

Translate this page into:
Anatomic considerations during placement of mandibular retromolar miniplates for orthodontic anchorage – A study of the characteristics of retromolar fossa

*Corresponding author: Sharanya Sabrish, Associate Professor, Department of Orthodontics FDS, MSRUAS, Bengaluru, Karnataka, India. drsharanyaortho@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Sharma PN, Sabrish S, Prashantha GS, Sagarkar R, Mathew S, Krishnamurthy S. Anatomic considerations during placement of mandibular retromolar miniplates for orthodontic anchorage – A study of the characteristics of retromolar fossa. APOS Trends Orthod. 2025;15:42-8. doi: 10.25259/APOS_1_2024
Abstract
Objectives:
The mandibular retromolar area offers a novel site for orthodontic skeletal anchorage. It houses the retromolar foramen (RMF), and surgical interventions in this area can lead to undesirable outcomes. This study aims to assess the characteristics of the RMF and its relation to the occlusal plane (OP) using cone-beam computed tomography (CBCT) data.
Material and Methods:
This cross-sectional observational in vitro study involved the analysis of CBCT data from 136 samples (68 males and 68 females) within the age range of 18–40 years. The study focused on factors such as the presence or absence of the RMF, whether it was unilateral or bilateral, the number of foramina on each side, and the distance of the RMF from the OP. Data analysis was conducted using the Statistical Package for the Social Sciences software, with P < 0.05 deemed statistically significant at a 95% confidence level.
Results:
About 39% of the sample showed the presence of RMF. The prevalence of unilateral RMF was higher than that of bilateral RMF. The mean distance of RMF above the OP was 5.99 mm, and that below the OP was 3.82 mm.
Conclusion:
The high prevalence (39%) of RMF suggests that the retromolar fossa region should be evaluated before the placement of mini-plates. The prevalence of RMF above the OP was significantly higher than that below the OP.
Keywords
Cone-beam computed tomography
Miniplates
Retromolar area
Retromolar foramen
Retromolar miniplates

INTRODUCTION
For individuals with skeletal Class III malocclusion, orthognathic surgery is often the standard treatment choice. However, mild-to-moderate skeletal Class III cases can alternatively be managed with a camouflage.[1] In these instances, distalization of the mandibular molars allows for the retraction of the lower incisors to achieve a positive overjet.[2] The current trend in orthodontics involves utilizing stainless steel bone screws positioned in the buccal shelf area for mandibular arch distalization.[3] Buccal shelf screws offer enhanced stability compared to the traditional interradicular miniscrews.[3] An alternative approach involves the use of mini plates for anchorage. Notably, miniplates offer superior stability compared to miniscrews, thus constituting a key advantage.[4]
Sugawara and Nishimura incorporated miniplates in the mandibular body for various purposes such as distalizing the mandibular dentition, correcting mandibular anterior crowding, managing asymmetrical mandibular dentition, anterior crossbite with a Class III dentition, and to assist decompensation of the mandibular incisors in patients requiring mandibular advancement.[4,5] Other authors have placed the miniplates in the retromolar area to optimize the direction of the force application[2] [Figure 1]. During enmasse retraction involving either the anteriors or the full arch, it is advantageous for the line of action of the force to pass parallel to the occlusal plane (OP). This prevents rotation of the OP and dentition.[5]
