

Translate this page into:
Adjunctive surgery after total arch distalization to optimize esthetics


*Corresponding author: Yoon-Ah Kook, Department of Orthodontics, The Catholic University of Korea, Seocho-Gu, Seoul, Korea. kook190036@yahoo.com
-
Received: ,
Accepted: ,
How to cite this article: Abdulwhab A, Ku JH, Alfawaz F, Park JH, Kook Y. Adjunctive surgery after total arch distalization to optimize esthetics. APOS Trends Orthod 2020;10(3):185-90.
Abstract
This case report presents surgically assisted orthodontic treatment for an adult patient due to labial exostosis, prominent malar, and unesthetic chin. Her treatment was total arch distalization with modified C-palatal plate for maxillary arch and miniscrews for mandibular arch. In addition, she was treated with alveoloplasty, malarplasty, and genioplasty to improve the consistency of her profile. The total treatment duration was 28 months.
Keywords
Total arch distalization
Modified C-Platal plate
Buccal miniscrew
Adjunctive surgery
Esthetics

INTRODUCTION
The lower third of the face plays an important role in the overall harmony of the facial profile. Patients with prominent lips and chin are seeking orthodontic treatment or orthognathic surgery to improve their profile.[1,2]
An unfavorable bone response may occur after retraction of anterior teeth. The alveolar bone remodeling can cause visible bone exostosis, labial bone protuberance, and an irregular ridge of bone.[3-6] Exostosis usually causes esthetic problems and alveoloplasty can be used to eliminate excess alveolar bone. Yodthong et al.[7] concluded that rate of tooth movement and extent of intrusion were significant factors that may influence alveolar bone thickness during incisor retraction.
Recently, temporary skeletal anchorage devices (TSADs) have decreased the need for extractions and surgical approaches.[8-12] Previous studies have reported that miniscrews are often placed in the retromolar area, buccal shelves, and inter-radicular area for total arch distalization of the mandible.[9,10,13,14] In the maxilla, Kook et al.[15] have demonstrated the application of a modified C-palatal plate (MCPP) for total arch distalization. It is simple and effective in distalization of the maxillary dentition in both adolescents and adults.[16]
In this paper, we present a female adult patient with Class III skeletal pattern with low mandibular plane angle, who was treated by total maxillary and mandibular arch distalization with alveoloplasty and malarplasty in the maxilla and genioplasty in the mandible.
DIAGNOSIS
A 48-year-old Korean woman attended to the Department of Orthodontics, Seoul St. Mary’s Hospital, the Catholic University of Korea. Her chief complaints were protrusive lips, unesthetic chin, and prominent zygomatic process [Figure 1]. However, she had received orthodontic treatment previously in a private orthodontic office for two years but she was not satisfied with the result.
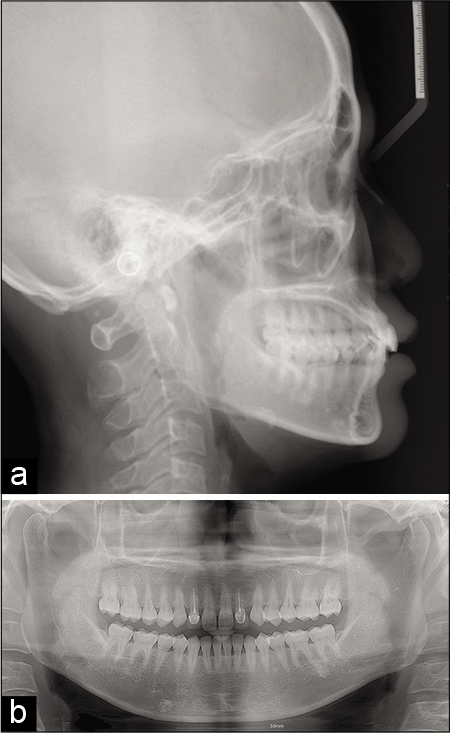
- Initial pre-treatment lateral cephalogram (a) and panoramic radiograph (b).
A clinical examination showed facial symmetry from the frontal view and a slightly concave profile with protrusive upper lip. The intraoral examination revealed Class I canine and molar relationships with a 2.7 mm overjet and 1.8 mm overbite, and the mandibular dental midline was shifted 1 mm right compared with her facial midline. Her maxillary lateral incisors had restorations. She also had an unesthetic gingival margin on the maxillary anterior teeth and open gingival embrasures on the mandibular incisors. In the maxilla, buccal exostoses were found in the posterior area [Figure 2].

