

Translate this page into:
Orthodontic treatment of a patient with cutis laxa


*Corresponding author: Cansu Tüfekçi, Department of Orthodontics, Faculty of Dentistry, Akdeniz University, Antalya, Turkey. cansu.tufekci@hotmail.com
-
Received: ,
Accepted: ,
How to cite this article: Bolat Gümüş E, Tüfekçi C. Orthodontic treatment of a patient with cutis laxa. APOS Trends Orthod. doı: 10.25259/APOS_311_2024
Abstract
Cutis laxa syndrome is a connective tissue disease characterized by loss of skin elasticity and increased skin folds. In addition to systemic findings, the disease also has craniofacial findings. Together with skeletal developmental retardation, these individuals with a loose and saggy skin structure have an aging appearance, which leads to serious esthetic problems. This case report describes the orthodontic treatment approach for an individual with cutis laxa. Orthopedic treatment was planned to be applied to the patient with severe transversal insufficiency and increased vertical dimensions, taking advantage of the fact that the patient was in the growth development period, thus contributing to the improvement of the patient’s facial appearance. Accordingly, the patient was first treated with rapid maxillary expansion. Later, the treatment was completed with fixed treatment mechanics. The orthodontic treatment produced good functional and esthetic results and patient pleasure.
Keywords
Cutis laxa
Orthodontic treatment
Facial features

INTRODUCTION
Cutis laxa syndrome is a connective tissue disease characterized by loss of elasticity of the skin and increased skin folds. Increased skin folds are thought to be the result of a disturbance in the metabolism of dermal elastic fibers.[1] There are two types of this rare disease: Hereditary and acquired.[2] Although different from the subtypes, patients usually have typical facial features such as large ears, drooping cheeks, a long philtrum, and prominent nasolabial folds. In addition, skin folds, which are prominent features of the disease, cause an aged appearance when seen on the face.[3] The current facial findings of the syndrome cause serious esthetic problems in patients and cause individuals to isolate themselves from society with a lack of self-confidence. For these reasons, it is important to rehabilitate the physical appearance of individuals with the syndrome as well as treat their systemic findings. However, as a result of the literature review, it was noted that plastic surgery procedures were generally preferred to improve the facial findings of the patients, and few studies were found in which the syndrome was associated with orthodontic treatment. Orthodontic treatment can be considered as an alternative to improve the facial appearance of individuals with this rare syndrome. However, it should be taken into consideration that the decreased skin elasticity of the syndrome may limit skeletal manipulation during orthodontic treatment, and it should also be taken into consideration that soft tissue problems may recur even if facial improvement is achieved at the end of the treatment since the disorders in the connective structure will continue.
In this study, a 13-year-old individual with cutis laxa syndrome was presented, considering that orthodontic treatment may be an option in the facial rehabilitation of individuals with cutis laxa syndrome, especially in the growth and development period. Skeletal and dental disorders were improved with orthodontic treatment, and soft tissue defects were camouflaged. It was aimed to contribute to the literature by looking at the treatment of individuals with the syndrome from a different perspective.
CASE REPORT
A 13-year-old girl presented in 2022 to the Department of Orthodontics, Faculty of Dentistry, University. Her chief complaint was that her teeth were crowded, and she could not have a beautiful smile. In the medical anamnesis of the patient, it was learned that she was followed up by the pediatric genetics department with a diagnosis of cutis laxa. An extraoral examination revealed typical facial findings of cutis laxa syndrome. Facial dysmorphism, including a convex profile with increased lower facial height, increased filtrum length, and inability to close the lips, are the findings detected during the extraoral examination [Figure 1]. Intraoral examination revealed a class II molar relationship with a 4 mm overjet, moderate crowding, non-overlapping upper and lower midlines, and a V-shaped maxillary arch. The patient also had a narrow and deep maxilla [Figure 2].

- (a) pre-treatment extraoral photographs; (b) pre-treatment intraoral photographs.
