
Translate this page into:
Class III Molar Finish as a Different Treatment Approach to Correct an Adolescent Class II Patient Using Headgear, Forsus, and Lower Arch Extraction
Address for correspondence: Dr. Shafees Koya, Department of Orthodontics and Dentofacial Orthopaedics, Yenepoya Dental College, Yenepoya University, Mangalore, Karnataka, India. E-mail: skoya@hotmail.com
This article was originally published by Wolters Kluwer and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Various treatment strategies are adopted to correct a Class II malocclusion depending on the age, the amount of remaining growth and severity of malocclusion. Single arch extraction of the lowers is rarely done in a Class II malocclusion. The following case report describes an alternate treatment approach of an adolescent Class II patient treated with a combination of headgear, fixed functional appliance (forsus), and single arch extraction only in the lower arch. The case was finished in a Class III molar and a Class I canine relationship. The results were stable in 3 years follow-up.
Keywords
Class II adolescent
Class III molar finish
driftodontics
forsus
headgear

[SHOW_RELATED_PUBMED_ARTICLES]
Introduction
A Class I canine relationship is considered important for proper function and stability. In finishing, an excellent intercuspation with a Class I canine relation is given importance irrespective of its molar relation. The most popular treatment option in a Class II malocclusion is a Class I molar finish followed by a Class II molar provided the canines are in Class I relation. Although a Class I canine with a Class III molar finish is also a treatment option, it is very rarely carried out.
Many a time, Class II malocclusions result due to combinations of skeletal and dental components, especially a prognathic maxilla and retruded mandible. Class II treatment alternatives vary depending on the age, the amount of remaining growth, and severity of malocclusion. Various treatment strategies can be adopted to correct a Class II malocclusion. Patients with Class II subdivision malocclusions have long been a treatment challenge for the clinicians. They are usually addressed in various treatment approaches showing its diversity in treatment philosophies such as asymmetric extractions, mandibular advancements with the functional appliance, distalization, temporary skeletal anchorage devices, surgical approaches, etc.[1]
A Class II molar finish is achieved by extraction only in the upper arch. Single arch extraction of the lowers is rarely done in a Class II malocclusion. The following case report describes an alternate treatment approach of an adolescent patient with an Angle’s Class II subdivision malocclusion and Class II skeletal pattern treated with a combination of headgear, fixed functional appliance (forsus) and single arch extraction only in the lower arch. The case was finished in a Class III molar and a Class I canine relationship.
Case Report
Diagnosis
A 13 years 7 months female patient presented with Angle’s Class II division 1 subdivision malocclusion and Class II skeletal base with normal vertical proportion [Figure 1]. She exhibited Angle’s Class I molar relation on the right side and Class II molar relation on the left side. Her extra-oral features included convex profile with a posterior facial divergence, protrusive and incompetent upper and lower lips and a normal nasolabial angle. Her visual treatment objective was positive. She also displayed 7 mm overjet, severe lower anterior crowding of 13 mm and upper potential crowding, overbite (5.5 mm), rotated lower second premolars, and 2 mm midline discrepancy. Upper midline was shifted to the right side by 1 mm with respect to the maxilla and lower midline by 1 mm to the left side with respect to the maxillary midline. Hand wrist radiograph was taken to assess the growth status of the patient. According to Fishman skeletal maturity indicator (SMI), the growth status was interpreted as SMI-7 indicating 31% of growth potential is remaining for the maxilla and 33% for the mandible. Huckaba’s analysis predicted 9 mm potential crowding for the erupting canines in the upper arch. The cephalometric analysis revealed Class II skeletal antero-posterior relationship with an ANB of 6°, Yen angle[2] of 114° and Wits appraisal of +7 mm [Table 1]. Effective maxillary length of 102 mm and mandibular length of 121 mm showed that maxilla was increased in length for that age and the mandible was decreased in length for that maxilla, suggesting an increased maxilla and decreased mandible responsible for its sagittal skeletal disharmony. Although clinically the upper incisor appeared proclined, cephalometrically, they were of ideal inclination (upper incisor to NA-4 mm). The lower incisors were mildly proclined in relation to the mandibular plane (IMPA-98°). The upper and lower lips were both significantly protrusive relative to Rickett’s E plane.
