

Translate this page into:
Anteroposterior relationship of the maxillary central incisors to the forehead in adult Chinese females

*Corresponding author: Peter Ngan, Department of Orthodontics, West Virginia University, Health Sciences Center North, Morgantown, United States. pngan@hsc.wvu.edu
-
Received: ,
Accepted: ,
How to cite this article: He H, Ngan P, Li M, Hua F, Zheng Z, Lei J, et al. Anteroposterior relationship of the maxillary central incisors to the forehead in adult Chinese females. APOS Trends Orthod 2022;12:277-83.
Abstract
Objectives:
The objectives of the study were to evaluate the anteroposterior (AP) relationship of the maxillary central incisors to the forehead in adult Chinese females.
Material and Methods:
The study sample consisted of 100 lateral smiling photographic images of adult Chinese females who were seeking orthodontic treatment (mean age = 24.0 + 6.5 years old). The study sample was compared to a control sample consisting of 100 images of adult Chinese females with harmonious facial profiles downloaded from the internet. The images were resized and rotated to the upright head position in an image editing software. Reference lines were constructed to evaluate forehead inclinations and AP positions of the maxillary central incisors.
Results:
In the control sample, 80% of the maxillary central incisors were positioned between the facial axis point of the forehead (FFA) and the glabella. About 13% were positioned posterior to the FFA point and 7% anterior to the glabella. In the study sample, 31% of the maxillary central incisors were positioned between the FFA point and glabella, 52% posterior to the FFA point, and 18% anterior to the glabella. There was a strong correlation between the position of the maxillary central incisors and forehead inclination in the control sample (r2 = 0.827). The difference in AP maxillary central incisor position relative to the forehead between the two groups was found to be statistically significant (P = 0.000).
Conclusion:
The forehead may be an important landmark when evaluating the AP position of maxillary incisors in adult Chinese female patients.
Keywords
Landmark
Forehead
Anteroposterior jaw relationship
Chinese female

INTRODUCTION
Evaluation of external facial soft tissues is an essential component of orthodontic diagnosis and treatment planning. In contemporary orthodontics, increasing emphasis is placed on improving facial esthetics.[1] The goals of orthodontic treatment have come to include functional occlusion as well as an esthetic facial profile.[2]
Numerous cephalometric analyses utilize internal osseous structures as landmarks for diagnosis. However, studies[3-5] indicate that relying solely on hard-tissue analysis is inadequate and may not yield the desired outcome. Tourne et al.[6] investigated the cephalometric variables for profile recognition and found that a combination of soft- and hard-tissue variables was most successful. However, the soft-tissue profile may not properly reflect underlying dental problems or changes to the skeletal structure that might occur during orthodontic treatment. It has been shown that subjects with good facial profiles do not necessarily present similar cephalometric values.[7] Studies also confirm a weak association between traditional cephalometric measurements and facial profile photographs.[8,9]
Andrews was the first to report on using the forehead as a landmark for determining the optimal anteroposterior (AP) position of the maxillary central incisors, and indirectly the maxilla, in White females.[10] This study was repeated in White males with similar findings.[11] Gidaly et al. reported that using the most anterior part of the forehead, or the Glabella vertical, was also a reliable landmark with which to access the AP maxillary incisal position in African-American females.[12] Schlosser et al.[13] investigated the effect of AP maxillary incisor movements on ratings of facial attractiveness and found that orthodontists and laypersons preferred the AP position of the maxillary incisor close to the Andrews Goal Anterior Limit Line (GALL), or “Element II,” position. Resnick et al.[14] reported that the Andrews analysis correlated well with the final esthetic sagittal maxillary position in a sample of orthognathic surgery patients, particularly for women, and could be a useful tool for planning orthognathic surgery. Other soft-tissue planes (STPs) have been proposed as landmarks for assessing the AP position of the maxillary incisors for improved facial esthetics. Alfaro[15] recommended that the AP position of the upper incisors should coincide with a plane passing through the soft-tissue nasion and perpendicular to the lower border of a photograph taken in NHP, which he termed the STP. Singh et al.[16] found that most young adults with good facial harmony had maxillary incisors positioned at or in front of a soft-tissue line dropping down from soft-tissue nasion (STP) and suggested that the STP line is a useful landmark in assessing the position of maxillary incisors in young adult patients seeking improved facial harmony. However, the use of the forehead to determine the AP position of the maxilla has not been studied in a Chinese sample. A recent study showed that both the labiolingual inclination and AP position of the maxillary incisors are essential in the aesthetics of the smiling profile in the Chinese population.[17] Miao et al. found that in Chinese Han males judged to have pleasing profiles, the sagittal position of the maxillary incisors was, on average, slightly (0.61) posterior to Andrews’ GALL line.[18]
The objective of this study is to determine the AP relationship of the maxillary central incisors to the forehead in a group of adult Chinese female patients seeking orthodontic treatment using adult Chinese females with attractive profiles as the control. These data may provide guidelines for evaluating the AP position of maxillary incisors in the orthodontic treatment planning of adult Chinese female patients.