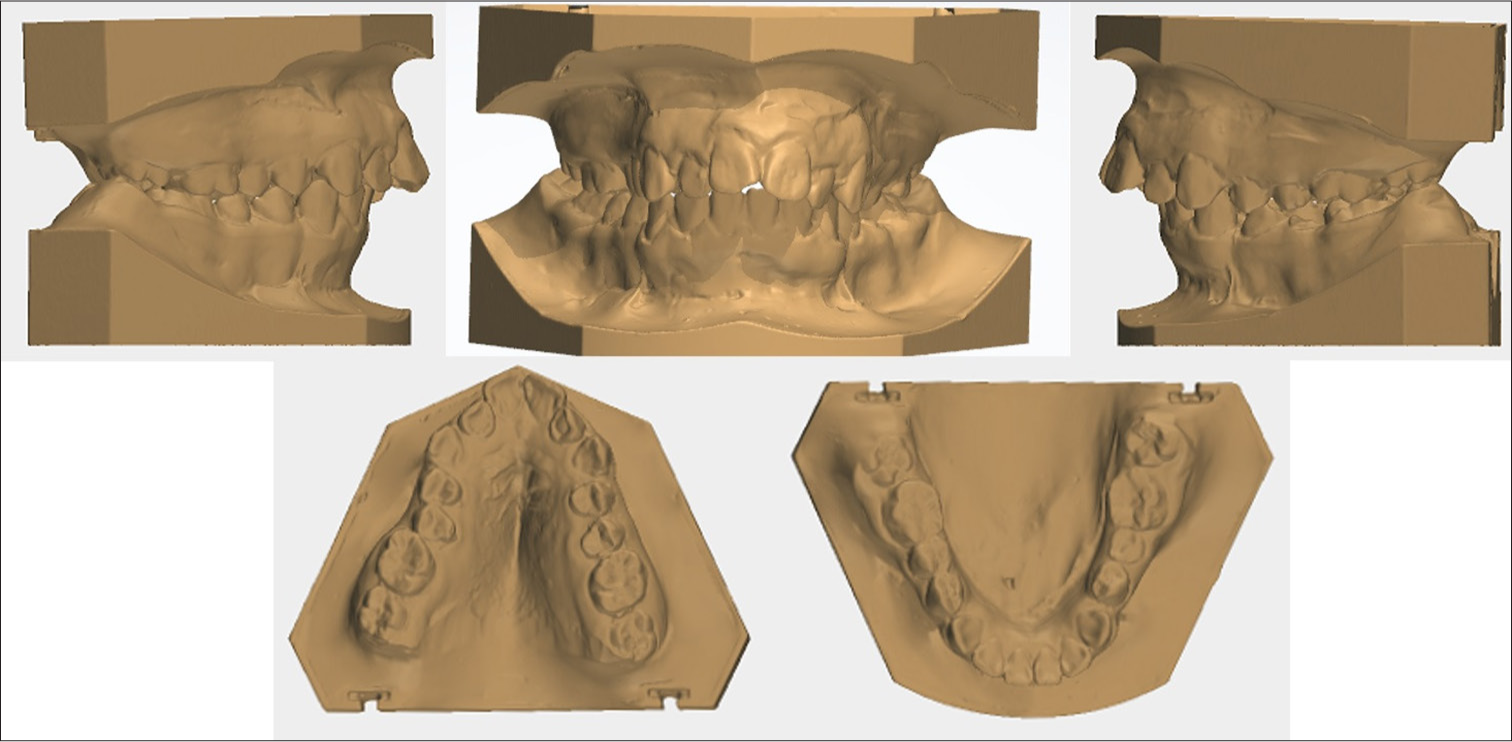
- Pre-treatment study models.
Radiographic examination revealed that the third molars were missing, and the loss of material in the lower left second premolar was noted. No other pathological findings were found. According to the hand-wrist radiograph taken to determine the growth development, it was determined that the patient was in the Dp3u period [Figure 3]. Cephalometric analysis revealed a Class II relationship with a retrusive maxilla (SNA, 71,8) and mandible (SNB, 62,8) and a vertical growth pattern (SN-GoGn, 59,2). The upper incisors were in normal inclination (U1-NA: 23,6°), and the lower incisors were protrusive (U1-NB: 40,8°, IMPA: 96°) [Table 1].