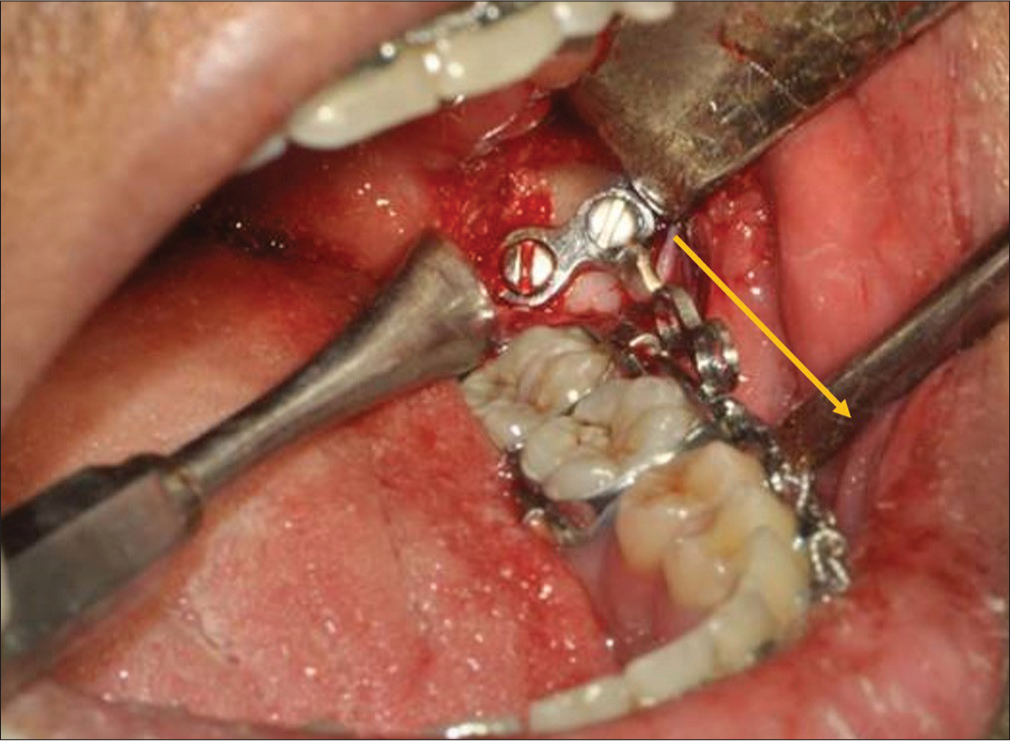
- Miniplate in the retromolar site surgically inserted to provide orthodontic anchorage. Note the point of force attachment is more along the line of occlusion as denoted by the yellow arrow leading to lesser side effects.
Despite their convenience, such extraradicular surgical anchorage sites should not be used indiscriminately. The anatomic landmarks in the area should be given due consideration. In this region, known as the retromolar area, one or more variable foramina, known as the retromolar foramen (RMF), can be present. These foramina allow the passage of vascular-nerve bundles that play a crucial role in supplying nutrition and providing innervation to the pulp and periodontium of the molar teeth[6] [Figure 2]. The RMF is the apertures of the retromolar canal (RMC), which normally arises from the mandibular canal behind the third molar and travels anterosuperiorly to the RMF.[7] The RMF is located posterior to the last molar in the “retromolar trigone” area [Figure 2], which is bounded anteriorly by the third molar, medially by the temporal crest, and laterally by the anterior border of the ramus.[8] The contents of the canal include a myelinated nerve and one or more arterioles and/or venules.[9] The nerve that runs through the RMC usually arises from the early accessory branches of the inferior alveolar nerve or long buccal nerve.[10]

- Anatomy of retromolar area showing the retromolar trigone and retromolar foramen (black arrows). RMF: Retromolar formamen
When a ramal plate is inserted in this region, there is a risk of placing the screws close to the RMF.[2] The incidence of this occurring has been reported to be variable.[2] The most common complications of such damage include paresthesia, traumatic neuroma, bleeding, hematoma, or bruising.[8] These plates will also need to be removed after the active phase of orthodontics, and hence, the second surgical procedure carries the same risk.
The presence and position of the RMF varies based on ethnicity and other factors.[11,12] The variability in the position and morphology of the foramen and canal should be taken into account during anesthetic, surgical, and implantation procedures of the mandible.[12] Studies have been carried out on dry bone samples documenting the prevalence of RMF.[13] However, the literature regarding the characteristics of the RMF in a South Asian (Indian) population assessed using cone-beam computed tomography (CBCT) and its relation to the OP is limited. These factors are important from an orthodontic point of view.
Thus, this study aimed to evaluate the anatomic considerations during the placement of retromolar miniplates and study the characteristics of the RMF using CBCT in a South Asian population sample.
MATERIAL AND METHODS
A cross-sectional observational in vitro study was designed. Data were sourced from CBCT images of the mandibular retromolar area and posterior dentition area obtained from the archives. The images underwent reconstruction and were standardized in their orientation. The study encompassed individuals within the age range of 18–40 years. Given that the application of retromolar miniplates for mandibular distalization is generally reserved for non-growing adult patients in orthodontics, the chosen age range for the study sample was set between 18 and 40 years. Furthermore, the position of the RMF tends to vary in younger patients due to ongoing growth and remodeling processes. As a result, individuals within this age group were excluded from the sample.
