

Translate this page into:
Accelerated and hybrid orthodontic treatment using a combination of 2D lingual appliance and in-house aligner: An anterior cross-bite and TMD case report after 1-year follow-up

*Corresponding author: Viet Hoang, Department of Orthodontics and Pedodontics, Faculty of Dentistry, Van Lang Univeristy, Ho Chi Minh, Vietnam. viet.h@vlu.edu.vn
-
Received: ,
Accepted: ,
How to cite this article: Hoang V, Dang TT, Nguyen MK, Tran PH. Accelerated and hybrid orthodontic treatment using a combination of 2D lingual appliance and in-house aligner: An anterior cross-bite and TMD case report after 1-year follow-up. APOS Trends Orthod. doi: 10.25259/APOS_22_2024
Abstract
Anterior cross-bite and Class I malocclusion are common in orthodontics. There are various methods to treat this condition. In this case report, we will be discussing our approach to treating anterior cross-bite in an adult patient. We used hybrid treatment by 2D lingual-fixed appliance and in-house clear aligner to provide esthetic orthodontic treatment. In addition, we utilized 3D simulation to ensure the accuracy of our treatment plan and mechanics. In this article field, we present the case of a 23-year-old woman who came to us with complaints of anterior cross-bite, smile esthetics, and her profile. On examination, we found that she had a skeletal Class I malocclusion and anterior cross-bite on the left side with erosion in her upper left incisors. Although she had good occlusion, there was some minor crowding in her upper and lower teeth. After conducting a 3D simulation, we decided to use a 2D lingual-fixed appliance on her upper teeth and an in-house aligner on her lower teeth. We chose this treatment plan because it was suitable, efficient, and cost-effective. However, after 2 months of treatment, the patient developed TMD, and her mandible shifted to the left. As a result, she had an X-bite on the right side. To address this issue, we removed the 2D appliance and switched to an in-house aligner for both upper and lower teeth. After 2 more months with the aligner, we noticed that the patient had occlusal interference in her left lateral incisor and erosion on this tooth. To fix this problem, we filled the tooth (22) and maintained the position of the lower teeth. We continued the finishing stage with the in-house aligner on both the upper and lower teeth. After 8 months of treatment, the case was successfully completed, and the patient no longer had TMD. Using a 2D lingual appliance and in-house aligner is an effective method for treating anterior cross-bites. Careful TMD control is essential in orthodontic treatments.