| Norms | Pretreatmant | Posttreatment | |
|---|---|---|---|
| Skeletal anlaysis | |||
| SNA (°) | 82±2 | 71.8 | 72.3 |
| SNB (°) | 80±2 | 62.8 | 60.7 |
| ANB (°) | 2±2 | 9 | 11.6 |
| SN-GoGn (°) | 32±4 | 59.2 | 63.5 |
| Dental analysis | |||
| U1-NA (°) | 22±4 | 23.6 | 7.8 |
| U1-NA (mm) | 4±2 | 7.9 | –1 |
| L1-NB (°) | 25±4 | 40.8 | 38.9 |
| L1-NB (mm) | 4±2 | 14.8 | 13.2 |
| IMPA (°) | 90±5 | 96 | 91.6 |
| Facial analysis | |||
| S-Line/UL (mm) | 0±1.5 | 7.4 | 4.9 |
| S-Line/LL (mm) | 0±2 | 10.9 | 7.8 |
SNA: Sella-Nasion-point A; SNB: Sella-Nasion-point B; ANB: point A-Nasion-point B; SN-GoGn: Sella- Nasion Gonion-Gnathion Angle;
U1: Upper central incisor; NA: Nasion point A; L1: Lower central incisor; NB: Nasion point B; IMPA: Lower central incisor mandibular plane angle; LL: Lower lip; UL: Upper lip
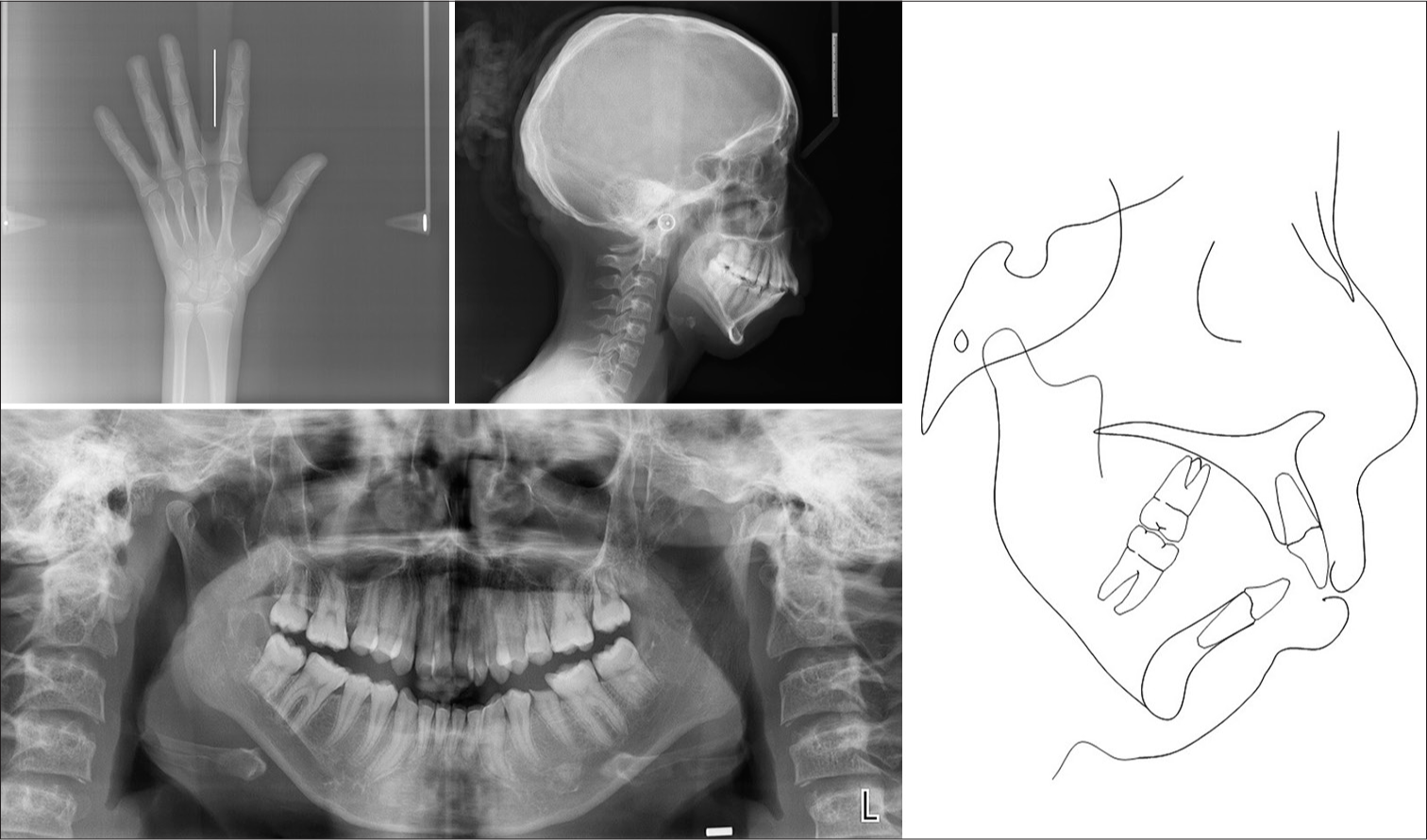
- (a) Pre-treatment hand-wrist radiograph; (b) pre-treatment lateral cephalogram; (c) pre-treatment panoramic radiograph; (d) pre-treatment cephalometric tracing
Treatment objectives
The main goals of treatment are (1) correction of transversal disharmony, (2) correction of vertical discrepancy, (3) removal of crowding in the maxillary and mandibular arch, (4) establishment of a stable Class I canine relationship and Class II molar relationship, and (5) improvement of tooth and facial structure. Thus, it is aimed to camouflage the facial appearance with skeletal and dental corrections independently of the defects in the dermal structure.
