

Translate this page into:
Assessment of contributing factors for discontinuation of orthodontic treatment

*Corresponding author: Nishanthi Vithanarachchi, Department of Community Dental Health, Faculty of Dental Sciences, University of Peradeniya, Kandy, Sri Lanka. nvithanaarachchi3@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Vithanaarachchi N, Medagama T, Nawarathna L. Assessment of contributing factors for discontinuation of orthodontic treatment. APOS Trends Orthod 2020;10(2):105-10.
Abstract
Objectives:
The aims of this study were to assess the prevalence and associated contributory factors for discontinuation of orthodontic treatment.
Materials and Methods:
A hospital-based retrospective study was conducted with the treatment records, whose orthodontic treatment was commenced in the year 2015 at the Division of Orthodontics, University Dental Hospital, Peradeniya. Information regarding age, gender, type of malocclusion, Index of Orthodontic Treatment Need, appliance type, duration of treatment, extraction versus non-extraction, stage of treatment, and the cost of treatment was obtained from the patient’s records. Statistical analysis was performed using the statistical software R 3.5.0.
Results:
The sample consisted of 310 treatment cases, of which 40 (12.9%) patients were discontinued. Among the discontinued patients, 50.6% were male and 49.3% were female. The discontinuation rate in the group of 12–17 years was higher than the other age groups, which was statistically significant (P = 0.005). Among the group of discontinued treatment, 49.3% were of Class II division 1 malocclusion and 37.1% and 37.4% of patients were in Grade 3 and 4 of IOTN, respectively. About 37% of patients have been discontinued before completion of 1 year which was statistically significant (P = 0.0005). About 59.5% of non-extraction patients were in the treatment discontinuation group which was also statistically significant (P = 0.023). About 32.5% of the patients who discontinued have obtained the treatment with the lowest cost with statistical significance (P = 0.026).
Conclusion:
Children with borderline and moderate occlusal irregularities treated with simple removable appliances which are affordable with low cost were more prone to discontinue in the early phase of active treatment.
Keywords
Orthodontic
Treatment
Discontinuation

INTRODUCTION
A course of orthodontic treatment could be considered as successfully completed if the aims of the treatment have been fully achieved and an adequate retention period has been completed. A patient who does not go through the whole of this process is considered a discontinued patient. Several researchers in different countries have studied this issue of discontinuation and have assessed the rate of patients who opt out of treatment before its successful completion. The studies show that the rate of discontinuing patients ranges normally between 10 and 20%.[1] Table 1 is a summary of the results of some of these studies.[1]
| Study by | Country | Number of study | Discontinuation percentage |
|---|---|---|---|
| Rose (1974) | UK | 1000 | 12 |
| Myrberg and ilander (1973b) | Sweden | 14.7 | 1486 |
| Cousns et al. (1981) | UK | 250 | 17 |
| Haynes (1982) | UK | 122 263 | 20 |
Since the above involved patients from the Western world with different socioeconomic factors that could influence the said findings, this may not be absolutely comparable to the discontinuation rates seen in Sri Lanka which is a developing country with the different socioeconomic milieu.
A search of the literature failed to show any previous study undertaken to analyze the discontinuation of orthodontic treatment in a Sri Lankan population to assess its incidence and prevalence. Different contributory factors have been assessed individually as well as on the whole study population including age, sex, socioeconomic level of patients, the severity of malocclusion, cost of treatment, and duration of the treatment.