MATERIAL AND METHODS
This study was approved by the Wuhan University School of Stomatology Institution Review Board (Protocol #2022B33).
Selection criteria
The study sample consisted of 100 lateral smiling facial profile photographs of adult Chinese females who were seeking orthodontic treatment at the Wuhan School of Stomatology Clinic. These patients were randomly selected based on the following criteria [Figure 1]:
Female patients over 18 years of age. No specific skeletal, dental, or facial characteristics were used as part of the inclusion criteria.
No history of orthodontic or orthognathic surgery treatment.
The maxillary central incisors and forehead were in full view in the photographs.

- Constructed landmarks and reference line with a patient in the study sample.
The mean age of the study sample was 24.0 + 6.5 years.
The control sample [Figure 2] consisted of 100 lateral smiling facial photographs of adult Chinese females with harmonious facial profiles. These images were downloaded from advertisements and entertainment news on the internet. These subjects were deemed to have attractive profile appearances by a panel of three orthodontic judges. These orthodontists were calibrated to select photographs of subjects with pleasing profiles. The subjects were selected if at least two of the three judges agreed on the decision.

- Constructed landmarks and reference lines with a patient in the control sample.
Landmark construction and measurements
All of the photographic images in both samples were imported into a PowerPoint file (Microsoft PowerPoint version 2010) then standardized in size and rotated “by eye” to an estimated upright head position. The average vertical distance between soft-tissue nasion (Ns point) and subnasale (Sn point) is 57 mm in Chinese females.[19] This mean distance of 57 mm was used to standardize the dimensions of the facial profile images used in the study sample.
[Figures 1 and 2] show the landmarks used in this study.[20] The definition of landmarks on the midsagittal plane of the head is described below: Trichion (when forehead contour is flat) or superion (when forehead contour is rounded or angular) is defined as the uppermost point of the forehead. Glabella is defined as the most inferior point of the forehead, which is located between the eyebrows. The forehead facial axis (FFA) point is defined as the midpoint between trichion and glabella (foreheads with flat contour) or that between superion and glabella (foreheads with rounded or angular contour). The maxillary central incisor’s FA point is defined as the occlusogingival midpoint of the facial axis of the clinical crown.[21] Four reference lines were constructed, among which three were vertical: Line 1 through the FFA point, line 2 through the glabella, and line 3 through the FA point of the maxillary central incisor. The fourth reference line (line 4) connected the glabella and the most superior point of the clinical forehead (superion or trichion). The angle between line 1 and line 4 represents the forehead inclination, while the distance between line 1 and line 3 represents the AP relationship of maxillary central incisors to the forehead. These landmarks and reference lines were constructed on each image in PowerPoint.
