

Translate this page into:
Assessing orthodontic treatment need in virtual consultations: A comparative analysis of photographic evaluations and clinical grading


*Corresponding author: Yuxuan Low, Department of Orthodontics, National Dental Centre of Singapore, Singapore, Singapore. low.yuxuan@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Low Y, Song Y, Yow M, Wong H, Tan EL. Assessing orthodontic treatment need in virtual consultations: A comparative analysis of photographic evaluations and clinical grading. APOS Trends Orthod. doi: 10.25259/APOS_222_2024
Abstract
Objectives
The increased use of virtual orthodontic consultations through photographic assessments prompts a need for rigorous evaluation to determine the accuracy and reliability compared to actual orthodontic treatment requirements. This study aimed to establish the consistency of orthodontic treatment need assessments from photographs, comparing evaluations between dental professionals and laypeople and the index of orthodontic treatment need dental health component (IOTN DHC) grading of study models within the same patient cohort.
Material and Methods
A retrospective analysis was conducted using intraoral photographs and digital study models selected from 50 orthodontic patients from a national dental center’s records archive, representing specific occlusal traits. Twenty-four assessors were categorized into orthodontists, general dentists, non-orthodontic specialists, orthodontic residents, and laypeople. Intergroup evaluations of treatment needs based on photographs were compared with the IOTN DHC grade of digital study models, employing Kappa statistics and percentage agreement for analysis.
Results
Agreement between photographic assessments and IOTN DHC grades varied from fair to substantial. Orthodontists, orthodontic residents, and general dentists exhibited higher agreement (k = 0.339–0.655) for photographic assessments in comparison to non-orthodontic specialists and laypeople (k = 0.075–0.468) against the IOTN DHC grade. Across all groups, agreement was substantial for photographs depicting crowding (k = 0.493–0.602) and low for spacing (k = −0.039–0.237). Spacing was perceived to require higher treatment intervention than indicated by IOTN DHC across all groups. Orthodontists and general dentists perceived reverse overjet, posterior crossbite, and lateral open bite photographs to necessitate higher treatment intervention compared to laypeople.
Conclusion
Photographic assessments of orthodontic treatment needs showed varying agreement with IOTN DHC grades, with dental professionals demonstrating higher consistency. Agreement was highest for crowding but lower for spacing, reverse overjet, posterior crossbite, and lateral open bite. These findings emphasize the need for improved patient-clinician communication and technological advancements to enhance virtual orthodontic assessments.
Keywords
Orthodontists
Treatment need
Malocclusion
Photographs
Digital study models

INTRODUCTION
Malocclusion prompts individuals to seek orthodontic treatment. Indices, such as the dental esthetic index;[1] index of orthodontic treatment need (IOTN);[2] and index of complexity, outcome, and need,[3] are employed to assess malocclusion severity and need for intervention. Despite their objective intent, indices have inherent limitations. The inclusion, weighting, and establishment of cut-off points for treatment needs are subjective, relying on the perspectives of expert orthodontists who designed the indices. Variations in methodologies and opinions[4] affect its overall accuracy and applicability across different cultures and countries.[5,6] Other reported limitations include inconsistent terminology,[7] lack of or inappropriate weightings, and failure to include certain occlusal traits.[8]
While clinicians play a pivotal role in determining treatment needs, consideration of the patient’s perception of malocclusion is equally crucial, which encompasses perceptual, functional, and social dimensions.[9] However, discrepancies exist between normative orthodontic treatment needs assessed through indices and self-perceived treatment needs reported by patients.[8,10] Existing indices prioritize the clinician’s perspective and have complex scoring procedures, in addition to the lack of uniformity in assessment tools used between participant groups. The majority of studies employ the IOTN esthetic component (AC) photographic scale for comparisons, which face limitations including the inadequate representation of anterior-posterior dentofacial imbalances,[11] and omission of certain malocclusions such as Class II division 2 incisor relationships and anterior open bites.[12]
Conventionally, orthodontic treatment planning relies on clinical assessments and study models. In the era of virtual consultations, intraoral photographs have emerged as a valuable tool in assessing malocclusion. Integrating photographs into orthodontic assessments offers simplicity and ease of interpretation, allowing different evaluators to visualize malocclusion features. Previous studies reported lower treatment need assessments using facial photographs for evaluation,[13-15] which may be attributed to the limitation of extraoral facial photographs to adequately visualize intraoral occlusal traits. In contrast, studies combining IOTN scores from plaster casts with extraoral and intraoral images demonstrated fair to substantial agreement.[13,16] However, these evaluations were conducted with orthodontists, overlooking the perspectives of other dental professionals and laypeople.
