

Translate this page into:
Accuracy of Three-dimensional Cone Beam Computed Tomography Digital Model Measurements Compared with Plaster Study Casts
Address for correspondence: Prof. Donald J. Ferguson, Dubai Healthcare City, Bldg 27, Block D, Office 302, PO Box 53382, Dubai, United Arab Emirates. E-mail: fergusonloud@gmail.com
This article was originally published by Wolters Kluwer and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Purpose
The purpose of this study was to assess the accuracy of three-dimensional (3D) cone beam computed tomography (CBCT) study casts by comparing with direct measurements taken from plaster study casts.
Materials and Methods
The dental arches of 30 patient subjects were imaged with a Kodak 9300 3D CBCT devise; Anatomodels were created and in vivo 5 imaging software was used to measure 10 dental arch variables which were compared to measurements of plaster study casts.
Results:
Three of the 10 variables, i.e., overbite, maxillary intermolar width, and arch length, were found significantly smaller (P < 0.05) using the Anatomodels following nonparametric Wilcoxon signed-rank testing. None of the differences found in the study averaged <0.5 mm.
Conclusions
3D CBCT imaging provided clinically acceptable accuracy for dental arch analysis. 3D CBCT imaging tended to underestimate the actual measurement compared to plaster study casts.
Keywords
Digital imaging
measurement accuracy
orthodontics
study cast analysis

Introduction
The importance of three-dimensional (3D) imaging and analysis of 3D study casts of dental arches based on computed tomography scans (CT) is increasing in orthodontic diagnosis, treatment planning, and simulation.[1-3] Regular CT scans failed to deliver accurate 3D reconstruction of dentition due to limited spatial resolution.[4-6] Since introduction of cone beam CT (CBCT) in dentistry in the late 1990s, CBCT imaging proved to be superior to the regular medical CT; costs and radiation exposure were reduced and CBCT had more spatial resolution with voxel size <80 μm.[7]
The amount of radiation exposure favors CBCT (25–150 μSv) technique when various radiographic imaging methods or combinations of methods are compared: exposure for a two-dimensional (2D) full mouth series is about 150 μSv; exposure for a 2D digital panoramic radiograph ranges from 4.7 to 26 μSv and averages about 10–15 μSv; average lateral cephalographs exposure is 5 μSv; exposure from a medical CT scan ranges from 1200 to 3300 μSv.[8,9]
Previous investigations have analyzed CBCT measurement accuracy of craniofacial landmarks by comparing with direct linear dry skull measurements.
Periago et al. reported that although many measurements were significantly different statistically from measurements taken with a digital caliper, CBCT measurements were considered sufficiently accurate to be clinically acceptable (90% of measurement mean differences were <2 mm).[10] Lagravère et al. compared measurements from 9- to 12-inch CBCT with a coordinate measuring machine and found no significant difference between linear and angular measurements; all differences were <1 mm or 1°.[11] Ballrick et al. used a custom phantom to evaluate images produced by a commercially available (CBCT) machine for measurement and spatial resolution for all settings and in all dimensions and found no significant difference for 3D images for all settings; there was a statistically significant difference when CBCT measurements were compared to caliper measurement; but clinically, it was <0.1 mm.[12]
Measurement accuracy of CBCT study casts has been compared with direct measurements using other study casts measurement techniques. Tarazona et al. (2013) found that CBCT digital models were as accurate and reliable as digital study casts obtained from plaster casts; differences found were clinically acceptable.[4] CBCT models and digital study casts were compared by de Waard et al. for reproducibility and accuracy of linear measurement; measurements made directly on CBCT images and Anatomodels were not as accurate as measurement on digimodels.[13] Baumgaertel et al. compared dry skull dental measurements with the accuracy and reliability of CBCT reconstruction dental measurements and found high reliability; however, the CBCT tended to slightly underestimate anatomic truth, but it was significant for combined measurements only.[14] Damstra et al. found that measurement on 3D models of 0.25 × 0.40 voxel is accurate compared with direct caliper measurements and increasing voxel resolution did not result in greater accuracy.[15]
Study cast digital imaging techniques have been investigated. Kau et al. found no statistically significant difference between CBCT digital model and OrthoCAD digital model in linear measurement for overbite (OB), overjet (OJ), and crowding.[16] Liu et al. studied the accuracy of volumetric analysis of teeth in vivo and found CBCT to be feasible with 4%–7% deviation in CBCT from the actual physical volume, and smoothing operation reduced the volume measurement.[17] Al-Rawi et al. studied the influence of field of view selection on the reconstruction accuracy and found that CBCT may provide accurate 3D reconstruction of the teeth.[18]
With the development in imaging technology and the growing awareness of the importance of chairside time and efficiency, many clinicians are using study casts obtained from CBCT because they are less time-consuming (no impression taking), do not require space for storage, and the technique is convenient for the patient. However, Kau et al. have pointed out that although CBCT volume images can give the clinician a 3D representation of the teeth, its accuracy and reliability for dental measurements have not been fully assessed.[16] While the 3D study cast technique is a relatively new trend, not many studies have been performed to assess 3D CBCT measurement accuracy.