The study aimed to achieve the following objectives:
To identify and compare the occurrence (presence or absence) of the retromolar fossa among individuals aged 18–40 years, considering both males and females, through the utilization of CBCT.
To study the laterality of the RMF (unilateral or bilateral)
To evaluate the number of foramina on each side
To establish the relationship between the RMF and the OP.
The primary source of CBCT images was the archives of the Oral Medicine and Radiology Department of a dental faculty, encompassing the past 5 years. To obtain the final sample, over 300 CBCT images were meticulously reviewed. The study protocol obtained the approval of the University’s Ethics Committee Review Board and was registered under the code EC2020/PG/21. These scans had been initially requested for procedures such as third molar extraction, minor surgeries, and diagnostic purposes. A few images were excluded due to factors such as low quality (motion blur) or the presence of significant metal artifacts. All the scans were generated by the same machine and utilized Carestream software (Carestream 9300). The settings employed were 6.3 mA, 90 kvp, a resolution of 300 microns, a full field of view (FOV) measuring 17 × 13.5 cm, and an exposure time of 11.30 s. Throughout the image acquisition process, the patient’s head was positioned in the natural head orientation.
The samples were selected based on specific inclusion and exclusion criteria. Inclusion criteria encompassed individuals aged 18–40 years and scans that encompassed a large FOV, ensuring the comprehensive coverage of the entire retromolar region on both sides of the mandible. The exclusion criteria comprised radiologic indications of bony injury or discontinuity, any prior surgical interventions (such as surgical defects resulting from procedures such as third molar extraction or sagittal split osteotomy), and the identification of apparent anomalies or pathologies within the retromolar region, except for the presence of an impacted third molar.
The determination of the sample size was conducted using G* Power 3.1.2 software. Considering input parameters of 95% power and an alpha error of 0.05, the minimal necessary sample size was calculated to be 136. Consequently, out of the initial 300 samples, 136 were ultimately chosen through a stringent selection process that adhered to the predefined inclusion and exclusion criteria.
The patient’s identification number, age, and sex were documented. Subsequently, each CBCT image underwent reconstruction and orientation using CS 3D CBCT software (Carestream Dental LLC, Atlanta). All sections of the CBCT images – axial, coronal, and sagittal – were meticulously assessed to ascertain the presence of the RMF. Data were systematically recorded as either 1 to denote presence or 0 to signify absence [Figure 3]. For instances of unilateral RMF presence, it was denoted by “U,” whereas bilateral presence was indicated as “B” [Figure 4]. The quantity of RMF on each side was also methodically noted. If there were two RMFs on the right side, it was recorded as “R2.”

- 3D cone-beam computed tomography image showing the presence of RMF (orange circle). RMF: Retromolar formamen.
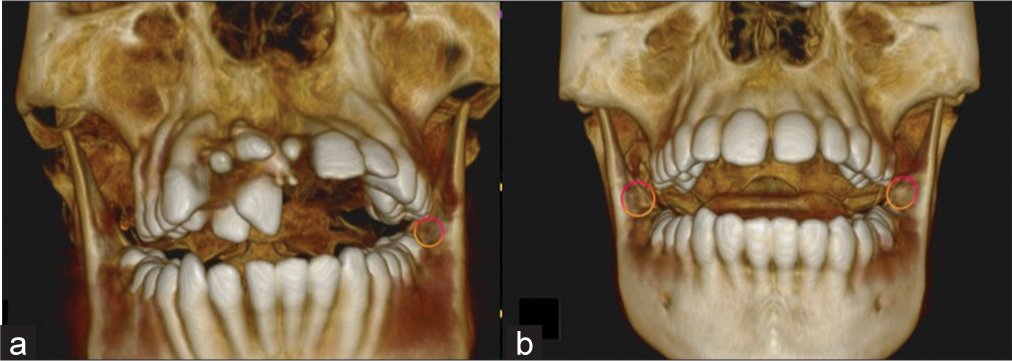
- Evaluation of 3D cone-beam computed tomography image showing (a) unilateral and (b) bilateral presence of RMF. (RMF: Retromolar formamen)
Subsequently, the coronal view of the samples that exhibited the presence of RMF was singled out. For the marking of the RMF, the nerve canal marking tool was employed, as shown in [Figure 5]. Following this, the chosen CBCT images underwent orientation to the sagittal view. The construction of the OP on the CBCT model was achieved by passing the axial plane (depicted as a yellow line) through the occlusal contact points of the first molars and first premolars, as shown in [Figure 6]. The measurement and recording of the shortest linear distance between the RMF and the OP ensued. In scenarios where two or more RMFs were identified, the measurement utilized the largest RMF. Notably, a positive value was attributed if the RMF was situated above the OP, while a negative value was recorded for instances where it lay below the OP.
