

Translate this page into:
Attachment geometry and clinical predictability in aligner treatment: A systematic review


*Corresponding author: Hajar Ben Mohimd, Department of Dentofacial Orthopedics, Faculty of Dental Medicine, Mohammed V University in Rabat, Rabat, Morocco. hajar_benmohimd@um5.ac.ma
-
Received: ,
Accepted: ,
How to cite this article: Ben Mohimd H, Oualalou Y, Zaoui F, Houb-Dine A, Benyahia H. Attachment geometry and clinical predictability in aligner treatment: A systematic review. APOS Trends Orthod. doi: 10.25259/APOS_109_2024
Abstract
Objectives
The aim of this systematic review was to assess attachment efficiency in the improvement of movement predictability in aligner treatment and to determine the impact of their type (conventional or optimized) on movement accuracy.
Material and Methods
Three electronic databases (PubMed, ScienceDirect, and Cochrane Library) were screened from initiation to December 2023 for studies assessing attachment efficacy using this search equation (Aligners OR Invisalign OR [clear aligners] OR [transparent aligners]) AND (attachments) AND (efficacy OR efficiency OR effectiveness) AND (orthodontics). Quality assessment of the included studies was performed using the JBI tool to assess cohort and case-control studies and Risk of Bias 2 (RoB 2) in randomized trials.
Results
A total of 970 publications were found as search results in the screened databases. Nineteen were included in this systematic review based on pre-determined inclusion criteria. The studies were published between 2009 and 2023. The analysis of the results was realized by examining all types of movements. RoB assessment in this systematic review was moderate in the majority of the studies.
Conclusion
The current systematic review showed that the use of attachments could improve movement accuracy. However, more interventional studies are necessary with control groups to support and confirm the results of the included studies.
Keywords
aligners
Attachments
Efficiency
Orthodontic tooth movement predictability

INTRODUCTION
Orthodontic treatment with aligners has spread quite rapidly, especially in adult patients to meet their esthetic requirements. Many systems are available in the market; each one has its specificities. Orthodontic treatment with aligners was first introduced by align technology in 1999 through the Invisalign system, offering an esthetic alternative to labial fixed appliances. Initially indicated only in the treatment of minor malocclusions[1] such as mild crowding and diastema closure; currently, thanks to improvements in thermoplastic materials and the introduction of SmartForce features such as attachments, pressure zones, power ridge, and smart staging have enabled additional treatment of more complex and difficult malocclusions with more precise and predictable results.[2,3]
With this technique, orthodontic movement results from a pre-determined mismatch between tooth and aligner which coincides with the desired position of the tooth.[4,5] Thus, reaching the final dental position implies a sequential aligner worn by the patient 22 h/day, which progressively repositions the teeth by small amounts. The aligner is capable of generating tooth movement using two different biomechanical approaches:[6]
Displacement-a driven system where the tooth moves gradually until reaching the final position which is imprinted in the aligner, the extensive and intimate contact that exists between the crown surface and the aligner allows the transmission of a force that decreases rapidly. This system is very effective in tipping movements, and
Force-driven system where the aligner is designed to emit a pure force or a system of specific forces to move a tooth or dental block. This approach implies the use of certain auxiliaries to make more efficient some complex movements.
Among these auxiliaries, we find attachments; these are small composite pads in three-dimensional geometric shapes bonded to the teeth to improve the biomechanics of the aligners by creating precise and directional forces and couples capable of producing the desired tooth movements with greater precision and predictability. Attachments are divided into 2 categories: conventional attachments which are passive attachments (rectangular, beveled, or ellipsoid) with a standardized shape and size, they can be positioned by the clinician on every tooth and can be oriented in any direction, acting as handles for the aligners and optimized attachments which are smaller in size and are automatically placed by the software when it detects certain thresholds of tooth movement.[7]
Attachments play an important role; they ensure the retention of the aligners, prevent them from slipping, and make it possible to provide pre-determined force vectors. In fact, these force vectors are determined by the shape and location of the attachment and more precisely by the orientation of their active surface which determines the point of application and the direction of the force. Therefore, it is important to plan these active surfaces with considered biomechanical intentionality, in accordance with clinical objectives.[8]
Several movements require the use of attachments, namely derotation, extrusion movement, intrusion, and root control. Many studies have evaluated aligner effectiveness with attachments in the establishment of these orthodontic movements. The objective of our systematic review was to search the literature and analyze the available scientific evidence regarding the efficiency of attachments in the achievement of orthodontic movements and to determine the impact of their type (conventional or optimized) on movement accuracy.
MATERIAL AND METHODS
Criteria for considering studies for this review
Types of studies
Randomized and non-randomized clinical trials, cohort studies, and prospective and retrospective studies assessing attachment effects in orthodontic treatment with aligners.
Types of participants
Orthodontic patients were treated with aligners either as the intervention or as the control group.
Types of interventions
Studies assessing attachment efficiency in aligner therapy. All aligner systems were included.
Outcome measures
The efficacy and efficiency of attachments were assessed with: movement accuracy movement pattern or movement amount.
Search methods for identification of studies
MEDLINE (PubMed), ScienceDirect, and Cochrane Library were screened using a combination of mesh terms for eligible studies related to the focused question [Table 1]. A complementary hand search was done in some journal databases. No restrictions on language or year of publication were placed.
| The focus question | Attachments efficiency in controlling orthodontic movement |
Search strategy
|
|
| Search combinations | 1 AND 2 AND 3 |
| Electronic databases | MEDLINE, Science Direct, and Cochrane |
Selection of studies
A systematic search was performed using a Population, Intervention, Comparison, and Outcome approach in the following databases: MEDLINE, PubMed, Cochrane Library, and Elsevier-ScienceDirect for eligible studies related to the focused question. No time restrictions were applied for the screening process. The last electronic search was performed in November 2023. In addition, a complementary hand search was done in some journal databases. No restrictions on language or year of publication were placed.
Data collection and analysis
Two review authors (H. Ben Mohimd and H. Benyahia) separately examined the title and abstract of each article identified. If the title or abstract did not provide sufficient information regarding the inclusion criteria, it was then necessary to proceed to a full-text reading before including or excluding the article.
Inclusion and exclusion criteria
Only clinical trials, prospective and retrospective studies, published in English or French, were included [Table 2].
| Inclusion criteria | Exclusion criteria |
|---|---|
| Prospective and retrospective | Studies on patients with |
| original studies on human | genetic syndrome and |
| subjects | severe facial |
| Studies on orthodontic | malformations |
| treatment with aligners | Case reports |
| Studies that included clear | Abstracts |
| descriptions of the attachment | Author debates |
| used | Summary articles |
| Studies with adequate | Studies on animals |
| statistical analysis Reviews | In vitro studies |
Data extraction and management
Full-text articles were checked according to eligibility criteria. Studies, that did not meet all the inclusion criteria, were excluded from the review. Any disagreements in terms of study selection were resolved by discussion with the third author.
The following information was determined for all articles:
Names of the authors
Year of publication
Study design
Number and groupings of participants
Type of intervention
Comparative groups, and
Type of clinical outcome.