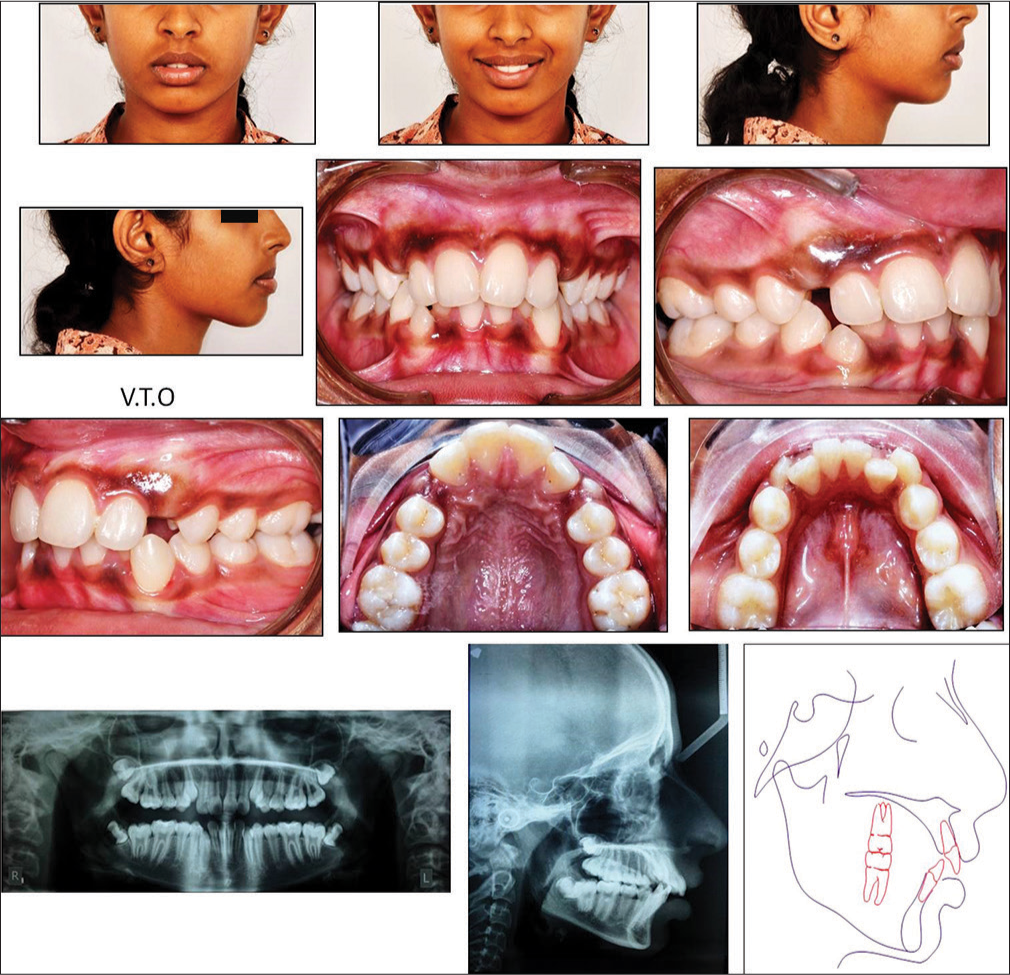
- Pretreatment photographs and radiographs
| Norm | Pre-treatment | Post treatment | Difference | |
|---|---|---|---|---|
| SNA | 82° ± 3 | 77° | 78° | 10 |
| SNB | 79° ± 3 | 71° | 75° | 4° |
| ANB | 3° ± 1 | 6° | 3° | -3° |
| SN to Maxillary plane | 8° ± 3 | 16° | 15° | 1° |
| Wits appraisal | 0mm | 7mm | 2mm | -5mm |
| Upper incisor to maxillary plane angle | 108° ± 5 | 114° | 108° | -6° |
| Lower incisor to mandibular plane angle | 92° ± 5 | 98° | 95° | -3° |
| Interincisal angle | 133° ± 10 | 126° | 134° | 8° |
| MM angle | 27° ± 5 | 24° | 24° | 0° |
| SN-GoGn | 32° | 41° | 42° | 1° |
| Lower incisor to A-Pog line | 0-2 mm | 2mm | 3mm | 1mm |
| Lower lip to Ricketts E plane | -2mm | 2mm | 2mm | 0mm |
| FMA | 22° | 25° | 28° | 3° |
| 1 TO NA (LINEAR) | 4 mm | 4mm | 3mm | -1mm |
| 1 TO NA (Degree) | 22° | 22° | 17° | -5° |
| Lower 1 TO NB (LINEAR) | 4 mm | 7mm | 7mm | 0mm |
| Lower 1 TO NB (Degree) | 25° | 26° | 29° | 3° |
| YEN Angle | 117-123° | 114° | 119° | 5° |
| Effective maxillary length | 92.1± 2.7mm | 102mm | 102mm | 0mm |
| Effective mandibular length | 118.9±5mm | 121mm | 125mm | 4mm |
| NLA | 90-110° | 100° | 108° | 8° |
The treatment goals were to correct the Class II skeletal pattern and maintain the vertical skeletal proportions, relief of crowding in the lower arch, guide the eruption of the upper right and left canines into the arch, correct the overjet and overbite and correct the midline discrepancy. Various treatment options of camoflaging with extractions were discussed. However, since the patient was in a growing period with almost 30% growth remaining, a growth modulation treatment plan was preferred over camouflage. The treatment plan decided was to use headgear to restrict the growth of maxilla and to unilaterally distalize the Class II side (upper left first molar) to a Class I molar relation. Since there was an increased sagittal (by 7 mm of effective maxillary length) and vertical growth of maxilla (increased FMA, SN-GoGn) a, a high pull headgear was preferred. It can also decrease the vertical development of the maxilla, thereby allowing for autorotation of the mandible and maximizing the horizontal expression of mandibular growth. Extraction of lower first premolars were also planned to correct the crowding and curve of spee followed by the advancement of the mandible to correct the overjet with fixed functional appliances (Forsus) to a Class I canine and Class III molar finish. Since the upper incisor to NA was normally positioned (4 mm) and inclined (22°), the planned upper incisor position was to keep in its position itself. Molar distalization will allow to relieve the potential crowding enabling the guidance of eruption of the canines in place. Due to the increased lower incisor to NB (7 mm) and the crowding of 13 mm lower premolars extractions were planned. Thus, after retraction the current overjet will be 10 mm which will be addressed by the advancement of the mandible by 7 mm using a fixed functional appliance achieving a Class I canine and Class III molar finish. Headgear will also help to control the vertical growth pattern. The lower arch was left for driftodontics to enable more physiological correction till sufficient alignment was achieved.