- Pre-treatment photographs and lateral cephalogram after orthodontic treatment at the private orthodontic office.
Panoramic evaluation showed no pathologic signs and an absence of third molars. The maxillary right and left lateral incisors had received root canal treatment.
Lateral cephalometric analysis revealed Class III relationship (ANB, 0.2°; Wits, –3.2 mm) with a hypodivergent growth pattern (FMA, 20.2°). Regarding soft tissue, upper lip, lower lip, and soft tissue Pog to TVL were 9.3 mm, 7.1 mm, and 2.2 mm, respectively and nasolabial angle was 67.8°. All these measurements indicate that the patient’s lips and chin were protrusive.
TREATMENT OBJECTIVES
The treatment objectives were to correct the protrusive lips and chin in order to improve the patient’s profile, obtain optimal inclination of the anterior teeth, maintain the normal overbite and overjet, and maintain the Class I molar and canine relationships. The patient also wanted to improve her facial appearance; she had a brachycephalic face with zygomatic protrusion.
TREATMENT ALTERNATIVES
Three different treatment options were suggested. The first option was two-jaw surgery without extraction of premolars. The second option was to extract the four first premolars. The third option was the total arch distalization of the maxillary and mandibular dentition using a MCPP and miniscrews for for intrusion of mandibular anterior teeth combined with alveoloplasty, genioplasty, and malar reduction. The patient agreed to the third plan because she did not like to extract her teeth and did not wish to have her teeth extracted and did not want orthognathic surgery.
TREATMENT PROGRESS
Before orthodontic treatment, the patient was referred to a periodontist for the treatment of periodontitis. A fixed appliance with straight wire technique and 0.022 inch slot brackets and bands (Tomy, Tokyo, Japan) was placed on the maxillary and mandibular teeth including the second molars. A MCPP was placed in the palate with three miniscrews (2.0 × 8 mm; Jeil Medical, Seoul, Korea) [Figures 3a and b]. The maxillary first molars were banded, and a palatal retraction arch was fabricated with the arch running above the gingival margin. Approximately 250 g of distalizing force was engaged from the hooks on the palatal retraction arch to the notches of the palatal plate by elastomeric chains or nickel-titanium closed coil springs. They were replaced at every visit, and the length of the chain was updated. A miniscrew with 1.8 mm diameter and 8 mm in length was placed bilaterally between the roots of the mandibular first and second molars for 16 months, and 400 g of distalization force was applied bilaterally [Figure 3c]. Total treatment duration was 28 months.
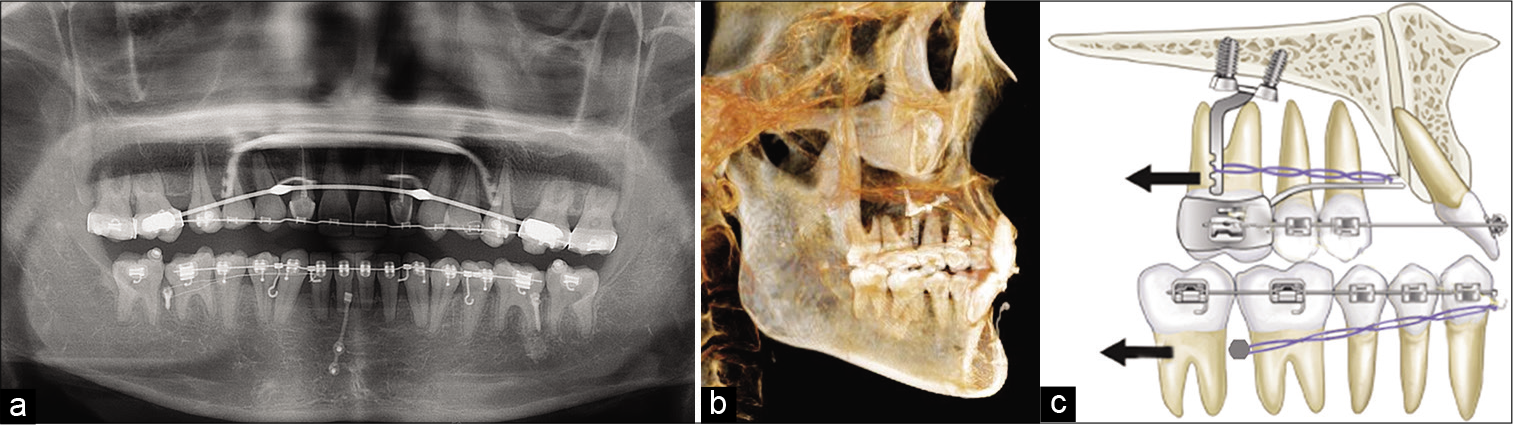
- Treatment progress radiographs (a) 13 months, (b) 26 months, (c) total arch distalization with modified C-palatal plate in the maxilla and buccal miniscrews in the mandible (black arrow means direction of distalization).