Quality of the studies
To determine the methodological quality and the level of evidence, two authors (B-M. H and B. H) independently analyzed all studies to identify existing biases. In case of disagreement, the judgment of a third reviewer (O. Y) was planned.
Quality assessment of the included studies was performed using the revised tool to assess the risk of bias 2 (RoB 2) in randomized trials and Joanna Briggs Institute (JBI) RoB quality assessment for prospective and retrospective cohort and case-control studies.
According to RoB 2, the assessment was based on five domains (randomization process, deviations from intended interventions, missing outcome data, measurement of the outcome, and selection of the reported result). Within each domain, one or more signaling questions were answered. These answers allowed us to formulate a judgment of “low risk of bias,” “some concerns,” or “high risk of bias.” The judgments within each domain lead to an overall RoB judgment for the result being assessed.
RESULTS
Study selection
The database search identified a total of 193 literature references on MEDLINE (PubMed), 725 on ScienceDirect, 37 on the Cochrane Library, and 15 by manual research with a total of 970 reference titles. After title and abstract reading, 853 titles were removed including all duplicates and those considered as irrelevant. Finally, after full-text reading and analyzing, only 19 studies met the pre-established eligibility criteria [Figure 1].
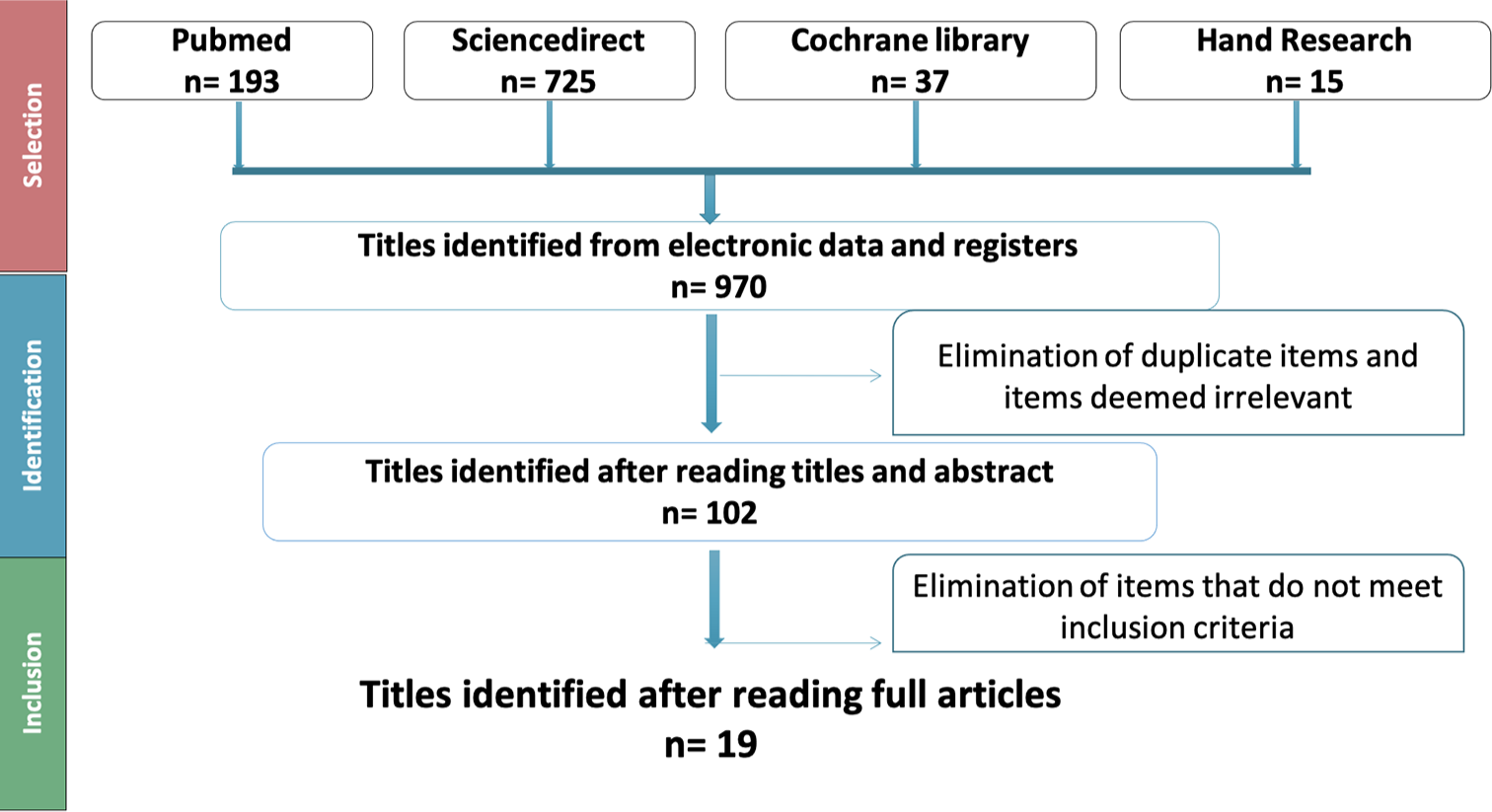
- Flow chart of the systematic review.
Study characteristics
The characteristics of each study are presented in [Table 3]. [Table 4] gives an overview of the results of the included studies regarding the clinical parameters of each type of orthodontic movement.