Hayness (1982) found that the age of the patients correlates directly with the discontinuation rate, older the patient, higher the discontinuation rate had been.[2] An American study revealed that age correlated with the cooperation of the patient, although at a fairly low level of significance.[3]
The sex ratio of patients who discontinued their orthodontic treatment has been reported as female:male = 3:2.[4,5] The same study investigated the association between socioeconomic patterns among the patients who discontinued the treatment.[4] Rolling (1982) reported that more patients from social Classes IV and V tend to drop out from treatment and social Classes I, II, and III usually completed the treatment in a sample of Danish schoolchildren.[5] Turbill also has highlighted in their research that lower social class may be a contributory factor for discontinuation, but it cannot be considered as a predictor for discontinuation itself.[6]
Studies have been carried out on the effect of the type or the severity of malocclusion on treatment discontinuation. These studies have employed different types of indices such as an index of orthodontic treatment need in categorizing the severity of malocclusion and patient compliance in both fixed and non-fixed orthodontic treatments.[7,8]
Accurate information on the prevalence of discontinuation from treatment and associated contributory factors is needed to address them at the stage of treatment planning as it would be beneficial to the patient as well as the clinician in maximizing the ultimate benefits from orthodontic treatments. Hence, the present study aimed to assess the prevalence and associated contributory factors for the orthodontic treatment discontinuation.
MATERIALS AND METHODS
This hospital-based retrospective study was conducted with the available treatment records at the Division of Orthodontics, University Dental Hospital, Peradeniya in Sri Lanka, whose orthodontic treatment was commenced in the year 2015. Ethical clearance was obtained from the Ethics Review Committee of the Faculty of Dental Sciences, University of Peradeniya. The definition of completed treatment was that all the treatment aims were achieved, and appropriate retainers were fitted following the completion of active orthodontic treatment. Discontinued treatment was defined as early termination of active treatment with any reason and with failure to complete the aims of the treatment. Information regarding age, gender, type of malocclusion, Index of Orthodontic Treatment Need (IOTN), appliance type, duration of treatment, extraction versus non-extraction, stage of treatment, and cost of the treatment was obtained from the patient’s record to assess the contributing factors for the discontinuation. Medically compromised and syndromic patients were excluded from the study.
All the computations in this study have been performed using the statistical software R 3.5.0. Descriptive statistics, including the frequencies, percentages, mean, and standard deviation (SD), were computed for each variable. Wilcoxon rank-sum test was carried out to assess the significance of the variables of the study sample when the population cannot be assumed to be normally distributed. Significant differences were determined at 95% probability level. Since all the categorical variables had been converted into numerical data, Pearson correlation matrix had been used to identify the association between all the data. Pearson’s Chi- square test of association was used to discover if there is a relationship between two categorical variables. Fisher’s exact test was indicated to assess the association between variables when the sample size was small. Logistic regression was used to build up a model to predict the discontinuation of orthodontic treatments of dental patients. Further, it is used to determine the factors associated with discontinuing the orthodontic treatments.
RESULTS
A total of 310 treatment cases, with an age range of 6–30 years, were analyzed and 40 cases were recorded as discontinued treatment and 270 cases were identified as successfully completed treatment. The discontinuation rate was 12.9% with a mean age of 12.51 ± 4.10 years. Among the discontinued patients, 50.6% were male with a mean age of 12.53 ± 4.37 years and 49.3% were female with a mean age of 12.71 ± 4.98 years. The highest discontinuation rate was observed in the group of 12–17 years of age and it was statistically significant (P = 0.005).
In the assessment of malocclusion among the group of discontinued treatment, 49.3% were of Class II division 1 malocclusion and 29.6% had Class I malocclusion. The highest percentage of patients was identified as discontinuation in Grade 3 (73.1) and 4 (37.4) of IOTN without any statistical significance. Among the discontinued patients, 37.1% were treated with simple removable appliances and 30% with functional appliances and 14.5% with fixed appliances [Figure 1]. The percentage of patients who discontinued during active treatment was 61.8% and 12% discontinued during the retention phase. Among the patients who discontinued during active orthodontic treatment, 37% discontinued before completion of 1 year and this was statistically significant (P = 0.0005) [Figure 2]. Furthermore, 61% of patients who discontinued in the retention phase were indicated for removable retainers. Furthermore, 59.5% of non-extraction patients were in the treatment discontinuation group and this was statistically significant (P = 0.023). In the assessment of the cost of the treatment, 32.5% of the patients who discontinued have obtained the treatment with the lowest cost and this finding was statistically significant (P = 0.026) [Table 2].

