

Translate this page into:
A standardized hands-on protocol effectively enhanced orthodontic education on bonding clear aligner attachments


*Corresponding authors: Yu Li, State Key Laboratory of Oral Diseases, National Center for Stomatology, National Clinical Research Center for Oral Diseases, Department of Orthodontics, West China Hospital of Stomatology, Sichuan University, Chengdu 610041, Sichuan, China. yuli@scu.edu.cn
-
Received: ,
Accepted: ,
How to cite this article: Li S, Mei L, Yi J, Abdulghani EA, Zheng W, Li Y. A standardized hands-on protocol effectively enhanced orthodontic education on bonding clear aligner attachments. APOS Trends Orthod. 2024;14:57-63. doi:10.25259/APOS_89_2023
Abstract
Objectives:
The objectives of this study were to develop and evaluate the effectiveness of a hands-on approach for training orthodontic postgraduates to bond clear aligner (CA) attachments.
Material and Methods:
Twenty orthodontic novice postgraduate students were recruited for the study and randomly divided into two groups. The training group (n = 10) received theory teaching followed by a hands-on training approach; the control group (n = 10) received only theory teaching. The students’ performance of bonding attachments, including bonding failure, marginal flash, and morphological defects, was assessed by a panel of clinical supervisors.
Results:
The hands-on training approach promoted the students’ performance of bonding CA attachments, with an increased success rate (from 34% ± 6% to 81% ± 6%, P < 0.01) and a reduced operating time (from 89 ± 5 min to 65 ± 4 min, P < 0.01) compared with the control group. The most challenging parts of attachment bonding were found to be resin loading, followed by template removal and flash removal.
Conclusion:
The hands-on approach developed in the present study was effective to train orthodontic postgraduates to bond CA attachments, with an increased success rate and reduced operating time.
Keywords
Dental education
Orthodontics
Attachment bonding
Clear aligner
Invisalign

INTRODUCTION
Clear aligners (CAs) have become increasingly popular for orthodontic treatment, due to the advantages such as comfort, esthetics, enhanced periodontal health, and less prevalence of apical root resorption.[1-3] A recent study highlighted that 79% of clinicians incorporate CA in their practices, and this proportion has been increasing in the past five years.[4] The CA companies and brands have also been increasing rapidly year by year.[5] In addition, during the challenging COVID-19 pandemic, CA wearers reportedly faced fewer complications and exhibited lower levels of depression compared to those with fixed orthodontic devices.[6]
For effective CA treatment, several attachments, primarily made of composite resin, are bonded to the teeth to enhance precision and efficiency in tooth movement.[7] These attachments are composite resin structures that are often bonded on the buccal or lingual surfaces of the teeth to maximize the retention of CA and facilitate tooth movement.[8] Their incorporation has expanded CA’s clinical application, making it suitable for a diverse array of malocclusions.[9] It has been found that CA attachments can increase treatment efficacy by improving mesiodistal movement, anterior root torque, and rotation.[7]
The precision of bonding CA attachments plays a pivotal role in ensuring optimal clinical outcomes. Conversely, subpar bonding can distort the force dynamics, impeding tooth movement, and jeopardizing overall treatment.[10,11] Some errors in bonding attachments have often been observed in the clinic, especially in the postgraduate students and junior clinicians,[8] such as bonding failure, marginal flash, and morphological defects. Despite the pressing need, a comprehensive and standardized training regimen addressing these concerns remains elusive in academic literature.
The aim of this study was to develop a standardized protocol, including theory and hands-on approach, for training postgraduates to bond CA attachments, and evaluate its effectiveness.
MATERIAL AND METHODS
This study was approved by the Ethics Committee of West China Hospital of Stomatology, Sichuan University (WCHSIRB-CT-2021-402). A total of 20 participants were recruited in the study, and the sample size was calculated based on the previous literature,[12] with α = 5% and β = 10%, allowing for a 20% dropout. These participants were postgraduate orthodontic novices who had the basic dental lectures and clinical practice, without any exposure to the CA treatment or attachment bonding.
The participants were randomly divided into the training group (n = 10) and control group (n = 10).
Training group
A standardized training protocol for bonding CA attachments was developed, including video and oral instructions followed by the hands-on practice developed in the present study.
For the theory teaching part, the students firstly learned the bonding procedures by watching the Invisalign official video for bonding attachments (https://learn.invisalign.com/videos) under the supervision of a clinical supervisor. The supervisor explained each procedure in detail to make sure that each student fully understood the bonding process.