| Authors/year | Title | Study design | Intervention group | Comparison | Outcome (s) |
|---|---|---|---|---|---|
| Kravitz et al. 2008[11] | Influence of Attachments and Interproximal Reduction on the accuracy of canine rotation with Invisalign | Prospective | Canine rotation with neither attachments nor interproximal reduction | G1: Canines with attachments only (AO) G2: Interproximal reduction only | Rotation accuracy |
| Simon et al. 2014[12] | Treatment outcome and efficacy of an aligner technique regarding incisor torque, premolar derotation and molar distalization | Retrospective study (cohort pronostic) | *Upper incisor torque 10° with horizontal ellipsoid attachment’ *PM derotation > 10° with optimized rotation attachment’ *Molar distalization 1.5 mm with horizontal beveled gingival attachment’(10) | Upper incisor torque with power ridges Premolar derotation) with no auxiliary Molar distalization with no auxiliary (10) | The accuracy of molar distalization, premolar derotation, and incisor torque |
| Ravera et al. 2016[26] | Maxillary molar distalization with aligners in adult patients: A multicenter retrospective study | Retrospective | Sequential distalization with Invisalign | No control group | -Amount of distalization - Vertical and sagittal movement |
| Garino et al. 2016[27] | Effectiveness of composite Attachments in controlling upper-molar movement with aligners | Case control | Group 1: Molar distalization with rectangular composite attachments from canine to second molar (five attachments per quadrant | Group 2: AO on the first and second premolars and the first molar (three attachments per quadrant) Group 3: control group | - Amount of bodily upper-molar distalization - Anchorage |
| Dai et al. 2019[35] | Comparison of achieved and predicted tooth movement of maxillary first molars and central incisors: First premolar extraction treatment with Invisalign | Retrospective | Maxillary first molar and incisors angulation achieved | Maxillary first molar and incisors angulation predicted | Differences between predicted and achieved tooth movement |
| Haouili et al. 2020[13] | Has Invisalign improved? A prospective follow-up study on the efficacy of tooth movement with Invisalign | Prospective | Movement achieved | Movement predicted | Movement accuracy of mesial-distal crown tip, buccal-lingual crown tip, intrusion, extrusion and rotation |
| Dai et al. 2021[37] | Comparison of achieved and predicted crown movement in adults after 4 first premolar extraction treatment with Invisalign | Retrospective | 3-Dimensional crown movement of Maxillary and mandibular Canine, molar and incisor achieved | 3-Dimensional crown movement of Maxillary and mandibular Canine, molar, and incisor predicted | - Movement accuracy |
| Bilello et al. 2022[14] | Accuracy evaluation of orthodontic movements with aligners: A prospective observational study | Prospective observational | -Movement achieved | Movement predicted | -Movement accuracy of buccal-lingual tip -Anterior intrusion - Rotation < 30° |
| Karras et al. 2021[15] | Efficacy of Invisalign attachments: A retrospective study | Retrospective | Optimized rotation and extrusion attachments | Conventional rotation and extrusion attachments | Movement accuracy Amount of tooth movement |
| Castroflorio et al. 2023[16] | Predictability of orthodontic tooth movement with aligners: effect of treatment design | Prospective observational study | Without attachments | Conventional attachments Optimized attachments | Predictability of orthodontic movement Lack of correction Movement prescribed |
| Smith et al. 2022[31] | Predictability of lower incisor tip using clear aligner therapy | Retrospective | No attachments | Vertical attachments | Movement accuracy |
| Ren et al. 2022[36] | The predictability of orthodontic tooth movements through clear aligner among first-premolar extraction patients: a multivariate analysis | Retrospective Cohort | Movement achieved | Movement predicted | Movement predictability |
| Groody et al. 2023[18] | Effect of clear aligner attachment design on extrusion of maxillary lateral incisors: A multicenter, single-blind randomized clinical trial | Randomized clinical trial | Extrusion with optimized attachments | Extrusion with horizontal attachments | Extrusion efficacy |
| Stephens 2022 et al.[17] | Clinical expression of programmed mandibular canine rotation using various attachment protocols and 1- versus 2-week wear protocols with Invisalign SmartTrack aligners: A retrospective cohort study | Retrospective cohort study | Group 1: optimized rotation attachments using 1-week wear | Group 2: optimized rotation attachments using 2-week wear Group 3: conventional rectangular attachments using 2-week wear. | Rotation accuracy |
| Burached et al. 2023[23] | Quantifying the efficacy of overbite reduction in patients treated with clear aligners using optimized versus conventional attachments | Retrospective cohort study | Conventional attachments | Optimized attachments | Efficacy of deep bite correction |
| Burached et al. 2023[19] | The efficacy of anterior open bite closure when using Invisalign’s optimized extrusion versus conventional attachments | Retrospective cohort study | Horizontal conventional attachments | Optimized extrusion attachments | Efficacy of open bite closure |
| Tang et al. 2023[38] | Relative anchorage loss under reciprocal anchorage in mandibular premolar extraction cases treated with clear aligners | Retrospective study | L4 extraction (38 quadrants) | L5 extraction (22 quadrants) | Relative anchorage lost |
| D’Anto et al. 2023[28] | Predictability of Maxillary Molar Distalization and Derotation with Clear Aligners: A Prospective Study | Prospective Study | Movement achieved | Movement planned | Movement predictability or accuracy |
| Al-Balaa et al. 2021[22] | Predicted and actual outcome of anterior intrusion with Invisalign assessed with cone-beam computed tomography | Retrospective | Movement achieved | Movement planned | Movement efficacy |
| Orthodontic movement | Authors | System used | Attachments features | Comparison | Outcome assessed | Method of outcome assessment | Results |
|---|---|---|---|---|---|---|---|
| Derotation | Kravitz et al. 2008[18] | Invisalign | *Ellipsoid (16) *Rectangular (1) *Ellipsoid and vertical (12) *Ellipsoid and horizontal (4) Rectangular and horizontal (1) |
Group: Interproximal reduction only Group: neither attachments nor interproximal reduction |
Movement accuracy | Superimposition of The pretreatment and posttreatment virtual models | There was no statistically significant difference in rotation accuracy of maxillary and mandibular canines for any of the treatment groups. |
| Simon et al. 2014[12] | Invisalign | Optimized rotation attachment’ | Group (b): No auxiliary | Movement accuracy | Superimposition of initial and final digital casts of Invisalign treatment | The use of attachments had no statistically significant influence on the accuracy of derotation movement. | |
| Haouili et al. 2020 [13] |
Invisalign | Optimized attachments | No control group | Movement accuracy | Superimposition of initial and final digital casts of Invisalign treatment | The lowest accuracy occurred with rotation (46%). Rotational movement was still difficult for the canines, premolars, and molars even with the use of optimized attachments. | |
| Bilello et al. 2022[14] | Invisalign | Optimized attachments | No control group | Movement accuracy | Superimposition of initial, and final digital casts (real and ideal) | The overall accuracy for rotation resulted in 86%, ranging from 96% for the maxillary central incisors to 70.4% for the mandibular first premolars. | |
| Karras et al. 2021[15] | Invisalign | Optimized rotation attachments | Conventional rotation attachments | Movement accuracy | Superimposition of initial, and final digital casts (real and ideal) | Conventional attachment types may be just as effective as Invisalign's proprietary optimized attachments for rotations of canines and premolars | |
| Castroflorio et al. 2023[16] | Invisalign | Without attachment | Optimized and conventional attachments | Movement predictability | The superimposition of the post-treatment .stl file (achieved outcome) on the planned final stage .stl file (predicted outcome) | Optimized attachments for upper canines and lower premolar rotation seem not working properly. The lack of correction is reduced in comparison to others studies so attachments should be applied but the design of the used attachments is not sufficient to control the prescribed movement. |
|
| Stephens 2022 et al.[17] |
Invisalign | Optimized rotation attachment 1 week wear | -Optimized attachment 2 week wear -Conventional rectangular attachments 2 week wear |
Rotation accuracy | Superimposition of initial and final digital casts of Invisalign treatment | Vertical rectangular attachments were associated with the least accurate expression of prescribed movement | |