Keywords
Hybrid orthodontic treatment
2D lingual appliance
In-house aligner
Anterior cross-bite
Orthodontics

INTRODUCTION
Anterior cross-bite is defined as a malocclusion resulting from the lingual positioning of the maxillary anterior teeth in relationship to the mandibular anterior teeth.[1] Dental cross-bite involves localized tipping of a tooth or teeth and does not involve basal bone.[2] Patients with anterior dental cross-bite will show a normal anterior-posterior skeletal relationship with a smooth path of mandibular closure into an angle Class I relationship and coincident centric occlusion (CO) and centric relation (CR).[3] In this case study, we present a patient with an anterior cross-bite who underwent esthetic treatment. Lingual orthodontics is an effective form of orthodontic treatment that is both esthetically pleasing and inconspicuous. Modern dentistry has seen advancements in clear aligners, which have become a popular option for patients seeking a discreet solution to dental malocclusion. In some cases, a combination of lingual orthodontics and clear aligner treatment is used to achieve optimal results, saving time and avoiding unnecessary orthodontic movement [Graph 1]. This combination is referred to as hybrid orthodontic treatment, wherein the fixed component is a planned part of comprehensive, clear aligner treatment that performs skeletal or dental movements that the aligners alone could not predictably achieve.[4]
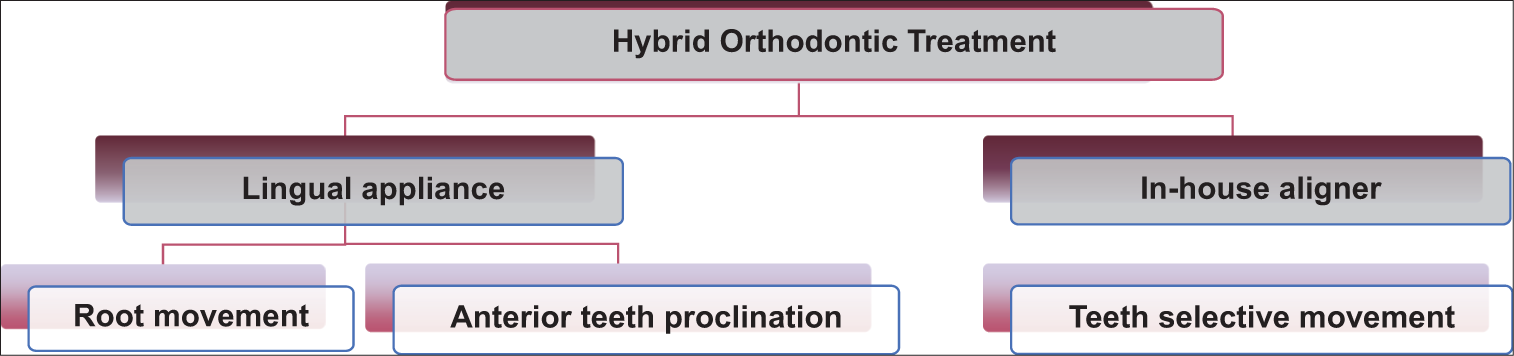
- Hybrid orthodontic treatment plan and advantages.
CASE REPORT
Diagnosis and etiology
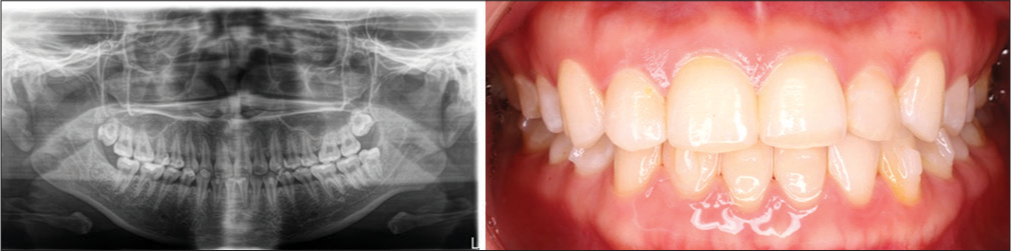
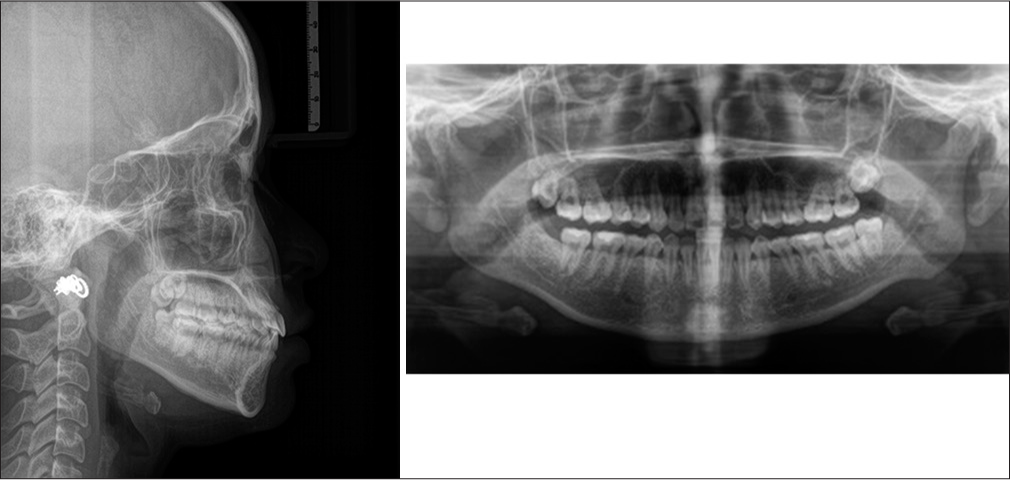
This case study presents the treatment of a 24-year-old patient with anterior cross-bite and lower crowding through esthetic orthodontic procedures. The treatment involved the use of a 2D lingual appliance[5] and an in-house aligner. The patient had skeletal Class I (ANB 2.2°), concave profile with a functional shift in anterior-posterior dimension and CO-CR discrepancy, and normal buccal corridor[6] with 80% teeth exposure, resulting in an unesthetic smile due to cross-bite. In addition, the chin had shifted to the left; there was a Class III molar and Class I canine relationship, and cross-bite from 21 to 22 with an edge-to-edge bite on 23. The patient also had moderate crowding on the upper and lower arch, and the lower midline had shifted to the left by 1mm, along with impacted upper wisdom teeth. However, the condylar position was normal before the treatment [Figures 1 and 2, Table 1].

