

Translate this page into:
Accelerated orthodontics: Getting ahead of ourselves?

*Corresponding author: Padhraig S. Fleming, Department of Orthodontics, Institute of Dentistry, Queen Mary University of London, London, United Kingdom. padhraig.fleming@qmul.ac.uk
-
Received: ,
Accepted: ,
How to cite this article: Fleming PS. Accelerated orthodontics: Getting ahead of ourselves? APOS Trends Orthod 2020;10(3):142-9.
Abstract
There is disagreement as to what constitutes an acceptable duration for orthodontic treatment but seeming unanimity that acceleration is required. This contention has spawned a range of surgical and non-surgical adjuncts designed to accelerate orthodontic tooth movement, geared at reducing overall treatment times while maintaining optimal occlusal results. Largely, however, marketed non-surgical adjuncts and involved surgical procedures have shown equivocal effectiveness in reducing treatment times. Notwithstanding this, a range of key treatment decisions and approaches may have a more potent effect. While external solutions may offer alluring possibilities, perhaps, more mundane realities including refinement of orthodontic planning and decision-making with efficiency and process, as well as final outcome, in mind continue to offer the most accessible and influential means of improving orthodontic efficiency?
Keywords
Orthodontic
Treatment
Efficiency

INTRODUCTION
Comprehensive orthodontic treatment is lengthy with the time frame largely dictated by biologic processes as well as mechanical principles and treatment approaches.[1] On the basis of a large systematic review, it appears reasonable to suggest that the mean duration of treatment may be of the order of 20 months.[2] This estimate was based on data from 22 prospective studies. There is, however, an appreciation that duration may be extended in more challenging malocclusions.[3]
There is relatively little agreement as to what constitutes an acceptable treatment duration with age, malocclusion, and treatment-related factors influencing this. Moreover, it is largely accepted that the quality of treatment outcome takes precedence over both the length of treatment and appliance esthetics.[4] Notwithstanding this, there has been an increasing drive to reduce the duration of orthodontic treatment in recent years with a seeming acceptance that treatment duration is excessive both among adults and adolescents. This assumption has spawned a range of surgical and non-surgical adjuncts designed to accelerate orthodontic tooth movement, ultimately directed at reducing overall treatment times while maintaining optimal occlusal results.
Modern adjuncts developed to hasten treatment include newer technologies and novel surgical procedures, while the notion of eschewing integral treatment phases and objectives has also gained localized traction to prioritize shorter treatment times.[5] However, a plethora of non- marketed techniques and approaches can be used in selected cases to limit excessive treatment duration. While clinicians may be infatuated by light, surgery, vibrations, and other attractions, perhaps, bone turnover and related tooth movement may be more responsive to more banal influencers including fundamental treatment planning decisions and related basic decision-making?
RATIONALE FOR SHORTER TREATMENT DURATION
Extended treatment may increase the susceptibility to iatrogenic damage including root resorption and plaque- induced conditions, chiefly demineralization, and periodontal problems.[6] However, it is reasonable to suggest that the associated risks are only likely to increase markedly with treatments in excess of 2 years or more. An association has also been found between duration in rectangular arch wires,[7] the use of interarch elastics,[7,8] and the severity of root resorption. There may be monetary benefit in delivering more efficient treatment for treatment providers linked both with fewer visits and reduced chairside times. However, this may be offset by the need for additional procedures (surgical or non-surgical) or adjuncts that might promote efficiency.
It is accepted that compliance may diminish over longer treatment increasing the risk of both iatrogenic effects and suboptimal outcomes. Classically, there is, for example, evidence that more prolonged, two-phased courses of Class II correction are no more effective than more efficient single-phase approaches.[9,10] It is also accepted that compliance during treatment is often suboptimal both in terms of wear of removable appliances and adjuncts with adherence waning over time, exemplified by declining wear rates of removable retainers.[11,12] Nevertheless, it remains unclear whether a threshold treatment duration exists among varying population groups beyond which negative patterns of behavior become more prevalent and problematic.
A further important consideration is the impact of treatment from a sociopsychological perspective. Oral health-related quality of life may be impaired by longer treatment, particularly in adults.[13] The latter stems from the social impact of appliance therapy allied to pain and discomfort, which tends to be more marked among adult patient groups.[14] Consequently, efforts to reduce treatment duration may be more apposite to adult groups, in particular. It is, however, incumbent on researchers to ensure that the impact of appliance therapy, including patient experiences as well as objective measures of treatment outcome, is considered to evaluate the impact of variation in treatment duration holistically.[15] The latter should be balanced against the need to optimize and measure occlusal and facial outcomes as part of orthodontic treatment. Clearly, obtaining optimal outcomes is an imperative; however, further information on the relative importance of optimal technical intra- and inter-arch relationships allied to the impact of treatment duration and appliance esthetics are warranted, particularly given the capacity to adapt to and function with occlusal imperfection.[16] Notwithstanding this, the trend seems to have trumped the argument and the consensus appears to be that treatment is overly lengthy stimulating the feverish development of techniques and adjuncts directed at reducing treatment duration.