Treatment alternative
Another treatment alternative to improve the facial esthetics of the patient with transversal and vertical skeletal deviations was maxillary impaction. However, the fact that the patient was in the growth and development stage was an advantage, and skeletal correction with orthopedic treatment was considered. After orthopedic treatment, tooth extraction was planned to eliminate class II occlusion and increased overjet. So that an adequate lip closure would be provided and the patient’s vertical dimension would be kept under control. Alternatively, distalization with Temporary anchorage devices (TADs) mechanics can be considered. However, it was not preferred because it is an invasive method and may lead to undesirable results in the vertical aspect of the patient and worsen facial esthetics.
Treatmant progress
Because of the genetic disorder, before starting orthodontic treatment, it was decided to obtain medical authorization from the patient’s physician. The patient required antibiotic premedication before each appointment with a risk of bleeding due to a history of heart disease due to cutis laxa.
A two-stage treatment plan was planned to improve the patient’s facial esthetics and to correct the maxillary transversal deficiency. In the first stage, it was aimed to widen the narrow maxillary arch, and in the second stage, it was planned to finish the treatment of the patient with fixed orthodontic mechanics. The lower second premolar tooth with loss of material was retained until the end of the treatment and restored at the end of the treatment.
In the first stage of the treatment, an acrylic Mcnamara type expansion appliance was used for maxillary expansion, which included the posterior teeth with Hyrax screws. In addition, it was aimed to use occipital headgear with expansion by adding headgear tubes at the upper first molar level of the appliance. The rapid maxillar expander is cemented to the teeth with glass ionomer cement. The screw of the rapid maxillary expansion (RME) appliance was activated twice a day (0.5 mm/day) in the 1st week, and after the sutural opening was determined at the end of the 1st week, it was activated once (0.25 mm/day) a day, and the expansion was completed in a total of 3 weeks. Occipital headgear was applied at the same time with RME, and a force of 500 g was applied unilaterally. After the RME screw was fixed following expansion, the patient was waited for 3 months for retention and then the second phase of treatment was started.
In the second stage of treatment, fixed treatment with tooth numbers 14–24 extractions was planned. McLaughlin and Bennett System (MBT) brackets with 0.022 inch slots were used, and segmental mechanics were applied with 0.017 × 0.025 nickel-titanium wire in the upper arch. Fixed treatment of the lower arch was started at the same time as the upper arch. The canines were distalized with 3/16 heavy class II elastics. After class I relationship was achieved in the canines, palatinal root torque was applied to the incisors and incisor retraction was performed with bull loops. The active treatment period was completed in a total of 22 months. At the end of the treatment, upper and lower lingual retainers and Essix plaques were applied for retention.
Treatmant results
Because the patient was in the growth and development stage, maxillary expansion was obtained as a result of RME, and the maxillary deficiency in the transversal aspect was corrected. A stable class 2 occlusal relationship with maximum intercuspation and acceptable overjet and overbite was achieved. The crowding in the upper and lower dental arches was resolved, and extraction spaces were closed. Adequate lip closure was achieved by eliminating the overjet and uprighting the upper incisors. Thus, it contributed to the improvement of the patient’s facial esthetics. In addition, the vertical aspect dimensions were controlled throughout the treatment [Figure 4].

- (a) post-treatment extraoral photographs; (b) post-treatment intraoral photographs.