Treatment progress
Upper arch was bonded with preadjusted edgewise fixed appliances (0.022” × 0.028” slot) with MBT prescription and molars were banded. Open coil spring was placed between lateral incisor and first premolar on both sides in the upper arch to maintain the space for the eruption of canines [Figure 2a]. High pull headgear was prescribed in the following appointment to restrict the growth of maxilla and for unilateral distalization of the left first molar. The force levels were varied to enable unilateral distalization with 250 g on the right side, and 450 g on the left side [Figure 2b]. Patient was advised to wear it for 14 h a day along with other safety instructions. In the lower arch, the first premolars were extracted, and anteriors were left for alignment by driftodontics. The upper left first molar was distalised from an Angle’s Class II to a Class I molar relation in 8 months which also enabled the upper canines to erupt in place. The headgear therapy was continued until the end of the treatment to retrict the growth of maxilla, control vertical growth pattern, and to maintain the achieved distalization. The wires were sequence changed from 0.016 nickel-titanium (NiTi) to 0.019 × 0.025 NiTi arch wire. The upper canines were bonded and tied to the 0.019 × 0.025 NiTi main archwire to allow its further eruption [Figure 3]. After its sufficient eruption, the archwire was engaged in the canine brackets. After 9 months of driftodontics, the lower anteriors were sufficiently aligned with a residual space of 2–3 mm [Figure 2c]. At this point of time, the brackets were bonded for further levelling and aligning. Lingual buttons were bonded and couple force were given to correct the rotated lower second premolars. The residual space of the lower arch were closed by e-chain retraction in 0.019 × 0.025 S.S archwire. After the space closure, the lower arch was consolidated and cinched back and forsus fatigue resistance device (FRD)[3] (29 mm size) was placed bilaterally, passively advancing the mandible by 2 mm [Figure 4]. In further visits, forsus were activated by 2 mm by adding crimbs both the sides. An advancement of 6 mm was achieved after 5 months of forsus therapy giving a Class I canine and Class III molar relation. Forsus therapy was done for 7 months and then replaced with a Class II elastics to maintain the achieved advancement along with settling elastics. Settling elastics were given to settle the posterior occlusion. Fixed appliance was debonded after overall active treatment of 29 months. Beggs wrap around retainers were given for both the arches.