FIXED APPLIANCE ATTACHMENTS
Technological advances have led to the advent of customization of both bracket slot and base. The latter, in particular, has raised the possibility of more precise finishing potentially reducing the time required to detail the occlusion. Workflows are revised accordingly with chairside time potentially reducing although non-clinical time may increase. However, clinical research has failed to demonstrate significant benefit with no difference observed either in terms of treatment duration or quality of outcome [Figure 1].[17] Similarly, the reemergence of self-ligation was greeted with claims of reduced treatment duration associated with decreased resistance to sliding; however, this was not substantiated in prospective research.[18,19]

- A very mild Class II div 2 malocclusion (a-c) with mild to moderate crowding of both arches (a). Treatment involved use of a customised upper lingual appliance. The maxillary arch was over-expanded resulting in buccal displacement and flaring of 13 (b). Local wire-bending and detailing were required to address this complication leading to excessive treatment duration (23 months).
NON-SURGICAL AND SURGICAL ADJUNCTIVE PROCEDURES
A range of experimental approaches to accelerate tooth movement has been developed;[20] however, the majority of these have not yet been translated into the clinic. Of the non-surgical adjuncts, resonance vibration and low- level laser therapy have undergone the greatest degree of refinement and investigation. Encouraging results have been demonstrated in vitro with resonance vibration, in particular. Based on a rodent model, for example, application of a 60 Hz resonance vibration to the first molars on a weekly basis was associated with 15% increase in the rate of tooth movement.[21] The potential of marketed devices has, however, largely not been replicated in vivo with no evidence of changes in salivary biomarkers of bone turnover[22] and a failure to show reduced treatment time on the basis of clinical trials involving fixed appliance- based treatment in extraction cases.[23,24] Low-level laser therapy or photobiomodulation has also shown some promise in vitro with effects in relation to osteoblast numbers, osteoclastogenesis, and extracellular matrix differentiation. At this stage, however, robust prospective evidence of accelerated orthodontic tooth movement with photobiomodulation continues to be lacking with only preliminary data present at this stage.[25]
A plethora of surgical interventions and protocols has been developed to accelerate tooth movement. These range in invasiveness from transmucosal procedures to more involved surgery including osteotomy. Inconsistent findings concerning the potential value of these procedures have again been illustrated.[26] Furthermore, there is a suggestion that increased efficacy may necessitate a higher burden of intervention and may require precisely timed interventions, or either more frequent or more invasive procedures to potentiate sustained regional accelerated phenomena. The latter may be associated with increased risk with patients and parents reticent to undergo additional procedures within a predominantly non-surgical specialty such as orthodontics.[27]
“SHORT-TERM ORTHODONTICS”
Orthodontic treatment has become more accessible both to patients and practitioners in recent years. Adult orthodontics, in particular, has become increasingly ingrained with biologic processes underpinning tooth movement slower in adults. Moreover, the social impact of appliances on adults can be significant.[28] This has spawned the concept of “short-term” or “limited objective” orthodontics, either as an isolated intervention or to facilitate minimally invasive cosmetic dentistry. These systems have been marketed heavily both to patients, students, and general dentists.[29] Typically, short-term orthodontics involves an abbreviated course of orthodontics focusing on the alignment of the anterior teeth, with a trade-off between shorter treatment and less complete occlusal correction [Figure 2]. Conversely, comprehensive orthodontics is directed at obtaining holistic occlusal and esthetic correction while maximizing the prospect of long-term stability. While a perfect occlusal outcome is often elusive,[30] it is contingent on adequate expression of tip and torque, combined with careful treatment planning and mechanics. Achieving these objectives may be necessarily slow, with complete torque expression, particularly time consuming. However, with short-term orthodontic approaches, a compromised result is often premeditated and patients should be aware of the objectives and limitations of treatment before commencing. Moreover, it is clear that this approach does not represent a “fair comparison” with alternatives, as the planned outcome is likely to diverge from that associated with comprehensive correction.