The photographs were then deleted from the PowerPoint slides, leaving only the reference lines and points. Each PowerPoint slide was then printed on white paper at standardized dimensions. One examiner was employed to measure all the linear and angular measurements on white paper, using a metric ruler and protractor. The angle between line 1 and line 4 was corrected to 0.5°, while the distance between line 1 and line 3 was corrected to 0.1 mm. The value was positive if line 3 was anterior to line 1 and vice versa.
Statistical analysis
Statistical Product and Service Solutions 18.0 was used to calculate the descriptive and comparative statistical analyses. The standard deviations (SD), means, and the ranges of forehead’s inclination and maxillary central incisors AP position relative to the forehead were calculated. An Independent two-tailed t-test was performed to compare the means of the control and study groups. Differences were regarded as statistically significant if P < 0.05. The correlation between maxillary central incisors and forehead inclination in both groups was analyzed using simple linear regression. Confidence intervals were set at 95%.
Error measurements
Ten subjects were randomly selected from both the study and control groups to be included in the error study. The measurements of these 20 subjects were repeated by the original examiner and by another examiner, respectively, 3 weeks apart. The error variance was calculated according to the Dahlberg formula (ME=√∑d22n/).
[Table 1] shows the error measurements using the Dahlberg formula.
| Intrarater reliability (same examiner) |
Inter-rater reliability (between two examiners) | |
|---|---|---|
| AP position of maxillary central | 0.29 | 0.43 |
| Forehead’s inclination | 0.48 | 0.59 |
AP: Anteroposterior
RESULTS
[Figures 3 and 4] illustrate the locations of the maxillary central incisors concerning the vertical reference lines in each sample. In the control group, there were 80 subjects (80%) whose maxillary central incisors were positioned between FFA point and glabella, 13 subjects (13%) whose maxillary central incisors were posterior to FFA point, and only 7 subjects (7%) anterior to glabella [Figure 3]. In the study group, just 30% of the subjects had maxillary central incisors positioned between the FFA point and glabella. The proportions of maxillary central incisors that were posterior to FFA point and anterior to glabella were 52% and 18%, respectively [Figure 4].

- Percentage of maxillary central incisors in the control sample that was behind FFA, between FFA and glabella, and in front of glabella. FFA: Forehead facial axis.
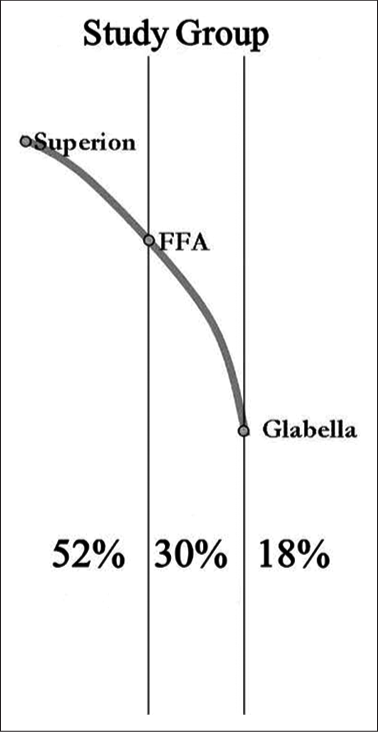
- Percentage of maxillary central incisors in the study sample that was behind FA, between FFA and glabella, and in front of glabella. FFA: Forehead facial axis.
In the control group, the AP position of the maxillary central incisors relative to the FFA point ranged from −3.6 mm to 11.4 mm. The mean and SD were 2.1 mm and 2.9 mm, respectively. In the study group, the AP position of the maxillary central incisors relative to the FFA point ranged from −9.3 mm to 11.4 mm. The mean and SD were −0.3 mm and 5.1 mm, respectively. Significant differences were found between the control group and the study group (P = 0.000) [Tables 2 and 3].