However, after distalization of the maxillary and mandibular arches, the chin had become more prominent [Figure 3b], and the patient still had a protrusive upper lip [Figure 4]. Therefore, the patient was referred to an oral surgeon for the alveoloplasty in the maxillary anterior segment, genioplasty, and malar reduction [Figure 5].

- Post-treatment photographs and CBCT images with exostoses between upper right and left canines.
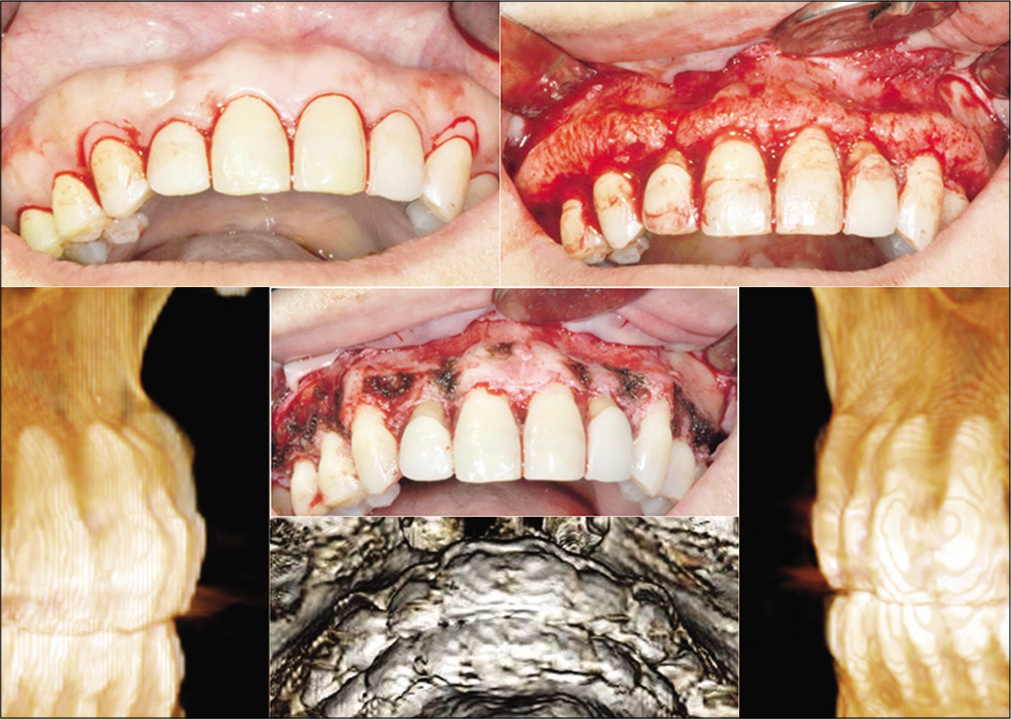
- Intraoral photographs during alveoloplasty and CBCT images after alveoloplasty.
TREATMENT RESULTS
Class I canine and molar relationships were maintained with a canine-protected occlusion. The post-treatment photographs show an improved profile with a beautiful smile [Figure 6a]. Lip protrusion and chin contour were improved. A balanced lip position was achieved. The panoramic radiograph showed good root paralleling with no spacing and a slight root resorption in the mandibular anterior teeth [Figure 6b].