The aim of our study was to assess the accuracy of 3D CBCT study casts by comparing with direct measurements taken from plaster study casts.
Materials and Methods
Sample
The 3D CBCT study cast images of 30 patient subjects, 17 males (mean age 31.6 years) and 13 females (mean age 29.1 years) treated at European University College comprised the sample; initial diagnoses were Class III (n = 2), Class II (n = 11), and Class I (n = 19).
Procedures
Study casts were obtained using alginate impression material and poured immediately. 3D study cast images were secured using a Kodk 9000C (Carestream Health, Inc., France) machine with exposure conditions of 120 kV, 5 mA, voxel size 76 × 76 × 76 and scope of exposure set to 50 mm × 37 mm. The subjects were seated comfortably maintaining a maximum intercuspal position and asked to stare at their own eyes in a mirror reflection with the mirror located 1.5 m in front of them. The CBCT scans were sent to Anatomage where 3D facial model was obtained with 3D Anatomodel images of study casts (Anatomage Inc., 111 N. Market St. Suite 500, San Jose, CA 95113, www.anatomage.com).
Using direct and 3D CBCT measurement techniques, the following 10 study variables were recorded [Figure 1]:
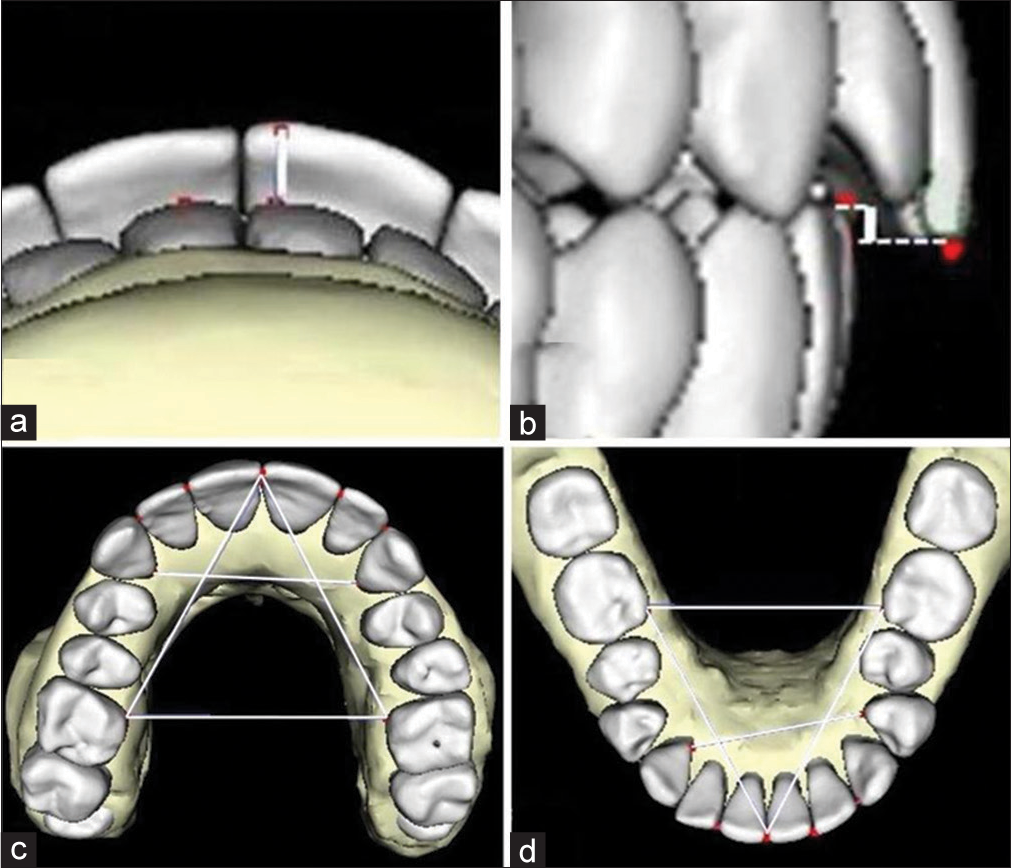
- Measurements used in the study (white lines connected to red dots) representing overjet (a), overbite (b), maxillary arch length, intercanine and intermolar distances (c) and mandibular arch length, intercanine and intermolar distances (d). See narrative for landmark identification.
OB
OJ
Intercanine width for maxillary dental arch (UIC)
Intercanine width for mandibular dental arch (LIC)
Intermolar width for maxillary arch (UIM)
Intermolar width for mandibular arch (LIM)
Arch length for maxillary arch (UAL)
Arch length for mandibular arch (LAL)
Anterior Bolton ratio (ABR)
Overall Bolton ratio (OBR).