- Pre-treatment intra and extraoral pictures.

- Pre-treatment X-rays.
| Measurement | Norm | Pre-treatment | |
|---|---|---|---|
| SNA (°) | 81.1±3.7 | 86.4 | Skeletal |
| SNB (°) | 79.2±3.8 | 84.2 | |
| ANB (°) | 2.5±1.8 | 2.2 | |
| FMA (°) | 25.0±4.0 | 29 | |
| U1 – SN (°) | 105.3±6.6 | 104 | Dental |
| U1 - NA (mm) | 4.0±3.0 | 3 | |
| U1-NA (°) | 22.0±5.0 | 17.5 | |
| U1 - L1 (°) | 128.0±5.3 | 128 | |
| L1 – NB (mm) | 4.0±2.0 | 7.3 | |
| L1-NB (°) | 25.0±5.0 | 32 | |
| IMPA (°) | 90.0±3.5 | 92 | |
| UL – E line (mm) | 0±2 | -0.5 | Soft tissue |
| LL – E line (mm) | 0±2 | 2.3 | |
ANB: A point, nasion, B point, FMA: Frankfort mandibular plane angle, IMPA: Incisor mandibular plane angle, L1: Lower central incisor, LL: Lower lip, MP: Mandibular plane, NA: Nasion point A NB: Nasion point B, SNA: Sella nasion point A, SNB: Sella nasion point B, U1: Upper central incisor, UL: Upper lip, E-line: Ricketts
Treatment objectives
Eliminate the anterior cross-bite and teeth alignment
Achieving satisfactory smile esthetics and masticatory function
Stable occlusion and treatment outcome in the long term.
Treatment plan
First, we discussed mechanics and the treatment plan with the patient using 3D simulation [Figure 3]. Then, we used a 2D lingual appliance using a direct bonding technique on the upper teeth from 15 to 25 and a clear aligner in-house on the lower teeth. However, normally for lingual appliances, we can use the indirect bonding technique to achieve good brackets position and less time on the chair.[7] We performed interproximal reduction (IPR) on the lower teeth from 33 to 43 by reducing 3 mm. We raised the bite and used a bonding fixed retainer on the labial side from 15 to 17 and 25 to 27 to solve the anterior cross-bite. We also extracted 85. Before the treatment, there was a 3–3 Bolton discrepancy of 80.5%. Hence, IPR on the lower was suitable for the mechanics and ensured good occlusion after the treatment. We opted for a 2D lingual appliance on the upper and a clear aligner treatment on the lower as it provided the advantages of both techniques. We designed the treatment plan after reviewing the 3D simulation. We observed that the required mechanics were to procline the upper anterior teeth and retract the lower anterior teeth on the 1st day of the treatment. The techniques were suitable for both the upper and lower teeth. With clear aligners, we could choose the desired movement and retract the anterior teeth on the 1st day, which was difficult with braces [Figure 4].