- Percentage of appliance wear by the treatment discontinued patients.
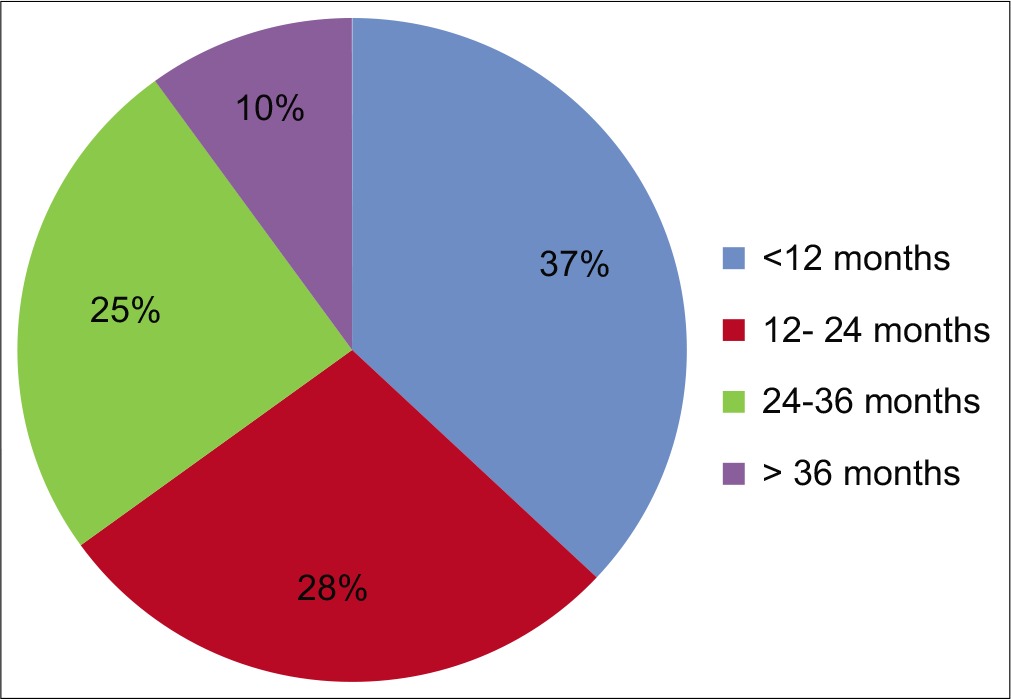
- Percentage of treatment duration of discontinued patients.
| Variables | Estimate | Std. error | z value | P-value | |
|---|---|---|---|---|---|
| Gender | |||||
| Intercept | 4.04E+01 | 8.52E+03 | 0.005 | 0.9962 | |
| Female | 8.26E-01 | 6.52E-01 | 1.266 | 0.2054 | |
| Age (years) | |||||
| 6–12 | 2.97E-03 | 7.87E-01 | 0.004 | 0.9970 | |
| 12–17 | -3.30E+00 | 1.68E+00 | −1.959 | 0.0501* | |
| 17–23 | −3.76E-01 | 1.79E+04 | 0.000 | 0.9999 | |
| 23–30 | 1.92E+01 | 1.77E+04 | 0.001 | 0.9991 | |
| Type of malocclusion | |||||
| Class I | 1.53E+00 | 2.05E+00 | 0.749 | 0.4538 | |
| Class II division 1 | 1.17E+00 | 8.32E-01 | 1.409 | 0.1587 | |
| Class II division 2 | 8.39E-01 | 1.10E+00 | 0.766 | 0.4434 | |
| Class III | −1.33E-01 | 8.00E-01 | −0.167 | 0.8676 | |
| Severity of malocclusion | |||||
| IOTN–Grade 2 | -1.62E+01 | 8.10E+03 | −0.002 | 0.9984 | |
| IOTN–Grade 3 | -2.05E+01 | 8.10E+03 | −0.003 | 0.9979 | |
| IOTN–Grade 4 | -2.06E+01 | 8.10E+03 | −0.003 | 0.9979 | |
| IOTN–Grade 5 | -1.90E+01 | 8.10E+03 | −0.002 | 0.9981 | |
| Type of appliance | |||||
| Simple removable appliance | 2.62E+00 | 1.90E+00 | 1.383 | 0.1666 | |
| Fixed appliance (Single arch) | 1.29E+01 | 7.46E+03 | 0.002 | 0.9986 | |
| Fixed appliance (both arches) | −2.88E-01 | 1.87E+00 | −0.154 | 0.8778 | |
| Functional appliances | 9.95E-01 | 1.88E+00 | 0.528 | 0.5974 | |
| Head gears | -4.45E+00 | 6.77E+00 | −0.658 | 0.5108 | |
| Combined treatment | -1.87E+00 | 8.10E+03 | −0.003 | 0.9967 | |
| Stage of treatment | |||||
| Active treatment | -2.39E+01 | 2.66E+03 | −0.009 | 0.9928 | |
| Retention phase | -2.59E+01 | 2.66E+03 | −0.010 | 0.9922 | |