This study aims to evaluate the consistency of orthodontic treatment need assessments between dental professionals and laypeople using intraoral photographs and compare them with IOTN dental health component (DHC) grades of orthodontic study models. By highlighting the perceptual differences, this study explores the clinical implications and opportunities in orthodontic treatment planning, particularly in virtual consultation.
MATERIAL AND METHODS
Ethical approval for the study was obtained from the SingHealth Centralized Institutional Review Board (RC2018/3052).
The study population was recruited from the National Dental Centre Singapore. A power calculation based on the proposed method by Cicchetti[17] produced a minimal required sample size of 20 subjects. In total, 50 subjects representing a range of distinct malocclusion traits of varying severity were included in the study. The malocclusion traits were crowding, spacing, posterior crossbite, anterior crossbite, increased overjet, reverse overjet, anterior open bite, lateral open bite, and deep overbite [Figure 1]. All were in full permanent dentition. Data were retrospectively collected by means of intraoral photographs and digital study models. These were obtained as part of standard clinical procedures by trained clinicians and assistants before orthodontic treatment.
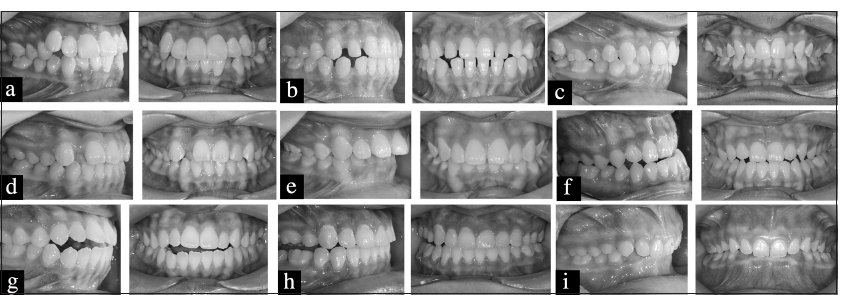
- Example of oral photographs with buccal and frontal views representing malocclusion traits of (a) crowding, (b) spacing, (c) posterior crossbite, (d) anterior crossbite, (e) increased overjet, (f) reverse overjet, (g) anterior open bite, (h) lateral open bite, and (i) deep overbite.
The IOTN DHC was used to assess orthodontic treatment needs and malocclusion traits. Each subject’s digital study model was examined using 3 Shape OrthoAnalyzer ™ (3Shape, Copenhagen, Denmark) software by an investigator (L.Y) who underwent calibration with an experienced orthodontist trained in an occlusal index calibration course by Professor Stephen Richmond. The investigator recorded the most severe occlusal trait as the DHC score and corresponding treatment need grade. Detailed measurements for applicable trait specifications were recorded to the nearest 0.5 mm for each case. The DHC grade and measurements were repeated after a 15-day interval.
Intraoral photographs, featuring a frontal and a right buccal view, were assembled for each subject. The photographs were taken with the use of cheek retractors at maximum intercuspation before the start of orthodontic treatment. The images were converted from color to grayscale using PowerPoint software (Microsoft, Redmond, Wash) to eliminate color influence on treatment need assessments.
Twenty-four assessors, comprising orthodontists, orthodontic residents, non-orthodontic specialists, general dental practitioners, and laypeople, participated in the study. Assessors independently rated photographs of each subject on a scale of great, moderate, or no need for orthodontic treatment. Individual assessments were conducted in separate sessions without time constraints. Following a 4-week washout period, four assessors were randomly selected to repeat the evaluation for reliability testing.