Intercanine width was measure from deepest point in the lingual gingival border below the cingulum. Intermolar width was measured from the mesiolingual gingival margin of the first molar. Arch length measurement was the distance from mesiolingual gingival margin of the first molar to the contact point between the incisors then taking the sum of the right and left.[19,20]
The measurements on the plaster study casts were performed using a digital caliper; measurements on CBCT were performed on Anatomodel images using In Vivo 5 imaging software. All the measurement on the plaster study casts and the 3D CBCT model were performed by the primary examiner (Shuaib Al Ali). Differences between 3D CBCT and direct study cast images are illustrated for one subject [Figure 2].

- Overall comparison of three-dimensional anatomodel image reconstructed from cone beam computed tomography scans (top row) with plaster study casts (bottom row)
Statistical analysis
Measurements for 10 cases randomly selected were performed twice, once by the primary examiner (SAA) and a second examiner (PP), at 10 days apart to determine measurement technique reliability. Paired t-test results indicated no significant (P > 0.05) intra- or inter-operator differences.
All measurements values were recorded in Excel and imported for analysis with Statistical Package for Social Services software, version 15.0.1, IBM, Armonk, NY. Statistical analysis demonstrated that the data were not equally distributed; thus, the nonparametric Wilcoxon signed-rank test was used with significance level established at P < 0.05; measurement differences averaging >0.5 mm were considered “clinically” significant.
Results
Three measurement variables averaged significantly smaller (P < 0.05) for the Anatomodel images: OB (1.87 vs. 2.20 mm), maxillary intermolar width (33.70 vs. 34.17 mm), and maxillary arch length (62.80 vs. 63.27 mm). All the mean differences were <0.5 mm; hence, the differences were considered clinically insignificant [Table 1].