| Extraction versus non-extraction | |||||
| Non-extraction | -2.08E+00 | 9.17E-01 | −2.272 | 0.0231* | |
| Extraction of permanent teeth | 2.08E-01 | 9.08E-01 | 0.229 | 0.8186 | |
| Cost of treatment | |||||
| <2000 LKR | 3.72E+00 | 3.33E+00 | 2.117 | 0.0263* | |
| 2000–5000 LKR | 5.88E+00 | 3.59E+00 | 1.639 | 0.1013 | |
| 5000–10,000 LKR | 4.81E+00 | 3.72E+00 | 1.294 | 0.1955 | |
| <10,000 LKR | 6.77E+00 | 3.76E+00 | 1.800 | 0.1718 | |
| Duration of treatment (months) | |||||
| <12 | -4.55E+00 | 1.30E+00 | −3.493 | 0.0005* | |
| 12–24 | 1.44E+00 | 1.20E+00 | 1.196 | 0.2315 | |
| 24–36 | 4.44E-01 | 1.14E+00 | 0.391 | 0.6959 | |
| >36 | 2.94E+00 | 1.54E+00 | 1.910 | 0.0560 | |
DISCUSSION
Discontinuation rate
The discontinuation rate among patients in this study was 12.9% and this finding is exactly compatible with discontinuation rate reported by McDougall study done in the primary care orthodontic practice in the UK[9] and also comparable to the finding of a similar study undertaken at the Eastman Dental Hospital in London.[1] However, some of the discontinuation rates reported in the literature vary from 3% to 42%.[5,10] When the discontinuation rate of Sri Lankan study is composed with other research findings, it appears to be at a lower rate, which could be attributed to a better quality of orthodontic care provided by the National Health Services. Further, the percentage of completed treatment is one of the determinant indicators of the quality of orthodontic services provided by the National Health Services. However, it is needed to continue this study regionally as well as nationally to conclude the ultimate discontinuation rates of orthodontic services in the country.
