnea”) AND (“orthodontic appliance design”/exp OR “aligners”) AND (“mandibular advancement”/exp OR “mandibular advancement”) |
| Web of Science | TS=(“Sleep Apnea, Obstructive” OR “sleep apnea”) AND TS=(“Orthodontic Appliance Design” OR “aligners”) AND TS=(“Mandibular Advancement” OR “mandibular advancement”) |
| Scopus | (TITLE-ABS-KEY [“Sleep Apnea, Obstructive” OR “sleep apnea”] AND TITLE-ABS-KEY [“Orthodontic Appliance Design” OR “aligners”] AND TITLE-ABS-KEY (“Mandibular Advancement” OR “mandibular advancement”]) |
| PsycINFO | (AB [“Sleep Apnea, Obstructive” OR “sleep apnea”] AND AB [“Orthodontic Appliance Design” OR “aligners”] AND AB [“Mandibular Advancement” OR “mandibular advancement”]) |
| CINAHL | (MH “Sleep Apnea, Obstructive” OR TX “sleep apnea”) AND (MH “Orthodontic Appliance Design” OR TX “aligners”) AND (MH “Mandibular Advancement” OR TX “mandibular advancement”) |
| Cochrane Library | (“Sleep Apnea, Obstructive:” ti, ab, kw OR “sleep apnea”) AND (“Orthodontic Appliance Design:” ti, ab, kw OR “aligners”) AND (“Mandibular Advancement:” ti, ab, kw OR “mandibular advancement”) |
| Google Scholar | “Sleep Apnea, Obstructive” OR “sleep apnea” “Orthodontic Appliance Design” OR “aligners” “Mandibular Advancement” OR “mandibular advancement” |
MeSH: Medical subject heading
Selection criterion
The inclusion criteria were as follows: (1) Studies that included patients diagnosed with sleep apnea, regardless of the severity of the condition, age, or gender of the patients; (2) studies that evaluated the use of aligners for MA as an intervention for sleep apnea. This included both prospective and retrospective case studies, case series, cohort studies, and randomized controlled trials; (3) studies that reported at least one of the following outcomes: Reduction in symptoms of sleep apnea, improvement in sleep quality, and adverse events associated with the treatment; and (4) studies that were published in the English language.
On the contrary, the exclusion criteria were as follows: (1) Studies that included patients with sleep apnea but did not use aligners for MA as an intervention; (2) studies that did not report on any of the specified outcomes; (3) abstracts, conference presentations, editorials, commentary pieces, and reviews, as these did not provide primary data for analysis.
Data extraction
Two independent reviewers used a pre-made data extraction form to perform the data extraction. The form included fields for bibliographic information (author names, publication year), study characteristics (study design, sample size, duration of follow-up), participant information (age, gender, severity of sleep apnea), intervention specifics (type of aligner, duration of treatment), and outcome data (reduction in sleep apnea symptoms, improvement in sleep quality, adverse events). To ensure the reliability of the data extraction process, an internal reliability test was conducted. After the independent extraction of data by the two reviewers, the Cohen’s Kappa statistic was calculated. A value of 0.85 was achieved, indicating a high level of agreement between the two reviewers, thus demonstrating the reliability of the data extraction process. Any disagreements in the data extraction process were resolved by discussion and consensus, with a third reviewer consulted when necessary. The extracted data was then synthesized and analyzed to draw conclusions regarding the effectiveness and safety of MA using aligners in patients with sleep apnea.
Bias assessment
The bias assessment protocol for this review included the use of two different tools. The quality and completeness of reporting in case reports and case series were assessed using the CARE (case report) guidelines[14] for this review [Figure 2]. For observational studies, including cohort and case-control studies included in the review, the Newcastle– Ottawa scale was used[15] [Figure 3].
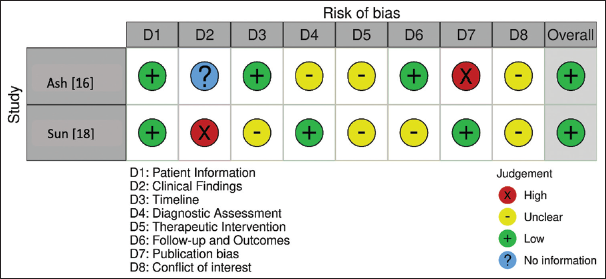
- Bias assessment protocol utilized for the case reports included in this review.