Statistical analysis
Statistical analysis was conducted using SAS version 9.4 (SAS Institute, Cary, NC, USA) with a significance level set at 5%. Cohen’s Kappa statistics were employed to assess agreement for treatment needs between intraoral photographs and IOTN DHC grades, assessors, groups, and intra-rater reliability. The agreement was evaluated for the entire set of 50 cases and after categorization into individual malocclusion traits. Fleiss’ Kappa statistics were used for intra-group agreement. Percentage agreement was calculated for cases without agreement with IOTN DHC grades. Kappa coefficients were evaluated using the guidelines outlined by Landis and Koch.[18]
RESULTS
Agreement between photographic assessments and IOTN DHC grade ranged from slight (k = 0.075) to substantial (k = 0.655) for dental professionals [Table 1] and laypeople [Table 2]. Fair agreement was observed among the majority of the assessors with IOTN DHC. The percentage agreement for photographic assessments with IOTN DHC grade varied from 40.0% to 78.0%. Orthodontists (k = 0.454), orthodontic residents (k = 0.450), and general dentists (k = 0.457) exhibited higher agreement in photographic assessments with IOTN DHC grade compared to laypeople (k = 0.309) and non-orthodontic specialists (k = 0.225).
| Dental professionals | Mean kappa (range) | P-value | % |
|---|---|---|---|
| Total | 0.353 (0.197–0.655) | ||
| Orthodontists | 0.454 (0.419–0.506) | ||
| Orthodontist 1 | 0.437 | <0.001 | 64.0 |
| Orthodontist 2 | 0.506 | <0.001 | 68.0 |
| Orthodontist 3 | 0.419 | <0.001 | 64.0 |
| Orthodontic residents | 0.450 (0.395–0.522) | ||
| Orthodontic resident 1 | 0.522 | <0.001 | 70.0 |
| Orthodontic resident 2 | 0.395 | <0.001 | 62.0 |
| Orthodontic resident 3 | 0.434 | <0.001 | 64.0 |
| Nonorthodontic specialists | 0.225 (0.197–0.251) | ||
| Nonorthodontic specialist 1 | 0.197 | 0.025 | 44.0 |
| Nonorthodontic specialist 2 | 0.251 | 0.010 | 50.0 |
| Nonorthodontic specialist 3 | 0.228 | 0.011 | 48.0 |
| General dentists | 0.457 (0.339–0.655) | ||
| General dentist 1 | 0.655 | <0.001 | 78.0 |
| General dentist 2 | 0.339 | <0.001 | 60.0 |
| General dentist 3 | 0.378 | <0.001 | 60.0 |
Strength of agreement for the kappa coefficient: 0: None, 0.01–0.20: Slight, 0.21–0.40: Fair, 0.41–0.60: Moderate, 0.61–0.80: Substantial, 0.81–1.00: Almost perfect agreement (Landis and Koch, 1977). IOTN: Index of orthodontic treatment need, DHC: Dental health component
| Laypeople | Mean kappa (range) | P-value | % |
|---|---|---|---|
| Total | 0.309 (0.075–0.468) | ||
| Layperson 1 | 0.075 | 0.454 | 40.0 |
| Layperson 2 | 0.123 | 0.230 | 62.0 |
| Layperson 3 | 0.432 | <0.001 | 62.0 |
| Layperson 4 | 0.262 | 0.008 | 52.0 |
| Layperson 5 | 0.468 | <0.001 | 66.0 |
| Layperson 6 | 0.318 | 0.001 | 54.0 |
| Layperson 7 | 0.426 | <0.001 | 62.0 |
| Layperson 8 | 0.442 | <0.001 | 50.0 |
| Layperson 9 | 0.251 | 0.010 | 50.0 |
| Layperson 10 | 0.315 | 0.001 | 54.0 |
| Layperson 11 | 0.429 | <0.001 | 62.0 |
| Layperson 12 | 0.177 | 0.086 | 48.0 |
Strength of agreement for the kappa coefficient: 0: None, 0.01–0.20: Slight, 0.21–0.40: Fair, 0.41–0.60: Moderate, 0.61–0.80: Substantial, 0.81–1.00: Almost perfect agreement (Landis and Koch, 1977).
IOTN: Index of orthodontic treatment need, DHC: Dental health component
Agreement between orthodontists and laypeople (k = 0.280) and general dentists and laypeople (k = 0.208) was fair.