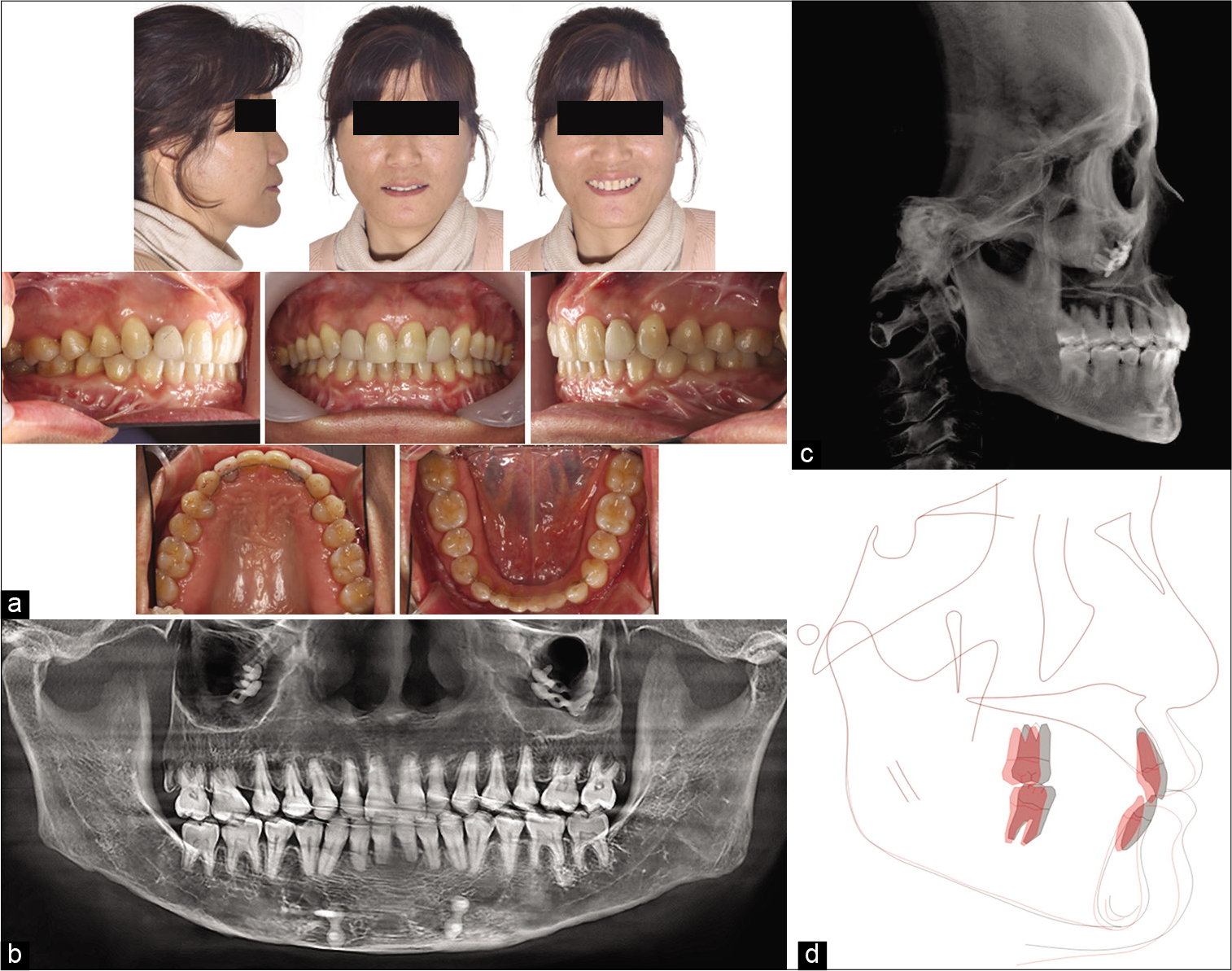
- Post-treatment photographs (a), panoramic radiograph (b), lateral cephalogram (c), and superimposition (d).
A lateral cephalogram shows the mandibular plane angle was maintained, which made her chin point more prominent [Figures 6c and d]. The superimpositions showed the amounts of retraction and uprighting of the maxillary and mandibular incisors that contributed to improved profile [Figure 6d]. The patient had no temporomandibular joint pain or discomfort after treatment and she was satisfied with the result.
DISCUSSION
At present, increasing numbers of patients are seeking orthodontic treatment to improve facial attractiveness, which improves their quality of life.[17,18] Especially lip position, cheek volume, and chin contour play an important role with facial profiles.[19,20]
In this case report, the patient had prominent lips and chin with a broad zygomatic process and slightly concave profile which is considered less attractive. However, total arch distalization with TSADs along with adjunctive surgery improved the protrusive lips, chin, and cheeks without orthognathic surgery. MCPP was applied for total maxillary arch distalization because she rejected extraction. Previous MCPP studies reported distalization of the maxillary dental arch and correction of protruded anterior teeth without the need for extractions.[15,21]
On the other hand, total distalization of the mandible is challenging. In this report, miniscrews were placed between the mandibular first and second molars for total mandibular arch distalization in 14 months. After distalization of both arches, FMA was maintained and incisors were retracted, which made the chin point more protrusive.