- (a) Open coil spring was placed to maintain the space for the eruption of canines (b) force levels was varied to enable unilateral distalization (c) after 9 months of driftodontics, the lower anteriors were sufficiently aligned
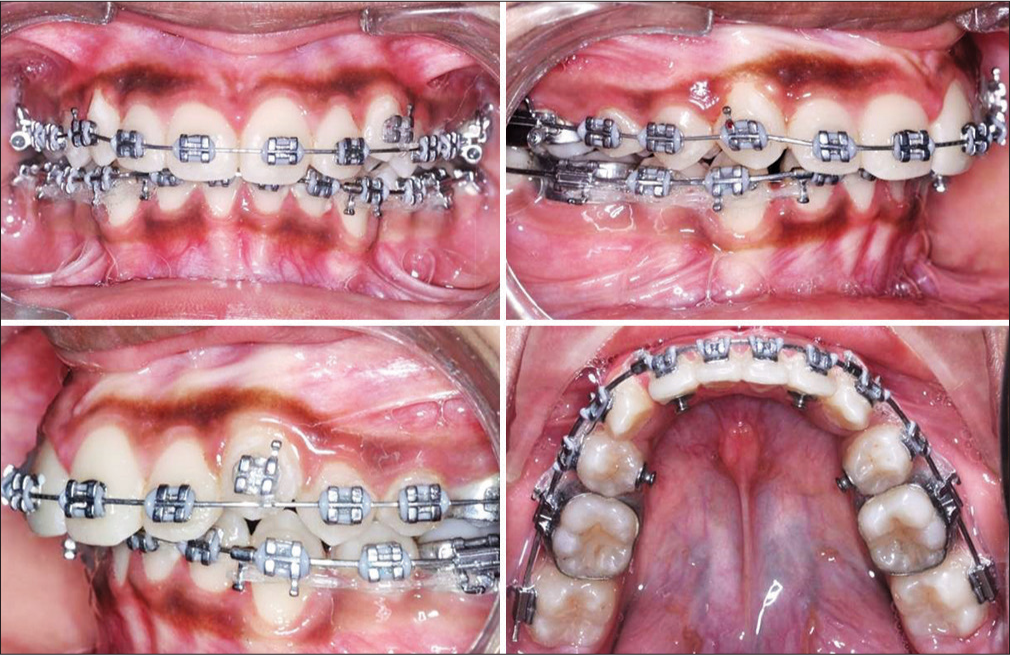
- Upper canines were bonded and tied to the 0.019 × 0.025 nickel-titanium archwire. Lingual buttons were bonded to derotate lower second premolars
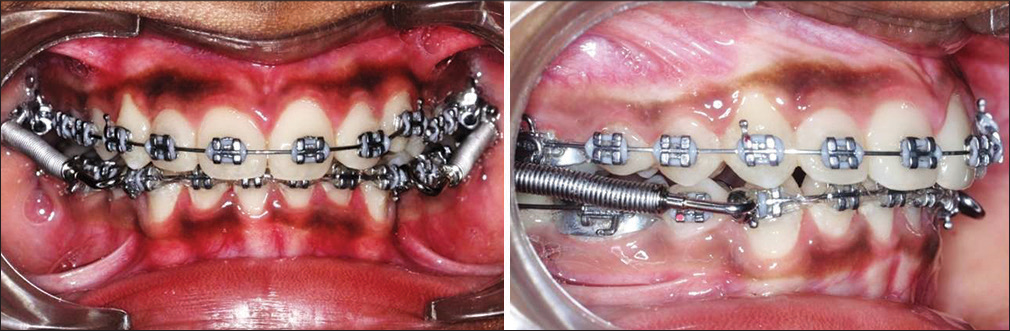
- After space closure forsus fatigue resistance device (29 mm size) was placed
Treatment results
All the treatment goals were achieved with excellent intercuspation, overbite and overjet finishing the case in a Class I canine and Class III molar relation [Figure 5]. The patient showed good compliance in wearing her headgear and elastics, but not in oral hygiene. Progression of the gingival recession was noticed in 41 despite proper oral prophylaxis and oral hygiene instructions. The posttreatment extraoral photographs demonstrated an improved profile and chin-to-lip contour. Lips were competent at rest with the upper incisor under the control of lower lip which will help for a long-term stability. Both the patient and her parents expressed satisfaction with her facial appearance, profile, and smile.