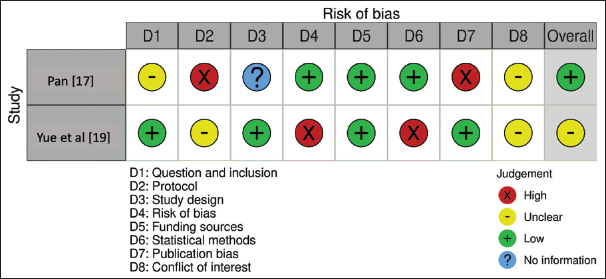
- Bias assessment protocol utilized for the retrospective studies included in this review.
RESULTS
Study selection process
In the identification phase, a comprehensive search of relevant databases yielded 392 records. However, no records were identified from the registers. To streamline the review process, duplicate records, amounting to 68, were removed. In addition, automated tools marked a number of records (31) as ineligible, which helped to further refine the database for screening. After the initial pruning, 293 records underwent screening. At this juncture, no records were excluded, leading to the retrieval of all these reports for further assessment. However, 55 reports could not be retrieved, which left 238 reports for eligibility assessment. The eligibility assessment phase entailed a meticulous review of these reports, employing the PECO framework to establish their relevance for the review. A substantial number of studies were dismissed due to various reasons: 86 studies did not respond to the PECO criteria; 59 were animal-based studies; 63 were literature reviews; and 26 were dismissed due to full-text unavailability. Following these rigorous stages of filtering and scrutiny, a total of four studies[16-19] were deemed suitable and were included in the final systematic review.
Bias assessment findings
Ash[16] had a low risk of bias in terms of patient data, timeline, and follow-up outcomes but presented no information on clinical findings. Some concerns were noted for diagnostic assessment and therapeutic intervention, while a high risk was identified for publication bias. Despite some conflicts of interest, the overall risk of bias was deemed low. Sun[18] also exhibited low risk in patient data and diagnostic assessment. However, the study showed a high risk of bias in clinical findings and some concerns in the timeline and therapeutic intervention. Follow-up outcomes were unclear, and some conflicts of interest were noted, while the risk of publication bias was low. The overall risk of bias for this study was also low.
Pan[17] had some concerns with the inclusion criteria and a high risk of bias in the protocol. Despite missing study design information, the risk of bias was low, just like for funding sources and statistical methods. However, a high risk was identified for publication bias, and there were some concerns about conflicts of interest. Overall, the study was deemed to have a low risk of bias. In contrast, Yue et al.[19] showed a low risk of bias in the question, inclusion criteria, and study design. Some concerns were noted for the protocol, while a high risk was found in the overall study bias and statistical methods. Both funding sources and publication bias carried a low risk, but some concerns were raised about conflicts of interest. The overall risk of bias was unclear.
Baseline characteristics
Two of the four studies were case reports,[16,18] each involving a single male subject aged 51 and 39-year old, respectively. These case reports offered detailed insights into individual cases but lacked a control group for comparison. The other two studies were retrospective in design,[17,19] allowing for a review of past events and the potential to establish temporal relationships. The retrospective studies incorporated a broader age range, with pediatric and adult subjects included. The study by Pan[17] encompassed a sample of 19 subjects, divided into 13 pediatric and 6 adult patients, with a gender ratio heavily skewed toward males. A control group of 8 pediatric patients was also included, enabling a comparison of outcomes between the treatment and control cohorts. The study by Yue et al.,[19] conducted in 2023, included 32 subjects, divided equally between two treatment groups, namely the MA group and the TB group. The age range of the subjects was narrower, between 8 and 11.5 years, with a predominance of male subjects [Table 2]. However, this study did not include a control group for comparison.