| (mm) | Mean | SD | Minimum | Maximum |
|---|---|---|---|---|
| Control group (n=100) | 2.1 | 2.9 | −3.6 | 11.4 |
| Study group (n=100) | −0.3 | 5.1 | −9.3 | 11.4 |
AP: Anteroposterior, FFA: Forehead facial axis
| Control | Study | P | |
|---|---|---|---|
| Position (mm) | 2.1 | −0.3 | 0 |
| Forehead inclination (°) | 16.7 | 16.2 | 0.355 |
In the control group, the range of the forehead’s inclination was from 8° to 27°. The mean and SD were 16.7° and 4.4°, respectively. In the study group, the range of the forehead’s inclination was from 7° to 28.5°. The mean and the SD were 16.2° and 4.1°, respectively. There was no significant difference between the control group and the study group (P = 0.355) [Tables 3 and 4].
| (°) | Mean | SD | Minimum | Maximum |
|---|---|---|---|---|
| Control group (n=100) | 16.7 | 4.4 | 8 | 27 |
| Study group (n=100) | 16.2 | 4.1 | 7 | 28.5 |
In the control group, the AP positions of the maxillary central incisors were strongly correlated with the forehead inclination (r2 = 0.827) [Figure 5], while that of the study group was poorly correlated (r2 = 0.291) [Figure 6]. An equation was obtained in the simple linear analysis in the control group, which showed that when the maxillary central incisors were positioned directly under the forehead’s FFA point, the forehead inclination was calculated to be 13.95°. For each degree, the forehead was inclined >13.95°, the incisors were correspondingly 0.74 mm more anterior to the forehead’s FFA point.

- Correlation between the position of maxillary central incisors and forehead inclination in the control sample (r2 = 0.827). The X-axis represented the AP position of the maxillary central incisors (mm) and the Y-axis represented the angle of the forehead inclination (°). AP: Anteroposterior.

- Correlation between the position of maxillary central incisors and forehead inclination in the study sample (r2 = 0.291). The X-axis represented the AP position of the maxillary central incisors (mm) and the Y-axis represented the angle of the forehead inclination (°). AP: Anteroposterior.
Table 5 indicates the subjects in each type of position of maxillary central incisors according to the Angle classification.
| Angle classification | Posterior to FFA point | At or between FFA point and glabella | Anterior to glabella |
|---|---|---|---|
| I | 23 | 7 | 3 |
| I1 | 11 | 7 | 10 |
| I2 | 11 | 6 | 2 |
| III | 9 | 10 | 1 |
FFA: Forehead facial axis
DISCUSSION
Significant differences were found between the study and control samples. Most (80%) of the adult Chinese females with attractive profiles in the control sample had maxillary central incisors positioned at or between the FFA point and glabella, compared with only 31% in the study sample. In addition, most (52%) of the adult Chinese females seeking orthodontic treatment had maxillary central incisors positioned posterior to the FFA point. In the control sample, the AP positions of maxillary central incisors were strongly correlated with forehead inclination. This suggests that the most preferred AP position of maxillary central incisors and the optimal AP position of the maxilla itself could be determined diagnostically. These findings are in agreement with those reported by Andrews[10] for adult White females and for adult White males reported by Adams et al.[11] In addition, the average location of the maxillary central incisors in the control group was 2.1 mm anterior to the FFA point, which was similar to that of adult White females (2.5 mm) and males (3.2 mm). In contrast, the maxillary central incisors were positioned 0.3 mm posterior to the FFA point, compared to 1.2 mm posterior in adult white females and 0.3 mm posterior in adult White males, respectively.
There was no significant difference found in forehead inclination between the study group and the control group. This is similar to those reported by Andrews[10] in adult White females. However, a few differences were found between the adult Chinese and White males and females. When the maxillary central incisors were positioned directly under the FFA point, the forehead angulation was, on average, 13.95° in adult Chinese females, whereas in adult White females, it was 7.5° and 16.21° in adult White males. These discrepancies may be due to ethnic differences. The previous studies[22-24] have indicated that the soft-tissue profile characteristics of Chinese were different from those of Caucasians, showing that the Chinese dentition demonstrates greater bimaxillary alveolar protrusion and incisal labial inclination. In addition, the Chinese soft-tissue profile shows a less obtuse nasolabial angle and more protrusive lips.