Age
The results of the present study have shown higher discontinuation rate in the preadolescent age (12– 17 years) group than the other groups and the mean age of discontinuation was around 12.5 ± 4, which was statistically significant. Confirming our findings, some of the studies have also reported that younger patients have a higher discontinuation rate than the older patients.[11] However, some researchers have identified that adult patients show more cooperation toward orthodontic treatment than younger patients and some studies have highlighted the positive correlation of age and compliance of orthodontic patient.[12]
Gender
The discontinuation rates in both males and females of the present study were found to be nearly equal. Similar gender distribution has been observed in a study in a rural sample from North-Central Appalachia in the USA.[13] However, some other studies have identified a male predominance among those who discontinued orthodontic treatment highlighting better adherence to facial appearance, in relation to attractiveness in females.[14]
Type of malocclusion
The present study shows that patients with Class II division 1 malocclusion failed to complete treatment compared those with the other malocclusions. This finding could be due to the fact that the majority of patients who seek orthodontic treatment are with proclined upper incisors due to its unesthetic nature. Besides, Class I malocclusion showed the second highest discontinuation rate compared to other malocclusions. However, a study among patients in North- Central Appalachia in the USA showed that patients with Class III malocclusion had greater premature discontinuation of treatment although this finding was statistically not significant.[13] The study highlighted that this finding could be due to the protrusion of lower teeth in Class III malocclusion being less noticeable and thus socially less compelling for patients to complete treatment. However, contrary to these findings, some other studies failed to find the presenting malocclusion being a significant factor in the discontinuation of treatment.[1]
IOTN index
According to the present study, the patients who were identified in IOTN 3 and 4 categories at the commencement of treatment discontinued in a higher percentage than other categories. This finding could be due to the patients being less concerned with their borderline esthetic issues than severe dental irregularities. Furthermore, these patients0020could have been primarily influenced by the opinion of the referring dentist or their peers rather than of their own wish in seeking treatment. Fox (2004) reported that most failures of orthodontic treatment were identified in borderline groups compared to other categories of IOTN, which further confirms with the present study.[8] Nonetheless, some studies have identified higher rates of failures in cases with IOTN Category 5 when compared with cases of 3 and 4.[15]
Appliance type
When considering the type of appliance is considered, the highest percentage of discontinuation was associated with simple removable appliances. Similar results were observed with a study done in general dental services of England and Wales.[15] Patients who wore functional appliances also showed higher rates of discontinuation than those with fixed appliance. McDougall also identified that the majority of failed treatment were from the group of functional appliances compared to other orthodontic appliances.[9] In general, fixed appliances were only infrequently associated with discontinuation and this could be due to the relative ease of discontinuation with removable appliances than with fixed appliances which necessitate removal by a clinician. The retrospective study conducted in the UK by Turbill (2003) also showed that relatively fewer discontinued cases identified with a group of fixed appliances, which suggests that, if a fixed appliance alternative exists, this may be preferable to removable and/or functional appliances.[6]
Discontinuation stage
Among the discontinued group, 47% of patients discontinued during the period of active orthodontic treatment phase, in which 37% of them were discontinued in the period of the first 12 months of active treatment which was statistically significant. Nearly 15% of patients who discontinued at the end of active treatment and 12% discontinued within the period of a retention phase. Similar results were observed with the study conducted by McDougall with the orthodontic patients from the primary care orthodontic practice in the UK.[9] These research findings highlight the importance of patients being able to comprehend the difficulties that would be encountered with removable and functional appliances before the commencement of treatment. Further, it is important to gain sufficient motivation before patients consented for such treatment. The present study showed that the majority of patients who discontinued treatment in the retention phase were treated with removable retainers. This could be due to the poor compliance of the patient toward removable devices which have been confirmed by a previous study conducted on patient’s compliance.[11] Therefore, it is of paramount importance to plan non-compliance hand in hand with more esthetic retainers to maximize the benefit achieved with the active phase of treatment.
Extraction versus non-extraction
There is a greater failure rate of non-extraction patients with positive significance when compared with the patients who have undergone extractions for orthodontic purposes. The similar results have been observed with the study done by McDougall, in 2017.[9] Richmond also reported that non-extraction treatment was more often discontinued than extraction treatment with positive significance.[15] However, some patients discontinue the treatment even after extractions. Therefore, it is important to consider this issue by the patients as well as clinicians to minimize the discontinuation of treatment, especially following extractions which may give rise to more unesthetic appearance due to remaining spaces.