| Extrusion | Haouili et al. 2020[13] | Invisalign | Optimized attachment | Movement predicted | Movement accuracy | Superimposition of initial and final digital casts of Invisalign treatment | Maxillary incisor extrusion improved with attachments (55%) whereas extrusion of the maxillary and mandibular molars (40%) had the lowest accuracy |
| Karras et al. 2021[15] | Invisalign | Optimized attachments | Conventional attachments | Movement accuracy | Superimposition of initial, and final digital casts (real and ideal) | Differences between mean accuracies of incisor extrusion using Invisalign’s optimized versus conventional attachments were neither statistically nor clinically significant. | |
| Groody et al. 2023 [18] |
Invisalign | Optimized (O) attachments. | Horizontal attachments: - Rectangular horizontal non-beveled, - Rectangular horizontal incisally- beveled, - Rectangular horizontal gingivally- beveled |
Movement efficacy | Digital Models superimposition | Horizontal attachments were significantly more effective at achieving prescribed maxillary incisor extrusion (76% of the predicted amount) compared with O attachments (62% of the predicted amount) | |
| Burached et al. 2023 [19] |
Invisalign | Optimized attachments | Horizontal attachments | Openbite correction efficacy | Digital Models superimposition | Optimized attachments are no more effective than using conventional attachments in incisor extrusion to correct open bite. | |
| Intrusion | Burached et al. 2023 [23] |
Invisalign | Optimized (O) attachments | Attachment conventionals | Movement efficacy | Digital Models superimposition | Movement accuracy: (33–40%) Optimized attachments are no more effective than using conventional attachments in reducing deep overbite |
| Al-Balaa et al. 2021 [22] |
Invisalign | Passive optimized deepbite attachments | No control group | Movement accuracy | Pre and posttreatment cone-beam computed tomography scans | For anterior intrusion>1 mm), the predictability of intrusion for patients treated only with pressure areas and passive OA without bite ramps is 51.19% | |
| Haouili et al. 2020 [13] |
Invisalign | G5 attachments | No control group | Movement accuracy | Digital Models superimposition | The low accuracy of mandibular incisor intrusion (35%) may be related to the lack of posterior anchorage | |
| Incisor torque | Simon et al. 2014[12] | Invisalign | Group (a): “horizontal ellipsoid attachment” | Group (b): Power ridges | Movement accuracy | Superimposition of initial and final digital casts of Invisalign treatment | No substantial differences were observed if the upper central incisor torque was supported with a horizontal ellipsoid attachment or with a Power Ridge |
| Molar distalization | Simon et al. 2014[12] | Invisalign | Horizontal beveled gingival attachment | No attachments | Movement accuracy | Superimposition of initial and final digital casts of Invisalign treatment | Movement accuracy : -Without att: 86.9% (SD=0.2) -With att: 88.4% (SD=0.2) Bodily tooth movement can be effectively performed using Invisalign, irrespective to attachments |
| Ravera et al. 2016[26] | Invisalign | 5 Rectangular and vertical attachments on the distalizing teeth (3, 4, 5, 6, 7) | No control group | Amount of distalization and movement pattern | Pre-and post-treatment lateral cephalometric radiographs | Distal movement of the 1stand 2ndmolar: 2.25 mm and 2.52 mm respectively without significant tipping and vertical movements | |
| Garino et al. 2016[27] | Invisalign | 5 rectangular attachments (3, 4, 5, 6, 7): group 1 | Group 2: 3 rectangular attachments (4, 5, 6) Group 3: control group (no treatment) |
Amount of distalization | Linear (horizontal, vertical) and angular Measurements on cephalogram | - No significant differences in the amount of 2ndmolar movement with or without vertical rectangular attachments. There was significantly more distal movement of the first molar and central incisor when vertical rectangular attachments were placed on all five distalized teeth |
|
| D’Anto et al. 2023[28] | Invisalign | Horizontal rectangular attachments on both 1M and 2M | No control group | Movement accuracy | Superimposition of initial and final digital casts | Clear aligners can be regarded as a valuable option for the distalization of first and second molars. Mean accuracy: 2M 75.2%/1M 69.4% |
|
| Tipping movement | Smith et al. 2022[31] | Invisalign | 45: No attachments | 21: Vertical attachments | Lower incisor tip accuracy | Superimposition of initial, and final digital casts (real and ideal) | Vertical rectangular attachments are recommended when large amounts of root movement are planned, and their presence improves the ability to translate the root apex |
| Molar anchorage | Linghuan et al. 2022[36] | Invisalign | G6 optimized attachments 25 (43.9%) | Conventional attachments Horizontal attachment 13 (22.8%) Vertical attachment 19 (33.3%) |
Movement predictability | Superimposing the actual and virtual post-treatment models | mesial movement and extrusion did not differ among different types of attachments, but mesial tipping decreases with Invisalign G6 attachments |
| Dai et al. 2021[37] | Invisalign | G6 Optimized[22] -5mm horizontal rectangular attachments (14) -4mm horizontal rectangular attachments (16) -3mm horizontal rectangular attachments (6) -3mm vertical rectangular attachments (10) |
No control group | 3 Dimensional crown movement | Superimposition of pretreatment, predicted posttreatment and actual posttreatment maxillary and mandibulary dental models | Relative to predicted changes, first molars achieved greater mesial displacement, mesial tipping, and buccal inclination in both the maxilla and mandible, greater intrusion in the maxilla, and greater mesial-lingual rotation and less constriction in the mandible. | |
| Dai et al. 2019[35] | Invisalign | Attachment G6-optimized[23] | -3mm vertical attachment (8) -3mm horizontal attachment (15) -5mm horizontal attachment (14) |
Differences between predicted and achieved tooth movement | Superimposition of pretreatment, predicted posttreatment and actual posttreatment maxillary and mandibulary dental models |
First molar anchorage control was not fully achieved as predicted even with the use of attachments. | |
| Canine retraction | Linghuan et al. 2022[36] | Invisalign | Canine attachment Vertical attachment |
Optimized attachment | Movement predictability | Superimposing the actual and virtual post-treatment models | - Significant decrease in distal movement by 1.3 mm was achieved, with a significant increase in distal tipping, lingual inclination, and distal rotation than predicted - Distal tipping was associated with optimized attachments - Vertical rectangular attachments on canines are superior to optimized attachments on canine root control among extraction cases. |
| Tang et al. 2023[38] | Clear aligner | Rectangular att (22) Optimized att (38) |
Rectangular att (22) Optimized att (38) |
First and second PM extraction | Relative anchorage loss | Unwanted extrusion and distal crown tipping during anterior retraction; attachments had little effect on preventing this from occurring. | |
| Dai et al. 2021[37] | Invisalign | G6 Optimized (51) -3mm vertical rectangular attachment (1) -4mm vertical rectangular attachment (16) |
3 Dimensional crown movement | Superimposition of pretreatment, predicted posttreatment and actual posttreatment maxillary and mandibulary dental models | Both the maxillary and mandibular canines achieved notably more distal tipping than predicted Limited benefit in using optimized attachments to control canine angulation |
||
| Incisor retraction | Ren et al. 2022[36] | Invisalign | Power ridge 23 (37.1%) used on central incisors; associated with different canine attachments (optimized or Vertical) | no power ridge on central incisors; associated with different canine attachments (optimized or Vertical) | Movement predictability | Superimposing the actual and virtual post-treatment models | The power ridge did not influence the lingual tipping, extrusion, and retraction of central incisors When power ridges are prescribed on incisors, lingual root-torquing and intrusion of incisors are more predictable with vertical rectangular attachments than with optimized attachments on canines |
| Dai et al. 2021[37] | Invisalign | Optimized att (2) Power ridge (12) |
No auxillary used (54) | Crown movement | Superimposition of pretreatment and predicted post-treatment models | Both maxillary and mandibular central incisors achieved notably more lingual inclination than predicted | |
| Dai et al. 2019[35] | Invisalign | Power ridge (11) | None (49) | Differences between predicted and achieved tooth movement | Superimposition of pretreatment and predicted post-treatment models | Central incisors tipped more lingually, retracted less and extruded more than predicted |
Among the studies included, one study was a randomized clinical trial, five studies were prospective, 13 studies were retrospective, and one was a case-control study. The selection process of articles is presented in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow diagram.