The prominence and contour of the forehead have an essential effect on profile appearance and it is necessary to evaluate the whole face, including the forehead, in a facial evaluation.[25] In Andrews Six Elements of Orthodontic Philosophy,[19] there are three defined forehead shapes: Flat, round, and angulated. In this study, the percentage of round and angulated forehead is 43% and 37.5%, respectively, while that of straight contour profile is only 19.5%. Further studies are needed to compare the frequency of occurrence of different forehead shapes among and between White females and Chinese females to shed light on any differences between these two ethnic groups. Apart from forehead contour, the discrepancy may also be ascribed to the distinct esthetic sense of the mass media between Chinese and White people.
The correlation between the AP positions of maxillary central incisors and forehead inclination in adult Chinese females was strong (r2 = 0.827), and even greater than that of the adult White females (r2 = 0.642) and adult White males (r2 = 0.53). For every degree, the forehead was canted more than 13.95°, and the AP positions of maxillary central incisors were located 0.74 mm more anterior relative to the FFA point, compared to 0.5 mm in adult White females. Gidaly et al.[12] found maxillary incisors to be consistently anterior to glabella in adult African-American females with attractive profiles but still strongly correlated with forehead inclination, as in the present study.
The concept of using a visual treatment objective (VTO) has been advocated as a helpful aid in diagnosis and treatment planning.[26] VTO can be used to estimate and illustrate planned tooth and/or jaw movements and their impact on the facial profile. The results of this study could be used as a form of VTO, in that it represents a template for the optimal AP position of maxillary central incisors. The use of a frontal (vertical) plane passing through the FFA point (Andrews’ Forehead Anterior Limit Line) along with the forehead’s inclination to predict the optimal position of the maxillary central incisors can be used to graphically display the most esthetic AP position of the maxillary incisors and possibly the maxilla itself.
CONCLUSION
About 80% of the Chinese female adults with pleasing facial esthetics had maxillary central incisors positioned between the FFA point and glabella. By contrast, only 30% of Chinese female adults seeking orthodontic treatment had maxillary central incisors positioned between the FFA point and glabella.
The AP position of maxillary central incisors was strongly correlated with forehead inclination in adult Chinese females with harmonious profiles. For each degree, the forehead was inclined greater than 13.95°, the incisors were correspondingly 0.74 mm more anterior to the forehead’s FFA point.
When evaluating the facial profile of adult Chinese females and assessing the AP position of the maxillary central incisors, the forehead is a useful and important landmark.
Declaration of patient consent
Patients’ consent not required as patients’ identity is not disclosed or compromised.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Smile esthetics: Perception and comparison of treated and untreated smiles. Am J Orthod Dentofacial Orthop. 2006;129:8-16.
- [CrossRef] [PubMed] [Google Scholar]
- Diagnosis and treatment planning in orthodontics. Am J Orthod Oral Surg. 1946;32:68-87.
- [CrossRef] [PubMed] [Google Scholar]
- Cephalometric soft tissue facial analysis. Am J Orthod Dentofacial Orthop. 1999;116:373-89.
- [CrossRef] [PubMed] [Google Scholar]
- A soft-tissue cephalometric analysis and its use in orthodontic treatment planning. Part I. Am J Orthod. 1983;84:1-28.
- [CrossRef] [PubMed] [Google Scholar]
- Facial keys to orthodontic diagnosis and treatment planning. Part I. Am J Orthod Dentofacial Orthop. 1993;103:299-312.
- [CrossRef] [PubMed] [Google Scholar]
- A validity test of cephalometric variables as a measure of clinical applicability in anteroposterior profile assessment. Int J Adult Orthodon Orthognath Surg. 1993;8:95-112.