The hands-on practical training was performed on the three dimensional (3D) printed models of a CA patient, featuring a total of 19 attachments (ten rectangular and nine optimized) and 2 mm crowding, under the supervision using a tell-show-do teaching model [Figure 1]. The most used anterior and posterior attachments, as well as conventional and optimized attachments, were bonded using the templates provided by Align Technology.
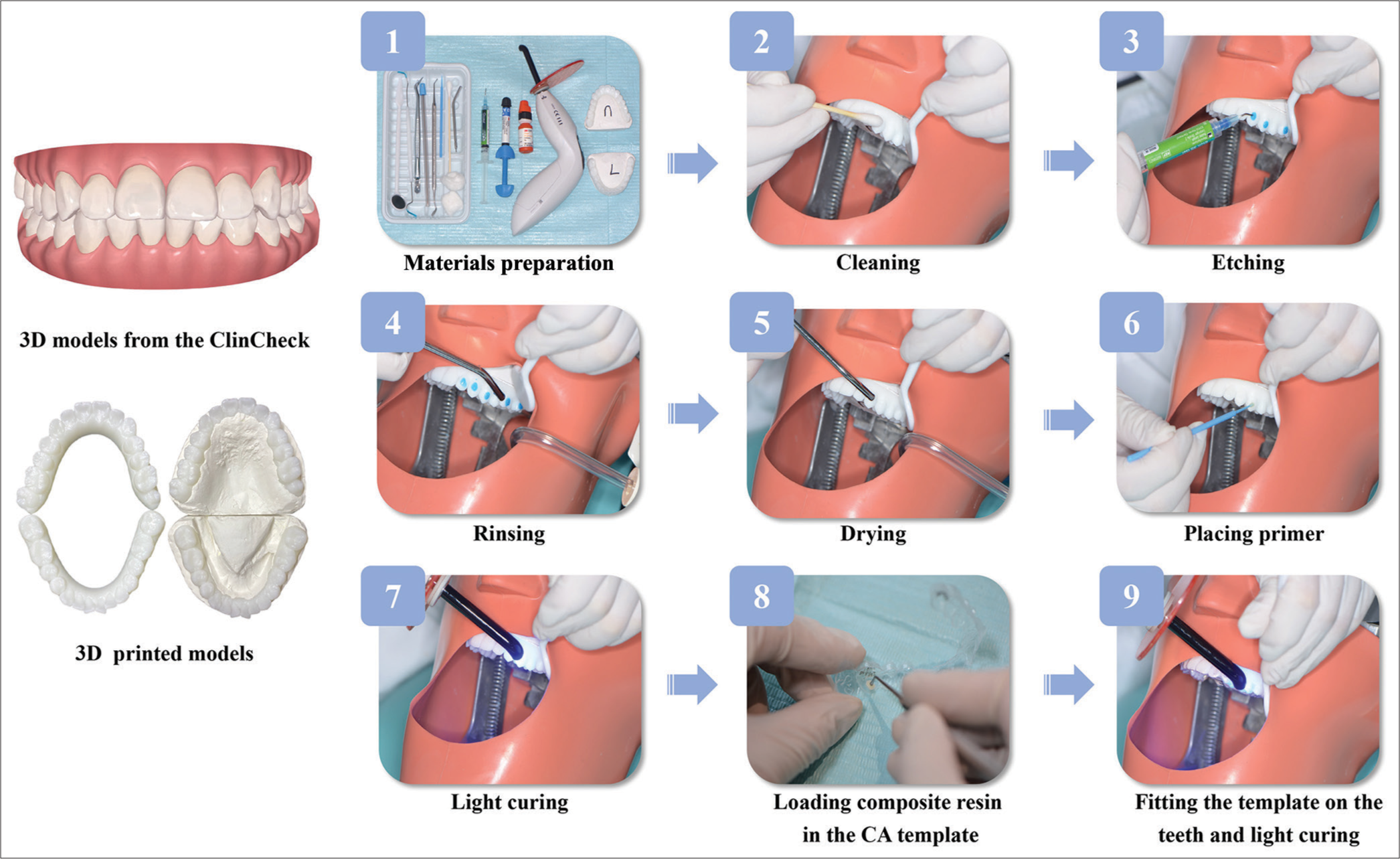
- Flow chart of bonding clear aligners attachments: (1) Material preparation, (2) cleaning, (3) etching, (4) rinsing, (5) drying, (6) placing primer, (7) light curing, (8) loading composite resin in the clear aligner template, (9) and fitting the template on the teeth and light curing; 3D: three-dimensional.