| Study | Year | Study design | Age range | Gender ratio | Number in treatment group | Number in control group |
|---|---|---|---|---|---|---|
| Ash[16] | 2020 | Case report | 51yearold | 1 male | 1 | N/A |
| Pan[17] | 2022 | Retrospective | 6–13 years (pediatric), 31–52 years (adult) | 10 males | 19 (13 pediatric, 6 adult) |
8 (pediatric) |
| Sun[18] | 2021 | Case report | 39year old | 1 male | 1 | N/A |
| Yue et al.[19] | 2023 | Retrospective | 8–11.5 | 15 males | 32 (16 in MA group, 16 in TB group) | N/A |
TB: Twinblock, N/A: Not Applicable
Research focus across studies
Ash[16] focused on the management of snoring and mild OSA in an individual undergoing orthodontic treatment who desired to continue using a cast chrome cobalt MAD. The treatment involved the co-utilization of a cast chrome cobalt MAD in conjunction with orthodontic aligners. The study provided a unique perspective on dual appliance use, focusing on a patient-centered approach that considered the individual’s desire to continue with a specific type of MAD while receiving orthodontic treatment. Pan[17] investigated the impact of clear aligners on the nasal airway volume and morphology. The study’s treatment modality involved the use of clear aligners for upper arch expansion. This study helped us learn more about how orthodontic devices, especially clear aligners, can change the nasal airway, which is an important part of breathing, especially for people who have breathing problems at night.
Sun[18] explored a treatment protocol involving MMA followed by post-operative sequential clear aligner (SCA) treatment. This study taught us a lot about a two-step treatment plan that combined surgery and orthodontic procedures. The goal was to make the upper airway bigger and maybe help people with sleep apnea. The goal of Yue et al.[19] was to look at and compare how the upper airway morphology and hyoid bone position changed in kids who were treated with Invisalign MA and TB appliances. Comparing two different orthodontic devices was done to see how well they changed the upper airway characteristics and the position of the hyoid bone. Both of these are important in understanding how OSA happens and how to treat it [Table 3].
| Study | Study question | Treatment | Outcome measures | Key findings |
|---|---|---|---|---|
| Ash[16] | Manage snoring and mild OSA in a patient undergoing orthodontic treatment and seeking to continue using a cast chrome cobalt MAD | Cast chrome cobalt MAD worn in conjunction with orthodontic aligners | Successful management of snoring and OSA; Continuation of orthodontic treatment; Patient satisfaction |
|
| Pan[17] | Investigate the effect of clear aligners on nasal airway volume and morphology | Clear aligners for upper arch expansion | Nasal airway volume and intermolar distance |
|
| Sun[18] | Explore the treatment protocol for MMA followed by post-operative SCA treatment | MMA followed by post-operative SCA treatment | Successful post-operative surgical outcomes; Resolution of OSA |
|
| Yue et al.[19] | Evaluate and compare improvement of upper airway morphology and hyoid bone position in children treated with Invisalign MA and TB appliances | Invisalign MA and TB appliances | Changes in upper airway morphology and hyoid bone position |
|
MAD: Mandibular advancement devices, OSA: Obstructive sleep apnea, TB: Twin-block, MA: Mandibular advancement, AHI: Apnea-Hypopnea Index, MMA: Maxillomandibular advancement, SCA: Sequential clear aligners
Outcomes discussed
The successful management of snoring and OSA, the continuation of orthodontic treatment, and patient satisfaction were all outcome measures in the study by Ash.[16] These outcomes encapsulate both clinical and subjective elements, focusing not only on the medical aspects of OSA management but also on the patient’s perspective. The results would have offered insights into the effectiveness of the treatment protocol, its impact on ongoing orthodontic care, and the patient’s overall experience and satisfaction. The study by Pan[17] considered nasal airway volume and intermolar distance as outcome measures. These parameters are significant in assessing the anatomical changes induced by clear aligners. This research would have provided valuable data on how these orthodontic appliances influence the nasal airway’s size and shape and the upper jaw’s width. Such changes might have implications for respiratory function and the management of conditions like OSA.
Sun[18] focused on successful post-operative surgical outcomes and the resolution of OSA as outcome measures. These measures are critical in assessing the efficacy of the combined MMA surgery and SCA treatment protocol. The study would have shed light on the treatment’s success rate, its impact on OSA symptoms, and the overall postoperative recovery process. The study by Yue et al.[19] evaluated changes in upper airway morphology and hyoid bone position as the primary outcomes. These outcomes are significant in understanding the impact of Invisalign MA and TB appliances on the anatomical structures involved in breathing and swallowing. Changes in these factors could have implications for the pathogenesis and treatment of sleep-related breathing disorders, such as OSA.