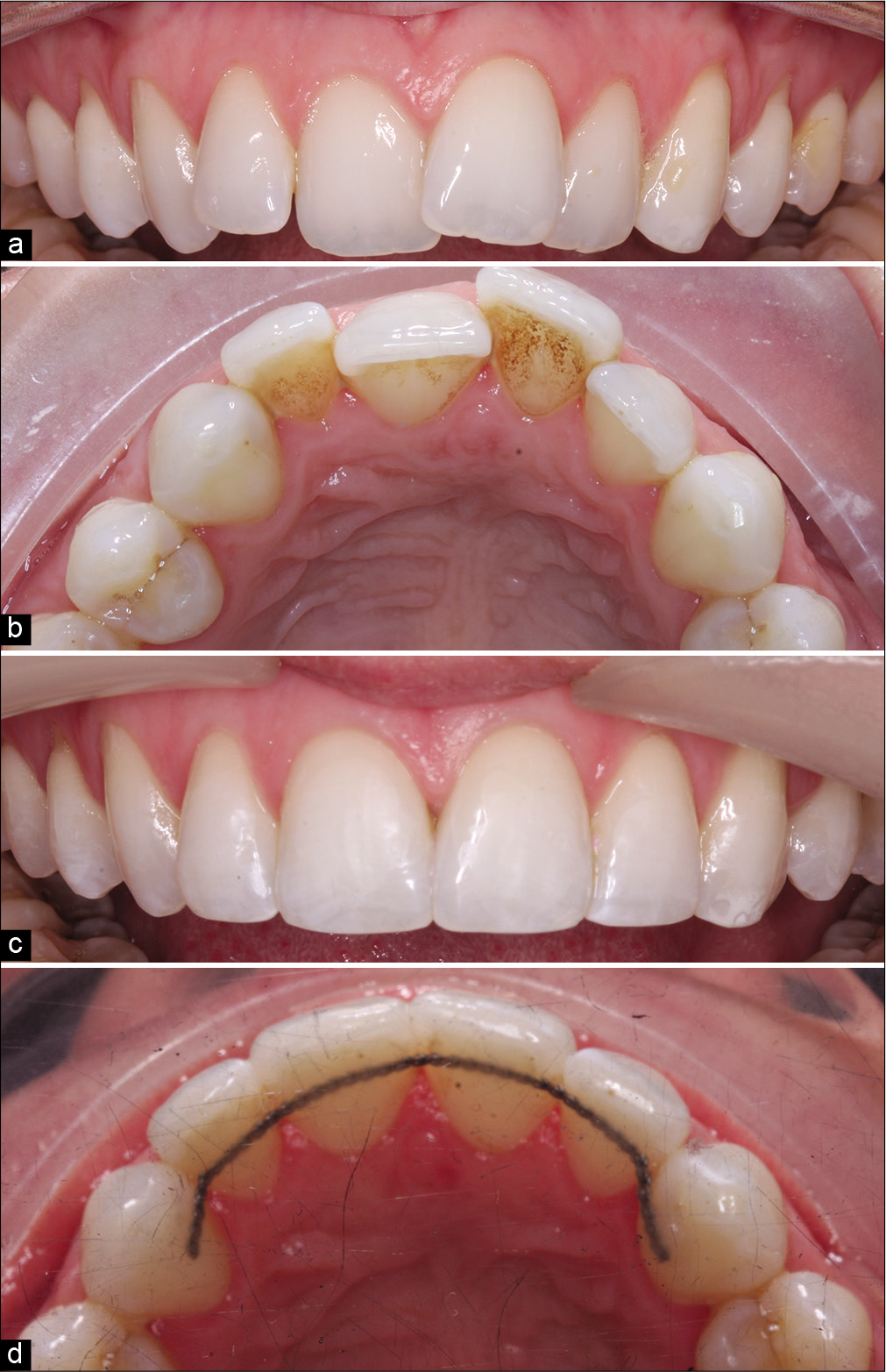
- Malaligned upper anterior teeth (a, b) treated with a very brief phase of fixed appliance-based orthodontics (c, d). Treatment was undertaken over a period of just 33 days with appliances removed prematurely. While acceptable alignment of the incisors has been achieved, torque correction on 13 would necessitate more comprehensive treatment with full three-dimensional control.
As such, there is little proof that either surgical or non- surgical adjuncts are universally helpful, although there may be speculative indications on an individual basis. Consequently, if these procedures are to be planned, a blanket approach does not appear to be indicated with any supernumerary interventions best targeted based on occlusal dictates and timed most appropriately to reduce the surgical insult and additional burden of care.
OPTIMIZING EFFICIENCY: TREATMENT PLANNING AND MECHANICS
A plethora of studies has been undertaken in recent years in relation to the efficiency of treatment predominantly centering on the use of adjuncts to accelerate tooth movement.[15]
It is telling, however, that stark differences exist in relation to the mean duration of treatment identified between many of these studies indicating that the chief arbiter of treatment duration may not reside in exploitation of regional accelerated phenomena using proprietary adjuncts but may instead be governed by clinical skills and decision-making. As such, it seems pertinent that our attention should be focused on maximizing efficiency and optimizing treated results by exhausting inherent opportunities before graduating to costly, burdensome, and potentially risky supplementary measures.