The bonding protocol was standardized, including material preparation, cleaning, etching, rinsing, drying, placing primer, light curing, loading composite resin in the CA template, and fitting the template on the teeth and light curing [Figure 1]. Students were taught to load the composite resin Filtek Z350XT (3M ESPE Dental Products, USA) flush with the edge of the template, and tamp down the occlusal template surface to tightly fit to the teeth surfaces.
Control group
Students in the control group received the same theory teaching (i.e., oral and video instructions) as the training group, however, did not have practical hands-on training.
For ethical consideration, the control group received a catch-up practical hands-on training (the same as the training group) after the completion of this study.
Students’ performance and learning experience
A testing case, with similar dental condition and attachments as the training case was selected from the Invisalign database to test, and evaluate the students’ performance of bonding attachments (nineteen total attachments, eleven rectangular attachments, and eight optimized attachments, and two mm crowding). Both groups bonded the attachments on the testing models under the same environment as the training session.
Students’ performance was evaluated and scored by two experienced orthodontists, who had profound experience in aligner orthodontics and were blinded to the grouping. The parameters evaluated were attachment position, bonding failure, morphological defects, and marginal flash, as well as the students’ operation time. Qualified attachments were in the correct position, with complete shape, and without obvious marginal flash. Unqualified attachments were marked with specific reasons, including incorrect position, morphological defect, marginal flash, and falling off. To observe the students’ learning curve, the training group did three exercises at an interval of one week. In addition, the students’ learning experience in the training group was investigated using a questionnaire survey [Table 1].
Statistical analysis