DISCUSSION
Ash[16] demonstrated the successful use of the Somnowell® chrome cobalt MAD in conjunction with orthodontic aligners. This was contrasted by Pan,[17] who observed that clear aligners for upper arch expansion led to a significant increase in nasal airway volume and intermolar distance, mainly in pediatric patients, suggesting that the type of appliance and the age group significantly influence the treatment outcomes. For young adults in their early twenties, non-surgical rapid maxillary expansion (RME) has been demonstrated to be a viable procedure.
Sun[18] had taken the research a step further by integrating surgery with orthodontics. Their study showed that MMA surgery followed by post-operative treatment with SCAs not only successfully managed OSA but also led to an impressive resolution rate, with an apnea-hypopnea index (AHI) of just 2.9 events/hour. This finding was significant when compared to the non-surgical interventions used in the other studies and demonstrated the potential of this integrated approach for severe OSA cases. SCAs entail careful patient selection and are less effective in addressing significant intra- and inter-dental arch discrepancies.[19] With these removable appliances, regular usage for 20–22 hours/day is required; hence, strong patient compliance is essential. Sun report outlines a typical treatment protocol for patients who meet certain criterias: (1) have OSA that is not responsive to conservative treatment or is untreatable; (2) are able to tolerate significant advancements in their maxillomandibular jaws; (3) have a stable pre-operative occlusion; (4) have mild-to-moderate dental arch malocclusion; (5) have a surgically experienced SCA team; and (6) have a high level of health awareness and good adherence to treatment.
In a different vein, Yue et al.[19] compared the effectiveness of two specific appliances: Invisalign MA and TB appliances. They found that both appliances improved upper airway morphology and reduced respiratory resistance. Interestingly, when compared to the MAD used in the Ash study, the MA and TB appliances also promoted the anterior downward movement of the hyoid bone, thus further improving airway openness.
Our review’s findings resonate with those of Conley[20] and Palomo et al.,[21] while also offering additional insights and expanding the scope of orthodontic treatments considered for OSA management. Like Conley,[20] our study found that oral appliance therapy, specifically with a cast chrome cobalt MAD and orthodontic aligners, proved successful in managing snoring and mild OSA. Our findings also align with the notion that while CPAP remains the most effective therapy, patient preference and compliance are vital in the treatment choice. We further demonstrated the effectiveness of other orthodontic appliances, such as Invisalign MA and TB appliances, in improving upper airway morphology and hyoid bone position, which were not explicitly discussed in the review by Conley.
Comparing our findings with Palomo et al.,[21] both studies underscore the crucial role of orthodontic approaches in OSA management. However, our study extends the conversation to include clear aligners for upper arch expansion and a postoperative SCA treatment protocol following MMA surgery. Palomo et al. talked about the benefits of other devices and procedures, such as headgear, functional appliances, RME, micro-implant-assisted rapid palatal expansion, and orthognathic surgery.[21] However, our study did not specifically look into these areas.
OSA susceptibility can often be traced to certain anatomical deviations, such as a diminished mandibular length and jaw retrognathia, both of which can precipitate airway obstruction due to tongue displacement.[22, 23] Among the therapeutic strategies are (1) CPAP, a relatively intrusive device that necessitates nightly utilization for efficacy yet often faces patient non-compliance owing to its noise and bulk;[23] (2) mandibular repositioning appliances that advance the jaw, thereby precluding airway obstruction;[24] and (3) surgical interventions.[25] Typically, non-surgical modalities are explored before resorting to surgical measures, yet CPAP therapy is often declined or poorly tolerated by many patients, making mandibular repositioning appliances a preferred alternative.[22]
Patients with sleep-related respiratory disorders may already be undergoing or require orthodontic intervention to rectify malocclusions.[26] It was observed that patients with severe OSA have significantly narrower upper and lower arches and shorter and more tapered maxillary arch with reduced palatal height and area.[27,28] Orthodontic correction of these conditions may create additional space for the tongue, thereby mitigating or even eliminating OSA symptoms.[22,29] However, the extended duration of orthodontic treatment can pose an obstacle to the concurrent utilization of sleep appliances. This has historically been a conundrum, necessitating the completion of orthodontic therapy before the initiation of sleep oral appliance treatment.[30] This delay can be a concern given the serious, potentially life-threatening implications of OSA and other sleep-related respiratory disorders.