EXTRACTION DECISIONS
There is an acceptance that the orthodontic extraction pendulum has hovered in a non-extraction direction for some time with evidence that 95% of orthodontists are extracting less than 5–10 years previously in the U.K.[31] Many of the more challenging malocclusions may necessitate orthodontic extractions to produce holistic correction of presenting features. Clearly, the outcome of treatment in terms of esthetics, function, optimal periodontal health, and stability may all be affected by extraction decisions. Admittedly, eschewal of extractions may obviate the need for orthodontic space closure and simplify overbite reduction in certain cases; however, space requirements typically override any potential increase in treatment duration associated with extractions. Notwithstanding this, it appears that the decline in extraction tendency may not be predicated on mechanical advancements or an evolving approach to retention.[31]
The merits and demerits of extraction-based therapy have been contested for many years and a discussion of these is beyond the scope of this paper. However, from a personal perspective, I am extracting slightly less than I did 10 years ago too; however, a more significant alteration has been a tendency to remove second premolars as opposed to first premolars, particularly in the mandibular arch. There is relatively little evidence to underpin differences in this respect; however, closure of lower first premolar extraction space is often more time consuming. Removal of lower first premolars can introduce Class II problems that might not have existed previously and/or compound Class II correction due to the relative tendency for the upper posterior teeth to migrate mesially during space closure, while the lower posterior teeth appear to offer more posterior anchorage. This tendency for maxillary arch space to close more readily from behind means that posterior anchorage may need to be bolstered from the outset leading to more intervention, time, and appointments. Alternatively, individual tooth retraction (often of the maxillary canine) or the introduction of Class II elastics may be necessary during space closure to manage anchorage requirements. These eventualities risk the introduction of Class II relationships and the potential for more prolonged treatment to mitigate this.
Mechanical eruption and alignment of ectopic canines are known to be complex and often lengthy with failure rates of up to 30% ascribed to alignment of ectopic canines above 30 years of age.[32] The treatment duration is influenced by a host of factors chiefly the position of the canine (buccal vs. palatal), degree of ectopia, and age. Given the advent of three- dimensional imaging, there is now a more accurate means of localizing ectopic canines and predicting the complexity and indeed the length of treatment required to align these teeth. In certain instances in quadrants requiring significant space, it may be sensible to use this three-dimensional appreciation to consider loss of the canine rather than trying to align the tooth potentially averting lengthy and unsuccessful treatment in selected cases.
EXTRACTION TIMING