| Variable 3D | CBCT | Study cast | P significant | |||
|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | P | P<0.05 | |
| OJ | 3.57 | 3.73 | 3.63 | 3.88 | 0.536 | NS |
| OB | 1.87 | 2.01 | 2.20 | 1.96 | 0.005 | ** |
| UIC | 24.27 | 3.45 | 24.47 | 3.31 | 0.339 | NS |
| UIM | 33.70 | 5.07 | 34.17 | 4.73 | 0.017 | * |
| LIC | 20.07 | 1.36 | 20.33 | 1.85 | 0.174 | NS |
| LIM | 35.13 | 4.64 | 34.90 | 4.64 | 0.257 | NS |
| UAL | 62.80 | 6.39 | 63.27 | 6.62 | 0.037 | * |
| LAL | 55.23 | 5.53 | 55.70 | 5.38 | 0.114 | NS |
| ABR | 76.77 | 4.42 | 76.90 | 4.32 | 0.690 | NS |
| OBR | 84.70 | 5.77 | 84.73 | 5.72 | 0.923 | NS |
OJ - Overjet; OB - Overbite; UIC - Maxillary inter-canine distance; UIM - Maxillary inter-molar distance; LIC - Mandibular inter-canine distance; LIM - Mandibular inter-molar distance; UAL - Maxillary arch length; LAL - Mandibular arch length; ABR - Anterior Bolton ratio; OBR - Overall Bolton ratio; CBCT - Cone beam computed tomography; SD - Standard deviation; NS - Not significant; *-P<.05; ** - P<.01
The results indicated that CBCT tends to underestimate the actual measurements slightly when compared with direct study cast measurement as all the mean differences were found smaller in the 3D CBCT method except mandibular intermolar width which was slightly larger. Angle classification did not appear to influence the differences between the two measurement methods.
Discussion
There are various methods of producing images of 3D digital study casts. Using the Kodak 9000C CBCT machine, CT images were captured and reassembled by Anatomage to render 3D study casts images that were subsequently measured and compared to direct measurements from plaster study casts. The primary findings of the present study were that three of 10 measurement variables differed statistically, i.e., OB, maxillary intermolar width (UIM), and maxillary arch length (UAL). None of the measurement differences exceeded 0.5 mm. Moreover, there were no significant (P > 0.05), intra- or inter-operator differences indicating technique reliability.
Based on the conditions of the present study, i.e., measurement differences <0.5 mm considered “clinically” acceptable, results are consistent with Tarazona et al.[4] and Ballrick et al.[12] However, present results were not consistent with de Waard et al.[13] who reported average differences between Anatomodels and plaster study casts ranged from −0.42 to −0.84 mm with limits of agreement values up to 1.65 mm; the authors concluded that Anatomodels were not as accurate as measurements on plaster study casts.
Baumgaertel et al.[14] reported that combined measurements were less accurate which was demonstrated in the present study, wherein maxillary arch length consisting of two linear measurements was found to be significantly different; the combined measurements of the present study represented by anterior and OBRs were not significantly different between the direct and 3D CBCT techniques.
Reasons for significant differences of the three measurements found in the present study are difficult to explain. The differences may be due to technical difficulties in the In Vivo 5 program as some measurements have been shown to be difficult to measure such as OJ in open bite cases or inaccurate reconstruction of the anatomic feature of the occlusal surfaces.[13]
The time required to do measurements on the 3D CBCT model image was almost the same as that needed to do the measurement on the plaster study casts, especially after becoming familiar, with the In Vivo 5 application and doing a few cases.
The In Vivo 5 method presented an advantage over the plaster study cast method in that clinical time needed to take an impression was eliminated in addition to the inconvenience to the patient with impression taking. Moreover, the 3D CBCT imaging technique was an easy way to capture and retain an image of the patient’s dentition. Transfer the records between practitioners, especially with the volume wrapping features of Anatomage, provided 3D facial models that proved to be accurate and can aid in the diagnosis as reported by Premjani et al.[21]
The advantages of CBCT must be balanced with the additional cost needed either to have the CBCT or the 3D model and the exposure to ionizing radiation even though the radiation dose is much less than that of normal CT. Furthermore, the presence of implants, metallic braces, or metallic prosthetic restorations can impair the quality of the image obtained. Hence, use of CBCT imaging may not be feasible as a clinical routine.
Conclusions
The dental arches of 30 patient subjects were imaged with a Kodak 9300 3D CBCT devise; anatomodels were created and In Vivo 5 imaging software was used to measure 10 dental arch variables which were compared to measurements of plaster study casts. Three of the 10 variables, i.e., OB, maxillary intermolar width, and arch length, were found significantly smaller (P < 0.05) using the 3D CBCT method following nonparametric Wilcoxon signed-rank testing. None of the differences found in the study averaged >0.5 mm.