GraphPad Prism 9 (GraphPad Software, San Diego, California) was used for the statistical analysis. The student’s t-test was used for statistical comparisons. The significance level was set as P < 0.05.
RESULTS
The training group had a higher bonding success rate (81% ± 6%) [Figure 2a] and shorter operation time (65 ± 4 min) [Figure 2b] than the control group (34% ± 6% and 89 ± 5 min, respectively).
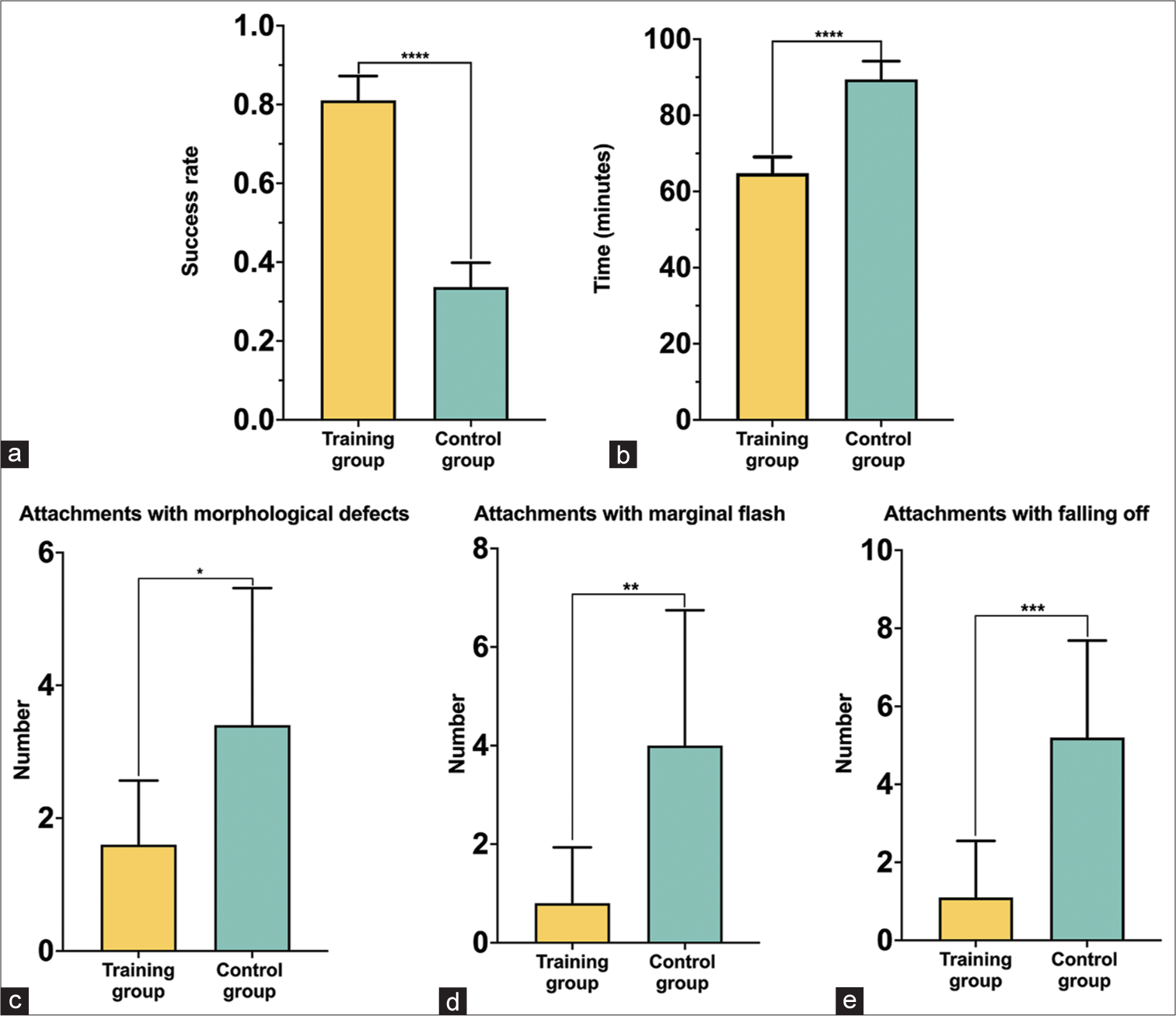
- Comparison of the training group and control group. (a) Bonding success rate, (b) operation time, (c) the number of attachments with morphological defects, (d) the number of attachments with marginal flash, and (e) the number of attachments with falling off. *P < 0.05, **P < 0.01, ***P < 0.001, ****P < 0.0001.
The bonding failure (number of attachments with morphological defects, marginal flash, and falling off) in the training group (19% ± 6%) was lower than that in the control group (66% ± 6%) (P < 0.05 for all) [Figure 2c-e]. The inter-doctor reliability was calculated by Cohen’s kappa (Kappa score = 0.91). The bonding success rate in the training group was higher than that in the control group, regardless of the type of attachments (conventional or optimized attachments) [Figure 3].
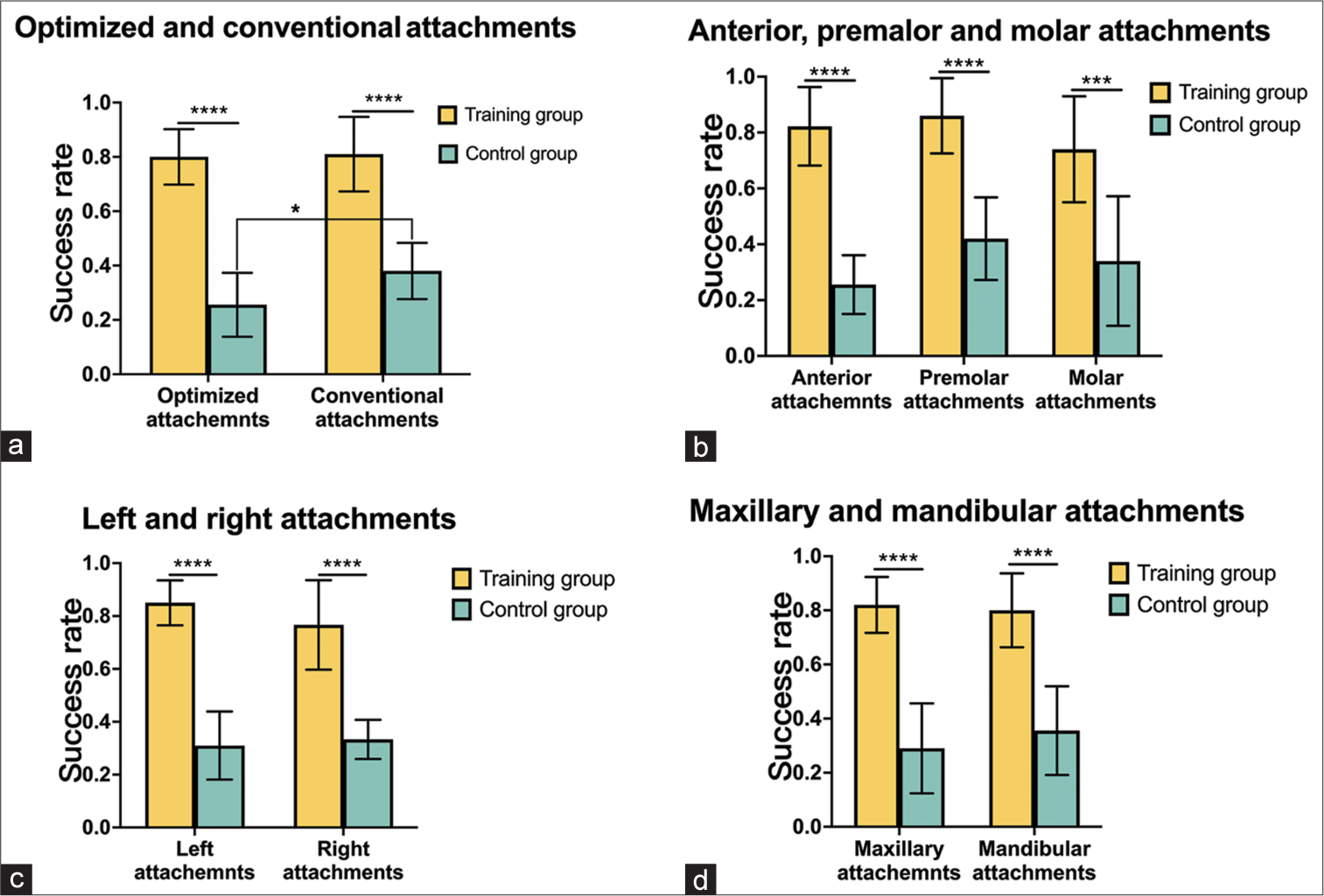
- Comparison of the success rate of different attachments between the training group and control group. (a) Optimized and conventional attachments, (b) anterior, premolar, and molar attachments, (c) left and right attachments, and (d) maxillary and mandibular attachments. *P < 0.05, ***P < 0.001, ****P < 0.0001.
The students’ learning curve analysis showed that with the increase of practice, the bonding success rate was improved, the operation time was shortened [Figure 4a and b], and the bonding defects rate was reduced [Figure 4c-e].

- The learning curve of the students in the training group. (a) Bonding success rate, (b) operation time, (c) the number of attachments with morphological defects, (d) the number of attachments with marginal flash, and (e) the number of attachments with falling off. ns: No significance, ***P < 0.001, ****P < 0.0001.