Considerable variation in treatment need agreement was observed across all occlusal traits when comparing photographic assessments with IOTN DHC grade. High agreement was noted for crowding (k = 0.493–0.602) across all groups, whereas spacing (k = −0.039–0.237) and lateral open bite (k = 0.093–0.263) exhibited lower agreement [Table 3].
| Occlusal trait | Orthodontists (n=3) | General dentists (n=3) | Laypeople (n=12) | |||
|---|---|---|---|---|---|---|
| Mean kappa (range) | Mean kappa (range) | Mean kappa (range) | ||||
| Crowding | 0.517 | (0.276–0.741) | 0.602 | (0.533–0.741) | 0.493 | (−0.05–1.00) |
| Spacing | −0.039 | (−0.250–0.333) | 0.149 | (−0.125–0.571) | 0.237 | (−0.25–1.00) |
| Posterior crossbite | 0.515 | (0.00–1.00) | 0.333 | (0.00–1.00) | 0.347 | (−0.364–1.00) |
| Increased overjet | 0.286 | (0.286–0.286) | 0.651 | (0.286–1.00) | 0.041 | (−0.364–1.00) |
| Reverse overjet | 0.534 | (0.375–0.643) | 0.424 | (0.00–0.688) | 0.270 | (−0.071–0.444) |
| Anterior crossbite | 0.389 | (0.00–1.00) | 0.630 | (−0.111–1.00) | 0.138 | (−0.136–1.00) |
| Anterior open bite | 0.444 | (0.333–0.667) | 0.333 | (0.00–1.00) | 0.388 | (−0.063–0.688) |
| Lateral open bite | 0.263 | (−0.250–0.706) | 0.093 | (−0.25–0.412) | 0.134 | (−0.333–0.688) |
| Deep overbite | 0.438 | (0.063–1.00) | 0.444 | (−0.111–1.00) | 0.198 | (−0.25–0.688) |
Strength of agreement for the kappa coefficient: 0: None, 0.01–0.20: Slight, 0.21–0.40: Fair, 0.41–0.60: Moderate, 0.61–0.80: Substantial, 0.81–1.00: Almost perfect agreement (Landis and Koch, 1977). IOTN: Index of orthodontic treatment need, DHC: Dental health component
Crowding (71.0%) and posterior crossbite (78.9%) photographs had the highest agreement with IOTN DHC grades among all orthodontists, general dentists, and laypeople. For cases without agreement with IOTN DHC grades, all photographs depicting spacing were assessed as having higher treatment needs by orthodontists (61.0%) laypeople (48.5%), and the majority of general dentists (44.7%). In addition, a higher proportion of photographs featuring anterior open bite (32.2%) and deep overbite (37.8%) were rated with higher treatment needs than indicated by the IOTN DHC grade across all participant groups. In contrast, all photographs illustrating anterior crossbite were consistently assessed with lower treatment needs by orthodontists (33.3%), general dentists (26.7%), and laypeople (58.3%) than indicated by the IOTN DHC grade. Similarly, increased overjet photographs received lower treatment need ratings from orthodontists (26.7%), general dentists (26.7%), and laypeople (45.0%). Inter-group variability was found for reverse overjet, posterior crossbite, and lateral open bite. Orthodontists and general dentists assessed these malocclusion traits with higher treatment needs, whereas laypeople rated them with lower treatment needs [Table 4].
| Occlusal trait | Orthodontists (n=3) | General dentists (n=3) | Laypeople (n=12) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Higher (%) | Same (%) | Lower (%) | Higher (%) | Same (%) | Lower (%) | Higher (%) | Same (%) | Lower(%) | |
| Crowding | 9.5 | 71.4 | 19.0 | 19.0 | 76.2 | 4.8 | 8.3 | 65.5 | 26.2 |
| Spacing | 61.0 | 39.0 | 0.0 | 44.4 | 44.4 | 11.0 | 48.6 | 51.4 | 0.0 |
| Posterior crossbite | 6.7 | 86.7 | 6.7 | 13.3 | 86.7 | 0.0 | 1.7 | 63.3 | 35.0 |
| Increased overjet | 13.3 | 60.0 | 26.7 | 0.0 | 73.3 | 26.7 | 11.7 | 43.3 | 45.0 |
| Reverse overjet | 20.0 | 73.3 | 6.7 | 20.0 | 73.3 | 6.7 | 15.0 | 55.0 | 30.0 |
| Anterior crossbite | 0.0 | 66.7 | 33.3 | 0.0 | 73.3 | 26.7 | 0.0 | 41.7 | 58.3 |
| Anterior open bite | 33.3 | 66.7 | 0.0 | 40.0 | 60.0 | 0.0 | 23.3 | 60.0 | 16.7 |
| Lateral open bite | 26.7 | 53.3 | 20.0 | 53.3 | 40.0 | 6.7 | 13.3 | 46.7 | 40.0 |
| Deep overbite | 40.0 | 60.0 | 0.0 | 40.0 | 60.0 | 0.0 | 33.3 | 46.7 | 20.0 |
IOTN: Index of orthodontic treatment need, DHC: Dental health component
Intragroup agreement was moderate for orthodontic residents (k = 0.485) and fair for non-orthodontic dental specialists (k = 0.364), orthodontists (k = 0.354), and laypeople (k = 0.246). Intra-rater reliability ranged from moderate (k = 0.431) to substantial (k = 0.693) for four randomly selected participants. Intraexaminer reliability of scoring of the DHC of IOTN was substantial (k = 0.953).