The sample size in the 19 studies included ranged from 10 to 100 patients with a total of 803 patients, mostly adults. All the studies used the Invisalign system. Articles that did not specify the type of attachment used were excluded.
Attachment efficiency was assessed in the majority of included studies through the comparison of the movement planned on Clincheck and the movement obtained except for two studies that compared pre- and post-treatment cephalometric values.
Attachments used in the studies were conventional rectangular, rectangular beveled, ellipsoid, and optimized. The movements evaluated by the studies were derotation, extrusion, intrusion, torque, and radicular control in mesio-distal movement. Expansion-contraction movement and posterior bucco-lingual tip were not studied.
The analysis of the results obtained was studied for each type of orthodontic movement. Regarding root control movement during mesio-distal displacements, we chose to evaluate separate cases with and without extraction. Thus, attachment efficacy was assessed first for distalization movement and the correction of dental axes and secondly for anchorage management and canine and incisor retraction.
RoB assessment
Quality assessment of the nineteen studies was performed using different tools for RoB assessment based on the study type. The number of included studies is limited compared to published reports in medical sciences. The adopted search strategy identified one randomized controlled trials (RCTs), seventeen cohort studies, and one case-control. 13 studies were considered according to JBI at a medium RoB, 2 at low, and one at high risk [Table 5a and b].
| Study | Q1a | Q2 | Q3 | Q4 | Q5 | Q6 | Q7 | Q8 | Q9 | Q10 | Q11 | % Yes | Riskb |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Dai et al. 2019[35] | Yes | Yes | Yes | Unclear | Unclear | Yes | No | Yes | Unclear | Not applicable | Yes | 54 | Moderate |
| Bilello et al. 2022[14] | Yes | Yes | No | No | No | Yes | Yes | No | Unclear | Unclear | Yes | 45 | High |
| Dai et al. 2021[37] | Yes | Yes | Yes | Unclear | Unclear | Yes | Yes | Yes | Not applicable | Not applicable | Yes | 63 | Moderate |
| Ren et al. 2022[36] | Yes | Yes | Yes | No | No | Yes | Unclear | Unclear | Unclear | Unclear | Yes | 45 | High |
| Haouili et al. 2020[13] | Yes | Yes | Yes | Unclear | Unclear | Yes | Unclear | Yes | No | No | Yes | 54 | Moderate |
| Simon et al. 2014[12] | Yes | Yes | Unclear | Unclear | Unclear | Yes | Unclear | No | No | No | Yes | 36 | High |
| Kravitz et al. 2008[11] | Yes | No | Unclear | Yes | No | Yes | Yes | Yes | Unclear | Unclear | Yes | 54 | Moderate |
| Stephens et al.[17] | Yes | Yes | Unclear | Yes | No | Yes | Yes | Yes | Unclear | Unclear | Yes | 63 | Moderate |
| Ravera et al. 2016[26] | Yes | Yes | Yes | Yes | Unclear | Yes | Yes | Yes | No | No | Yes | 72 | Low |
| Castroflorio et al. 2023[16] | Yes | Yes | Yes | Unclear | Unclear | Yes | Yes | Yes | No | No | Yes | 63 | Moderate |
| Al-Balaa et al.[22] | Yes | Yes | Yes | No | No | Yes | Yes | Yes | Unclear | Unclear | Yes | 63 | Moderate |
| D’Anto et al. 2023[28] | Yes | Yes | Yes | Unclear | Unclear | Yes | Yes | No | No | Unclear | Yes | 54 | Moderate |
| Karras etal.2023[15] | Yes | Yes | Yes | No | Unclear | Yes | Yes | Unclear | Unclear | Unclear | Yes | 54 | Moderate |
| Tang et al. 2023[38] | Yes | Yes | Yes | No | No | Yes | Unclear | Yes | No | Unclear | Yes | 54 | Moderate |
| Smith et al. 2022[31] | Yes | Yes | Yes | No | No | Yes | Yes | Yes | Unclear | No | Yes | 63 | Moderate |
| Burached et al. 2023[35] | Yes | Yes | Yes | No | Unclear | Yes | Yes | Unclear | No | Unclear | Yes | 54 | Moderate |
| Burached et al. 2023[37] | Yes | Yes | Yes | No | Unclear | Yes | Yes | Unclear | No | Unclear | Yes | 54 | Moderate |
JBI: Joanna Briggs Institute, aQ1-Q11 indicates questions 1–11 based on the JBI risk assessment, bThe risk of bias was ranked as high when the study reached up to 49% of yes scores, moderate when the study reached from 50% to 69% of yes scores and low when the study reached more than 70% of “yes” scores
| Study | Q1a | Q2 | Q3 | Q4 | Q5 | Q6 | Q7 | Q8 | Q9 | Q10 | % Yes | Riskb |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Garino et al. 2016 [27] | Yes | Yes | Yes | Yes | Yes | No | Unclear | No | Unclear | Yes | 60 | Moderate |
JBI: Joanna Briggs Institute, aQ1-Q10 indicates questions 1–11 based on the JBI risk assessment, bThe risk of bias was ranked as high when the study reached up to 49% of yes scores, moderate when the study reached from 50 to 69% of yes scores and low when the study reached more than 70% of “yes” scores
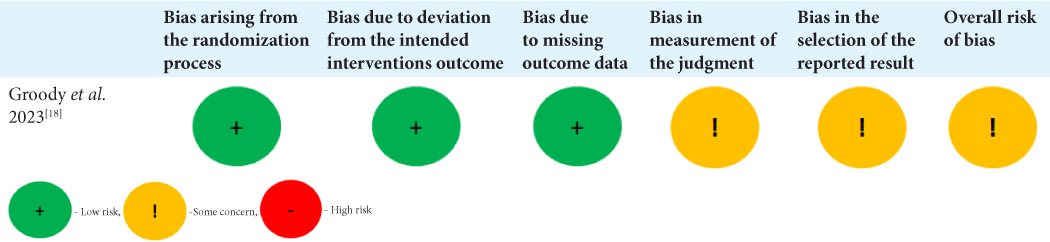
Concerning the one RCT included, the randomization process was well described and was at low RoB, deviations from intended interventions and missing outcome data were also at low RoB. However, the measurement of the outcome and the selection of the reported results raised some concerns [Table 5c].
 |
DISCUSSION
To increase aligner efficiency, many auxiliaries can be prescribed to improve orthodontic movement accuracy and make more efficient complex movements. Among these auxiliaries, we find composite attachments that are used to improve the biomechanics of the aligners by creating precise and directional forces and couples capable of producing the desired tooth movements with greater precision and predictability. The aim of our systematic review was to evaluate the efficiency of attachments in the achievement of orthodontic movement and to assess if the type of attachment had an impact on movement efficacy. For didactic reasons, we decided to analyze separately each type of orthodontic movement.