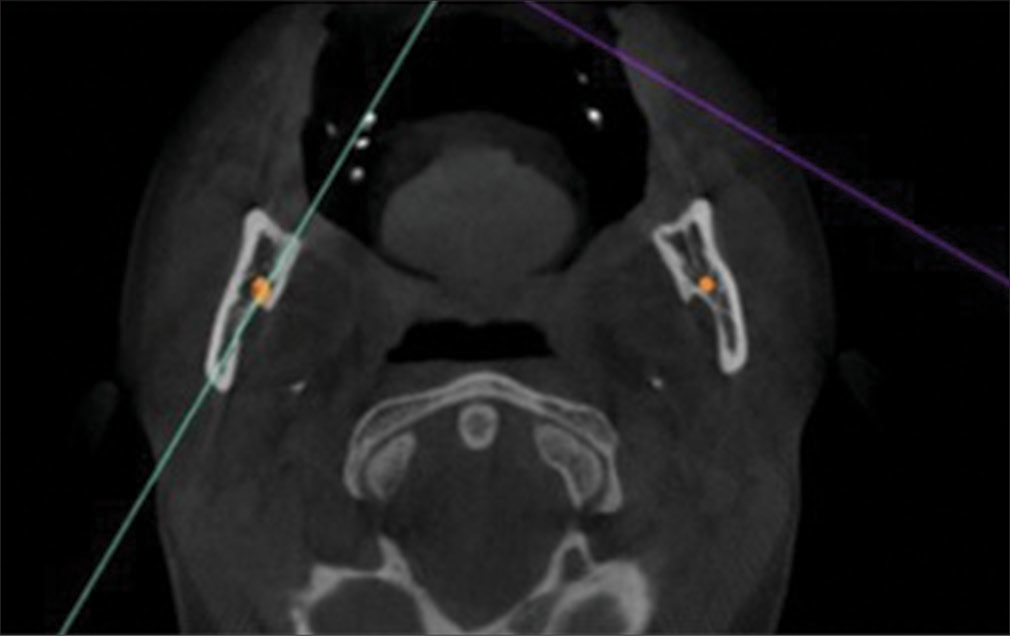
- Orientation of cone-beam computed tomography image in the coronal view and marking of the RMF using nerve tool. (RMF: Retromolar formamen)
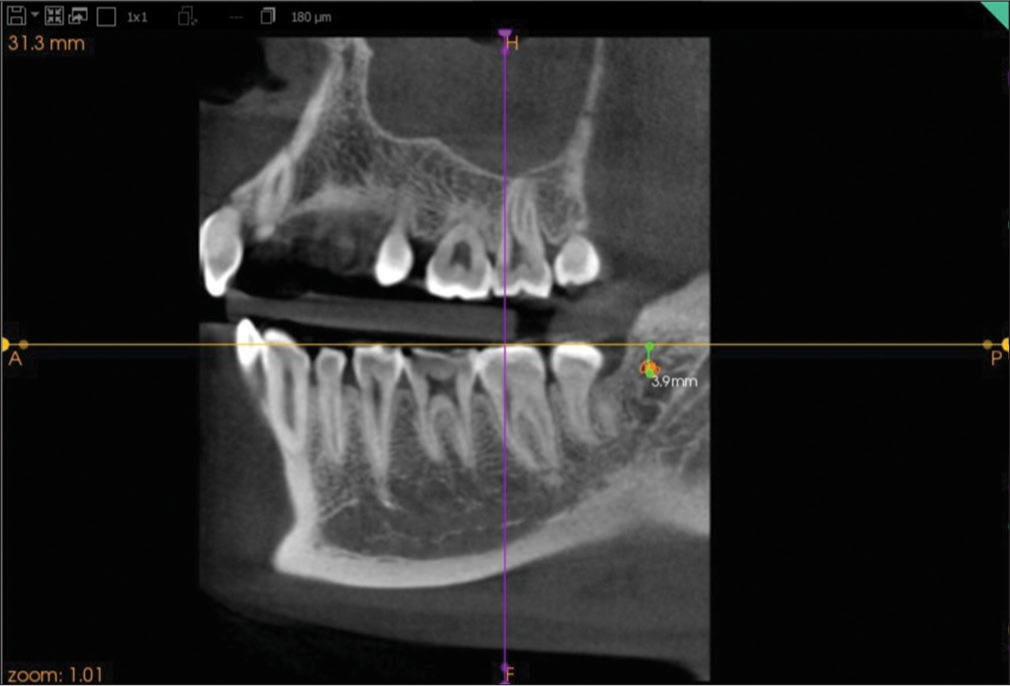
- Linear distance of retromolar foramen from the occlusal plane.