DISCUSSION
The adoption of virtual orthodontic consultations has led to a deviation from traditional in-person clinical examinations. Clinical photography and photogrammetry are important tools for virtual treatment planning and follow-ups of various orthodontic treatment procedures. The reliance on intraoral photographs submitted through digital platforms necessitates an accurate interpretation of the type and severity of malocclusion from these images to determine and recommend appropriate treatment plans.
Our findings indicated that the agreement between orthodontic treatment needs assessed from intraoral photographs and IOTN DHC grades was found to be lower than that reported in studies comparing plaster casts and their digital images[13] or intraoral and extraoral photographs.[16] These studies were conducted with orthodontists, whose specialized expertise may have contributed to higher agreement levels. Consistent with this, our study observed higher agreement among orthodontists, orthodontic residents, and general dentists compared to non-orthodontic specialists and laypeople. This underscores the influence of professional background, education, and experience on the accuracy of photographic assessments of malocclusion.
Patient perceptions of malocclusion and orthodontic treatment needs are crucial for the acceptance and success of orthodontic treatment. We investigated the agreement among orthodontists, general dentists, and laypeople, given their higher levels of interaction in clinical settings. Laypeople were recruited by convenience sampling. Although sociodemographic characteristics were not controlled, gender,[19,20] ethnicity,[20,21] and history of orthodontic treatment[22] were not found to influence the perception of malocclusion and treatment need. Our study found lower agreement between orthodontists, general dentists, and laypersons than in previous studies, which may be attributed to differences in assessment tools. Previous studies used Visual Analog Scales by utilizing photographs from the AC of IOTN[9,12,23-25] or questionnaires on the patient’s own malocclusion[26-28] to measure laypeople’s perception of treatment needs against clinical examinations or IOTN DHC scores by dental professionals, whereas our study employed a standardized set of photographs across all assessors. This approach aimed to reduce variability and ensure a uniform basis for evaluation.
Disparities in the perception of individual occlusal traits were evident, consistent with existing literature.[29] Crowding exhibited the highest agreement with IOTN DHC grades, reflecting its visibility and significant esthetic and orthodontic implications. Conversely, spacing showed the lowest agreement across all groups and was perceived to require higher treatment intervention than indicated by IOTN DHC. This discrepancy suggests that the IOTN criteria which focus on dental health impact may not adequately reflect the concern[24,30] and the impact of spacings on quality of life.[31]
Further discrepancies were observed for reverse overjet, posterior crossbite, and lateral open bite. Orthodontists and general dentists rated these traits as requiring higher treatment intervention than indicated by IOTN DHC, whereas laypeople rated them as less severe. Previous studies have highlighted that orthodontists place greater emphasis on the esthetic impact of reverse overjet[32] and may categorize posterior open bite as a higher treatment priority than the IOTN DHC.[7] In addition, traits affecting posterior teeth, such as posterior crossbite and lateral open bite, are less visible,[33] and therefore, less concerning to laypeople.[34] This finding highlights the potential variations in photographic assessments of orthodontic treatment needs among different groups and the difference in perspective between the clinician and patient on the importance of correcting different types of malocclusions. While dental professionals can more accurately evaluate orthodontic treatment needs from photographs in alignment with IOTN DHC indications, they may prioritize the correction of certain malocclusions such as reverse overjet, posterior crossbite, and lateral open bite, which may not be what the patient wants or understands.