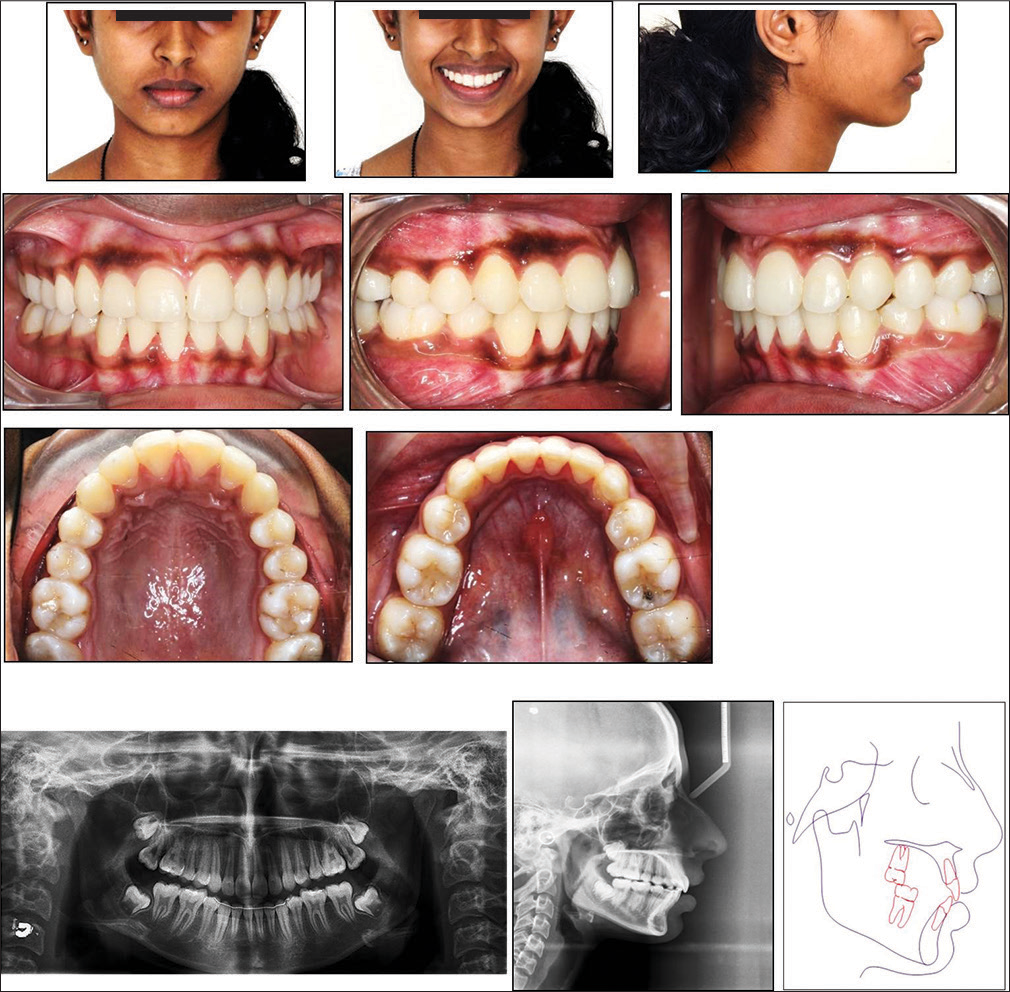
- Posttreatment photographs and radiographs
Post-treatment cephalometric values [Table 1] and superimpositions [Figure 6] supported the improved clinical appearance. The lower incisor to mandibular plane angle was decreased by-3° making it normally inclined. Thus, the unwanted proclination of lower anteriors that may result from a fixed functional was controlled. The lower incisor position with respect to A-Pog was also within the normal range. SNB was increased by 4° suggesting the forward movement of point B in relation to the cranial base. Sympathetic nerve activity was increased by 1°. Thus, ANB was decreased by 3° improving from a Class II skeletal pattern to a Class I skeletal pattern. Wits appraisal (2 mm) and Yen angle (119°) also supported the improvement to a Class I skeletal pattern. The effective mandibular length was increased by 4 mm and maxillary length remained the same. Vertical proportions were controlled, and there was no relevant increase in it as indicated by FMA and SN-GoGn. The overall superimposition showed the mesial movement of the lower molars due to advancement. Mandibular superimposition registered on Bjork’s