Derotation movement
Derotation is one of the challenging movements in aligner biomechanics. To improve its predictability, the use of attachments will allow the aligner to lock in the dental crown, reducing considerably the sliding effect and emphasizing the force system through the increase of the lever arm.[9,10] According to our results, 7 included studies evaluated attachment efficiency in derotation movement.
Among these 7 studies, two compared the accuracy of derotation movement of the canines[11] and premolar (PM)[12] with and without attachment and reported no significant difference between the 2 groups with a mean accuracy of 35.8% and 39.95%, respectively. These results can be explained by several elements, first of all, the cylindrical morphology of canines and PM which classifies them among the most difficult teeth to derotate due to the absence of interproximal undercuts and the reduction of force application surface causing the aligner to slip when it attempts to rotate. In addition, the majority use of ellipsoidal attachment shape in the study of Kravitz et al.[11] remains unsuitable for rotational movement. At last, the aligner material used was EX30 whose biomechanical properties are less compared to the SmartTrack.
The other 5 studies[13-17] assessed the accuracy of derotation movement with optimized and/or conventional attachments with or not a control group without attachments and reported variable predictability percentages ranging from 46% to 86%. That said, despite this difference, we noted an improvement over time in the predictability even for lower C and PM which can be explained by the evolution of the smartforce and SmartTrack functionality. Concerning the impact of attachment type on the accuracy of movement, there was no statistically significant difference between the use of optimized and conventional attachments but both Karras et al.,[15] and Stephens et al.[17] reported a more precise movement expression with optimized attachments.
Extrusion movement
The correction of several malocclusions requires recourse to extrusion movement (open bite, deepbite, ectopic teeth). The absence of a surface on which the aligner can rest to extrude the tooth causes it to slip. The use of attachment is essential so that the aligner rests on the active surface and brings the tooth vertically.[7] According to our results, 4 studies[13,15,18,19] evaluated the effectiveness of attachments in extrusion movement. Concerning the anterior teeth, the results showed an improvement in the percent of predictability, especially for the maxillary incisors with an increase from 56% to 79%. Indeed in comparison to the Kravitz et al. study[20] where movement accuracy was 18% for maxillary incisors, we noted an evolution in the percent (Haouili et al. 2020[13]: 55%, Karras et al. 2021[15]: 66.3%) reaching 79% according to Groody et al.[18] This result implies a better orthodontic management of open bite cases.
Concerning posterior teeth, Haouili et al.[13] reported only a 40% accuracy for maxillary and mandibular molars with optimized extrusion attachments. In fact, posterior extrusion could be difficult to obtain due to the bite block effect of aligners or to the patient’s muscles.
The comparison of conventional and optimized attachments showed no statistically significant difference; however, Groody et al.[18] reported the superiority of the conventional one in the maxillary lateral incisor extrusion with a 22% improvement using a horizontal attachment design. This can be related to the larger active surface of horizontal rectangular attachments allowing the aligner to push on, thus improving biomechanical properties.
Intrusion movement
One of the difficult movements to achieve in orthodontics is intrusion. In aligner treatment, the use of passive or active attachments on the buccal surface of the first and second PM increases retention and provides anchorage for the intrusion of the anterior teeth.[21]
Only 3 studies assessed the accuracy of intrusion movement and reported variability in the % of predictability not exceeding 50%, in fact, Haouili et al.[13] using the G5 protocol reported a low accuracy of mandibular incisor intrusion with a mean average of 35%, Al-Balaa et al.[22] found 51% and Burashed and El Sebai[23] found 30–40%. This low accuracy of intrusion movement of the anterior region could be related to the lack of posterior anchorage especially since all studies used only passive deepbite optimized attachment on the first premolar. In addition, the use of other auxiliaries like bite ramps is frequently indicated to enhance the correction of deepbite; however, none of the studies reported using it in their patients. Finally, it is important to control the incisor’s axis during the movement which might be difficult with aligner material.
Concerning the impact of the type of attachments used, Burashed and El Sebai[23] reported that optimized attachments are no more effective than using conventional attachments in reducing deep overbite.
Torque
Anterior root torque is one of the challenging movements to obtain with aligner treatment.[24] The use of some auxiliaries such as attachments or mostly power ridge is important to accomplish better root control. According to our results, only one study evaluated root torque efficiency with aligners using attachments and reported the ability of aligners to induce root displacement. However, a torque loss (up to 50%) was noticed. Moreover, the comparison of the attachment group with the power ridge showed no differences if the upper central incisor torque was supported with a horizontal ellipsoid attachment or with a Power Ridge.[12]
Radicular control in mesiodistal displacement (non-extraction cases)
Molar distalization
In molar distalization with aligners, the appliance produces the distalization force and since the force passes away from the center of resistance, we witness a version of the crown. The use of an attachment counteracts the uncontrolled tipping during distalization through the generation of a countermoment that ends in the root uprighting making it possible to provide a force couple to move the roots and obtain a translational movement.[5] According to our results, 4 studies evaluated the efficacy of attachments in molar distalization movement.
Among these 4 studies, one by Simon et al.[12] compared horizontal gingival beveled attachments with the use of no attachments and reported that bodily tooth movement can be effectively performed using Invisalign, irrespective of attachments (without att: 86.9%, with att: 88.4%). This result agrees with that of Saif et al.[25] who reported an accuracy of 73.8% with no statistically significant difference between the group with and without attachments with the absence of a standardized protocol of attachments. Hence, these results should be taken with caution, especially the Simon et al. study[12] where the results were taken directly after the distalization of first and second molars without considering the anchorage lost in the posterior region during the retrusion of anterior teeth.
Concerning the other studies, Ravera et al.[26] and Garino et al.[27] both reported good control of the molar axis, reinforcement of the posterior anchorage during incisor retraction, and a greater amount of distalization with the use of 5 configurations (vertical attachment from canine to second molar). D’Anto et al.[28] used horizontal attachment with a 5 configuration from canine to second molar and staging of 50% and reported a 2.5 mm amount of molar distalization, an optimal vertical control thanks to the significant molar intrusion associated with the block bite effect without loss of anterior anchorage. These results agree with those obtained by finite element studies which confirm the contribution of attachments in controlling the translation movement of the molars with the configuration of 5 attachments from canine to the 2nd molar is the most promising (Rossini et al., 2020; Ayidaga and Kamiloglu, 2021).[29,30]
Dental axe correction
Only one study assessed the attachment effect on lower incisor tip accuracy and reported a better translation of the root apex with the use of vertical rectangular attachments when large amounts of root movement are planned in comparison to no attachment group. In fact, Smith et al.[31] found that the presence of an attachment resulted in a 1.2° greater tip (F = 3.7; P = 0.062) and 0.5 mm greater movement of the predicted apex of the tooth (F = 4.3; P = 0.042) compared with the no attachment group.
Radicular control in extraction cases
The management of extraction cases requires a good control of the anchorage and incisor torque allowing to reach class IC and M and to re-establish a functional anterior guide.