A disconnect between the goals of the patient and the clinician may lead to the patient being less cooperative, tired, and disinterested in the procedures, eventually resulting in patient burnout.[35] Effective communication between the clinician and patient is essential to understand the patient’s needs, align treatment plans with patient expectations, and achieve satisfactory outcomes.
The limitations of our study include the challenges of assessing malocclusion traits from photographs. The use of photographs displaying distinct occlusal traits may oversimplify the complex interplay of multiple traits and their impact on treatment needs. In addition, the position and angle of the camera may also lead to an underestimation of discrepancies, particular in the anterior-posterior dimension, and may render posterior malocclusions less visible. While two-dimensional photographic assessments have utility in virtual consultations, we acknowledge their limitations for posterior malocclusions and occlusal discrepancies. Future integration of advanced imaging technologies, such as three-dimensional imaging technology could enhance visualization and address these limitations, providing a more comprehensive assessment of orthodontic treatment needs.
CONCLUSION
Agreement for treatment needs based on photographic assessments compared to IOTN DHC grade ranged from slight to substantial, with higher agreement among orthodontists, orthodontic residents, and general dental practitioners.
Photographs of crowding demonstrated the highest agreement with IOTN DHC grades, while spacing showed the lowest agreement.
Orthodontists and general dentists assessed photographs of reverse overjet, posterior crossbite, and lateral open bite as requiring higher treatment intervention than laypeople.
This study explores the complexities of assessing orthodontic treatment needs using photographs in virtual consultations and emphasizes the importance of considering professional expertise and technological advances. Three-dimensional imaging may improve accuracy and bridge disparities in perception, refining virtual orthodontic assessments and ensuring optimal patient communication in the digital era.
Acknowledgment
This manuscript has not been published, simultaneously submitted or already accepted for publication elsewhere. All authors have contributed significantly, and all authors are in agreement with the content of the manuscript.
Ethical approval
The research/study was approved by the Institutional Review Board at SingHealth Centralized Institutional Review Board, number RC2018/3052, dated March 02, 2019.
Declaration of patient consent
Patient’s consent not required as patient identity is not disclosed or compromised.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship: Nil.
References
- The development of an index of orthodontic treatment priority. Eur J Orthod. 1989;11:309-20.
- [CrossRef] [PubMed] [Google Scholar]
- The development of the index of complexity, outcome and need (ICON) J Orthod. 2000;27:149-62.
- [CrossRef] [PubMed] [Google Scholar]
- The dental aesthetic index and dental health component of the index of orthodontic treatment need as tools in epidemiological studies. Int J Environ Res Public Health. 2011;8:3277-86.
- [CrossRef] [PubMed] [Google Scholar]
- Validity assessment and determination of the cutoff value for the index of complexity, outcome and need among 12-13 year-olds in Southern Chinese. Int J Oral Sci. 2012;4:88-93.
- [CrossRef] [PubMed] [Google Scholar]
- Potential application of the dental aesthetic index to prioritize the orthodontic service needs in a publicly funded dental program. Am J Orthod Dentofacial Orthop. 1999;116:279-86.
- [CrossRef] [PubMed] [Google Scholar]
- Evaluation of the dental health component, of the index of orthodontic treatment need, by Swedish orthodontists. Eur J Orthod. 2009;31:184-8.
- [CrossRef] [PubMed] [Google Scholar]
- Subjective and objective perception of orthodontic treatment need: A systematic review. Eur J Orthod. 2013;35:347-53.
- [CrossRef] [PubMed] [Google Scholar]
- The relationship between patient, parent and clinician perceived need and normative orthodontic treatment need. Eur J Orthod. 2004;26:265-71.
- [CrossRef] [PubMed] [Google Scholar]
- The relationship between normative orthodontic treatment need and oral health-related quality of life. Community Dent Oral Epidemiol. 2003;31:426-36.
- [CrossRef] [PubMed] [Google Scholar]
- Preliminary evaluation of an illustrated scale for rating dental attractiveness. Eur J Orthod. 1987;9:314-8.
- [CrossRef] [PubMed] [Google Scholar]
- Orthodontic concern among 11-year-old children and their parents compared with orthodontic treatment need assessed by index of orthodontic treatment need. Am J Orthod Dentofacial Orthop. 1996;110:197-205.