The collected data were meticulously entered into a Microsoft Excel spreadsheet and subsequently subjected to analysis utilizing Statistical Package for the Social Sciences (SPSS) software (IBM SPSS Statistics, Version 20.0, Armonk, NY: IBM Corp.). To succinctly summarize and present the data, descriptive statistics were employed. The normality of the data distribution was assessed using the Shapiro–Wilk test. The significance level was established at 5%. A comparison between the mean distance from the occlusal plane on the right side and the mean distance from the OP on the left side was executed through one-way analysis of variance (ANOVA). To assess the difference in the distribution of the RMF between males and females, the Chi-square test was employed.
The findings were recorded by two skilled orthodontists who were calibrated for the study. Each observer independently performed the measurements. Following 1 week, the measurements were repeated. The interobserver agreement was evaluated employing Kappa statistics, and the calculated Kappa coefficient stood at 0.9. This robust value indicated a high level of agreement between the observers.
RESULTS
[Table 1] illustrates the categorization of study subjects according to their age. The average age within the study sample was 27.14 ± 6.7 years, and there existed no statistically significant disparity between the mean ages of males and females. The comprehensive study population comprised 71 males and 65 females. The distribution of males and females within the study showcased no statistically significant variance, as shown in [Table 1].
| Gender | Age | |
|---|---|---|
| Mean | Std. Deviation | |
| Male | 25.80 | 6.69 |
| Female | 28.61 | 6.57 |
| Overall | 27.14 | 6.76 |
| Independent t-test value | 0.66 | |
| P–value | 0.41 | |
[Table 2] provides an overview of the general occurrence of the RMF as well as a comparison of its prevalence across genders. No notable significant variations were observed in the RMF prevalence between the two sexes. On the whole, out of the 136 samples examined, the presence of RMF was identified in 39% (53 samples) of the total. This substantial prevalence underscores the significance of regular assessment during clinical procedures such as implant placement. [Table 3] delineates the comparison of RMF prevalence based on lateralization (unilateral/bilateral) and gender. A statistically significant contrast was noted concerning the laterality of RMF, indicating P = 0.01. The prevalence of unilateral RMF was found to be higher than that of bilateral RMF.
| Prevalence of retromolar foramen (n=136) |
Gender | ||
|---|---|---|---|
| Male n(%) | Female n(%) | Total n(%) | |
| Absent | 43 (31.6) | 40 (29.4) | 83 (61.0) |
| Present | 28 (20.6) | 25 (18.4) | 53 (39.0) |
| Chi-square test value | 0.014 | ||
| P–value | 0.90 | ||
| Prevalence of retromolar foramen based on side (n=136) |
Gender | ||
|---|---|---|---|
| Male n(%) | Female n(%) | Total n(%) | |
| Absent | 43 (31.6) | 40 (29.4) | 83 (61.0) |
| Unilateral | 28 (20.6) | 18 (13.2) | 46 (33.8) |
| Bilateral | 0 (0) | 7 (5.2) | 7 (5.2) |
| Chi-square test value | 0.03 | ||
| P-value | 0.01** | ||
[Table 4] presents a comparison of the RMF prevalence based on its lateralization. In instances with bilateral RMF presence, both sides displayed a similar number of foramina. However, in cases featuring unilateral RMF presence, a notably higher count of RMFs was observed on the left side. [Table 5] outlines the comparison of the mean distance of the RMF from the OP utilizing one-way ANOVA. The calculated mean distance of the RMF above the OP stood at 5.99 mm, while that below the OP was 3.82 mm. Notably, the prevalence of RMF situated above the OP exhibited a statistically significant elevation in comparison to its counterpart positioned below the OP.