Baldwin et al. 2008[32] reported a lack in the control of tooth movement using aligners, with significant tipping of the teeth adjacent to the extraction sites in both the maxilla and mandible. A few years later, Li et al. 2015[33] reported a good root angulation with the Invisalign system thanks to the use of adequate attachments with some limitations regarding occlusal contacts and buccolingual inclination. In fact, Invisalign proposed the G6 protocol in extraction cases, in which they use optimized anchorage attachment on posterior teeth and optimized retraction attachment on the canine achieving maximum anchorage control.[34]
According to our results, 4 studies assessed the efficacy of attachments in extraction cases, Dai et al.[35] studied only maxillary first molars and central incisors after monomaxillary extraction, Ren et al.[36] added maxillary canine distalization, Dai et al.[37] worked on molar anchorage and canine and incisor retraction in both the maxilla and mandible and Tang et al.[38] and al evaluated mandibular anchorage loss and canine and incisor retraction efficacy between first and second premolar extraction cases.
Molar anchorage
All the studies included in our systematic review reported that 1M anchorage control was not fully achieved as predicted with the G6 protocol. In fact, 1M achieved greater mesial displacement, mesial tipping, buccal inclination in both the maxilla and mandible, greater intrusion in the maxilla, and greater mesial-lingual rotation in the mandible.
Molar mesial movement varied between studies with averages ranging from 2.01 ± 1.11 mm to 3.16 mm which implied the quarter or one-third of 1st PM extraction space. However, Dai et al.[37] reported better anchorage control in the mandibular first molar in comparison with maxillary molars. In the case of the second PM extraction, mandibular anchorage loss reached 40% with a mean average of 3.25 ± 1.19.
Concerning mesial tipping, molar angulation achieved, varied from 2.9° to 5.4° even if molars were predicted to tip distally which can be related to the mesial force applied on the molar crown.
Our results suggest that the use of attachments alone at the molar level is insufficient to prevent loss of anchorage, especially in case of maximum anchorage hence the need to add other means such as mini-screws.
The comparison of G6 optimized attachments and 5 mm or 3 mm horizontal rectangular attachments showed similar control in molar angulation and mesiodistal translation. However, Ren et al.[36] reported less mesial tipping with G6 attachments which can be explained by the mesial functional surface of the attachment whose design promotes mesial tipping resistance.
Canine retraction
Canine retraction involves a distal displacement of the root and the crown. The use of attachments is supposed to allow this translational movement. In our systematic review, only 3 studies evaluated attachment efficiency in canine retraction.
All authors reported for both the maxillary and mandibular canines less retraction, more distal tipping, lingual inclination, and distal rotation than predicted with limited benefit in using optimized attachments to control canine angulation.
The distal movement was less than predicted by 1.3 mm according to Ren et al.,[36] distal tipping difference between angulation planned and achieved varied among studies, Dai et al.[37] found 6.00 ± 4.44 for maxillary canines, and 7.44 ± 3.83 in the mandible. Ren et al.[36] reported an increase in distal tipping of 10.1° whereas Tang et al.[38] found 10.33 ± 8.138 more distal crown tipping. This result can be related to the lingual tipping of canines during distalization which can bring the root of the canine into contact with the external vestibular cortex interfering with canine root movement, resulting in distal tipping. Concerning the impact of the type of attachment, Ren et al.[36] reported the superiority of vertical rectangular attachments to optimized attachments on canine root control among extraction cases.
Incisor retraction
Root control during incisor retraction requires a rigorous biomechanics strategy that implies adequate intrusion and palatal root-torquing of incisors.[38,39] Attachments and mostly power ridges on central incisors are the tools used to offer additional lingual root torque on incisors and to avoid their lingual tipping and extrusion.[40] In our systematic review, we decided to assess incisor retraction efficacy and search for an eventual interaction between canine attachments and the expression of incisor torque. According to our results, all the studies included evaluating incisor retraction accuracy in extraction cases reported more lingual tipping, less retraction, and more extrusion than predicted.
Dai et al.[35] reported more lingual tipping by 5.16° ± 5.92°, less retraction by 2.12 ± 1.51 mm, and more extrusion by 0.50 ± 1.17 mm relative to predicted changes. Ren et al.[36] found less incisor retraction of 2 mm than the designed retraction, lingual tipping of (10.6°), and extrusion of (1.5 mm) of incisors. The central incisors’ actual retraction was 2 mm less than the designed retraction. In contrast, the central incisors achieved more extrusion (1.5 mm) and more lingual inclination (10.6°) than predicted movements. These results can be explained by the increase in aligner flexibility after PM extraction which reduces the intrusive force of the aligners on the anterior teeth. Therefore, the use of a power ridge on central incisors did not influence the lingual tipping, extrusion, and retraction of central incisors. However, the low prescription of power ridge in the majority of included studies represents a major bias in the interpretation of results, in fact, Ren et al.,[36] Dai et al.,[37] and Tang et al.[38] reported that only 37%, 17.64%, and 18.33% of patients, respectively, had power ridges. Moreover, Ren et al.[36] found that when power ridges were prescribed on incisors, lingual root-torquing and intrusion of incisors are more predictable with vertical rectangular attachments than with optimized attachments on canines thanks to their size which increase aligner retention. Thus, we could deduce that the use of rectangular vertical attachment on canine enhances root control during canine and incisor retraction.
Study limits
Given the results of our systematic review, further clinical trials are necessary to assess the impact of attachments on the effectiveness of aligners during different orthodontic movements.
Our results emphasize that attachments can produce significant therapeutic effects allowing the improvement of aligner biomechanics. However, despite these results, it is not without limitations, often related to the nature of studies that included sample size, the absence of no attachment control group, and variability of means of outcome assessment (cephalometry, superposition of 3D models, facial superposition). The literature has shown great heterogeneity; there are few clinical trials, and the risk of bias at the level of the included studies was variable with the majority having a medium RoB. Other well-designed prospective studies are necessary with a high level of proof, respecting the randomization protocol, with a homogeneous population and no-attachment control group, and representative sample size is needed to better define the role of attachments in aligner therapy and to clarify what is the best configuration for each movement. It would also be interesting to introduce cone beam and facial superposition to maximize the stability of superposition structures, improve the reproducibility of measurements, and benefit from artificial intelligence to ensure an effective location of attachments.
CONCLUSION
Within the limitations of the extracted data, it appears that the use of attachments increases the efficiency of aligners by improving the accuracy of rotation movement, extrusion, and mesiodistal displacement requiring radicular control. The improvement of certain movements may require an association of attachments with other auxiliaries such as power ridge and bite ramps.
Impact assessment of the type of attachments on movement accuracy showed no significant difference between optimized attachments and conventional attachments in terms of biomechanical efficiency. However, we noticed less mesial tipping of the first molar with G6 protocol in extraction cases and an improvement in movement accuracy with conventional attachments during extrusion movement of incisors and canine retraction.
Ethical approval
Institutional Review Board approval is not required.
Declaration of patient consent
Patient’s consent is not required as there are no patients in this study.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship: Nil.
References
- Patient survey on Invisalign! treatment comparen the SmartTrack! material to the previous aligner material. J Orofac Orthop. 2016;77:432-8.
- [CrossRef] [PubMed] [Google Scholar]
- Clear aligners generations and orthodontic tooth movement. J Orthod. 2016;43:68-76.