The questionnaire survey showed that 90% of the students felt that the attachment bonding was difficult, and the most tough procedure was “loading the composite resin in the template” [Table 1]. All students (100%) believed that this hands-on practice was very helpful for learning, and most of them (90%) felt confident to bond attachments after the training [Table 1].
| Questionnaire list | Percentage |
|---|---|
| 1. Do you think attachment bonding is difficult? | |
| A. Difficult | 30 |
| B. Acceptable | 60 |
| C. Easy | 10 |
| 2. Which step do you think is the most difficult for attachment bonding? | |
| A. Etching and bonding | 0 |
| B. Loading attachment template | 90 |
| C. Template removal and flash removal | 10 |
| 3. Do you think this training program is helpful for you to master attachment bonding? | |
| A. Very helpful | 70 |
| B. A little helpful | 30 |
| C. Little helpful | 0 |
| 4. Which teaching method do you prefer? | |
| A. Watching videos | 20 |
| B. Theoretical interpretation | 0 |
| C. Practical instruction | 80 |
| 5. How many times do you think the attachment bonding exercise is appropriate | |
| A. 1–2 | 0 |
| B. 3 | 70 |
| C. ≥4 | 30 |
| 6. How well do you think you master attachment bonding through this training program? | |
| A. > 60% | 90 |
| B. 30–60% | 10 |
| C. <30% | 0 |
| 7. Do you hope this training program to be included in orthodontic teaching | |
| A. Very hope | 70 |
| B. A little hope | 30 |
| C. Not hope at all | 0 |
DISCUSSION
Attachments are pivotal in CA treatment, contributing to enhanced 3D control of tooth motions, improved aligner retention, and more efficient orthodontic force delivery.[7] Typodont has been commonly used in dental orthodontic teaching and practice for decades,[13,14] but training in bonding CA attachments on a typodont has not been reported. This study, to the best of our knowledge, was the first study that developed a standardized hands-on approach for training bonding attachments. This standardized training protocol significantly enhanced the students’ performance with a greater bonding success rate, less operation time, and less bonding defects. It is practical, convenient, effective, and economical for orthodontic education. Invisalign is the first CA brand with the greatest number of CA patients all over the world, and therefore, it was used in this study.
