

Translate this page into:
Clinical and molecular factors associated with external apical root resorption by orthodontics: Umbrella review
 , Daniela Alzate Rivera2, Ana María Salgado Amaya1, Juan C. Hernandez3,4, David Arboleda Toro2, Natalia Vélez Trujillo1
, Daniela Alzate Rivera2, Ana María Salgado Amaya1, Juan C. Hernandez3,4, David Arboleda Toro2, Natalia Vélez Trujillo1

*Corresponding author: Eliana Lucena Pineda Vélez, Professor, Endodontist, Faculty of Dentistry, Universidad Cooperativa de Colombia, Medellín, Colombia. Faculty of Dentistry, Medellín, Colombia. eliana.pineda@campusucc.edu.co
-
Received: ,
Accepted: ,
How to cite this article: Pineda Vélez EL, Alzate Rivera D, Salgado Amaya AM, Hernandez JC, Arboleda Toro D, Vélez Trujillo N. Clinical and molecular factors associated with external apical root resorption by orthodontics: Umbrella review. APOS Trends Orthod. 2024;14:214-24. doi: 10.25259/APOS_176_2022
Abstract
The objective of this study was to analyze the available evidence on external apical root resorption (EARR) due to orthodontic movement to identify clinical and molecular factors associated with this condition. An umbrella review that included systematic reviews and meta-analysis was performed. Four databases were used (PubMed, Science Direct, Scopus, and Cochrane), and critical evaluation following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) and admeasurement tool to assess systematic reviews (AMSTAR-2) guidelines were carried out. The study protocol was registered in PROSPERO (International prospective register of systematic reviews, CRD42020198971). One hundred and twenty-four papers were eligible for this investigation. After exclusion by title and abstract, 10 papers (four systematic reviews and six meta-analyses) were included in the study. Guideline AMSTAR-2 was applied, and evaluation was performed using the PRISMA guideline. Factors such as female gender, adulthood, conventional fixed orthodontic treatment, heavy, continuous, and prolonged loads, intrusive movements, and anterior superior teeth with abnormal roots increase the risk of developing this condition. At the molecular level, some biomarkers, such as interleukins (IL) I-1B, I-6, I-4, and dentin phosphoprotein, are significant to reach an early diagnosis of external root resorption (ERR), especially the gene of polymorphism IL-1B (+3954), which is the most important predictor of this condition in patients under orthodontic treatment. Clinical and molecular factors respond to individual characteristics that must be identified to define the risk of developing EARR. Cone-beam computed tomography is the most accurate tool to evaluate the dimension of this condition. Prolonged treatments must be avoided, and immunoassays to analyze proteins in the gingival crevicular fluid should be included to reach an early diagnosis.
Keywords
Orthodontic
Root resorption
Gingival crevicular fluid
Biomarkers
Cytokines

INTRODUCTION
External apical root resorption (EARR) is one of the undesired biological effects of an orthodontic treatment.[1-3] Permanent loss of root structure is originated by excessive pressure, which leads to capillary collapse, reduction in blood flow, and override of the repair capacity of supporting tissues. These, in turn, lead to the formation of necrotic areas, known as hyaline zones, and activation of the inflammatory response, activating cellular and molecular mechanisms that promote EARR.[1,2,4-7]
Formation of hyaline areas during orthodontic treatment is unavoidable, but the incidence and severity of EARR are variable,[7-9] ranging from 26% to 100% as a function of biological, mechanical, and molecular factors, as the orthodontic movements are not the only factor that influences the onset of EARR.[7,10-13]
Different investigative approaches associate the following factors with a risk of developing EARR: age, gender, nutrition status, medication, systemic diseases, genetics, oral habits, malocclusion, tooth type, root morphology, history of dental trauma, previous orthodontic treatments, pulp vitality, infections, and inflammations are the most relevant biological factors.[2,3,6,11,14-18] Mechanical factors include the type of orthodontic appliances, orthodontic movement type, extractions, treatment time, and level of force magnitude.[6,19-27]