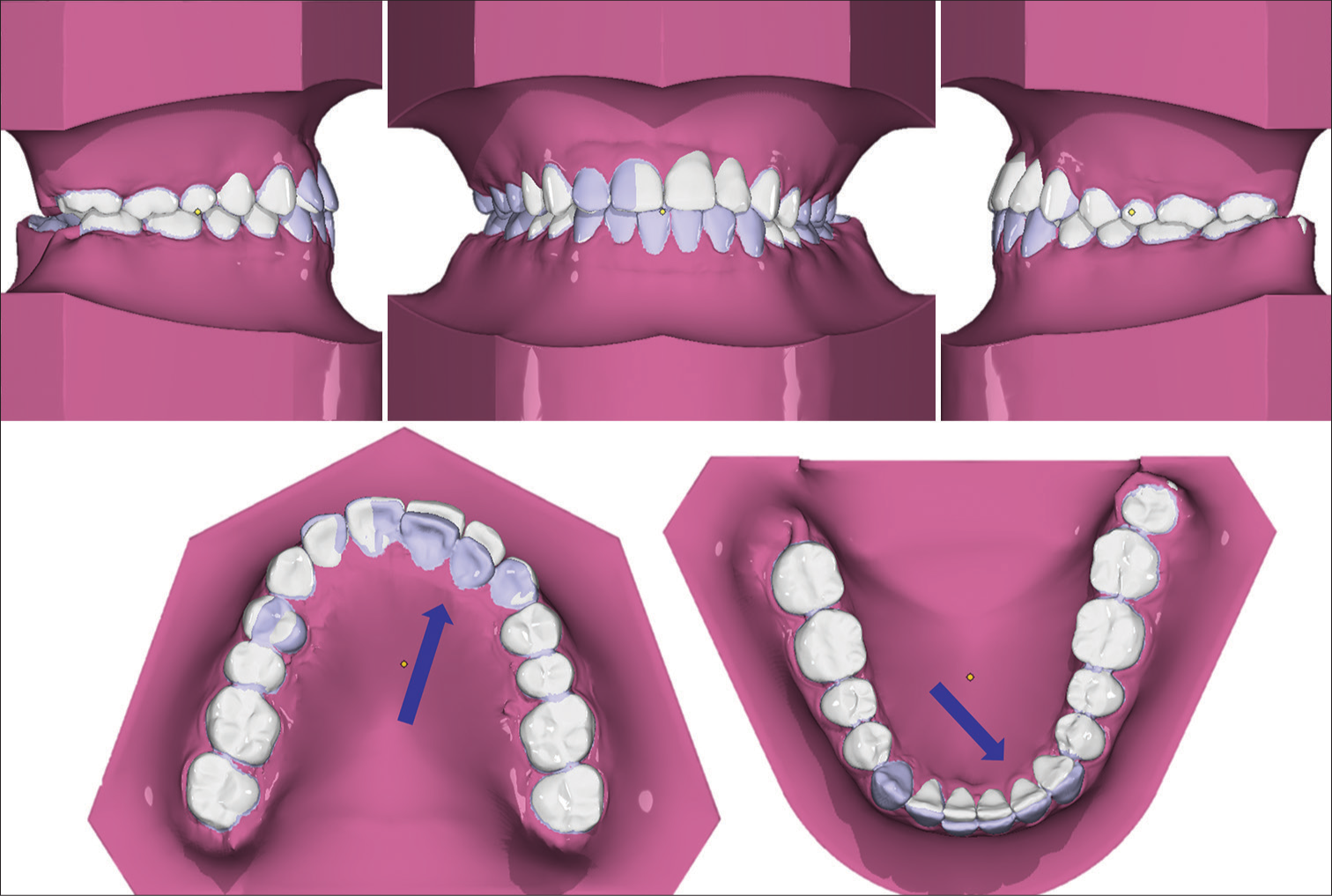
- 3D simulation of the treatment for checking mechanics before treatment. Blue arrow shows the simulated movement and position of the teeth before and after treatment.

- 2D braces, attachments bonding, and interproximal reduction at 1st day of treatment.