stable mandibular structures shows leveling of the spee by extrusion of posteriors and intrusion of anteriors. Maxillary superimposition registered on the anterior surface of the palatal vault shows distalization of molars and slight lingual movement of incisors [Figure 7]. The nasolabial angle was increased by 8°, but was within normal range. The lower lip position relative to Ricketts E-plane remained the same.
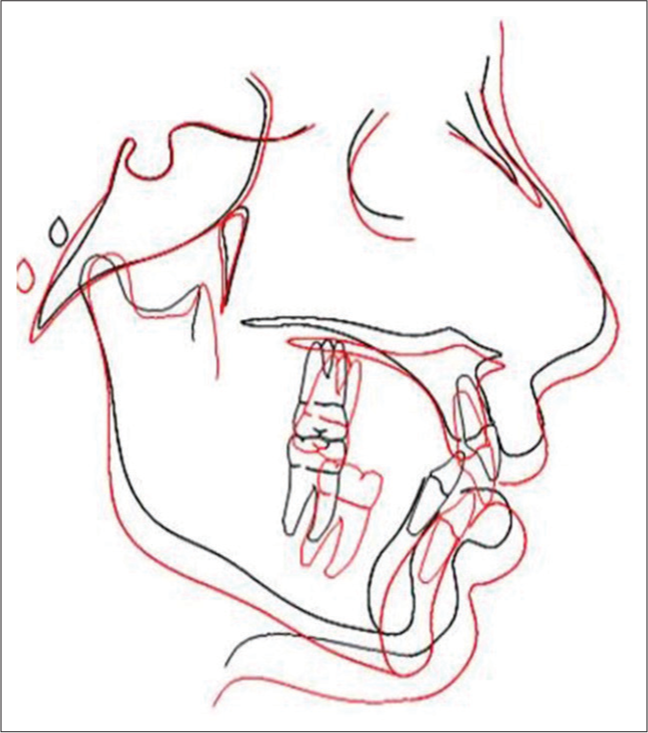
- Posttreatment Superimposition
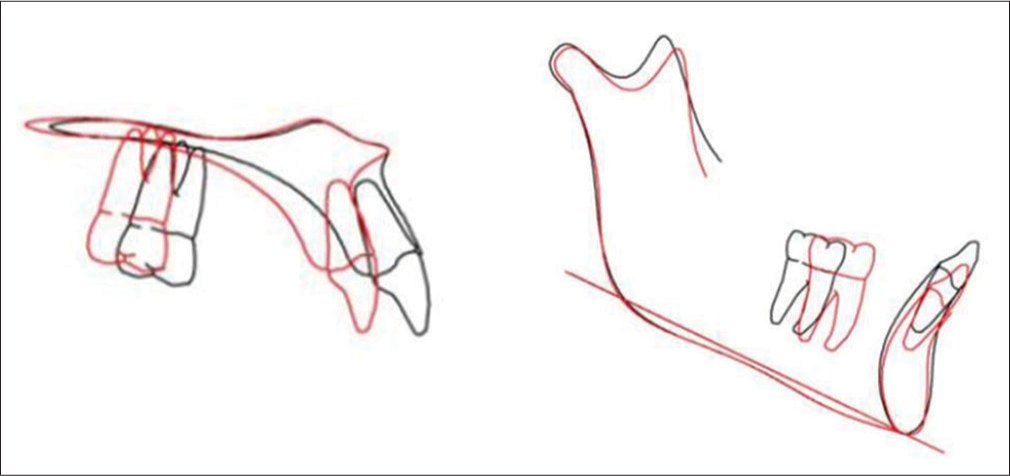
- Posttreatment superimposition of maxilla and mandible
Three years follow-up revealed the occlusion to be stable with good intercuspation, overjet and overbite [Figure 8]. The Class I canine and Class III molar finish achieved posttreatment is maintained. Her smile and profiles looked pleasing. The patient is happy and satisfied with the results. There was a slight lower midline relapse by 1 mm to the left side with respect to the maxillary midline. As a result of poor oral hygiene, marginal gingivitis with the gingival recession in relation to 41 was present. The patient was educated and motivated about the oral hygiene and the importance of regular checkup.