Based on the conditions of the present investigation, it may be concluded that 3D CBCT imaging provided clinically acceptable accuracy for dental arch analysis. 3D CBCT imaging tended to underestimate the actual measurement compared to plaster study casts.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Validation and reproducibility of a high-resolution three-dimensional facial imaging system. Br J Oral Maxillofac Surg. 2008;46:27-32.
- [CrossRef] [Google Scholar]
- State of the art of fusion of computed tomography data and optical 3D images. Int J Comput Dent. 2007;10:11-24.
- [Google Scholar]
- A comparison of craniofacial morphology in patients with and without facial asymmetry – A three-dimensional analysis with computed tomography. Int J Oral Maxillofac Surg. 2006;35:43-8.
- [Google Scholar]
- A comparison between dental measurements taken from CBCT models and those taken from a digital method. Eur J Orthod. 2013;35:1-6.
- [Google Scholar]
- Three-dimensional digital modeling and setup. Am J Orthod Dentofacial Orthop. 2006;129:605-10.
- [CrossRef] [PubMed] [Google Scholar]
- Fusion of computed tomography data and optical 3D images of the dentition for streak artefact correction in the simulation of orthognathic surgery. Dentomaxillofac Radiol. 2004;33:226-32.
- [Google Scholar]
- Large scan field, high spatial resolution flat-panel detector based volumetric CT of the whole human skull base and for maxillofacial imaging. Dentomaxillofac Radiol. 2007;36:317-27.
- [Google Scholar]
- Operational principles for cone-beam computed tomography. J Am Dent Assoc. 2010;141(3):3S-6S.
- [CrossRef] [Google Scholar]
- Comparison of radiation levels from computed tomography and conventional dental radiographs. Aust Orthod J. 2003;19:67-75.
- [Google Scholar]
- Linear accuracy and reliability of cone beam CT derived 3-dimensional images constructed using an orthodontic volumetric rendering program. Angle Orthod. 2008;78:387-95.
- [Google Scholar]
- Three-dimensional accuracy of measurements made with software on cone-beam computed tomography images. Am J Orthod Dentofacial Orthop. 2008;134:112-6.
- [Google Scholar]
- Image distortion and spatial resolution of a commercially available cone-beam computed tomography machine. Am J Orthod Dentofacial Orthop. 2008;134:573-82.
- [Google Scholar]
- Reproducibility and accuracy of linear measurements on dental models derived from cone-beam computed tomography compared with digital dental casts. Am J Orthod Dentofacial Orthop. 2014;146:328-36.
- [CrossRef] [PubMed] [Google Scholar]
- Reliability and accuracy of cone-beam computed tomography dental measurements. Am J Orthod Dentofacial Orthop. 2009;136:19-25.
- [CrossRef] [Google Scholar]
- Accuracy of linear measurements from cone-beam computed tomography-derived surface models of different voxel sizes. Am J Orthod Dentofacial Orthop. 2010;137:16.e1-6.
- [Google Scholar]
- Evaluation of CBCT digital models and traditional models using the little’s index. Angle Orthod. 2010;80:435-9.
- [CrossRef] [PubMed] [Google Scholar]
- The validity of in vivo tooth volume determinations from cone-beam computed tomography. Angle Orthod. 2010;80:160-6.
- [Google Scholar]
- Accuracy assessment of three-dimensional surface reconstructions of teeth from cone beam computed tomography scans. J Oral Rehabil. 2010;37:352-8.
- [Google Scholar]
- Mandibular dental arch form and dimension. Treatment and postretention changes. Am J Orthod. 1974;66:58-70.
- [Google Scholar]
- Artifact-resistant superimposition of digital dental models and cone-beam computed tomography images. J Oral Maxillofac Surg. 2013;71:1933-47.
- [Google Scholar]
- Accuracy of 3D facial models obtained from CBCT volume wrapping. J Clin Orthod. 2015;49:641-6.
- [Google Scholar]