Cost of treatment
In the assessment of the association between the cost of treatment and discontinuation rate, the highest percentage of patients who failed to complete treatment was those who had obtained treatment with the lowest cost, which was statistically significant. Much less discontinuation rate was observed when the treatment cost was high. These findings were further confirmed by the study conducted with a rural sample in North-Central Appalachia.[13] This finding explains well with the cognitive dissonance theory which implies when one is interested in a task (with money or resources) it values to a greater degree, with more motivation to successfully accomplish the task.[16,17] These results highlight the prompt consideration of orthodontic payment structure that involves in cost sharing and value for health care.[18,19]
CONCLUSION
Based on the results of the present study, it may be concluded that children who are treated with removable appliances are more prone to discontinue the orthodontic treatment during the early phase of active treatment. Furthermore, orthodontic patients who are in IOTN 3 and 4 categories are more prone to discontinue than the other categories. This study also confirms that the amount of financial investment has a positive correlation with the compliance toward orthodontic treatment. It should also be stressed that these factors are not absolute predictors for the discontinuation of orthodontic treatment unless confirmed with further studies with a wider sample. However, so far, there is no proper index, or a tool identified to predict the compliance level of a patient. Therefore, while considering all these contributory factors, it may be high time to develop a psychological- based questionnaire that may help to determine the patient’s attitudes and motivation toward successful treatment.
Declaration of patient consent
Patients consent not required as patients identity is not disclosed or compromised.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Discontinuation of the orthodontic treatment: A study of contributory factors. Br J Orthod. 1989;16:1-7.
- [CrossRef] [PubMed] [Google Scholar]
- Discontinuation of orthodontic treatment in the general dental service in England and Wales 1972 to 1979. Br Dent J. 1982;152:127-9.
- [CrossRef] [PubMed] [Google Scholar]
- A thousand consecutive treated orthodontic cases-a survey. Br J Orthod. 1974;1:45-54.
- [CrossRef] [PubMed] [Google Scholar]
- Orthodontics as a public service: The Wessex survey. Trans Br Soc Orthod 1966:1-10.
- [Google Scholar]
- Orthodontic treatment and socio economic status in Danish school children aged 11-15 years. J Community Dent Oral Epidemiol. 1982;12:130-2.
- [CrossRef] [PubMed] [Google Scholar]
- Social inequality and discontinuation of orthodontic treatment: Is there a link? Eur J Orthod. 2003;25:175-83.
- [CrossRef] [PubMed] [Google Scholar]
- Influence of severity of malocclusion on the duration of orthodontic treatment. Am J Orthod. 1973;63:533-6.
- [CrossRef] [Google Scholar]
- Measuring failure of orthodontic treatment: A comparison of outcome indicators. J Orthod. 2004;31:319-22.
- [CrossRef] [PubMed] [Google Scholar]
- Factors associated with discontinued and abandoned treatment in primary care orthodontic practice part 2: A practice based study. J Orthod Update. 2017;10:52-8.
- [CrossRef] [Google Scholar]
- The use of personality measurements as a determinant practice. Am J Orthod. 1968;54:433-9.
- [CrossRef] [Google Scholar]
- Assessment of factors associated with patient's compliance in orthodontic treatment. Sri Lanka Dent J. 2017;47:1-12.
- [Google Scholar]
- Non-completion of active orthodontic treatment. Br J Orthod. 1992;19:147-54.
- [CrossRef] [PubMed] [Google Scholar]
- Orthodontic treatment completion and discontinuation in a rural sample from North Central Appalachia in the USA. Front Public Health. 2017;5:171.
- [CrossRef] [PubMed] [Google Scholar]
- The influence of dentofacial appearance on the social attractiveness of young adults. Am J Orthod. 1985;87:21-6.
- [CrossRef] [Google Scholar]
- Discontinued orthodontic treatment in the general dental services of England and Wales (1990-1991) Br J Orthod. 1995;22:263-8.
- [CrossRef] [PubMed] [Google Scholar]
- Assessing the evidence for value-based insurance design. Health Aff (Millwood). 2010;29:1988-94.
- [CrossRef] [PubMed] [Google Scholar]
- 'Nudging' your patients toward improved oral health. J Am Dent Assoc. 2012;143:907-15.
- [CrossRef] [PubMed] [Google Scholar]