In addition, several biomarkers are related to the progress of EARR as a response to the orthodontic dental movement. Tissue tension generates tissue structural reorganization that releases neurotransmitters, growth factors, and cytokines, which have been attempted to study in-depth by analyzing the gingival crevicular fluid (GCF) that constitutes their releasing medium.[4,7,16,28-30]
Interleukins (ILs) are a complex of cytokines or low-molecular weight proteins that act as messengers and are physiologically secreted during the bone remodeling process in response to local stress (IL 1 β, IL-6, IL-7, IL-8, TNFα, IL-4, IL-10, IL-13, IL18, and Interferon-γ). The human genome codifies around 50 ILs and associated proteins. However, their association with EARR has not been conclusive, as data convergence has not been obtained. [7,8,10,16,29-34]
Diagnosis of EARR depends on early detection using routine radiographies. Root shortening begins between the second and fifth treatment weeks, but such change will be only visible in panoramic or periapical radiographs 3 or 4 months after the beginning of the orthodontic treatment. As these diagnostic aids underestimate the extension and produce negative false cases, the “gold standard” to diagnose EARR is cone-beam computed tomography (CBCT) because it accurately detects EARR without the existing limitations of other techniques. CBCT offers high-resolution structural analysis in the three planes of space and superimposition elimination, which provide high sensitivity and specificity in the identification of these types of conditions. [2,3,10,35-37]
Consequently, multiple clinical and orthodontic variables are associated with EARR. However, investigations show contradictory results, so careful analysis is necessary due to the high heterogeneity within original studies. Therefore, the main objective of this umbrella review was to analyze current evidence on orthodontically induced EARR to identify clinical and molecular factors associated with this condition.
MATERIAL AND METHODS
Design
An umbrella review was performed, beginning with a Population, Intervention, Comparison, and Outcome (PICO) question. A search strategy, inclusion criteria, and quality assessment with analysis of results were carried out. The study’s protocol was inscribed in the PROSPERO (International Prospective Register of Systematic Reviews) database (CRD42020198971).
Search strategy
Four electronic databases were used: PubMed, Science Direct, Scopus, and Cochrane. Systematic reviews and meta-analyses were identified using the terms orthodontic AND root resorption. The search was conducted, including articles from 2015 to 2020. To guarantee the exhaustivity of the protocol, an additional search using thesaurus terms and different word combinations was performed. This addition search included (((((“orthodontal”[All Fields] OR “orthodontic”[All Fields]) OR “orthodontical”[All Fields]) OR “orthodontically”[All Fields]) OR “orthodontics”[MeSH Terms]) OR “orthodontics”[All Fields]) AND ((“root resorption”[MeSH Terms] OR (“root”[All Fields] AND “resorption”[All Fields])) OR “root resorption”[All Fields]))))).
Inclusion and exclusion criteria
The PICO question used in the current work according to the main objective was as follows: (P) patients from different ages, genders, and ethnicities; (I) previous orthodontic treatment; (C) during orthodontic treatment; and (O) what clinical and molecular factors are associated with the incidence of EARR? Systematic reviews and meta-analyses performed on human subjects and published between 2015 and 2020 were included in the study. Exclusion criteria included other types of investigations (analytical, clinical, guidelines, review articles, letters to the editor, opinion articles, and observational studies).
The following inclusion criteria were applied to the title and abstract reading:
Search terms in the title or abstract
Publications in human subjects
Systematic review or meta-analysis.
Article selection
A total of 124 potentially eligible articles were identified. After duplicate elimination, 118 articles remained, which were then screened for title and abstract. One hundred articles were not related to the topic and were discarded. The remaining 18 articles were read and analyzed and eight were subsequently discarded because the studied population was animals. Ten articles (four systematic reviews and six systematic reviews with meta-analysis) were selected for data analysis and validation using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) and Admeasurement Tool to Assess Systematic Reviews (AMSTAR-2) guidelines. The flow of article selection is shown in [Figure 1].