A key consideration during extraction-based treatment is the rate at which sites remodel and mature. It has been estimated that extraction sites are likely to have matured within 100 days of extractions.[33] If we consider that a premolar is approx. 7 mm wide and spaces close at up to 1 mm/month, it is unsurprising that the final millimeter of space closure can be challenging. There is some clinical evidence that fresh extraction sites may be advantageous utilizing a planned regional accelerated phenomenon to move teeth efficiently soon after extractions.[34] This approach can be particularly effective where reciprocal space closure is permissible avoiding extraction site maturation [Figure 3]. While space closure can be initiated early in treatment, with continuous archwires, this may necessitate space closure on light, flexible wires predisposing to unwanted tipping in the first instance followed by a period of root uprighting. Notwithstanding this, this approach may be useful in adult patients, in particular. Moreover, the use of segmental approaches can be considered or indeed extractions deferred until space closure is to be initiated in less crowded arches to facilitate for space closure on more rigid wires.
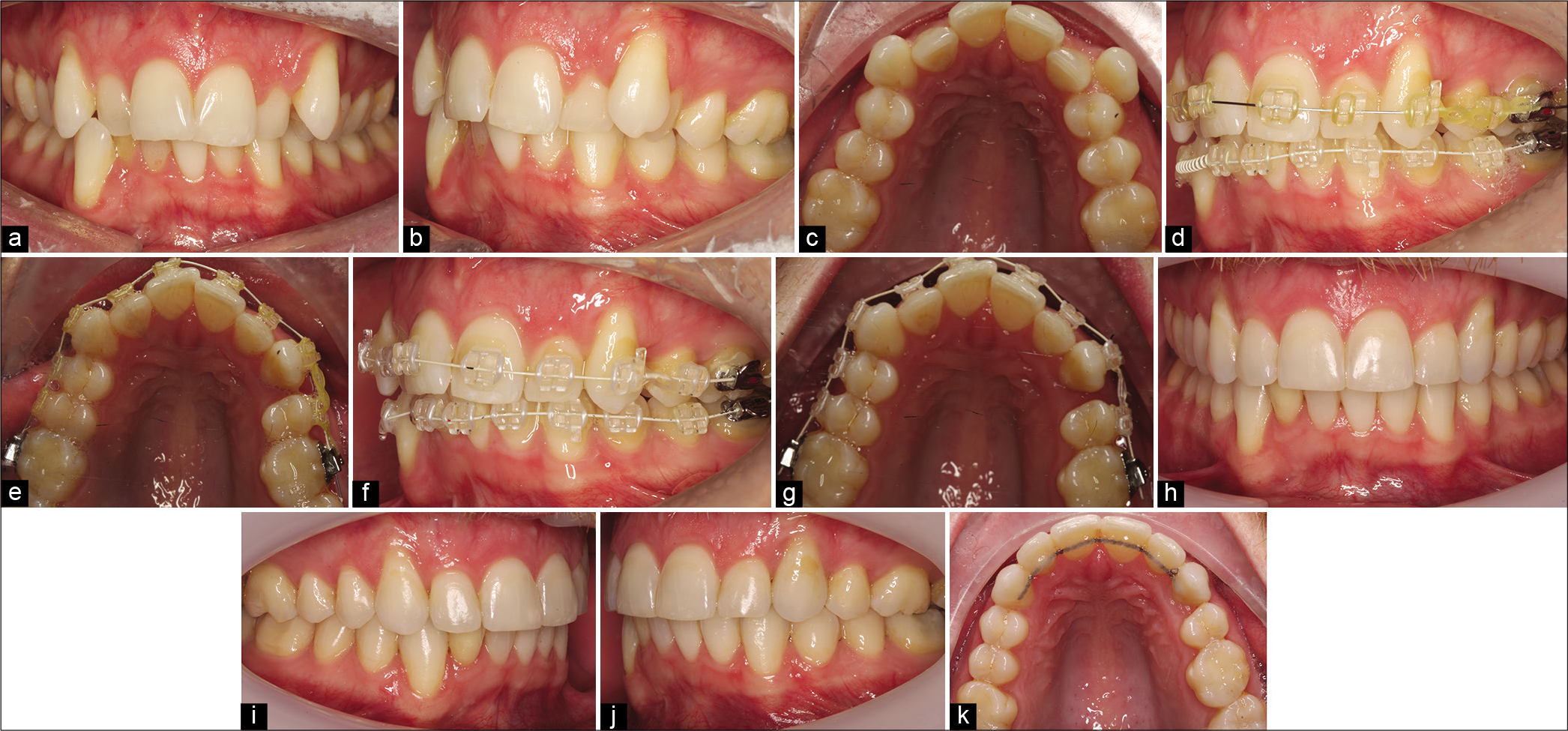
- A Class I malocclusion with dual-arch crowding, asymmetric molar relationships, and thin gingival biotype (a-c). Treatment involved upper and lower fixed appliances with loss of 24 in isolation to facilitate relief of crowding, alignment, and improvement of the midline shift. Immediately following extractions, light elastomeric chain was used locally to align 23 and to facilitate early space closure in this adult patient. At 6-week review (d and e), dramatic space closure had already been achieved with a significant excess of wire distal to 26. Very light elastomeric chain was subsequently reapplied (f and g) to finalize space closure with treatment completed in a period of 11 months (h-k).
It is important to highlight, however, that more efficient initial alignment and/or space closure does not necessarily translate into a shorter overall course of treatment. However, any time savings may be harnessed to dedicate additional time to achieving complex, time-consuming change including localized torque correction.
OVERLAPPING TREATMENT PHASES
Conventionally, the division of treatment into distinct phases has been advocated.[35] These include initial alignment and leveling, overbite reduction, overjet reduction, space closure, and finishing and detailing of the occlusion. While this approach forms a very sensible basis for treatment and underpins much of our teaching, the distinction between some of these phases is becoming increasingly blurred as materials and mechanics evolve and can be exploited to reduce treatment duration. Mechanics including the use of fixed Class II correctors and fixed anterior bite planes are becoming more accepted mechanisms of streamlining treatment without resorting to compromised objectives, although evidence of reduced treatment duration associated with these techniques per se remains limited.
Clearly, the mechanism of overbite reduction is influenced by the etiology of the vertical issue; however, the use of fixed anterior bite planes involving anterior disclusion to promote a combination of anterior intrusion and posterior extrusion can be particularly potent. This approach may facilitate concomitant alignment of the arches in tandem with overbite reduction. Alternatives might include use of an upper removable appliance as a prelude to fixed appliances, staged placement of fixed appliances, or indeed use of posterior disclusion. The latter may provide adequate space to place the lower appliance without introducing occlusal contact on the lower anteriors but risks posterior intrusion exacerbating overbite reduction and indeed local posterior open bites.