- Three years follow-up photographs
Discussion
This patient was successfully treated with fixed mechanotherapy, growth modulation using head gear and forsus, unilateral distalization of the Class II side with head gear along with the single arch extraction of the lowers. In the upper arch, space was gained by distalization of upper left first molar (Class II side) and in the lower arch by the extraction of first premolars. The potential crowding in the upper arch was never revealed, and driftodontics approach in the lower arch enabled the patient to have a shorter period of appliance wear in the lower arch. She had a Class II skeletal pattern due to increased maxillary length and decreased mandibular length for that maxilla. The use of high pull headgear helped to restrict the further growth of maxilla and to maintain the vertical proportions. The distalization was due to the distal force of the head gear (450 g) and the open coil spring which was placed between lateral and first premolar. Both produced opposite moments which cancelled each other leading to bodily distalization of upper left molar [Figure 9].The light force (250 g) given on the right side was not sufficient for further distalization of the right first molar. The fixed functional appliance encouraged mandibular advancement finishing the case in a Class I canine and a Class III molar relationship.
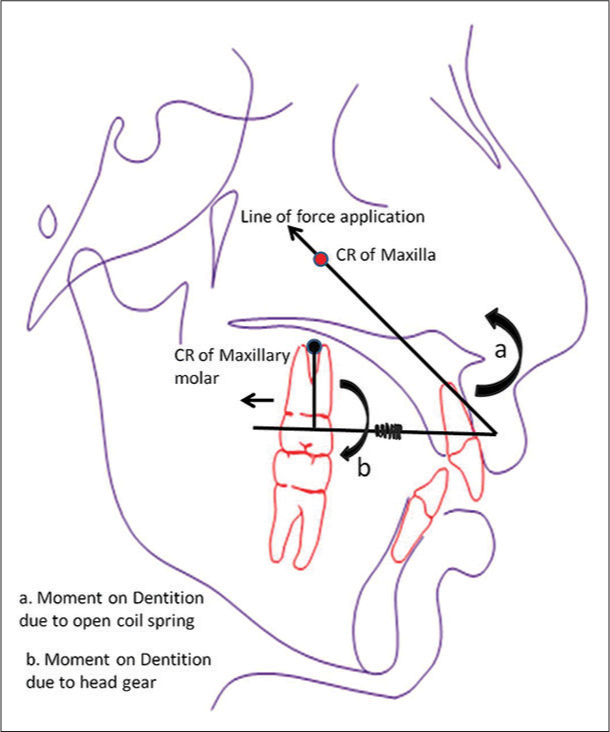
- Force vector analysis depicted for the headgear enabling unilateral distalization, sagittal and vertical control
A high pull headgear restricts the horizontal and vertical growth of maxilla along with distalization and intrusion of the maxillary molars.[4-6] Many studies have shown that a combination of headgear and removable functional appliance therapy restricts the forward growth of the maxilla, inhibits the mesial displacement of the maxillary teeth, inhibits maxillary tooth eruption, increases the horizontal growth of the mandible, remodels the condyle and glenoid fossa and by mesially moves the mandibular teeth.[7-10] In this case, we decided to go ahead with a combination therapy of high pull headgear and fixed functional appliance therapy as she had an increased maxilla and decreased mandible with vertical growth pattern. Headgear was also used for unilateral distalization of Class II side by varied forces. Posttreatment cephalometric assessment showed the catch-up growth of mandible. Mandible was increased in length by 4 mm, but the maxillary length remained the same. In the study of Franchi et al.,[11] Forsus FRD had a greater skeletal effect on the maxillary structures by restraining the sagittal advancement of the maxilla, but the effects of the mandible were mainly at the dentoalveolar level, with a large amount of mesial movement of the lower incisors (with its proclination) and first molars. In our patient also we were able to notice moderate dentoalveolar changes, but the combination of headgear had resulted in improved skeletal effects. The posttreatment lower incisor inclination values showed that they were controlled from unwanted proclination. Thus, a Class I skeletal pattern was achieved in this case mainly due to dentoalveolar changes, favorable mandibular growth and maxillary restraint as a consequences of these growth modulation appliances.