During the treatment, the patient developed temporomandibular disorder[8] (TMD), resulting in a leftward shift of the mandible. This prompted a series of treatment adjustments. We removed the 2D lingual appliance, paused the treatment for 2 weeks, and switched to in-house aligners for the upper and lower teeth to continue solving the anterior cross-bite and repositioning the mandible. After 5 months of the treatment, we filled in tooth 22. Before the treatment, due to the anterior cross-bite, there was an attrition on tooth 22. In this stage, we filled tooth 22 to solve the attrition and prevent the mandibular from shifting to the left. After the filling, tooth 22 could keep the mandible in a normal position. During the treatment, the jaw moved, causing two different bite positions for the patient. As a result, we needed to guide the jaw to the correct position. Initially, tooth 12 was attrition, and we planned to restore it after orthodontic treatment. However, we decided to restore tooth 12 before completing the jaw positioning to ensure that it remained in the proper place. After reshaping tooth 12, it became longer, allowing us to secure the jaw in the correct bite position. We finished the treatment with in-house aligners for the upper and lower teeth. While undergoing treatment, the patient experienced temporomandibular joint disorder (TMD) issues, and the posterior raising bite could potentially pose a problem in the future. As a result, we removed the raising bite and 2D lingual appliance. By that time, we had almost resolved the anterior cross-bite, so I transitioned to clear aligner treatment to complete the process. With clear aligners, we were able to finish the treatment without potentially exacerbating the patient’s TMD issue [Figures 5-7].
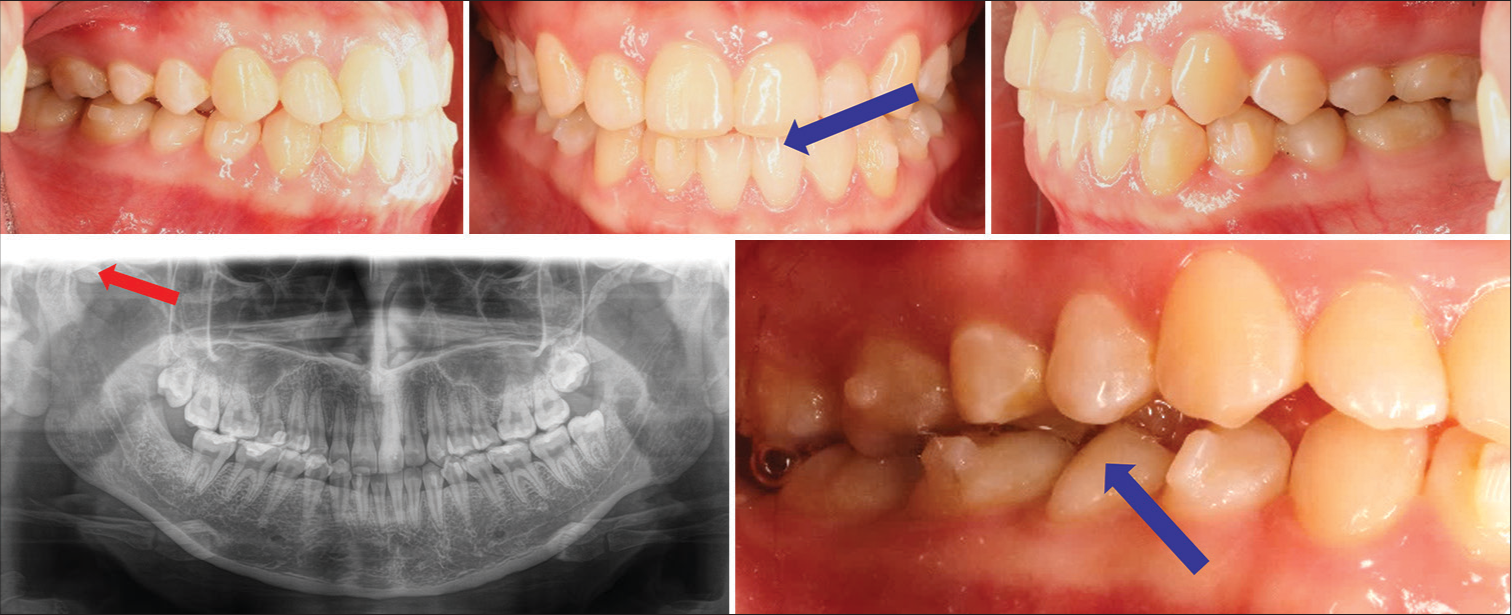
- After 2 months, the mandible shifted to the left, as the panoramic shows, because the patient got TMD during the treatment. The patient had a scissor bite on the right side. Blue arrows shows the mandible shifted to the left during the treatment. Red arrow shows the abnormal position of the condylar.