Composite resins are often used for bonding CA attachments. They have good mechanical and biological properties, esthetic shade, and are easy to use.[15] In the present study, 3M Filtek Z350XT composite resin was selected based on the literature. Chen et al. compared three different composite materials (Filtek Z350XT, Filtek Z350XT Flowable, and SonicFill) and assessed their operation time, shear bond strength, placement accuracy, and wear resistance, finding that the Filtek Z350XT Flowable had shorter operation time and less possibility of falling off.[16] On the contrary, another study done by Alsaud et al. found that the Filtek Z350XT had better shear bond strength than the Filtek Z350XT Flowable; furthermore, the Filtek Z350XT Flowable caused more resin materials overflowing under the pressure when tamping down the template, leading to attachments marginal flash.[17] In addition, the low elastic modulus of Filtek Z350XT Flowable made it easy to deform under stress;[15] therefore, the 3M Filtek Z350XT composite resin was used in the present study.
The most challenging aspect of bonding attachments, as highlighted in our study, is the correct loading of the composite resin. It is also of clinical importance. For example, if the loaded composite resin is excessive, the composite flash on the tooth surface would cause clinical problems, such as bacterial adhesion, enamel demineralization,[18] poor retentions, and off-track.[19] It is recommended to carefully clean the excessive composite resin. If the loaded composite resin is insufficient, attachments may have morphology defects or irregular shapes, resulting in poor retention and attachment loss. It has been found that these problems can prolong the treatment time, increase the number of revisits, and deteriorate the treatment result.[11]
The traditional teacher-centric education model has faced challenges, such as a singular teaching method, resource-intensive nature, limited data retention, and lack of repeatability.[20,21] Over the recent past, innovative educational strategies like the flipped classroom have emerged to elevate teaching quality.[21] The flipped classroom is a blended learning style in which students access teaching content before class, enabling interactive and collaborative activities during class. Analogous to the flipped classroom, the students in the present study received the theory teaching with the Invisalign official video for bonding attachments, followed by hands-on practical training on the 3D printed models. This standardized training protocol for bonding CA attachments provided a flexible platform for self-paced learning, and significantly improved the learning interests and training effects for orthodontic novice students.
It is generally acknowledged that the live demonstration teaching model is an efficient teaching approach in dental and orthodontic education. In the present study, video demonstration was integrated with the supervisor’s interpretation, offering media-rich audio and visual stimulation.[22] Several studies compared the teaching effect of the two methods and found that the procedural video demonstration was as effective as the live demonstration, and some students even thought that procedural video provided better visualization of operating steps.[20,21,23] Moreover, video demonstration can overcome some drawbacks of live demonstration, such as teacher dependency, inadequate field of view, and non-repeatability.[24]
CA attachments include the conventional and optimized attachments, and their efficacy for moving teeth has been investigated.[25] This study found that the quality of the conventional attachment bonding seemed slightly higher than that of the optimized attachments. This might be due to the irregular shape of the optimized attachment, making it more difficult for the novices to recognize the boundary when loading composite resin in the template. Loading too much or too little resin may result in attachments marginal flash or morphological defects, respectively.
CONCLUSION
The standardized hands-on protocol effectively enhanced orthodontic education on bonding CA attachments, with an increased success rate and reduced operating time.
Acknowledgments
The authors wish to thank all staff and students who participated in this study, for their time and commitment.
Ethical Approval
Approved by the Institutional Ethics Committee at West China Hospital of Stomatology, Sichuan University, number WCHS-IRB-CT-2021-402, dated 26 August 2021.
Declaration of patient consent
Patient’s consent not required as there are no patients in this study.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Major Special Science and Technology Project of Sichuan Province (grant no. 2022ZDZX0031).
References
- Periodontal health during clear aligners treatment: A systematic review. Eur J Orthod. 2015;37:539-43.