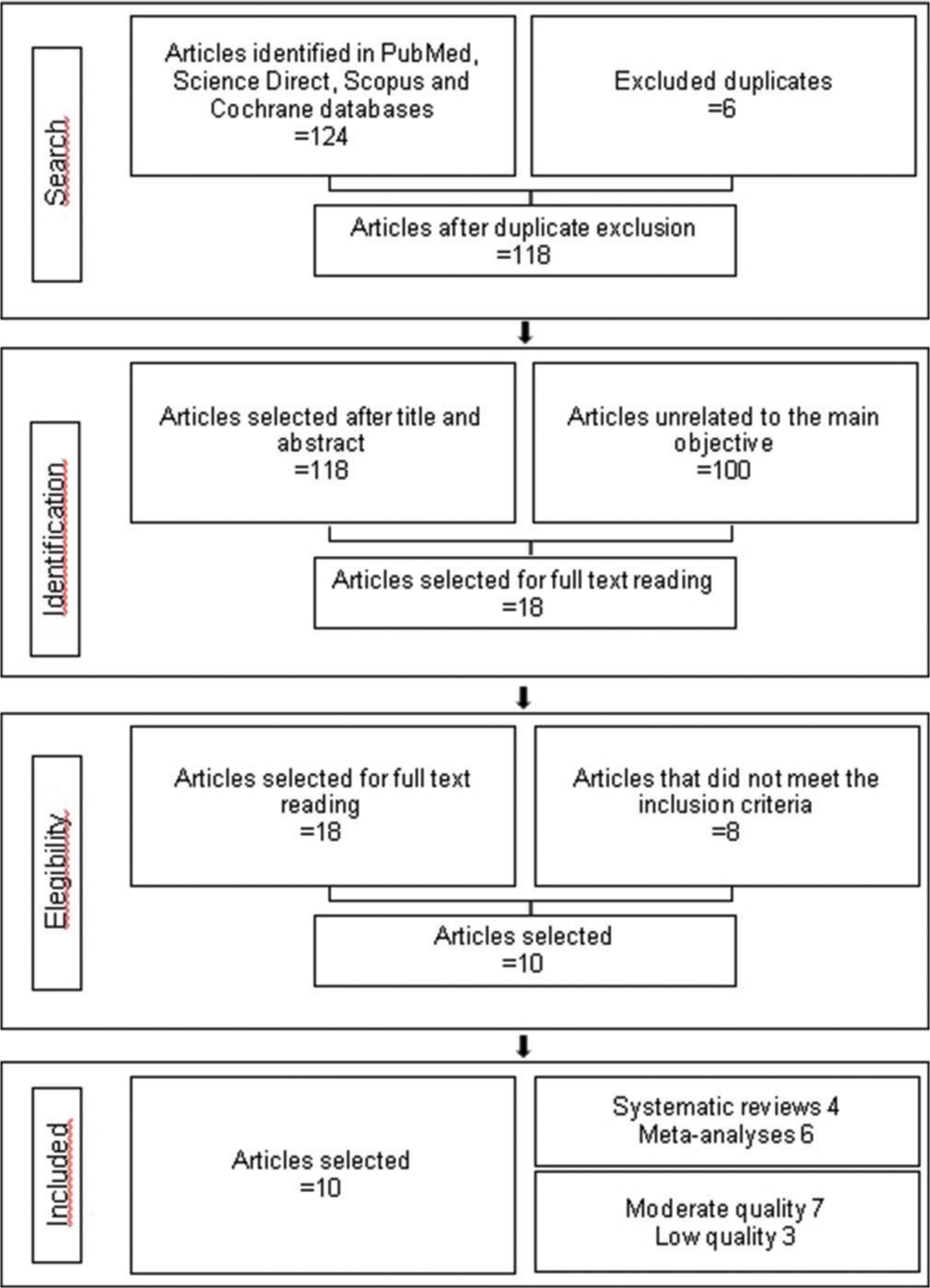
- