

Translate this page into:
Preliminary study: Evaluating the reliability of cone-beam computed tomography images for upper airway volume in orthodontics
 , Mohammad Zeinalddin2, Himawan Halim3, Krisna Fery Rahmantya4, Ani Melani Maskoen5, Ganesha Wandawa6, Endah Mardiati7
, Mohammad Zeinalddin2, Himawan Halim3, Krisna Fery Rahmantya4, Ani Melani Maskoen5, Ganesha Wandawa6, Endah Mardiati7

*Corresponding author: Ivan A. Halim, Doctoral Program, Faculty of Dentistry, Padjadjaran University, Bandung, Indonesia. ivan20003@mail.unpad.ac.id
-
Received: ,
Accepted: ,
How to cite this article: Halim IA, Zeinalddin M, Halim H, Rahmantya KF, Maskoen AM, Wandawa G, et al. Preliminary study: Evaluating the reliability of cone-beam computed tomography images for upper airway volume in orthodontics. APOS Trends Orthod. doi: 10.25259/APOS_216_2024
Abstract
Objectives:
The primary aim of this study was to evaluate the reliability of cone-beam computed tomography (CBCT) in measuring upper airway volume in orthodontics. The secondary aim was to compare the upper airway volumes between laypeople and military personnel (physically fit individuals).
Material and Methods:
This study included 36 male participants aged 21–29 years who had no upper airway pathology or history of upper airway surgery. CBCT scans had been previously obtained as part of routine dental checkups using a standardized protocol by the same operator. The digital imaging and communications in the medicine files of the subjects were imported into the 3D analysis software SimPlant® 17 Pro (Materialize Dental, Leuven, Belgium) to facilitate the measurement of upper airway volume. The upper airway volume was divided into three sections and measured on days 0 and 14 by the same operator. The intrarater intra-class correlation coefficient (ICC) and Bland-Altman plot were used to assess reliability. The upper airway volumes of the laypeople and military personnel were compared using Tukey’s pairwise test.
Results:
The variables demonstrated excellent reliability across all sections of the upper airway; the Superior part of the upper airway has an ICC of 0.993, the middle part of the upper airway has an ICC of 0.995, and the inferior part of the upper airway has an ICC of 0.989. The ICC for the entire upper airway was 0.987. The intrarater plot for superior airway measurement showed that 8 out of 8 measurements (100%) fell within the limits of agreement. Similarly, the intrarater plot for the middle airway measurements indicated that 8 out of 8 measurements (100%) fell within the limits of agreement. For inferior airway measurement, the intrarater plot revealed that 7 out of 8 measurements (87.5%) fell within the limits of agreement. No significant differences were found between the upper airway volumes of the laypeople and military personnel.
Conclusion:
Preliminary evidence suggests that CBCT using a standardized protocol is reliable for measuring upper airway volume. Separating the upper airway into three different parts also demonstrated high reliability and reproducibility among the raters. The ability to accurately measure the upper airway enhances the evaluation of the effects of orthodontic treatment by comparing the pre-and post-upper airway volume.
Keywords
Upper airway volume
Cone-beam computed tomography
Reliability
Orthodontics
Airway measurement

INTRODUCTION
The upper airway is a crucial part of the human body, comprising the pharyngeal airway, nasal cavity, and oral cavity. The pharyngeal airway is divided into the nasopharynx, oropharynx, and hypopharynx.[1,2] The upper airway interests many specialists, including Ear, Nose, and Throat doctor (ENT) or (otolaryngologists), cardiologists, pulmonologists, craniofacial orthodontists, dental sleep medicine specialists, and oral and maxillofacial surgeons.[3] For orthodontists, the upper airway is particularly significant due to its direct link with craniofacial growth and development.[4] Upper airway obstruction alters breathing and may affect normal growth and development, leading to changes in dentofacial morphology.[4,5] Chronic mouth breathing can hinder mandibular growth, causing mandibular retrusion and an imbalanced facial profile. Mouth breathers may also experience long-term effects, such as behavioral issues and serious health implications.[6]
Since the late 1990s and early 2000s, cone-beam computed tomography (CBCT) has made the three-dimensional evaluation of the upper airway has become easier.[7] Before CBCT, the airway was evaluated two-dimensionally using a lateral cephalogram, a method introduced by Broadbent et al. in 1930.[8-10] In its early days, CBCT images lacked high quality. It took several years for the technology to reach its current state. CBCT is now preferred by both patients and practitioners because it offers a lower radiation dosage than medical computed tomography (CT) scans and is more affordable.[7,11]
The reliability of CBCT has been confirmed in several head and neck anatomical areas. A systematic review in 2016 to assess the reliability of upper pharyngeal airway evaluations using dental CBCT.[12] Out of 42 studies reviewed through 2015, only five were reported to be of maximum quality. Many studies did not assess the entire upper pharyngeal airway and did not follow the standard protocol when obtaining CBCT images. CBCT imaging requires a standardized protocol. Minor head movement and different tongue positions resulted in significant differences in volume readings and reduced measurement accuracy.[13,14] This study used a standardized protocol for all CBCT images. The reliability of the CBCT protocol was evaluated by good-to-excellent intra- and interrater examiners.[15]
Most published papers did not evaluate CBCT reliability in the nasal cavity. Recent studies have attempted to assess the nasal cavity using CBCT images.[16] For orthodontics, the entire upper airway, from the pharyngeal airway to the nasal cavity, should be the area of interest. Many controversial claims exist regarding the effects of orthodontic treatment on the upper airway. Treatments such as extraction, expansion, and orthognathic surgery may affect the upper airway.[17] Having a tool to evaluate pre- and post-treatment differences will improve the quality of treatment provided to patients. At present, most studies evaluating treatment effects on the airways rely on lateral cephalograms.[18]
The purpose of this study was to find upper airway landmarks that provide acceptable intrarater reliability and to evaluate CBCT reliability in measuring upper airway volume. The study also compared the upper airway volumes of laypeople and military personnel. This comparison helps determine if healthy military personnel have a larger upper airway volume than laypeople who do not exercise. Reliable CBCT of the upper airway allows orthodontists to evaluate changes in the airway pre-and post-treatment.
MATERIAL AND METHODS
The goal of this study was to identify the upper airway landmark that provided acceptable intrarater reliability and to determine whether the upper airway volumes of laypersons and healthy military personnel were significantly different. This study was a small component of a larger study. The study design was reviewed and approved by the Research Ethics Committee of Padjadjaran University (registration number: 2211051399). All procedures were followed in accordance with the ethical standards of the responsible committee on human experimentation and with the Helsinki Declaration. CBCT data were existing data images, and all personal identifiers were removed.
Subjects and calculation of sample size
The subjects included 30 Indonesian male marines and six Indonesian male laypeople of the Deutromalay race. The sample size was calculated using the formula n = [(Zα/2 + Z β)2 × {(p1 (1-p1) + (p2 (1-p2))}]/(p1 – p2)2. n is the total number of subjects, p1 and p2 are the group proportion, Zα/2 is the significance level, and Zβ is the power level. The inclusion criteria for the subjects were male aged 21–29 years, healthy physically and mentally, do not have any systemic disease, Deutromalay race (two-generation), Class I malocclusion, normal (1–3 mm) overjet/overbite, none-to-mild crowding (<4 mm), no craniofacial syndrome, no upper airway pathology, no history of head and facial trauma and no history of orthognathic surgery or surgery around upper airway. Additional inclusion criteria for the laypeople included engaging in routine exercise no more than once a week. Since this study is a small part of a larger research, the 30 male marines (military personnel) were randomly divided into three different groups, 10 personnel each.
CBCT scans
A CBCT scan was taken as part of the routine dental checkup using a standardized protocol by the same operator.
The CBCT images were captured using Dentsply Sirona Orthophos S 3D (Charlotte, North Carolina, USA) with the “3D setting” to provide the necessary field of view to capture the upper airway. The volume size of the scan was 11 × 10 cm, with a voxel size of 0.3 mm, a scan time of 14.4 s, and a peak kilovoltage of 85 kV. The CBCT was performed with the Frankfort horizontal plane (orbitale to the porion) parallel to the floor. The subjects were asked to perform maximum intercuspation and place their tongue in the anterosuperior position, just lingual to the maxillary teeth. The subjects were then instructed to take a deep breath, exhale, and hold their breath after the end of expiration without swallowing while the CBCT image was taken. This protocol allows for static imaging of the upper airway and minimizes the variables caused by changes in the upper airway during the respiratory cycle and swallowing.[19,20]
Definition of anatomic landmarks and 3D image analysis
The digital imaging and communications in medicine (DICOM) files of the subjects were imported into the 3D analysis software SimPlant® 17 Pro (Materialize Dental, Leuven, Belgium) to facilitate the measurement of upper airway volume. Before analyzing the CBCT images, the orientation of the head was corrected using three different planes: Frankfort horizontal (plane through the left and right porions and the orbitale), midsagittal (plane through the posterior nasal spine [PNS], and parallel to the Frankfort horizontal (FH) plane), and transporionic (plane through the porion and perpendicular to the FH plane). Landmarks were established for the upper airway. To increase accuracy, the upper airway measurement was divided into three parts: Superior, middle, and inferior. The superior portion includes the nasal cavity and the volume from the PNS to the roof of the nasal cavity. The middle portion comprises the airway volume between the PNS and the plane through the inferior point of the soft palate (P-plane). The inferior portion of the upper airway is the space between the P-plane and epiglottis. Overall, the total upper airway is superior to the hyoid bone and epiglottis (most anteroinferior point of the third cervical vertebra) and extends to the roof of the nasal cavity [Figure 1].
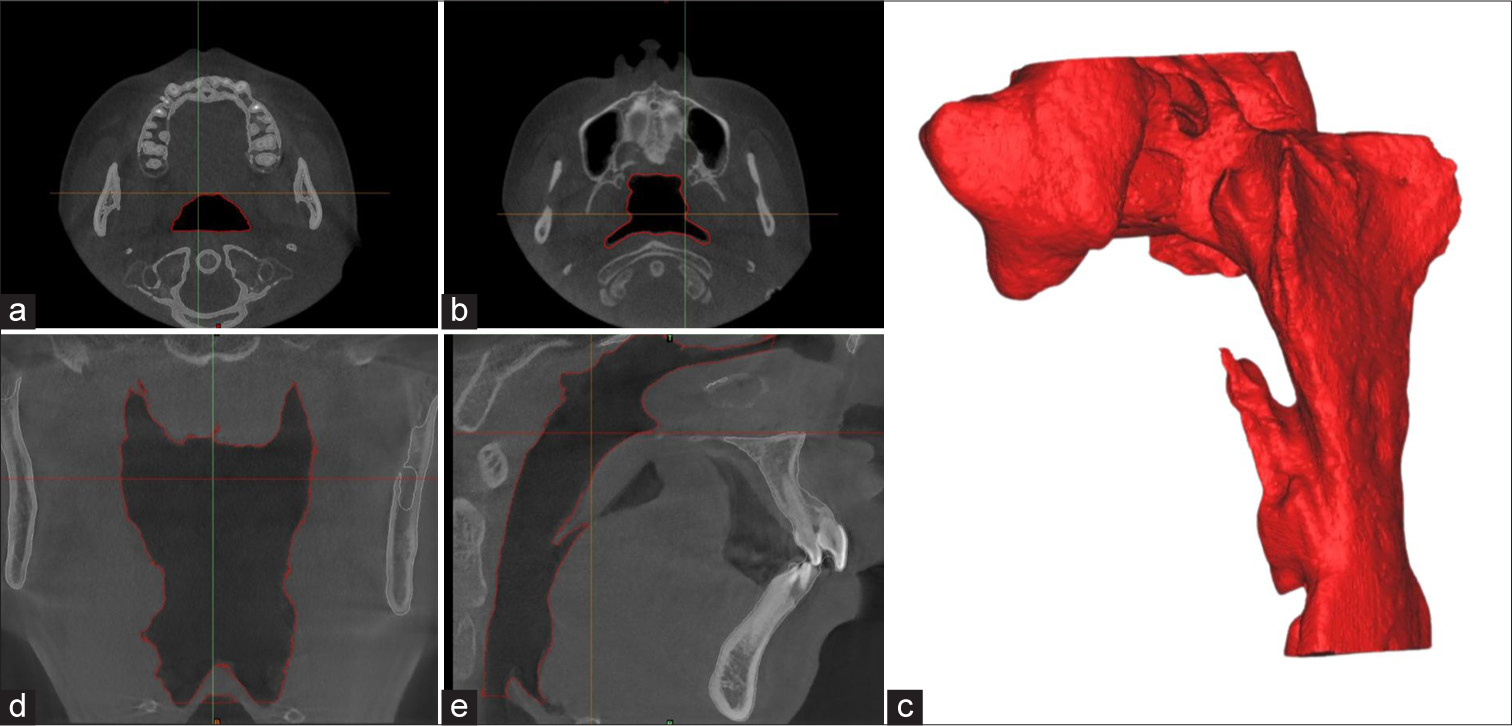
- (a) Axial slice of the middle part of the upper airway. (b) Axial slice of the superior part of the upper airway. (c) Total upper airway volume after segmentation. (d) Corona slice of the upper airway. (e) Sagittal slice of the upper airway.
Data collection
One orthodontist Mohammad Zeinalddin (MZ) collected the data. MZ has extensive training with the 3D image analysis software SimPlant® 17 Pro (Materialize Dental, Leuven, Belgium). MZ analyzed the DICOM files of 36 subjects (30 military personnel and six laypeople) [Figure 2]. To evaluate intrarater reliability, landmarks from eight subjects (six military personnel and two laypeople) were removed. Fourteen days after completing the analysis of the 36 subjects, the landmarks of eight subjects were replaced and measured for the 2nd time.
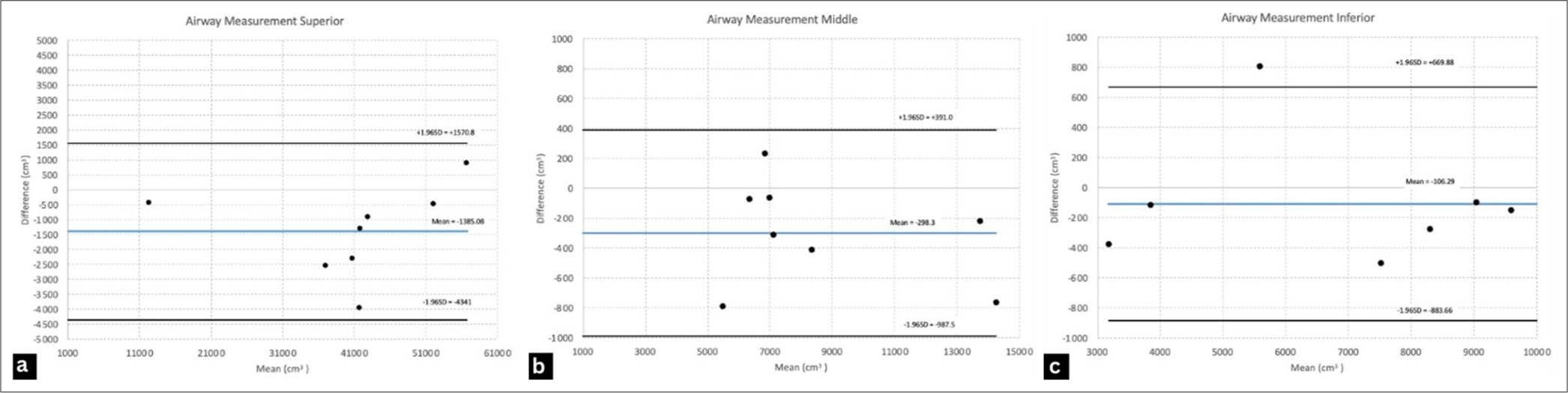
- Bland-Altman plots (cm3) for intra-rater airway measurements of cone-beam computed tomography day 0 and day 14 of 8 subjects (6 military personnel and two lay people). (a) Superior airway (b) Middle airway (c) Inferior airway.
Statistical analysis
Data were analyzed using the Statistical Package for the Social Sciences version 28 (IBM Corporation, Armonk, New York, USA). A reliability analysis was performed to assess the level of agreement across time points using a two-way random-effects model. The intrarater intra-class correlation coefficient (ICC) estimates the level of reliability, which varies between 0 and 1. Values below 0.5 indicate poor reliability, 0.5–0.75 indicates moderate reliability, 0.75–0.90 indicates good reliability, and 0.90 indicates excellent reliability.[21,22]
A Bland-Altman plot was used to assess further and visualize the agreement of the measurements.[21,23] The plot evaluated the bias between the mean measurement differences and agreement intervals within 95% between the two measurements. The X-axis on the Bland-Altman plot represents the average between the two measurements, while the Y-axis shows the differences between the two paired measurements. It is recommended that 95% of the data points fall within ±1.96 Standard deviation (SD) of mean differences.[24]
To compare significant differences in the upper airways between laypeople and military personnel, Tukey’s pairwise test was used. Tukey’s pairwise analysis was based on the t-distribution.[25] The tukey test determined whether there were any differences between the two groups.
RESULTS
[Table 1] shows the ICCs for intrarater reliability when comparing the measurements of CBCT scans on days 0 and day 14. The variables showed excellent reliability for all parts of the upper airway; the superior, middle, and inferior parts of the upper airway had ICC of 0.993, 0.995, and 0.989, respectively. The ICC for the entire upper airway was 0.987.
| Reliability measurement | Intraclass correlation | 95% Confidence interval | |
|---|---|---|---|
| Lower bound | Upper bound | ||
| Superior Part | 0.993 | 0.968 | 0.999 |
| Middle Part | 0.995 | 0.974 | 0.999 |
| Inferior Part | 0.989 | 0.945 | 0.998 |
| Total Upper Airway | 0.987 | 0.939 | 0.997 |
[Figure 2] provides the Bland-Altman charts for reading on days 0 and 14 for intrarater reliability of the superior, middle, and inferior airway measurements. The intrarater plot for superior airway measurement showed that 8 out of 8 measurements (100%) fell within the limits of agreement. The intrarater plot for the middle airway measurements showed that 8 out of 8 measurements (100%) fell within the limits of agreement. The intrarater plot for inferior airway measurement showed that 7 of 8 measurements (87.5%) fell within the limits of agreement.
[Table 2] shows a Tukey pairwise comparison of the upper airways between laypeople and military personnel. Thirty military personnel were divided into three groups for the main study. Based on these results, there were no differences between the upper airway volumes of laypeople and military personnel.
| Upper airway section | Group | 95% confidence interval | P-value | |
|---|---|---|---|---|
| Lower Bound | Upper Bound | |||
| Superior | Group 4 – Group 1 | −19478 | 21928 | 0,999 |
| Group 4 – Group 2 | −24898 | 16508 | 0,946 | |
| Group 4 – Group 3 | −20346 | 21059 | 1,000 | |
| Middle | Group 4 – Group 1 | −2803 | 8471 | 0,532 |
| Group 4 – Group 2 | −3633 | 7641 | 0,771 | |
| Group 4 – Group 3 | −2328 | 8946 | 0,399 | |
| Inferior | Group 4 – Group 1 | −2350 | 8086 | 0,456 |
| Group 4 – Group 2 | −5591 | 4845 | 0,997 | |
| Group 4 – Group 3 | −3147 | 7290 | 0,707 | |
| Total | Group 4 – Group 1 | −8924 | 22778 | 0,380 |
| Group 4 – Group 2 | −18416 | 13287 | 0,744 | |
| Group 4 – Group 3 | −10114 | 21588 | 0,466 | |
Group 1, Group 2, Group 3: Military, Group 4: Laypeople
DISCUSSION
The objective of this study was to evaluate the reliability of CBCT images taken using a standardized protocol for the evaluation of upper airway volume. The second objective of this study was to determine whether there is a difference between the upper airways of military personnel and those of laypeople. The upper airway is of interest to many specialties, such as orthodontists, surgeons, cardiologists, pulmonologists, ENT, and sleep medicine professionals. In the field of orthodontics, an increasing number of studies on the upper airways have been conducted.[11,26] The availability of CBCT in the dental field also allows more research to be conducted.[26] Radiation cost is very low, and it is cheaper than medical CT and magnetic resonance imaging.[27] The three-dimensional analysis is more accurate than two-dimensional analysis, particularly when comparing pre-and post-treatments. Three-dimensional (3D) software has also continued to improve, allowing researchers to measure and analyze 3D craniofacial anatomy more precisely.[28]
A systematic review of the reliability of upper pharyngeal airway assessment using dental CBCT was conducted. The limitations of many studies include not standardizing the image-capturing protocol, standardizing the image orientation for segmentation, and not determining the reliability of each part of the airway.[12] This study used a standardized protocol to capture CBCT images. Minor head posture changes, tongue posture, and position differences affect the accuracy of the measurement and result in analytical challenges.[13,26] Patient swallowing and breathing also affect upper airway volume.[14,29,30] All these movements change the hyoid level, leading to changes in the upper airway volume. The same protocol was used to evaluate the reliability of CBCT to measure tongue space and had good intrarater (0.75–90) and excellent interrater (>0.90) reliability. About 90–95% of the total measurements fell within the 95% limits of agreement for both intra- and interrater pairs.[15]
Studies have also shown that CBCT images are highly variable and lack a harmonious reproduction.[31] Image analysis in this study was also carried out using a standardized protocol for image orientation before segmentation. Three planes (Frankfort, midsagittal, and transporionic) were used to ensure reproducibility. The anatomy and landmarks of the upper airway were selected to reduce variability. The upper airway is divided into three sections: superior, middle, and inferior.
The method proposed in this study using orientation and anatomical landmarks suggests that the upper airway volume can be measured reliably using CBCT imaging. Reliability was assessed using the ICC and Bland-Altman methods. The intrarater ICC showed excellent reliability in all parts of the upper airway. Even if the ICC values are excellent, they may hide clinically important measurement errors.[32] Bland-Altman plot agrees with the results, showing that both the superior and middle parts of the upper airway showed a 100% fall within the SD. One of the inferior parts of the upper airway did not fall within the SD. This may be due to interference of the epiglottis in the airway, causing a measurement error.[32,33]
The high reliability showed that CBCT could be used to evaluate the upper airway volume. The second objective was to compare the upper airways of laypersons and military personnel. Military personnel completed daily training exercises. It is beneficial to see whether there is a difference between the upper airway volume of someone who exercises daily and someone who rarely and does not exercise at all. The superior part of the upper airway (nasal cavity) of military personnel is larger than that of laypeople, whereas the middle and inferior parts of the upper airway of military personnel are smaller than those of laypeople. The overall volume of the upper airways was approximately the same. There were no significant differences in the upper airway volume between laypeople and military personnel or those who exercised on a daily basis.
This finding suggests that upper airway volume is just one factor in evaluating the overall health of a person. The upper airway includes the nasopharynx, oropharynx, and hypopharynx.[1] The upper airway is important for health because it helps people inhale oxygen and exhale carbon dioxide while filtering dangerous microorganisms and bacteria.[3] A healthy upper airway helps stabilize acidic levels in the body. In addition, a good upper airway can improve a person’s quality of life. Overall, upper airway dynamics, such as airway pressure, air velocity, aerodynamic forces, and flow resistance, should be evaluated.[34,35]
Pre- and post-treatment upper airway volumes should be evaluated with high reliability. At present, there are many controversies regarding upper airway changes due to orthodontic treatments and products. Many researchers believe that extraction leads to airway constriction and increases sleep apnea. Hu et al. attempted to gather evidence regarding this controversy and concluded that there was insufficient evidence.[17] Guo et al. gathered data on the effect of premolar extraction and only found 12 studies; the results still need to be interpreted with caution, and further high-quality studies need to be completed.[36]
This is a preliminary study. Further studies with more participants are required to increase the validity of these results. The number of laypeople should be increased. The CBCT protocol was recently implemented, and not enough subjects (laypeople) that met the inclusion criteria. Interrater reliability should also be studied to ensure that there is no bias in the results. The protocol for taking and evaluating the CBCT images has been used in several studies and has been published previously. It has high interrater and intrarater reliabilities.
In summary, this study provides preliminary evidence that CBCT with a standardized protocol is reliable for measuring the upper airway volume. A standardized protocol is required to reduce variability and increase measurement accuracy. The findings showed that separating the upper airway into three different parts showed high reliability and reproducibility. The ability to measure the upper airway better evaluates the effects of orthodontic treatment by comparing the pre-and post-upper airway volumes.
CONCLUSION
Preliminary findings suggested that having a standardized protocol for taking CBCT images of the upper airway leads to high reliability and reproducibility among raters. The ability to use CBCT to accurately measure the upper airway will enable orthodontists to compare pre-and post-treatment upper airway volume.
Acknowledgment
The authors would like to thank the Center Study for Military Dentistry, Faculty of Dentistry, Padjadjaran University, Bandung, for providing resources and Dr. R Curtis Bay of A.T. Still University, Mesa, AZ, USA, for providing help with the statistical analysis. The authors would like to thank Editage (www.editage.com) for English language editing.
Ethical approval
The study design was reviewed and approved by the Padjadjaran University Research Ethics Committee (Registration number: 2211051399).
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- Comparative analysis of upper airway volume with lateral cephalograms and cone-beam computed tomography. Am J Orthod Dentofacial Orthop. 2015;147:197-204.
- [CrossRef] [PubMed] [Google Scholar]
- Three-dimensional analysis of pharyngeal airway in preadolescent children with different anteroposterior skeletal patterns. Am J Orthod Dentofacial Orthop. 2010;137:306.e1-11.
- [CrossRef] [PubMed] [Google Scholar]
- Airway growth and development: A computerized 3-dimensional analysis. J Oral Maxillofac Surg. 2012;70:2174-83.
- [CrossRef] [PubMed] [Google Scholar]
- Craniofacial growth: Current theories and influence on management. Oral Maxillofac Surg Clin North Am. 2020;32:167-75.
- [CrossRef] [PubMed] [Google Scholar]
- Nasal airway measurements in children treated by rapid maxillary expansion. Am J Rhinol. 2006;20:385-93.
- [CrossRef] [PubMed] [Google Scholar]
- Effects of mouth breathing on facial skeletal development in children: A systematic review and meta-analysis. BMC Oral Health. 2021;21:108.
- [CrossRef] [PubMed] [Google Scholar]
- Operational principles for cone-beam computed tomography. J Am Dent Assoc. 2010;141(Suppl 3):3S-6.
- [CrossRef] [PubMed] [Google Scholar]
- Value-addition of lateral cephalometric radiographs in orthodontic diagnosis and treatment planning. Angle Orthod. 2020;90:665-71.
- [CrossRef] [PubMed] [Google Scholar]
- Comparative dosimetry of dental CBCT devices and 64-slice CT for oral and maxillofacial radiology. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2008;106:106-14.
- [CrossRef] [PubMed] [Google Scholar]
- Cone-beam computed tomography and radiographs in dentistry: Aspects related to radiation dose. Int J Dent. 2012;2012:813768.
- [CrossRef] [PubMed] [Google Scholar]
- Reliability of upper pharyngeal airway assessment using dental CBCT: A systematic review. Eur J Orthod. 2017;39:489-96.
- [CrossRef] [PubMed] [Google Scholar]
- Cone-beam computed tomography airway measurements: Can we trust them? Am J Orthod Dentofacial Orthop. 2019;156:53-60.
- [CrossRef] [PubMed] [Google Scholar]
- Head posture and hyo-mandibular function in man. A synchronized electromyographic and videofluorographic study of the open-close-clench cycle. Am J Orthod Dentofacial Orthop. 1988;94:393-404.