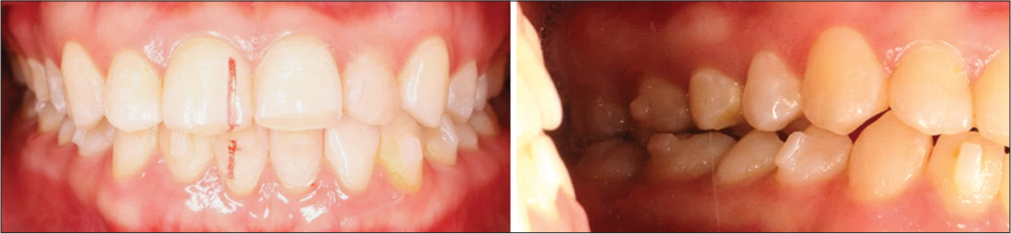
- After 5 months of treatment, we continued with in-house aligners and performed fillings on 22 teeth to prevent mandible movement to the left. Afterward, the occlusion came back to normal.
- After 7 months, everything was going well but there was a resorption of the right condyle.
Treatment results
After the treatment, we successfully achieved all the treatment objectives using esthetic orthodontic appliances. These appliances eliminated the cross-bite, aligned the teeth, improved the patient’s occlusion to Class I, enhanced facial esthetics, resolved the CO-CR discrepancy, and improved the patient’s smile in just 8 months. After the treatment, the lower midline no longer aligned with the upper midline, but this did not cause any issues. For tooth 22, a gingivectomy [9] is needed for a micro smile esthetic, but the patient declined. The superimposition showed that the results were consistent with our 3D simulation before treatment. An Essix retainer was used for the upper and lower teeth after treatment, and the results remained stable after a 1-year follow-up [Figures 8-11 and Table 2].

- Post-treatment intra and extraoral pictures after 8 months.
- Post-treatment X-rays.
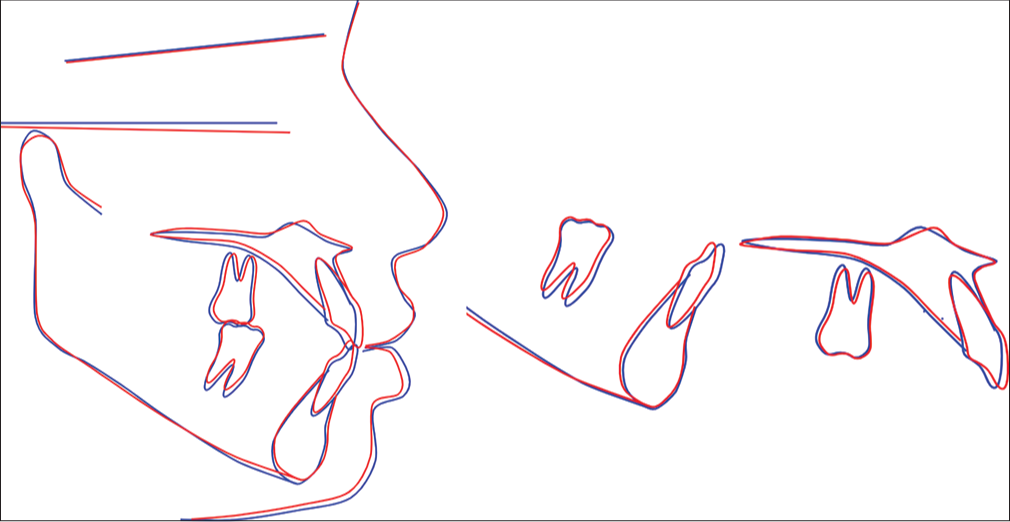
- Superimposition before and after treatment. Blue lines: Before treatment; Red lines: After treatment.