A Class III molar finish is a viable option, but the somewhat awkward intercuspation of the mandibular first molar with two maxillary premolars and the fear of long-term stability make the orthodontist cautious about this option. According to Hisano and Soma,[12] masticatory efficiency is not severely reduced in a Class III molar relationship. In addition, Bakke[13] ascribes the occlusal force more to the number and quality of occlusal contacts than to the sagittal relationship between the posterior teeth. Farret et al.[14] presented a case series of 3 patients with 13–14 years follow-up finished in Class III molar and Class I canine relation. Based on his clinical examples and related literature, he concluded that Class III molar finish is a viable option provided proper diagnosis and treatment planning is done. A 2 years follow-up in our patient showed that the Class III molar finish was stable without any signs of relapse. The patient was also happy and comfortable with the occlusion. Most of the time Class II Subdivision cases shows midline shift. Cassidy et al.[1] in their study on Class II subdivision explained about the difficulty of complete midline correction. In this case, we were able to achieve a reasonable midline.
Conclusion
An alternate treatment approach of an adolescent Class II patient is reported. The case was unique in its single arch extraction of lowers, unilateral distalization with head gear, growth modulation with head gear and forsus and finishing the case in a Class I canine and Class III molar relationship. The results were stable in 3 years follow up.
Acknowledgment
We would like to thank Dr Akhter Husain for his immense support and guidance and Dr Faizan Ahmed Khan for helping with the biomechanics part of the article.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Classification and treatment of class II subdivision malocclusions. Am J Orthod Dentofacial Orthop. 2014;145:443-51.
- [Google Scholar]
- Quantitative analysis of the orthodontic and orthopedic effects of maxillary traction. Am J Orthod. 1983;84:384-98.
- [CrossRef] [Google Scholar]
- Growth and treatment changes in patients treated with a headgear-activator appliance. Am J Orthod Dentofacial Orthop. 2002;121:376-84.
- [CrossRef] [PubMed] [Google Scholar]
- High-pull headgear versus cervical traction: A cephalometric comparison. Am J Orthod. 1972;62:517-29.
- [CrossRef] [Google Scholar]
- Stability of class II, division 1 treatment with the headgear-activator combination followed by the edgewise appliance. Angle Orthod. 2004;74:594-604.
- [Google Scholar]
- Response to activator treatment in class II malocclusions. Am J Orthod. 1985;88:242-51.
- [CrossRef] [Google Scholar]
- The effect of orthodontic treatment on the concurrent development of the craniofacial complex. Am J Orthod. 1963;49:15-26.
- [CrossRef] [Google Scholar]
- Dental and orthopedic effects of high-pull headgear in treatment of class II, division 1 malocclusion. Am J Orthod Dentofacial Orthop. 1992;102:197-205.
- [Google Scholar]
- Effectiveness of comprehensive fixed appliance treatment used with the forsus fatigue resistant device in class II patients. Angle Orthod. 2011;81:678-83.
- [CrossRef] [PubMed] [Google Scholar]
- Energy-based re-evaluation of Angle’s class I molar relationship. J Oral Rehabil. 1999;26:830-5.
- [CrossRef] [PubMed] [Google Scholar]
- Strategies to finish orthodontic treatment with a class III molar relationship: Three patient reports. World J Orthod. 2009;10:323-33.
- [Google Scholar]