- [CrossRef] [PubMed] [Google Scholar]
- Preliminary study: Evaluating the reliability of CBCT images for tongue space measurements in the field of orthodontics. Oral Radiol. 2021;37:256-66.
- [CrossRef] [Google Scholar]
- Evaluation of the average nasal and nasopharyngeal volume in 10-13-year-old children: A preliminary CBCT study. Int J Clin Pediatr Dent. 2021;14:187-91.
- [CrossRef] [PubMed] [Google Scholar]
- The effect of teeth extraction for orthodontic treatment on the upper airway: A systematic review. Sleep Breath. 2015;19:441-51.
- [CrossRef] [PubMed] [Google Scholar]
- Changes in upper airway anatomy following orthodontic treatment for malocclusion: A comparative retrospective study in 96 patients. Med Sci Monit. 2023;29:e941749.
- [CrossRef] [PubMed] [Google Scholar]
- Tongue posture improvement and pharyngeal airway enlargement as secondary effects of rapid maxillary expansion: A cone-beam computed tomography study. Am J Orthod Dentofacial Orthop. 2013;143:235-45.
- [CrossRef] [PubMed] [Google Scholar]
- Use of 3-dimensional computed tomography scan to evaluate upper airway patency for patients undergoing sleep-disordered breathing surgery. Otolaryngol Head Neck Surg. 2003;129:336-42.
- [CrossRef] [Google Scholar]
- A Guideline of selecting and reporting intraclass correlation coefficients for reliability research. J Chiropr Med. 2016;15:155-63.
- [CrossRef] [PubMed] [Google Scholar]
- Estimation of an inter-rater intra-class correlation coefficient that overcomes common assumption violations in the assessment of health measurement scales. BMC Med Res Methodol. 2018;18:93.
- [CrossRef] [PubMed] [Google Scholar]
- Statistical methods for assessing agreement between two methods of clinical measurement. Lancet. 1986;1:307-10.
- [CrossRef] [Google Scholar]
- Measurement in medicine: The analysis of method comparison studies. J R Stat Soc B. 1983;32:307-17.
- [CrossRef] [Google Scholar]
- What is the proper way to apply the multiple comparison test? Korean J Anesthesiol. 2018;71:353-60.
- [CrossRef] [PubMed] [Google Scholar]
- Applications of 3D imaging in orthodontics: Part II. J Orthod. 2004;31:154-62.
- [CrossRef] [PubMed] [Google Scholar]
- CBCT in orthodontics: Assessment of treatment outcomes and indications for its use. Dentomaxillofac Radiol. 2015;44:20140282.
- [CrossRef] [PubMed] [Google Scholar]
- Positional change of the hyoid bone at maximal mouth opening. Oral Surg Oral Med Oral Pathol. 1994;77:451-5.
- [CrossRef] [PubMed] [Google Scholar]
- Relationship between head posture and hyoid position in adult females and males. J Craniomaxillofac Surg. 2006;34:85-92.
- [CrossRef] [PubMed] [Google Scholar]
- Reorientation methodology for reproducible head posture in serial cone beam computed tomography images. Sci Rep. 2023;13:3220.
- [CrossRef] [PubMed] [Google Scholar]
- Reliability of upper airway linear, area, and volumetric measurements in cone-beam computed tomography. Am J Orthod Dentofacial Orthop. 2014;145:188-97.
- [CrossRef] [PubMed] [Google Scholar]
- Three-dimensional computed tomographic analysis of airway anatomy. J Oral Maxillofac Surg. 2010;68:363-71.
- [CrossRef] [Google Scholar]
- Upper airway flow dynamics in obstructive sleep apnea patients with various apnea-hypopnea index. Life (Basel). 2022;12:1080.
- [CrossRef] [PubMed] [Google Scholar]
- Functional respiratory imaging as a tool to assess upper airway patency in children with obstructive sleep apnea. Sleep Med. 2013;14:433-9.
- [CrossRef] [PubMed] [Google Scholar]
- Effect of premolar extraction on the upper airway in adult and adolescent orthodontic patients: A meta-analysis. Chin J Dent Res. 2023;26:35-45.
- [Google Scholar]