| Prevalence of retromolar foramen (n=136) |
Right side | Left side | ||||
|---|---|---|---|---|---|---|
| Absent n(%) | Present n(%) | Total n(%) | Absent n(%) | Present n(%) | Total n(%) | |
| Absent | 83 (61.0) | 0 | 83 (61.0) | 83 (61.0) | 0 | 83 (61.0) |
| Unilateral | 28 (20.6) | 18 (13.2) | 46 (33.8) | 18 (13.2) | 28 (20.6) | 46 (33.8) |
| Bilateral | 0 | 7 (5.1) | 7 (5) | 0 | 7 (5.1) | 7 (5) |
| Chi-square test value | 62.97 | 78.67 | ||||
| P-value | 0.001** | 0.001** | ||||
| Variable | Categories | n | Mean | Std. Deviation | One-way ANOVA | P-value |
|---|---|---|---|---|---|---|
| Distance from OP | At the OP | 3 | 0.00 | 0.00 | ||
| Above (+ve value) | 40 | 5.99 | 4.03 | 4.66 | 0.014 | |
| Below (-ve value) | 10 | -3.82 | 2.09 |
OP: Occlusal plane, ANOVA: Analysis of variance
DISCUSSION
Approximately a century following the initiation of tooth-borne anchorage in orthodontic treatment, temporary skeletal anchorage devices have emerged as a significant development.[4] Undertaking distalization of mandibular molars has historically proven to be more challenging than similar procedures involving maxillary molars. Where conventional mechanotherapy presented limited solutions, the introduction of orthodontic miniplates has effectively resolved the hindrances associated with distalizing mandibular molars.[14] In contrast to mini screws, the application of miniplates involves a higher level of invasiveness, underscoring the necessity for a comprehensive understanding of local anatomy.
Kook et al. strategically positioned miniplates within the retromolar fossa, a region situated between the anterior border of the mandibular ramus and the temporal crest.[2] They demonstrated that these plates enabled force application parallel to the functional OP and could effectively endure substantial forces. This approach proved advantageous and effective in scenarios like Class III cases with open bite, where complete arch distalization of the mandible was required.[2] The retromolar fossa, located posterior to the third mandibular tooth assumes a triangular shape. Within this area, the RMF occasionally manifests as an anatomical feature on the alveolar surface. Serving as the termination point of the RMC, this foramen is noteworthy due to its role in transmitting the neurovascular bundle. Given the significance of this canal’s anatomy and its variations, particularly in surgical mandibular procedures such as miniplate placement, its understanding remains crucial.[12]
Numerous studies have sought to assess the prevalence of the RMF. In one study involving 222 dry human mandibles from adult Brazilians, irrespective of gender, researchers found that it appeared unilaterally in 18.47% of cases (41 mandibles) and bilaterally in 12.16% of cases (18 mandibles).[6] A study on the American population identified the RMF in 18 out of 234 adult human mandibles, resulting in a prevalence rate of 7.7%.[15] In another investigation involving a Turkish population, 126 adult human mandibles were examined, revealing the presence of the RMF in 14 samples, indicating a prevalence rate of 11.1%.[16] Several dry bone studies have also documented the prevalence of the RMF. In one such study, which examined 71 dry mandibles and ten cadaveric specimens, researchers found the RMF in ten of the samples, with a prevalence rate of 14.1%.[13]
A recent study involving 80 CBCT scans of the mandible discovered that the prevalence of both RMF and RMC was 2.5% in males and 1.2% in females.[17] The reported frequency of RMF in CBCT studies varies widely, ranging from 5.4% to 75.4%, while human dry mandible studies have reported frequencies ranging from 3.2% to 72%.[8] This substantial variation can be attributed to numerous factors, including ethnic disparities, environmental and genetic influences, and differences in sample sizes among studies. Given the high prevalence found across various studies, it can be concluded that RMFs and RMCs are normal anatomical variations of the IAN rather than anomalies.[8]
Although several studies have concluded that CBCT imaging technology is the most valuable and accurate method for visualizing retromolar foramina and canals, there is no established protocol for determining the appropriate indications for utilizing CBCT in evaluating this area.[8] It is widely believed that panoramic radiography alone is insufficient for identifying the RMF, and its use is likely to lead to an underestimation of these structures.[18] Therefore, in this study, we employed CBCT to assess the area. CBCT enables antemortem evaluation in living subjects, with results that compare favorably to postmortem studies on cadavers and CBCT.[12]
According to Ossenberg, the highest incidence of RMF occurs in the adolescent age group. This reflects the increased neurovascular requirements in adolescents due to growth spurts and the eruption of third molars.[19] For our study, we selected samples within the age range of 18–40 years to best represent individuals who might undergo orthodontic anchorage procedures involving miniplates. The mean age of the sample was 27.14 ± 6.7 years [Table 1]. This study comprised 136 CBCT scans of the mandible, including 71 males (with a mean age of 25.80 ± 6.69 years) and 65 females (with a mean age of 28.61 ± 6.57 years). There was no statistically significant difference in the mean age between males and females in the study sample [Table 1].