- [CrossRef] [PubMed] [Google Scholar]
- Computational design and engineering of polymeric orthodontic aligners: Computational design and engineering of polymeric orthodontic aligners. Int J Numer Method Biomed Eng. 2017;33:e2839.
- [CrossRef] [PubMed] [Google Scholar]
- Initial force systems during bodily tooth movement with plastic aligners and composite attachments: A three-dimensional finite element analysis. Angle Orthod. 2015;85:454-60.
- [CrossRef] [PubMed] [Google Scholar]
- Orthodontic treatment with clear aligners and the scientific reality behind their marketing: A literature review. Turk J Orthod. 2019;32:241-6.
- [CrossRef] [PubMed] [Google Scholar]
- Clear aligner technique In: Clincheck software design. United States: Quintessence Publishing; 2018. Ch. 4
- [Google Scholar]
- Principles and biomechanics of aligner treatment (1st ed). Netherlands: Elsiever; 2021. Ch. 2
- [Google Scholar]
- The Invisalign system-challenging movements. Available from: https://www.aligntechinstitute.com/files/atearchive/pdf/challengingmovements_10-507-final.pdf [Last accessed on 2007 Apr]
- [Google Scholar]
- The Readers' Corner 2. What percentage of your patients are being treated with invisalign appliances? J Clin Orthod. 2004;38:544-5.
- [Google Scholar]
- Influence of attachments and interproximal reduction on the accuracy of canine rotation with Invisalign. Angle Orthod. 2008;78:682-7.
- [CrossRef] [PubMed] [Google Scholar]
- Treatment outcome and efficacy of an aligner technique-Regarding incisor torque, premolar derotation and molar distalization. BMC Oral Health. 2014;14:68.
- [CrossRef] [PubMed] [Google Scholar]
- Has invisalign improved? A prospective follow-up study on the efficacy of tooth movement with invisalign. Am J Orthod Dentofacial Orthop. 2020;158:420-5.
- [CrossRef] [PubMed] [Google Scholar]
- Accuracy evaluation of orthodontic movements with aligners: A prospective observational study. Prog Orthod. 2022;23:2-8.
- [CrossRef] [PubMed] [Google Scholar]
- Efficacy of invisalign attachments: A retrospective study. Am J Orthod Dentofacial Orthop. 2021;160:250-8.
- [CrossRef] [PubMed] [Google Scholar]
- Predictability of orthodontic tooth movement with aligners: Effect of treatment design. Prog Orthod. 2023;24:2.
- [CrossRef] [Google Scholar]
- Clinical expression of programmed mandibular canine rotation using various attachment protocols and 1-vs 2-week wear protocols with Invisalign SmartTrack aligners: A retrospective cohort study. Am J Orthod Dentofacial Orthop. 2022;162:e103-15.
- [CrossRef] [PubMed] [Google Scholar]
- Effect of clear aligner attachment design on extrusion of maxillary lateral incisors: A multicenter, single-blind randomized clinical trial. Am J Orthod Dentofacial Orthop. 2023;164:618-27.
- [CrossRef] [PubMed] [Google Scholar]
- The efficacy of anterior open bite closure when using Invisalign's optimized extrusion versus conventional attachments. J World Fed Orthod. 2023;12:112-7.
- [CrossRef] [PubMed] [Google Scholar]
- How well does invisalign work? A prospective clinical study evaluating the efficacy of tooth movement with invisalign. Am J Orthod Dentofac Orthop. 2009;135:27-35.
- [CrossRef] [PubMed] [Google Scholar]
- Predicted and actual outcome of anterior intrusion with Invisalign assessed with cone-beam computed tomography. Am J Orthod Dentofacial Orthop. 2021;159:275-80.
- [CrossRef] [PubMed] [Google Scholar]
- Quantifying the efficacy of overbite reduction in patients treated with clear aligners using optimized versus conventional attachments. J World Fed Orthod. 2023;12:105-11.
- [CrossRef] [PubMed] [Google Scholar]
- The clear plastic appliance: A biomechanical point of view. Angle Orthod. 2008;78:381-2.
- [CrossRef] [PubMed] [Google Scholar]
- Efficiency evaluation of maxillary molar distalization using invisalign based on palatal rugae registration. Am J Orthod Dentofacial Orthop. 2022;161:e372-9.
- [CrossRef] [PubMed] [Google Scholar]
- Maxillary molar distalization with aligners in adult patients: A multicenter retrospective study. Prog Orthod. 2016;17:12.
- [CrossRef] [PubMed] [Google Scholar]
- Effectiveness of composite attachments in controlling upper-molar movement with aligners. J Clin Orthod. 2016;50:341-7.
- [Google Scholar]
- Predictability of maxillary molar distalization and derotation with clear aligners: A prospective study. Int J Environ Res Public Health. 2023;20:2941.
- [CrossRef] [PubMed] [Google Scholar]
- Upper second molar distalization with clear aligners: A finite element study. Appl Sci. 2020;10:7739.
- [CrossRef] [Google Scholar]
- Effects of variable composite attachment shapes in controlling upper molar distalization with aligners: A nonlinear finite element study. Hindawi J Healthc Eng. 2021;2021:5557483.
- [CrossRef] [PubMed] [Google Scholar]
- Predictability of lower incisor tip using clear aligner therapy. Prog Orthod. 2022;23:37.
- [CrossRef] [PubMed] [Google Scholar]
- Activation time and material stiffness of sequential removable orthodontic appliances. Part 3: Premolar extraction patients. Am J Orthod Dentofacial Orthop. 2008;133:837-45.
- [CrossRef] [PubMed] [Google Scholar]
- The effectiveness of the Invisalign appliance in extraction cases using the ABO model grading system: A multicenter randomized controlled trial. Int J Clin Exp Med. 2015;8:8276-82.
- [Google Scholar]
- Design of the Invisalign system performance. Semin Orthod. 2017;23:3-11.
- [CrossRef] [Google Scholar]
- Comparison of achieved and predicted tooth movement of maxillary first molars and central incisors: First premolar extraction treatment with Invisalign. Angle Orthod. 2019;89:679-87.
- [CrossRef] [PubMed] [Google Scholar]
- The predictability of orthodontic tooth movements through clear aligner among first-premolar extraction patients: A multivariate analysis. Prog Orthod. 2022;23:52.
- [CrossRef] [PubMed] [Google Scholar]
- Comparison of achieved and predicted crown movement in adults after 4 first premolar extraction treatment with Invisalign. Am J Orthod Dentofacial Orthop. 2021;160:805-13.
- [CrossRef] [PubMed] [Google Scholar]
- Relative anchorage loss under reciprocal anchorage in mandibular premolar extraction cases treated with clear aligners. Angle Orthod. 2023;93:375-81.
- [CrossRef] [PubMed] [Google Scholar]
- Treatment of severe anterior crowding with the invisalign G6 first-premolar extraction solution. J Clin Orthod. 2019;53:459-69.
- [Google Scholar]
- Torque and intrusion control of the upper incisors with a modified posted archwire. J Clin Orthod. 2015;49:201-3.
- [Google Scholar]