Cephalometric superimpositions revealed several key changes in the dental and skeletal relationships [Figures 5 and 6]. Although it is aimed to keep the increased vertical dimensions under control, the amount of vertical dimension has increased as a result of posterior rotation of the mandible with growth and development. The increase in the ANB angle is associated with a similar reason. In addition, with the decrease in the upper incisor angle, adequate lip closure was obtained with the ideal closure of the lips.
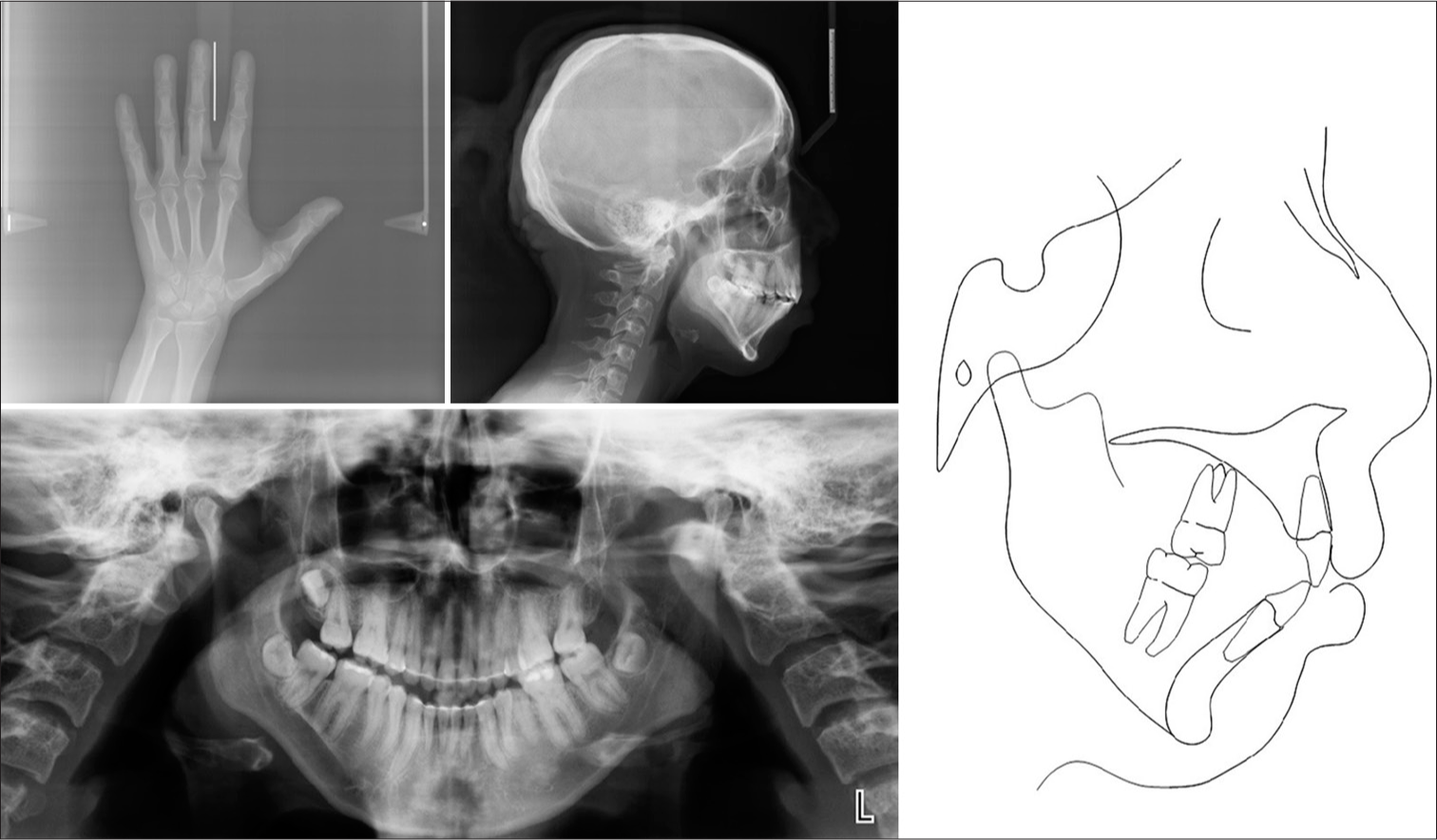
- (a) Post-treatment hand-wrist radiograph; (b) post-treatment lateral cephalogram; (c) post-treatment panoramic radiograph; (d) post-treatment cephalometric tracing.