[Table 2] depicts the prevalence of the RMF and its gender predilection. In this study, the prevalence of RMF was found to be 39% (53 out of 136). In the Brazilian population, the incidence was found to be 26.58%.[6] Ossenberg examined mandibles of different locations and found that the incidence of RMF in Italy was 8.1%, in Japan 3.2%, Eskimos had 8.2% incidence, and Canadians had 9.1%.[20] The incidence of RMF was found to be 22% in the Iranian population; thus, it should be considered as a normal anatomical variation rather than a rare finding.[21]
The prevalence reported in the South Asian (specifically Indian) population varies from 12 to 22%.[12] Akhtar et al. reported that the prevalence of RMF in 224 mandibles was 14.7%.[20] The higher prevalence observed in the present study (39%) could be due to the larger sample size and the use of CBCT to assess the samples. Another study that used CBCT to study the RMC and RMF found that the RMC was present in 16 of the 80 scans (20%). They also found that the two sides of the mandible are not identical as far as the prevalence of RMC is concerned.[17]
This study found no significant differences in the prevalence of RMF between the two sexes, which was similar to the results of earlier studies.[7] However, a study conducted on dried adult human mandibles found that the percentage of occurrence of RMF was higher in females as compared to males.[20]
The present study found that there was a higher prevalence of unilateral RMF than bilateral RMF with P = 0.01 [Table 3]. In another study, the RMF was present unilaterally in 41 mandibles and bilaterally in 18 mandibles, with prevalence of 18.47% and 12.16%, respectively.[6] In the present study, in cases with bilateral RMF, both sides had a similar number of foramen. However, in cases with the unilateral presence of RMF, there was a significantly higher number of RMF present on the left side [Table 4]. In a different study, the prevalence of RMF on the right side was higher than on the left, but the result was not statistically significant.[22]
Most studies have evaluated only the prevalence of RMF and not its position.[6,17,22] There are limited studies carried out to assess the relation of RMF in relation to the OP. One study, which investigated the position of the RMF, found that the RMF was present in the retromolar fossa above the OP and below the coronoid process of the ramus.[23] Studies have also assessed the distance from the RMF to the second molar.[7] However, from an orthodontic perspective, understanding the relationship between RMF and the OP is crucial. Miniplates are typically positioned in a manner that aligns the direction of force with the OP, making this parameter of great importance. Surprisingly, it had not been thoroughly investigated until this study. Our research revealed that the mean distance of RMF above the OP was 5.99 mm, while the mean distance below the OP was 3.82 mm [Table 5]. Importantly, there was a significantly higher prevalence of RMF located above the OP than below it.
The clinical significance of this data underscores the importance of approaching this area with caution during the routine placement of implants. Failure to identify anatomical variants such as the RMC and RMF can lead to trauma during intraoral procedures, such as third molar extraction, sagittal split ramus osteotomy, or miniplate insertion. Common complications that may arise from such trauma include paresthesia, traumatic neuroma, bleeding, or hematoma.[8] Accurate examination using CBCT is recommended.[24]
CONCLUSION
The presence of RMF was detected in 39% of the total sample. No significant differences in RMF prevalence were observed between the two sexes. Unilateral RMF was prevalent in 33.8% of cases, significantly exceeding the occurrence of bilateral RMF. Among cases with unilateral RMF, there was a notably higher occurrence on the left side (20.6%) compared to the right side (13.2%). In addition, the prevalence of RMF located above the OP was significantly greater than those below it. The mean distance of RMF situated above the OP was 5.99 mm, whereas below the OP, it measured 3.82 mm. This substantial prevalence (39%) of RMF underscores the importance of a thorough evaluation of the retromolar fossa region before placing mini-plates.
Ethical approval
The research/study approved by the Institutional Review Board at Faculty of Dental Sciences, MSRUAS, number EC2020/PG/21, dated 10th June 2020.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship: Nil.