Kook et al.[22] reported distalization of the mandibular dentition with a ramal plate. They showed clockwise rotation of the mandible with less protrusive chin due to extrusion of molars. Therefore, it is recommended to select the proper skeletal anchorage device based on the vertical pattern of each individual Class III patient. In our case, we might have been able to avoid reduction genioplasty if we had used ramal plates instead of miniscrew.
In a previous case report,[23] only Class III elastics were applied along with MCPP to distalize mandibular dentition, however to take advantage of the full retraction capacity of the MCPP, Jo et al.[24] recommended additional distalization modalities in the mandibular arch. In our case, miniscrews were used for the mandibular total arch distalization, which resulted in more efficient movement.
With orthognathic surgery, mandibular setback alone could correct mandibular prognathism but it does not make the chin region appear slender.[15,21] Therefore, reduction genioplasty was considered to improve her concave profile. Some clinicians and laypersons consider soft-tissue pogonion on or just behind the true vertical line to be the most attractive.[25]
In our case report, we achieved an ideal position of the soft-tissue pogonion post-treatment for well-perceived attractiveness [Table 1].
| Norm±S.D. | Pre-treatment | Post-treatment | |
|---|---|---|---|
| SNA (°) | 82.0±2.0 | 83.3 | 83.3 |
| SNB (°) | 80.0±2.0 | 83.1 | 82.7 |
| ANB (°) | 3.5±1.9 | 0.2 | 0.6 |
| Wits appraisal (mm) | ‒2.5±1.8 | ‒3.2 | ‒3.0 |
| Harvold analysis (mm) | 26.0±4.0 | 29.6 | 29.4 |
| FMA (°) | 22.0±3.0 | 20.2 | 20.2 |
| U1-FH (°) | 114.0±6.5 | 116.8 | 91.8 |
| IMPA (°) | 91.6±2.0 | 95.7 | 86.8 |
| Interincisal angle (°) | 124.0±8.3 | 126.3 | 159.1 |
| Nasolabial angle (°) | 84.9±5.0 | 67.8 | 81.3 |
| True vertical upper lip (mm) | 3.7±1.2 | 9.3 | 5.1 |
| True vertical lower lip (mm) | 1.9±1.4 | 7.1 | 2.4 |
| True vertical Pog (mm) | ‒2.6±1.9 | 2.2 | ‒0.2 |
| Sn-Stm (mm) | 22.6±2.1 | 21.3 | 22.7 |
| Stm-Me (mm) | 48.8±3.3 | 33.5 | 32.7 |
| Stm-Me/Sn-Stm | 2.0±0.2 | 1.6 | 1.4 |
Labial exostoses between the left and right canine area, labial surface of the maxillary alveolar ridge could have caused protrusion of the upper lip. Surgical reduction of the exostoses might have relieved the upper lip protrusion. Jainkittivong and Langlais[26] have reported that the existence of exostoses comes with aging and its etiology is multifactorial including genetic and functional influences. Our report showed improved lip protrusion after distalization and exostoses reduction.
A long and oval face is preferred, while a broad and square face is considered to be esthetically unattractive.[10] An unpleasant wide midface bony contour can be caused by prominence of the zygomatic bone. To improve unattractive midface, surgical zygomatic reduction methods are usually applied.
In our case report, the esthetic results with adjunctive surgery after total arch distalization were satisfactory. Further study is recommended to statistically analyze the treatment effects of total arch distalization using TADs with adjunctive surgeries in Class III cases.
CONCLUSION
Esthetic improvement of facial appearance can be achieved by total arch distalization of both arches using TADs and adjunctive surgeries in patients with bimaxillary protrusion and prominent chin without extraction and jaw surgery. It is recommended for clinicians to consider adjunctive surgeries for enhancing esthetics in diagnosis and treatment planning of Class III malocclusion.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
Dr. Yoon Ah Kook is on the Editorial Board of the Journal.
References
- Profile and soft tissue changes during and after orthodontic treatment. Eur J Orthod. 1979;1:193-9.
- [CrossRef] [PubMed] [Google Scholar]
- Influence of setback and advancement osseous genioplasty on facial outcome: A computer-simulated study. J Craniomaxillofac Surg. 2015;43:2017-25.
- [CrossRef] [PubMed] [Google Scholar]
- Observations on the response of alveolar bone to orthodontic force. Am J Orthod. 1970;58:284-94.
- [CrossRef] [Google Scholar]
- Changes in alveolar bone thickness due to retraction of anterior teeth. Am J Orthod Dentofacial Orthop. 2002;122:15-26.