- [Google Scholar]
- Facial harmony in orthodontic diagnosis and planning. Braz Oral Res. 2010;24:52-7.
- [CrossRef] [PubMed] [Google Scholar]
- Soft tissue adaptability to hard tissues in facial profiles. Am J Orthod Dentofacial Orthop. 1998;113:674-84.
- [CrossRef] [PubMed] [Google Scholar]
- Correlations between cephalometric and photographic measurements of facial attractiveness in Chinese and US patients after orthodontic treatment. Am J Orthod Dentofacial Orthop. 2009;136:762.e1-14. discussion 762-3
- [CrossRef] [PubMed] [Google Scholar]
- AP relationship of the maxillary central incisors to the forehead in adult white females. Angle Orthod. 2008;78:662-9.
- [CrossRef] [PubMed] [Google Scholar]
- Anteroposterior relationship of the maxillary central incisors to the forehead in adult white males. Orthodontics (Chic). 2013;14:e2-9.
- [CrossRef] [PubMed] [Google Scholar]
- Optimal anteroposterior position of the maxillary central incisors and its relationship to the forehead in adult African American females. Angle Orthod. 2019;89:123-8.
- [CrossRef] [PubMed] [Google Scholar]
- The effects of computer-aided anteroposterior maxillary incisor movement on ratings of facial attractiveness. Am J Orthod Dentofacial Orthop. 2005;127:17-24.
- [CrossRef] [PubMed] [Google Scholar]
- Evaluation of Andrews' analysis as a predictor of ideal sagittal maxillary positioning in orthognathic surgery. J Oral Maxillofac Surg. 2018;76:2169-76.
- [CrossRef] [PubMed] [Google Scholar]
- Upper incisor to Soft Tissue Plane (UISTP): A new reference for diagnosis and planning in dentofacial deformities. Med Oral Patol Oral Cir Bucal. 2010;15:e779-81.
- [CrossRef] [PubMed] [Google Scholar]
- Evaluation of anteroposterior relationship of maxillary central incisors to a soft tissue plane in profile analysis. J Indian Ortho Soc. 2014;48:180-3.
- [CrossRef] [Google Scholar]
- Effect of maxillary incisor labiolingual inclination and anteroposterior position on smiling profile esthetics. Angle Orthod. 2011;81:121-29.
- [CrossRef] [PubMed] [Google Scholar]
- Cone beam computed tomography imaging of sagittal positions of the mandibular prominence and maxillary central incisors in adult Chinese Han men as an aesthetic profile determinant. Medicine (Baltimore). 2020;99:e22778.
- [CrossRef] [PubMed] [Google Scholar]
- Cephalometric analysis of soft tissue profile for adults of Beijing with normal occlusion in the 1990s. Beijing Kou Qing Yi Xue Za Zhi. 2001;9:172-5.
- [Google Scholar]
- Syllabus of the Andrews Orthodontic Philosophy (8th ed). San Diego, California: Lawrence F. Andrews; 1999.
- [Google Scholar]
- The six keys to normal occlusion. Am J Orthod. 1972;62:296-309.
- [CrossRef] [PubMed] [Google Scholar]
- Racial variation of cephalometric measurements in Hawaii. J Craniofac Genet Dev Biol. 1982;2:99-106.
- [Google Scholar]
- Soft-tissue cephalometric norms in Chinese adults with esthetic facial profiles. J Oral Maxillofac Surg. 1992;50:1184-9.
- [CrossRef] [PubMed] [Google Scholar]
- Cephalometric norms for the Chinese: A compilation of existing data. Aust Orthod J. 2002;18:19-26.
- [Google Scholar]
- The effects of forehead and neck positions on profile esthetics. Eur J Esthet Dent. 2012;7:454-66.
- [Google Scholar]
- The dental VTO: An analysis of orthodontic tooth movement. J Clin Orthod. 1999;33:394-403.
- [Google Scholar]