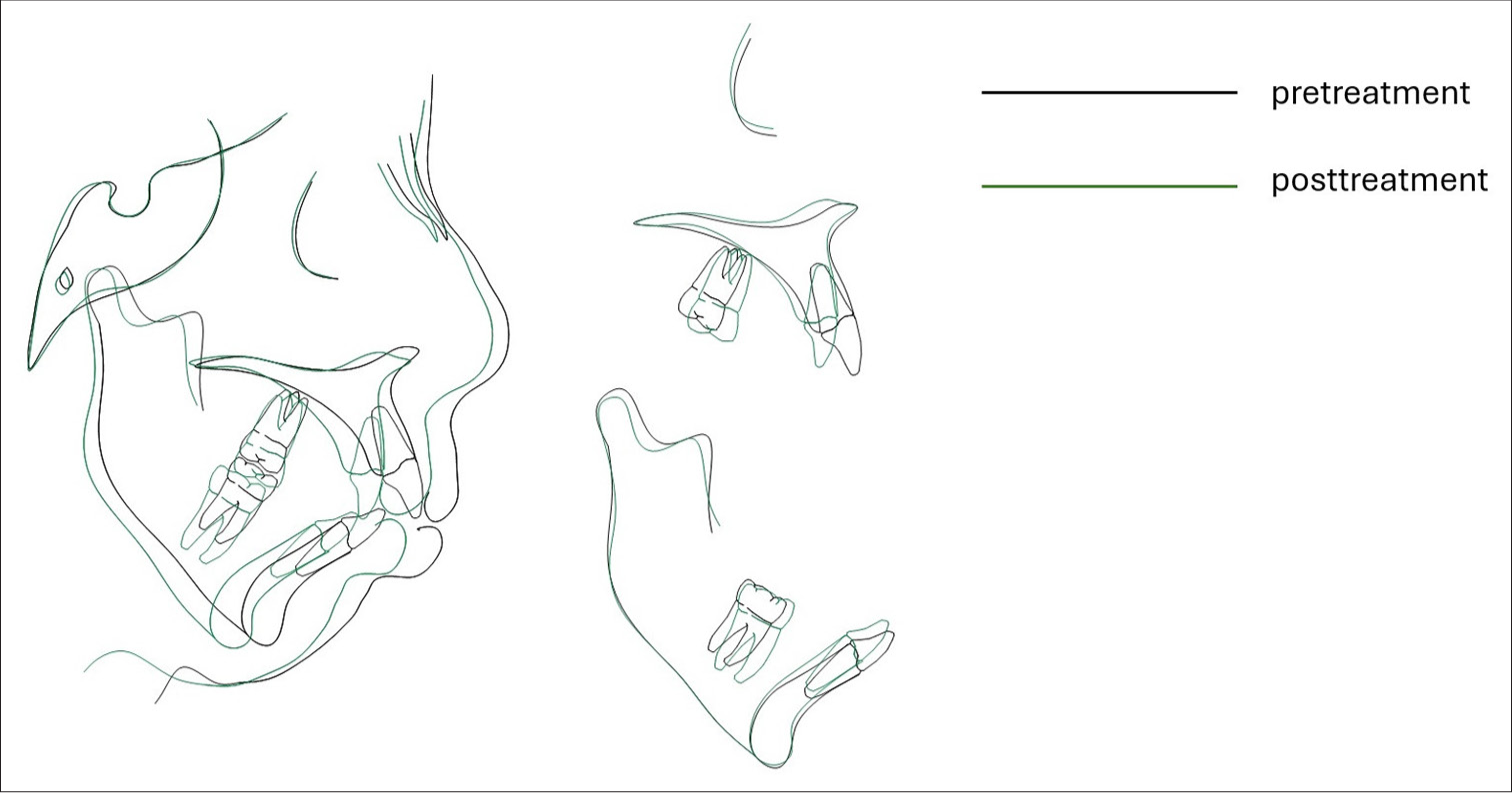
- Cephalometric superimposition showed significant maxillary incisor retrusion. It also resulted in clockwise rotation of the mandible.