- [CrossRef] [PubMed] [Google Scholar]
- Periodontal health during orthodontic treatment with clear aligners and fixed appliances: A meta-analysis. J Am Dent Assoc. 2018;149:712-20.e12.
- [CrossRef] [PubMed] [Google Scholar]
- Prevalence and severity of apical root resorption during orthodontic treatment with clear aligners and fixed appliances: A cone beam computed tomography study. Prog Orthod. 2020;21:1.
- [CrossRef] [PubMed] [Google Scholar]
- Clear aligner treatment: Different perspectives between orthodontists and general dentists. Prog Orthod. 2019;20:10.
- [CrossRef] [PubMed] [Google Scholar]
- Clear aligners brands and marketing claims: An overview of available information on the web. Australas Orthod J. 2022;38:1-11.
- [CrossRef] [Google Scholar]
- The impact of the COVID-19 epidemic on orthodontic patients in China: An analysis of posts on weibo. Front Med (Lausanne). 2020;7:577468.
- [CrossRef] [PubMed] [Google Scholar]
- Effects of composite attachments on orthodontic clear aligners therapy: A systematic review. Materials (Basel). 2022;15:533.
- [CrossRef] [PubMed] [Google Scholar]
- Orthodontics: Current principles and techniques, 6th ed. Am J Orthod Dentofacial Orthop. 2018;153:162.
- [CrossRef] [Google Scholar]
- Risk factors of composite attachment loss in orthodontic patients during orthodontic clear aligner therapy: A prospective study. Biomed Res Int. 2021;2021:6620377.
- [CrossRef] [PubMed] [Google Scholar]
- Effects of variable attachment shapes and aligner material on aligner retention. Angle Orthod. 2015;85:934-40.
- [CrossRef] [PubMed] [Google Scholar]
- Treatment outcome and efficacy of an aligner technique--regarding incisor torque, premolar derotation and molar distalization. BMC Oral Health. 2014;14:68.
- [CrossRef] [PubMed] [Google Scholar]
- Comparison of inclination and vertical changes between single-wire and double-wire retraction techniques in lingual orthodontics. Korean J Orthod. 2020;50:26-32.
- [CrossRef] [PubMed] [Google Scholar]
- Force direction using miniscrews in sliding mechanics differentially affected maxillary central incisor retraction: Finite element simulation and typodont model. J Dent Sci. 2019;14:138-45.
- [CrossRef] [PubMed] [Google Scholar]
- Surface wear of resin composites used for invisalign® attachments. Acta Odontol Latinoam. 2017;30:90-5.
- [Google Scholar]
- Comparative study of three composite materials in bonding attachments for clear aligners. Orthod Craniofac Res. 2021;24:520-7.
- [CrossRef] [PubMed] [Google Scholar]
- Bonding of clear aligner composite attachments to ceramic materials: An in vitro study. Materials (Basel). 2022;15:4145.
- [CrossRef] [PubMed] [Google Scholar]
- The oral microbiota changes in orthodontic patients and effects on oral health: An overview. J Clin Med. 2021;10:780.
- [CrossRef] [PubMed] [Google Scholar]
- Clear aligners: Between evolution and efficiency-a scoping review. Int J Environ Res Public Health. 2021;18:2870.
- [CrossRef] [PubMed] [Google Scholar]
- Live demonstration versus procedural video: A comparison of two methods for teaching an orthodontic laboratory procedure. BMC Med Educ. 2015;15:199.
- [CrossRef] [PubMed] [Google Scholar]
- Comparing flipped classroom and conventional live demonstration for teaching orthodontic wire-bending skill. PLoS One. 2021;16:e0254478.
- [CrossRef] [PubMed] [Google Scholar]
- Effect of a procedural video CD and study guide on the practical fixed prosthodontic performance of Iranian dental students. J Dent Educ. 2012;76:354-9.
- [CrossRef] [PubMed] [Google Scholar]
- The effect of live-video demonstration on dental students' orthodontic bending performance. J Dent Educ. 2020;84:377-84.
- [CrossRef] [PubMed] [Google Scholar]
- A comparison of two forms of teaching instruction: Video vs. live lecture for education in clinical periodontology. Eur J Dent Educ. 2014;18:31-8.
- [CrossRef] [PubMed] [Google Scholar]
- Efficacy of invisalign attachments: A retrospective study. Am J Orthod Dentofacial Orthop. 2021;160:250-8.
- [CrossRef] [PubMed] [Google Scholar]