- [CrossRef] [PubMed] [Google Scholar]
- Treatment of severe bimaxillary protrusion with miniscrew anchorage: Treatment and complication. Aust Orthod J. 2008;24:156-63.
- [Google Scholar]
- Treatment of skeletal-origin gummy smiles with miniscrew anchorage. J Clin Orthod. 2008;5:285-96.
- [Google Scholar]
- Factors related to alveolar bone thickness during upper incisor retraction. Angle Orthod. 2013;83:394-401.
- [CrossRef] [PubMed] [Google Scholar]
- Nonsurgical correction of a Class III malocclusion in an adult by miniscrew-assisted mandibular dentition distalization. Am J Orthod Dentofacial Orthop. 2013;143:877-87.
- [CrossRef] [PubMed] [Google Scholar]
- Dentoalveolar Class III treatment using retromolar miniscrew anchorage. Prog Orthod. 2013;14:7.
- [CrossRef] [PubMed] [Google Scholar]
- Use of mini-implants to avoid maxillary surgery for Class III mandibular prognathic patient: A long-term post-retention case. Korean J Orthod. 2014;44:342-9.
- [CrossRef] [PubMed] [Google Scholar]
- Distal movement of the mandibular dentition with temporary skeletal anchorage devices to correct a Class III malocclusion. Am J Orthod Dentofacial Orthop. 2013;144:715-25.
- [CrossRef] [PubMed] [Google Scholar]
- Primary failure rate for 1680 extra-alveolar mandibular buccal shelf mini-screws placed in movable mucosa or attached gingiva. Angle Orthod. 2015;85:905-10.
- [CrossRef] [PubMed] [Google Scholar]
- Biology of biomechanics: Finite element analysis of a statically determinate system to rotate the occlusal plane for correction of a skeletal Class III open-bite malocclusion. Am J Orthod Dentofacial Orthop. 2015;148:943-55.
- [CrossRef] [PubMed] [Google Scholar]
- Three-dimensional evaluation of interradicular spaces and cortical bone thickness for the placement and initial stability of microimplants in adults. Am J Orthod Dentofacial Orthop. 2009;136:314.e1-12.
- [CrossRef] [PubMed] [Google Scholar]
- Treatment effects of a modified palatal anchorage plate for distalization evaluated with cone-beam computed tomography. Am J Orthod Dentofacial Orthop. 2014;146:47-54.
- [CrossRef] [PubMed] [Google Scholar]
- A modified palatal anchorage plate for simple and efficient distalization. J Clin Orthod. 2010;44:719-30.
- [Google Scholar]
- A three-dimensional photogrammetric analysis of the facial esthetics of the Miss Korea pageant contestants. Korean J Orthod. 2017;47:87-99.
- [CrossRef] [PubMed] [Google Scholar]
- Orthodontic applications of psychological and perceptual studies of facial esthetics. Semin Orthod. 1995;1:82-93.
- [CrossRef] [Google Scholar]
- Change in quality of life after combined orthodontic-surgical treatment of dentofacial deformities. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2010;109:46-51.
- [CrossRef] [PubMed] [Google Scholar]
- Facial aesthetics and the assignment of personality traits before and after orthognathic surgery. Int J Oral Maxillofac Surg. 2012;41:469-76.
- [CrossRef] [PubMed] [Google Scholar]
- Comparison of treatment effects between the modified C-palatal plate and cervical pull headgear for total arch distalization in adults. Korean J Orthod. 2017;47:375-83.
- [CrossRef] [PubMed] [Google Scholar]
- Distalization of the mandibular dentition with a ramal plate for skeletal Class III malocclusion correction. Am J Orthod Dentofacial Orthop. 2016;150:364-77.
- [CrossRef] [PubMed] [Google Scholar]
- Application of palatal plate for nonextraction treatment in an adolescent boy with severe overjet. Am J Orthod Dentofacial Orthop. 2017;152:859-69.
- [CrossRef] [PubMed] [Google Scholar]
- Comparison of treatment effects between four premolar extraction and total arch distalization using the modified C-palatal plate. Korean J Orthod. 2018;48:224-35.
- [CrossRef] [PubMed] [Google Scholar]
- An evaluation of preferred lip positions according to different age groups. Int J Oral Maxillofac Surg. 2013;42:637-42.
- [CrossRef] [PubMed] [Google Scholar]
- Buccal and palatal exostoses: Prevalence and concurrence with tori. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2000;90:48-53.
- [CrossRef] [PubMed] [Google Scholar]