In response to this challenge, many clinicians are now employing clear aligner treatments to address orthodontic malocclusions.[31] When used in conjunction with ancillary accelerators such as micro-osteoperforation and/or high-frequency vibration, these treatments offer more predictable outcomes and can expedite the orthodontic treatment process by approximately 60%, thereby addressing both the orthodontic and sleep disorder treatment needs in a more efficient and patient-friendly manner.[32]
Several similarities and differences emerge when comparing our results to those of other recent investigations[32-38] in terms of maxillary and mandibular repositioning. We found that clear aligners showed promise in improving upper airway dimensions and reducing the severity of sleep apnea symptoms. These findings were consistent with the reviews by Wu et al.,[32] and Liu et al.,[33] which also investigated the use of clear aligners for MA, although their primary focus was on the treatment of Class II malocclusions in children and adolescents.
Interestingly, the reviews by Rocha et al.[34] and Gonçalves et al.[35] provided additional insights into the potential of clear aligners to achieve dentoalveolar expansion, which can indirectly contribute to the improvement of upper airway dimensions. While these studies did not directly address sleep apnea, their findings support the notion that clear aligners can effectively modify the dental arch form, potentially leading to favorable changes in the upper airway.
However, it is important to note that the other reviews included in this comparison had different primary objectives and patient populations compared to our systematic review. For instance, the reviews by Maino et al.,[36] Manni et al.,[37] and Akbulut et al.[38] focused on the treatment of various malocclusions, such as Class II and Class III, in growing patients. These studies also investigated the use of clear aligners in combination with other orthodontic appliances and treatment modalities, such as RME and facemask therapy. In contrast, our systematic review specifically targeted adult patients with sleep apnea and evaluated the effects of MA using clear aligners as a standalone treatment.
Furthermore, the outcome measures differed between our systematic review and the other reviews. While we primarily focused on the impact of MA on sleep apnea parameters and upper airway dimensions, the other reviews assessed various dentoskeletal effects, such as changes in sagittal and vertical skeletal relationships, dental alignment, and soft tissue profile.
Certain key recommendations can be hypothesized in light of the findings obtained through this review with regard to aligner therapy in cases of OSA, a domain with very little research, as evidenced by the literature on this. For patients undergoing orthodontic treatment who also suffer from snoring or mild OSA, the use of a cast chrome cobalt MAD in tandem with orthodontic aligners can be an effective management strategy. This approach not only addresses the symptoms of snoring and OSA but also allows the continuation of necessary orthodontic treatment without interruption. Clear aligners, particularly when used for upper arch expansion, can have a positive impact on nasal airway volume and morphology. This is especially significant in pediatric patients, where the effect was found to be more pronounced. However, a similar trend was observed in adult patients, albeit to a lesser degree, suggesting that this strategy may also be beneficial for them.
In cases where MMA surgery is performed to treat OSA, post-operative treatment with SCAs may be a viable protocol for maintaining the success of the surgical outcome. This approach has been demonstrated to effectively resolve OSA symptoms while ensuring successful post-operative orthodontic treatment. Both Invisalign MA and TB appliances were also found effective in improving the upper airway morphology and the position of the hyoid bone in children. These appliances can alleviate structural narrowness in the upper airway and reduce respiratory resistance, thereby enhancing breath quality. Furthermore, the MA appliance specifically showed superior efficacy in improving the narrowest part of the hypopharynx compared to the TB appliance. The hyoid bone could move forward and downward with the help of both appliances. This opened the upper airways in the oropharynx and hypopharynx and helped return the shape of the upper airways to normal.
Limitations
Despite the substantial insights garnered from this investigation, certain limitations were inherent in the research design and execution that may have potentially influenced the findings. First, the study involved the use of several different orthodontic treatments and appliances, each with its own range of variables and potential effects. This heterogeneity made it challenging to establish direct comparisons or to isolate the impact of each treatment modality. Second, the study did not explicitly account for individual patient variations such as age, severity of OSA, comorbidities, and anatomical differences. These factors can significantly influence both the presentation of OSA and the response to treatment, potentially confounding the study results. Particularly, the differential impact of clear aligners on nasal airway volume in pediatric and adult patients underscored the importance of considering age as a critical variable. Furthermore, the study did not explore long-term outcomes or track the sustainability of treatment effects beyond the immediate post-treatment period. The long-term efficacy and potential side effects of these orthodontic interventions remain unknown, limiting the applicability of the findings for the chronic management of OSA. This review also used certain outcome measures, such as nasal airway volume, upper airway morphology, and hyoid bone position, which are important but do not cover all the factors that are important for managing OSA. A more comprehensive assessment incorporating other parameters such as patient compliance, quality of life, sleep quality, and cardiovascular outcomes could have provided a more holistic understanding of the effects of these orthodontic treatments on OSA.