The approach to management of the transverse dimension may be influenced by a range of dictates chiefly the etiology in terms of skeletal and dentoalveolar contributions. However, for those cases requiring dentoalveolar change, in isolation, transverse change can be affected during the fixed multibracket phase without recourse to adjuncts, for example, quadhelices or active palatal arches. The use of a quadhelix is not known to produce meaningful skeletal changes; moreover, transverse correction can be time consuming and is normally undertaken before placement of multibracket appliances. Furthermore, overexpansion is often planned without solid evidence that this leads to more stable overall change. Equally, excessive expansion can lead to unwanted bite opening effects. Consequently, more controlled use of expanded archwires or indeed harnessing of preexisting displacements and crowding can be used as alternatives [Figure 4].[36]
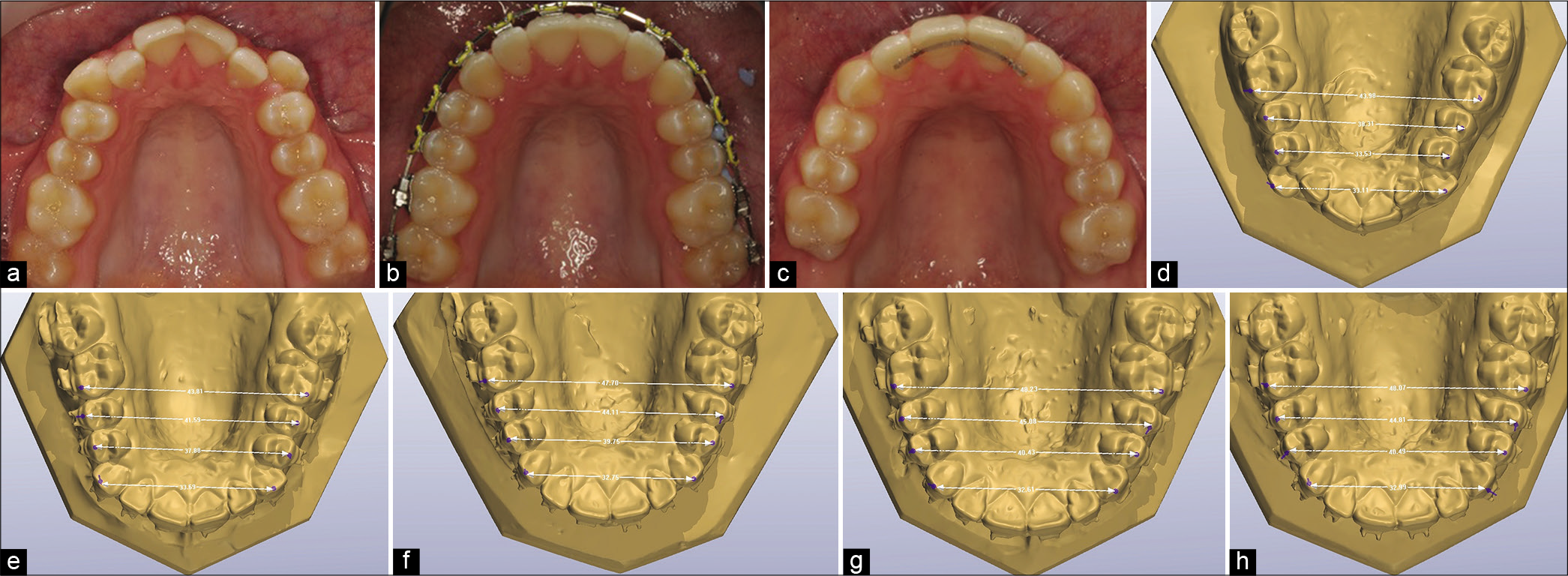
- A mild Class III malocclusion with buccally displaced canine and narrow inter-premolar dimension (a). Following engagement of the archwires in the buccally displaced canines, significant dental expansion was achieved without recourse to adjuncts (b and c). The initial buccolingual position of the canines (d) contributed to the final arch form due to its anchorage value. Following engagement of a 0.014 inch Ni–Ti 4 mm of inter-premolar expansion arose (e). This increased to 6–7 mm in 14 × 25 inch (f) and 18 × 25 inch (g) Ni–Ti with intermolar expansion developing in more rigid rectangular Ni–Ti wires. Changes were largely consolidated in 19 × 25 inch stainless steel (h).
ANCHORAGE SUPPLEMENTATION AND MANAGEMENT
Anteroposterior anchorage supplementation is planned and effected for a specific indication, namely, to manage space requirements and idealize the position of the teeth relative to the dental bases and facial structures. Clearly, these objectives may override the possible effect of the approach to anchorage supplementation on treatment duration; however, it is conceivable that the choice of approach and treatment protocols may have a bearing on the length of treatment.
Individual or en masse retraction?
Individual retraction of teeth is advocated to conserve anchorage by controlling the number of teeth in active relative to reactive units. This may be of some merit when dealing with teeth with large anchorage value (e.g., maxillary canines), particularly when used in conjunction with a supplementary approach to anchorage control. In a Class II case, for example, perhaps by retracting the canine to Class I, a “canine interlock” can be obtained, thereby reducing any residual overjet and closing space mesial to the maxillary canine with little or no further loss of anchorage. However, it is worthy of mention that each tooth retracted individually results in space closure but also space opening. The treatment time may well increase accordingly. Where numerous teeth are retracted individually (effectively “multi-step” retraction), this should make us question whether we might instead need to support our anchorage more positively (e.g., with TADs) so that more proactive approaches to space closure or redistribution can be planned reducing treatment time accordingly. Furthermore, clinical research has alluded to little additional benefit associated with two-step approaches in terms of anchorage conservation with a significant increase in treatment time also reported.[37-39]
Intra-arch auxiliaries or use of mini-implants
A well-designed clinical trial involving comparison of mini- implants, headgears, and Nance palatal arches failed to identify a difference related to treatment duration.[40] It is noteworthy that this study involved canine retraction in all three groups rather than en masse retraction. Mini-implants may be more amenable to en masse retraction in view of their higher inherent anchorage capacity. As such, further research may be helpful in clarifying this consideration further.