- 1-year follow-up treatment – The occlusion is stable.
| Measurement | Norm | Post- treatment | |
|---|---|---|---|
| SNA (°) | 81.1±3.7 | 85.6 | Skeletal |
| SNB (°) | 79.2±3.8 | 83.4 | |
| ANB (°) | 2.5±1.8 | 2.2 | |
| FMA (°) | 25.0±4.0 | 27 | |
| U1 – SN (°) | 105.3±6.6 | 108.3 | Dental |
| U1 - NA (mm) | 4.0±3.0 | 4.6 | |
| U1-NA (°) | 22.0±5.0 | 22.7 | |
| U1 - L1 (°) | 128.0±5.3 | 127.7 | |
| L1 – NB (mm) | 4.0±2.0 | 5.5 | |
| L1-NB (°) | 25.0±5.0 | 27.4 | |
| IMPA (°) | 90.0±3.5 | 88.8 | |
| UL – E line (mm) | 0±2 | -0.35 | Soft tissue |
| LL – E line (mm) | 0±2 | 2.2 | |
ANB: A point, nasion, B point, FMA: Frankfort mandibular plane angle, IMPA: Incisor mandibular plane angle, L1: Lower central incisor, LL: Lower lip, MP: Mandibular plane, NA: Nasion point A NB: Nasion point B, SNA: Sella nasion point A, SNB: Sella nasion point B, U1: Upper central incisor, UL: Upper lip, E-line: Ricketts
DISCUSSION
In this case, accelerated and hybrid orthodontic treatment using 2D braces on the upper teeth and clear aligners on the lower teeth was an ideal choice for the patient who desired an esthetically pleasing treatment. Hybrid orthodontic treatment provides the following benefits and advantages for patients:
Reduces the total treatment time over treatment with clear aligners alone
Reduces the time patients must spend wearing braces
Reduces cost of treatment in many cases
Clear, removable tooth aligners provide maximum comfort and convenience
Removable aligners allow for better dental hygiene than standard braces
Reduced emergency visits for problems with loose or broken brackets or poking wires
Aligner adjustments are completed through a simple 5-min 3D scan
We can control biomechanics and laboratory processes in-house with our own aligner laboratory. The process of in-house aligner production is illustrated in Figure 12.
Most treatment with clear aligners is completed in 3–4 months
Improved patient compliance.
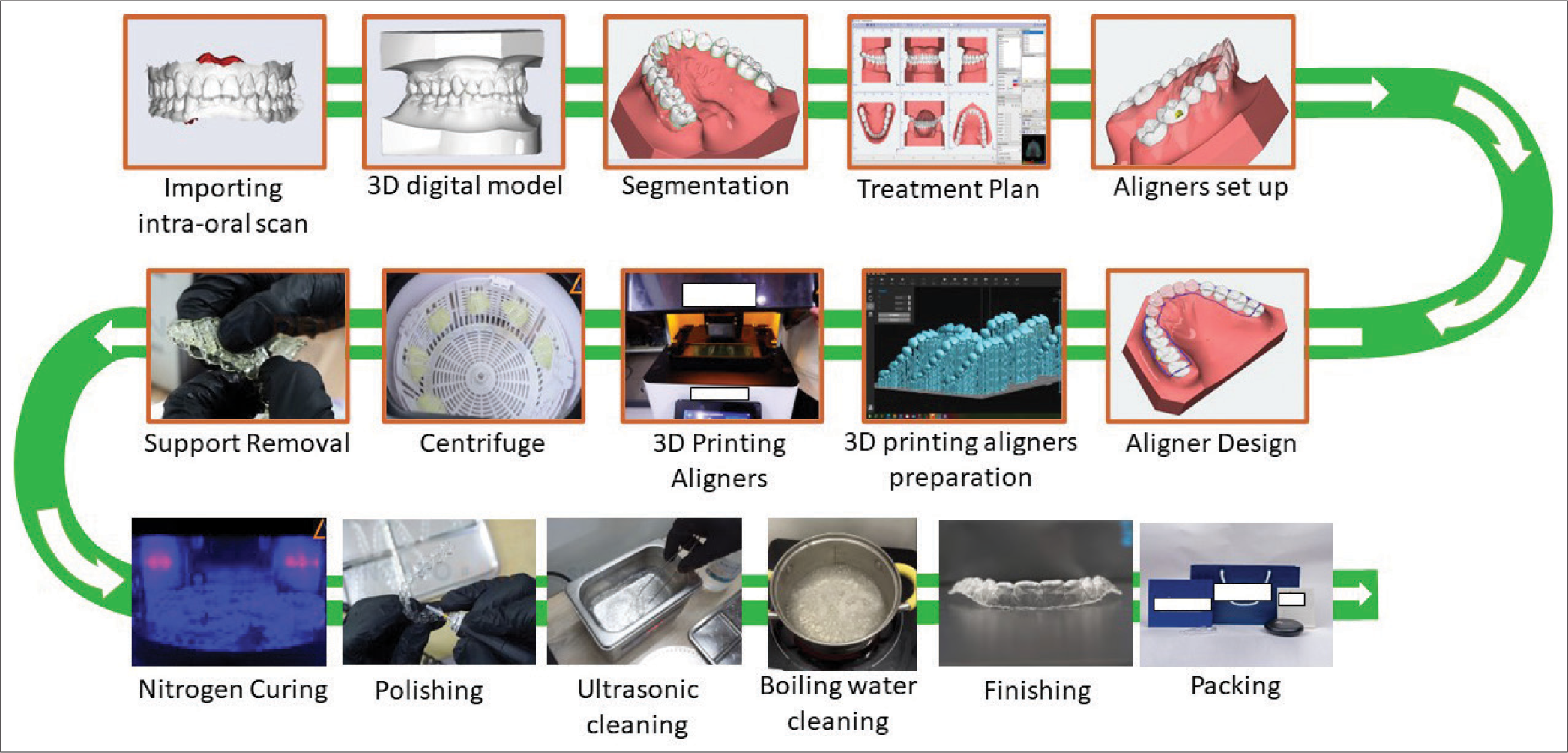
- Laboratory procedure for in-house aligner production.