References
- Soft tissue changes after mandibular setback and bimaxillary surgery in Class III patients. Angle Orthod. 2013;83:817-23.
- [CrossRef] [PubMed] [Google Scholar]
- Distalization of the mandibular dentition with a ramal plate for skeletal Class III malocclusion correction. Am J Orthod Dentofacial Orthop. 2016;150:364-77.
- [CrossRef] [PubMed] [Google Scholar]
- Primary failure rate for 1680 extra-alveolar mandibular buccal shelf mini-screws placed in movable mucosa or attached gingiva. Angle Orthod. 2015;85:905-10.
- [CrossRef] [PubMed] [Google Scholar]
- Temporary skeletal anchorage devices: The case for miniplates. Am J Orthod Dentofacial Orthop. 2014;145:559-65.
- [CrossRef] [PubMed] [Google Scholar]
- Minibone plates: The skeletal anchorage system. Semin Orthod. 2005;11:47-56.
- [CrossRef] [Google Scholar]
- Incidence of retromolar foramen in human mandibles: Ethnic and clinical aspects. Int J Morphol. 2012;30:1074-8.
- [CrossRef] [Google Scholar]
- Radiographic study of the mandibular retromolar canal: An anatomic structure with clinical importance. J Endod. 2011;37:1630-5.
- [CrossRef] [PubMed] [Google Scholar]
- Clinical anatomy and significance of the retromolar foramina and their canals: A literature review. Cureus. 2017;9:e1781.
- [CrossRef] [Google Scholar]
- The origin and distribution of the elements of the human mandibular retromolar canal. Arch Oral Biol. 1967;12:1261-8.
- [CrossRef] [PubMed] [Google Scholar]
- Cone beam CT findings of retromolar canals in a Korean population. Surg Radiol Anat. 2014;36:871-6.
- [CrossRef] [PubMed] [Google Scholar]
- Temporal crest canal: Case report and statistics on a rare mandibular variant. Oral Surg Oral Med Oral Pathol. 1986;62:10-2.
- [CrossRef] [PubMed] [Google Scholar]
- The retromolar foramen and canal in south Indian dry mandibles. Eur J Anat. 2002;6:141-6.
- [Google Scholar]
- Distal movement of mandibular molars in adult patients with the skeletal anchorage system. Am J Orthod Dentofacial Orthop. 2004;125:130-8.
- [CrossRef] [PubMed] [Google Scholar]
- Retromolar foramen: A mandibular variant important to dentistry. Ann Dent. 1991;50:16-8.
- [Google Scholar]
- Evaluation of perimandibular neurovascularization with accessory mental foramina using cone-beam computed tomography in children. J Craniofac Surg. 2013;24:e365-9.
- [CrossRef] [PubMed] [Google Scholar]
- Prevalence of retromolar canal and foramen: A cone beam computed tomography study. J Indian Acad Oral Med Radiol. 2018;30:216-22.
- [CrossRef] [Google Scholar]
- Descriptive study of the bifid mandibular canals and retromolar foramina: Cone beam CT vs panoramic radiography. Dentomaxillofac Radiol. 2014;43:20140090.
- [CrossRef] [PubMed] [Google Scholar]
- Retromolar foramen of the human mandible. Am J Phys Anthropol. 1987;73:119-28.
- [CrossRef] [PubMed] [Google Scholar]
- A morphological study of retromolar foramen and canal in Indian dried mandibles. J Evol Med Dent Sci. 2014;3:13142-51.
- [CrossRef] [Google Scholar]
- Incidence and anatomical properties of retromolar canal in an Iranian population: A cone-beam computed tomography study. Int J Dent. 2020;2020:9178973.
- [CrossRef] [PubMed] [Google Scholar]
- Occurrence of the retromolar foramen in dry mandibles of South-Eastern Part of India: A morphological study with review of the literature. Anat Res Int. 2014;2014:296717.
- [CrossRef] [PubMed] [Google Scholar]
- Prevalence and implications of accessory retromolar foramina in clinical dentistry. Gen Dent. 1999;47:500-3. quiz 504-5
- [Google Scholar]
- Mandibular retromolar foramen and canal-a systematic review and meta-analysis. Ann Maxillofac Surg. 2020;10:444-9.
- [CrossRef] [PubMed] [Google Scholar]