Functional appliance therapy
Efforts to accelerate active orthodontic treatment should clearly be balanced against both the outcome and the prospective stability of the outcome. Both fixed functional appliances and removable functional appliances worn on a full-time basis may reasonably be expected to produce molar and incisal over a 6-month period; however, relapse following withdrawal of the appliance is common.[41,42] Based on the study of rodents, bone formation at the condyle is incomplete 5–7 months into treatment with unstable Type III collagen present. Type III collagen tends to produce emergency-type bone, which is more susceptible to reversal during function and mastication. The authors advocated doubling the treatment time to allow for the establishment of replacement bone at the condyle.[43] While it is difficult to extrapolate these findings to the clinical situation, it is reasonable to suggest that Class II correction with functional appliance therapy should not be rushed to avoid occlusal relapse and the possible need for the reintroduction of means of Class II correction during the multibracket fixed appliance phase. This may be increasingly important when occlusal interdigitation is decreased during functional appliance therapy.[44]
CONCLUSION
There is an inexorable drive toward reducing orthodontic treatment times. This is understandable and may refine treatment experiences and limit iatrogenic effects. Notwithstanding this, the adoption of marketed surgical and non-surgical adjuncts does not appear to have been pivotal in reducing treatment duration. Moreover, the influence of more fundamental decision-making, including extraction decisions, planning of anchorage, and mechanics, allied to precision in terms of bonding and finishing may well dwarf the effects of optional extras in producing predictable efficiency in orthodontics.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Clinical and histologic observations on tooth movement during and after orthodontic treatment. Am J Orthod. 1967;53:721-45.
- [CrossRef] [Google Scholar]
- How long does treatment with fixed orthodontic appliances last? A systematic review. Am J Orthod Dentofacial Orthop. 2016;149:308-18.
- [CrossRef] [PubMed] [Google Scholar]
- Influence of radiographic position of ectopic canines on the duration of orthodontic treatment. Angle Orthod. 2009;79:442-6.
- [CrossRef] [PubMed] [Google Scholar]
- Esthetic perception of clear aligner therapy attachments using eye-tracking technology. Am J Orthod Dentofacial Orthop 2020:S0889-5406. (20)30291-2
- [CrossRef] [PubMed] [Google Scholar]
- Short-term cosmetic orthodontics for general dental practitioners. Br Dent J. 2013;214:83-4.
- [CrossRef] [PubMed] [Google Scholar]
- Meta-analysis of the treatment-related factors of external apical root resorption. Orthod Craniofac Res. 2004;7:71-8.
- [CrossRef] [PubMed] [Google Scholar]
- Patient characteristics and treatment variables associated with apical root resorption during orthodontic treatment. Am J Orthod Dentofacial Orthop. 1991;99:35-43.
- [CrossRef] [Google Scholar]
- Risk factors for apical root resorption of maxillary anterior teeth in adult orthodontic patients. Am J Orthod Dentofacial Orthop. 1995;108:48-55.
- [CrossRef] [Google Scholar]
- Early treatment for Class II Division 1 malocclusion with the Twin-block appliance: A multi-center, randomized, controlled trial. Am J Orthod Dentofacial Orthop. 2009;135:573-9.
- [CrossRef] [PubMed] [Google Scholar]
- Outcomes in a 2-phase randomized clinical trial of early Class II treatment. Am J Orthod Dentofacial Orthop. 2004;125:657-67.
- [CrossRef] [PubMed] [Google Scholar]
- Compliance with removable orthodontic appliances and adjuncts: A systematic review and meta-analysis. Am J Orthod Dentofacial Orthop. 2017;152:17-32.
- [CrossRef] [PubMed] [Google Scholar]
- Effects of fixed vs removable orthodontic retainers on stability and periodontal health: 4-year follow-up of a randomized controlled trial. Am J Orthod Dentofacial Orthop. 2018;154:167-74.
- [CrossRef] [PubMed] [Google Scholar]
- The impact of orthodontic treatment on quality of life and self-esteem in adult patients. Eur J Orthod. 2015;37:233-7.
- [CrossRef] [PubMed] [Google Scholar]
- Pain experience in adults undergoing treatment: A longitudinal evaluation. Angle Orthod. 2018;88:292-8.
- [CrossRef] [PubMed] [Google Scholar]
- Orthodontic trial outcomes: Plentiful, inconsistent, and in need of uniformity? A scoping review. Am J Orthod Dentofacial Orthop. 2018;153:797-807.
- [CrossRef] [PubMed] [Google Scholar]
- Occlusion for the Class II jaw relations patient. J Prosthet Dent. 1990;64:432-4.
- [CrossRef] [Google Scholar]
- Orthodontics with customized versus noncustomized appliances: A randomized controlled clinical trial. J Dent Res. 2017;96:1498-504.
- [CrossRef] [PubMed] [Google Scholar]
- Duration of treatment and occlusal outcome using Damon3 self-ligated and conventional orthodontic bracket systems in extraction patients: A prospective randomized clinical trial. Am J Orthod Dentofacial Orthop. 2011;139:e111-6.
- [CrossRef] [PubMed] [Google Scholar]
- Randomized clinical trial of orthodontic treatment efficiency with self-ligating and conventional fixed orthodontic appliances. Am J Orthod Dentofacial Orthop. 2010;137:738-42.