CONCLUSION
According to our findings, clear aligners have shown potential in managing OSA through MA. A cast chrome cobalt MAD and orthodontic aligners effectively treated snoring and mild OSA while permitting orthodontic treatment. Both Invisalign MA and TB appliances improved upper airway morphology and hyoid bone location, although MA more effectively improved the narrowest hypopharynx. These data imply that clear aligners, especially MA ones, may help manage OSA.
Ethical approval
Institutional Review Board approval is not required.
Declaration of patient consent
Patient’s consent is not required as there are no patients in this study.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship: Nil.
References
- Three-dimensional analysis of mandibular characteristics in patients with skeletal Class II malocclusion and chin deviation. Am J Orthod Dentofacial Orthop. 2021;160:392-400.
- [CrossRef] [PubMed] [Google Scholar]
- Obstructive sleep apnea in adults. N Engl J Med. 2019;380:1442-9.
- [CrossRef] [PubMed] [Google Scholar]
- Impact of continuous positive airway pressure (CPAP) on quality of life in patients with obstructive sleep apnea (OSA) J Sleep Res. 2016;25:731-8.
- [CrossRef] [PubMed] [Google Scholar]
- The effect of orthodontic vertical control on the changes in the upper airway size and tongue and hyoid position in adult patients with hyperdivergent skeletal class II. BMC Oral Health. 2022;22:532.
- [CrossRef] [PubMed] [Google Scholar]
- Anatomical determinants of upper airway collapsibility in obstructive sleep apnea: A systematic review and meta-analysis. Sleep Med Rev. 2023;68:101741.
- [CrossRef] [PubMed] [Google Scholar]
- Role of surgical hyoid bone repositioning in modifying upper airway collapsibility. Front Physiol. 2022;13:1089606.
- [CrossRef] [PubMed] [Google Scholar]
- Hyoid bone position as an indicator of severe obstructive sleep apnea. BMC Pulm Med. 2022;22:349.
- [CrossRef] [PubMed] [Google Scholar]
- Mandibular advancement with clear aligners in the treatment of skeletal Class II. A retrospective controlled study. Eur J Paediatr Dent. 2021;22:26-30.
- [Google Scholar]
- Comparison of airway space with conventional lateral headfilms and 3-dimensional reconstruction from cone-beam computed tomography. Am J Orthod Dentofacial Orthop. 2009;135:468-79.
- [CrossRef] [PubMed] [Google Scholar]
- Three-dimensional tomographic assessment of the upper airway using 2 different imaging software programs: A comparison study. Am J Orthod Dentofacial Orthop. 2021;159:217-23.
- [CrossRef] [PubMed] [Google Scholar]
- Asthma and obstructive sleep apnoea in adults and children-an up-to-date review. Sleep Med Rev. 2022;61:101564.
- [CrossRef] [PubMed] [Google Scholar]
- Pharyngeal airway, hyoid bone, and soft palate changes after Class II treatment with Twin-block and Forsus appliances during the postpeak growth period. Am J Orthod Dentofacial Orthop. 2021;159:148-57.
- [CrossRef] [PubMed] [Google Scholar]
- The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ. 2021;372:n71.
- [CrossRef] [PubMed] [Google Scholar]
- CARE guidelines for case reports: Explanation and elaboration document. J Clin Epidemiol. 2017;89:218-35.
- [CrossRef] [PubMed] [Google Scholar]
- Newcastle-Ottawa Scale: Comparing reviewers' to authors' assessments. BMC Med Res Methodol. 2014;14:45.
- [CrossRef] [PubMed] [Google Scholar]
- A chrome cobalt mandibular advancement appliance for snoring and obstructive sleep apnoea used during active aligner orthodontic treatment. J Orthod. 2020;47:181-4.
- [CrossRef] [PubMed] [Google Scholar]
- The effect of upper arch expansion by clear aligners on nasal airway volume in children and adults (Master's thesis) University of Alberta;.