- [CrossRef] [PubMed] [Google Scholar]
- Digital images as an alternative to orthodontic casts in assessing malocclusion and orthodontic treatment need. Acta Odontol Scand. 2007;65:362-8.
- [CrossRef] [PubMed] [Google Scholar]
- Assessment of orthodontic treatment need: A comparison of study models and facial photographs. Community Dent Oral Epidemiol. 2008;36:21-6.
- [CrossRef] [PubMed] [Google Scholar]
- Facial photographs and study models in assessment of orthodontic treatment needs: A comparative study. J Orofac Res. 2012;2:127-30.
- [CrossRef] [Google Scholar]
- Three-dimensional photographs for determining the index of orthodontic treatment need in scientific studies. Am J Orthod Dentofacial Orthop. 2016;150:64-70.
- [CrossRef] [PubMed] [Google Scholar]
- Testing the normal approximation and minimal sample size requirements of weighted kappa when the number of categories is large. Appl Psychol Meas. 1981;5:101-4.
- [CrossRef] [Google Scholar]
- An application of hierarchical kappa-type statistics in the assessment of majority agreement among multiple observers. Biometrics. 1977;33:363-74.
- [CrossRef] [Google Scholar]
- Perception of orthodontic treatment need in children and adolescents. Eur J Orthod. 2010;32:387-94.
- [CrossRef] [PubMed] [Google Scholar]
- Lay Person's perception of smile aesthetics in dental and facial views. J Orthod. 2004;31:204-9.
- [CrossRef] [PubMed] [Google Scholar]
- Orthodontically treated young adults: Awareness of their own dental arrangement. Eur J Orthod. 1991;13:7-14.
- [CrossRef] [PubMed] [Google Scholar]
- The value of the aesthetic component of the index of orthodontic treatment need in the assessment of subjective orthodontic treatment need. Eur J Orthod. 2003;25:57-63.
- [CrossRef] [PubMed] [Google Scholar]
- Normative and self-perceived orthodontic treatment need of a Peruvian university population. Head Face Med. 2006;2:22.
- [CrossRef] [PubMed] [Google Scholar]
- Association between normative and self-perceived orthodontic treatment need among Arab high school students. Am J Orthod Dentofacial Orthop. 2004;125:373-8.
- [CrossRef] [PubMed] [Google Scholar]
- Perceived aesthetic impact of malocclusion and oral self-perceptions in 14-15-year-old Asian and Caucasian children in greater Manchester. Eur J Orthod. 2000;22:175-83.
- [CrossRef] [PubMed] [Google Scholar]
- Orthodontic concerns of Brazilian children and their parents compared to the normative treatment need. J Oral Sci. 2010;52:101-7.
- [CrossRef] [PubMed] [Google Scholar]
- A longitudinal study on subjective and objective orthodontic treatment need. Eur J Orthod. 1997;19:85-92.
- [CrossRef] [PubMed] [Google Scholar]
- Smile esthetics from the layperson's perspective. Am J Orthod Dentofac Orthop. 2011;139:e91-101.
- [CrossRef] [PubMed] [Google Scholar]
- Laypeople's preferences regarding frontal dentofacial esthetics: Periodontal factors. J Am Dent Assoc. 2011;142:925-37.
- [CrossRef] [PubMed] [Google Scholar]
- Impact of malocclusions on quality of life from childhood to adulthood In: Issues in contemporary orthodontics. Vol 3. London: Intechopen; 2015. p. :39-55.
- [CrossRef] [Google Scholar]
- Perceptions of dental esthetics of Asian orthodontists and laypersons. Am J Orthod Dentofacial Orthop. 2006;130:170-6.
- [CrossRef] [PubMed] [Google Scholar]
- Relationships between eight orthodontic indices and an oral self-image satisfaction scale. Am J Orthod. 1978;73:328-34.
- [CrossRef] [PubMed] [Google Scholar]
- Psychosocial implications of malocclusion: A 15-year follow-up study in 30-year-old Danes. Am J Orthod. 1985;87:110-8.
- [CrossRef] [PubMed] [Google Scholar]
- Patient burnout-behaviour of young adults undergoing orthodontic treatment. Stress Med. 1989;5:183-7.
- [CrossRef] [Google Scholar]