It is known that the establishment of a good occlusion is an important factor for the long-term stability of the treatment results. In the present case, an ideal molar and canine relationship with adequate overjet and overbite was achieved at the end of the treatment. In addition, fixed lingual retainers and Essix plaques were used for retention. However, the negativities that may be observed in the soft tissue with age may need to be supported by plastic surgery or similar applications in the future. Therefore, attention should be paid to long-term follow-up in patients with such rare anomalies.
DISCUSSION
As a result of the literature review, limited studies evaluating cutis laxa syndrome in dentistry were found. It is noticed that systemic findings of the disease are generally focused on and oral and craniofacial features are not adequately evaluated. For this reason, it is thought that our study will contribute to the literature.
In the study by Beyens et al.,[1] facial features such as a long face, drooping cheeks, and increased filtrum length were found in most of the subtypes of Cutis Laxa syndrome. In addition, in the literature review by Steiner et al., it was stated that sagging and flaring of the lower lip may lead to eclabium, and ectropion may occur in the lower eyelids.[4] Similar findings were also presented in our patient, and it was observed that the findings of facial disformism were consistent with the literature. However, as seen in our patient, there is a consensus among researchers that individuals may generally have an aging appearance concerning the facial features of the syndrome.[1,3]
In addition to prominent dermatological features, the syndrome also has craniofacial findings. Especially, forehead dislocation, dolichofacial face shape, narrow maxillary arch, malar-maxillary hypoplasia, and prognathism are skeletal findings of the syndrome and may lead to serious esthetic and functional problems if left untreated.[5] Our patient also had craniofacial features associated with the syndrome, such as a narrow maxillary arch and hyperdivergent facial pattern, and these craniofacial features may be thought to occur as a result of the limitation of normal development of the underlying skeletal structures due to decreased skin elasticity.
The aged appearance seen in individuals with Cutis laxa syndrome may affect individuals esthetically and may cause a loss of confidence, especially socially. For this reason, while planning the treatment, it should be aimed to help the patient psychologically as well as to contribute functionally and esthetically. In literature, plastic surgery approaches are generally considered for the facial features of these patients, but in the case report prepared by Carrillo and Rossouw,[6] it was observed that an individual with cutis laxa syndrome was rehabilitated with orthodontic treatment. Since our patient was also in the growth and development period and was an alternative to surgical methods, a treatment plan was made to improve the skeletal structure and thus the facial appearance with orthopedic treatment. During the treatment planning, maxillary expansion with Mcnamara-type RME was performed to correct the existing skeletal disorders, and vertical direction control was performed with occipital headgear, which continued to be used throughout the treatment. In the fixed treatment phase, teeth numbered 14–24 extractions were planned, incisor retraction was performed, and a balanced occlusion with adequate lip closure, ideal overjet, and overbite was obtained at the end of the treatment.
Our current study sheds light on the literature on the effect of cutis laxa syndrome on craniofacial structures and orthodontic treatment, but it is thought that a larger perspective will be achieved with further studies.
CONCLUSION
In this patient, the treatment goals were achieved. Since the patient was in the growth and development period, the facial appearance of the patient was improved with non-invasive orthopedic and orthodontic methods. Moreover, the patient was reintegrated into society by increasing self-confidence.
Ethical approval
Institutional Review Board approval is not required.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship: Nil.
References
- Cutis laxa: A comprehensive overview of clinical characteristics and pathophysiology. Clin Genet. 2021;99:53-66.
- [CrossRef] [PubMed] [Google Scholar]
- Cutis laxa of the autosomal recessive type in a consanguineous family. Eur J Dermatol. 2003;13:529-33.
- [Google Scholar]
- New insights into the pathogenesis of autosomal-dominant cutis laxa with report of five ELN mutations. Hum Mutat. 2011;32:445-55.
- [CrossRef] [PubMed] [Google Scholar]
- Cutis laxa with growth and developmental delay, wrinkly skin syndrome and gerodermia osteodysplastica: A report of two unrelated patients and a literature review. Genet Mol Biol. 2005;28:181-90.
- [CrossRef] [Google Scholar]
- Gerodermia osteodysplastica and wrinkly skin syndrome: Are they the same. Am J Med Genet. 2001;101:213-20.
- [CrossRef] [PubMed] [Google Scholar]
- Orthodontic treatment for a patient with congenital cutis laxa. Am J Orthod Dentofacial Orthop. 2009;136:282-9.
- [CrossRef] [PubMed] [Google Scholar]