Throughout the treatment process, we carefully monitored each appointment to ensure its success. However, we discovered that the patient had developed TMD during the treatment, causing the mandible to shift to the left. Fortunately, we were able to resolve this issue easily while continuing with the treatment. Clear aligners in-house with hybrid orthodontic treatment can be very effective, and hopefully, in the future, the clear aligner can be biodegradable.[10]
CONCLUSION
For adult cases with high esthetic concerns, a combination of 2D lingual appliance and clear aligner (Hybrid treatment) can be an effective solution. Clinicians can use 3D simulation to plan the treatment and predict the movement of teeth. It is important to note that problems may arise during any stage of orthodontic treatment.
Ethical approval
The Institutional Review Board has waived the ethical approval for this study.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- Components of anterior crossbite in the primary dentition. ASDC J Dent Child. 2001;68:27-32.
- [Google Scholar]
- Fundamentals of pediatric dentistry (3rd ed). London: Quintessence Publishing Co; 1995. p. :355.
- [Google Scholar]
- Anterior crossbite correction in uncooperative or disabled children. Case reports. Aust Dent J. 1996;41:304-9.
- [CrossRef] [PubMed] [Google Scholar]
- The hybrid approach: A solution to overcome unpredictable movements in clear aligner therapy. APOS Trends Orthod. 2020;10:72-7.
- [CrossRef] [Google Scholar]
- The 2D lingual appliance system. J Orthod. 2013;40(Suppl 1):S60-7.
- [CrossRef] [PubMed] [Google Scholar]
- Buccal corridor and gummy smile treatment with MARPE and gingivoplasty: A 2-year follow-up case report. APOS Trends Orthod 2023
- [CrossRef] [Google Scholar]
- Management of moderate crowding by two-arch distalization using passive self-ligating lingual brackets, in-house digital indirect bonding, and mini-screw anchorage: A case report. APOS Trends Orthod. 2023;13:184-92.
- [CrossRef] [Google Scholar]
- Epidemiology, diagnosis, and treatment of temporomandibular disorders. Dent Clin North Am. 2013;57:465-79.
- [CrossRef] [PubMed] [Google Scholar]
- Digitally planned surgical crown lengthening: A novel bone reduction strategy to correct a gummy smile. J Surg Case Rep. 2024;2024:rjae202.
- [CrossRef] [PubMed] [Google Scholar]