- [Google Scholar]
- Surgery-first maxillomandibular advancement for obstructive sleep apnea with post-operative sequential clear aligner orthodontic treatment. Preprints; 2021
- [CrossRef] [Google Scholar]
- Comparison of invisalign mandibular advancement and twin-block on upper airway and hyoid bone position improvements for skeletal class II children: A retrospective study. BMC Oral Health. 2023;23:661.
- [CrossRef] [PubMed] [Google Scholar]
- Management of sleep apnea: A critical look at intra-oral appliances. Orthod Craniofac Res. 2015;18(Suppl 1):83-90.
- [CrossRef] [PubMed] [Google Scholar]
- Obstructive sleep apnea: A review for the orthodontist. Dental Press J Orthod. 2023;28:e23spe1.
- [CrossRef] [PubMed] [Google Scholar]
- Orthodontic view in the diagnoses of obstructive sleep apnea. J Orthod Sci. 2017;6:81-5.
- [CrossRef] [PubMed] [Google Scholar]
- Oral appliances for the treatment of snoring and obstructive sleep apnea: A review. Sleep. 1995;18:501-10.
- [CrossRef] [PubMed] [Google Scholar]
- Effect of micro-osteoperforations on the rate of tooth movement. Am J Orthod Dentofacial Orthop. 2013;144:639-48.
- [CrossRef] [PubMed] [Google Scholar]
- Vibratory stimulation increases interleukin-1 beta secretion during orthodontic tooth movement. Angle Orthod. 2016;86:74-80.
- [CrossRef] [PubMed] [Google Scholar]
- VPro5™ More efficient aligner seating with high-frequency vibration. Orthod Pract US. 2016;7:5.
- [Google Scholar]
- Correlation between dental arch form and OSA severity in adult patients: An observational study. Prog Orthod. 2023;24:19.
- [CrossRef] [PubMed] [Google Scholar]
- Maxillary morphology in obstructive sleep apnoea syndrome. Eur J Orthod. 2001;23:703-14.
- [CrossRef] [PubMed] [Google Scholar]
- Clinical practice guideline for the treatment of obstructive sleep apnea and snoring with oral appliance therapy: An update for 2015. J Clin Sleep Med. 2015;11:773-827.
- [CrossRef] [PubMed] [Google Scholar]
- Osteogenic effect of high frequency acceleration on alveolar bone. J Dent Res. 2012;91:413-9.
- [CrossRef] [PubMed] [Google Scholar]
- High-frequency acceleration: Therapeutic tool to preserve bone following tooth extraction. J Dent Res. 2016;95:311-8.
- [CrossRef] [PubMed] [Google Scholar]
- Does mandibular advancement with clear aligners have the same skeletal and dentoalveolar effects as traditional functional appliances? BMC Oral Health. 2023;23:65.
- [CrossRef] [PubMed] [Google Scholar]
- Functional clear aligner technique in the treatment of class II malocclusion in juvenile: A case report and literature review. J Radiat Res Appl Sci. 2022;15:59-64.
- [CrossRef] [Google Scholar]
- Efficiency and predictability of coronal maxillary expansion repercussion with the aligners system: A retrospective study. Dent J (Basel). 2023;11:258.
- [CrossRef] [PubMed] [Google Scholar]
- Efficiency of Invisalign First® to promote expansion movement in mixed dentition: A retrospective study and systematic review. Eur J Paediatr Dent. 2023;24:112-23.
- [Google Scholar]
- Long-term skeletal and dentoalveolar effects of hybrid rapid maxillary expansion and facemask treatment in growing skeletal Class III patients: A retrospective follow-up study. Prog Orthod. 2022;23:44.
- [CrossRef] [PubMed] [Google Scholar]
- Is significant mandibular advancement possible after the peak of puberty? Dento-osseous palatal expansion and the STM4 technique (Skeletal Therapy Manni Telescopic Herbst 4 miniscrews): A case report. Int Orthod. 2024;22:100868.
- [CrossRef] [PubMed] [Google Scholar]
- Comparison of the short-term effects of facemask therapy preceded by conventional rapid maxillary expansion or by an alternate rapid maxillary expansions and constrictions protocol: A retrospective study. J Orofac Orthop. 2023;84:278-86.
- [CrossRef] [PubMed] [Google Scholar]