- [CrossRef] [PubMed] [Google Scholar]
- Tooth Movement. In: Kantarci A, Will L, Yen S, eds. Frontiers of Oral Biology. Vol 18. Basel: Karger; 2016. p. :80-91.
- [CrossRef] [Google Scholar]
- Periodontal tissue activation by vibration: Intermittent stimulation by resonance vibration accelerates experimental tooth movement in rats. Am J Orthod Dentofacial Orthop. 2008;133:572-83.
- [CrossRef] [PubMed] [Google Scholar]
- Biomarkers of orthodontic tooth movement with fixed appliances and vibration appliance therapy: A pilot study. Eur J Orthod 2020:cjaa026.
- [CrossRef] [PubMed] [Google Scholar]
- Effects of supplemental vibrational force on space closure, treatment duration, and occlusal outcome: A multicenter randomized clinical trial. Am J Orthod Dentofacial Orthop. 2018;153:469-80.e4.
- [CrossRef] [PubMed] [Google Scholar]
- Assessment of the rate of premolar extraction space closure in the maxillary arch with the AcceleDent aura appliance vs no appliance in adolescents: A single-blind randomized clinical trial. Am J Orthod Dentofacial Orthop. 2018;153:8-14.
- [CrossRef] [PubMed] [Google Scholar]
- Intraoral photobiomodulation-induced orthodontic tooth alignment: A preliminary study. BMC Oral Health. 2016;16:3.
- [CrossRef] [PubMed] [Google Scholar]
- Surgical adjunctive procedures for accelerating orthodontic treatment. Cochrane Database Syst Rev. 2015;2015:CD010572.
- [CrossRef] [Google Scholar]
- Patients', parents', and orthodontists' perceptions of the need for and costs of additional procedures to reduce treatment time. Am J Orthod Dentofacial Orthop. 2014;145:S65-73.
- [CrossRef] [PubMed] [Google Scholar]
- Social perceptions of adults wearing orthodontic appliances: A cross-sectional study. Eur J Orthod. 2011;33:476-82.
- [CrossRef] [PubMed] [Google Scholar]
- A survey of undergraduate orthodontic teaching and factors affecting pursuit of postgraduate training. Br Dent J. 2016;221:487-92.
- [CrossRef] [PubMed] [Google Scholar]
- Comparison of Roth appliance and standard edgewise appliance treatment results. Am J Orthod Dentofacial Orthop. 1993;103:24-32.
- [CrossRef] [Google Scholar]
- Extraction of premolars for orthodontic reasons on the decline? A cross-sectional survey of BOS members. J Orthod 2018:1-6.
- [CrossRef] [PubMed] [Google Scholar]
- Success rate and duration of orthodontic treatment for adult patients with palatally impacted maxillary canines. Am J Orthod Dentofacial Orthop. 2003;124:509-14.
- [CrossRef] [Google Scholar]
- The time sequence of tissue regeneration in human extraction wounds. Oral Surg Oral Med Oral Pathol. 1969;27:309-18.
- [CrossRef] [Google Scholar]
- A clinical comparison of the rate of maxillary canine retraction into healed and recent extraction sites-a pilot study. Eur J Orthod. 1997;19:711-9.
- [CrossRef] [PubMed] [Google Scholar]
- Systemized orthodontic treatment mechanics Amsterdam: Elsevier Health Sciences; 2001.
- [Google Scholar]
- The timing of significant arch dimensional changes with fixed orthodontic appliances: Data from a multicenter randomised controlled trial. J Dent. 2014;42:1-6.
- [CrossRef] [PubMed] [Google Scholar]
- Which one closes extraction spaces faster: En masse retraction or two-step retraction? A randomized prospective clinical trial. Angle Orthod. 2019;89:855-61.
- [CrossRef] [PubMed] [Google Scholar]
- En masse retraction and two-step retraction of maxillary anterior teeth in adult Class I women. A comparison of anchorage loss. Angle Orthod. 2007;77:973-8.
- [CrossRef] [PubMed] [Google Scholar]
- Randomized clinical trial comparing control of maxillary anchorage with 2 retraction techniques. Am J Orthod Dentofacial Orthop. 2010;138:544.e1-9.
- [CrossRef] [PubMed] [Google Scholar]
- Effectiveness of 3 methods of anchorage reinforcement for maximum anchorage in adolescents: A 3-arm multicenter randomized clinical trial. Am J Orthod Dentofacial Orthop. 2014;146:10-20.
- [CrossRef] [PubMed] [Google Scholar]
- Intensive treatment of severe Class II malocclusions with a headgear-Herbst appliance in the early mixed dentition. Am J Orthod. 1984;86:1-13.
- [CrossRef] [Google Scholar]
- A controlled clinical trial of the effects of the twin block and dynamax appliances on the hard and soft tissues. Eur J Orthod. 2007;29:272-82.
- [CrossRef] [PubMed] [Google Scholar]
- Temporomandibular response to early and late removal of bite-jumping devices. Eur J Orthod. 2003;25:465-70.
- [CrossRef] [PubMed] [Google Scholar]




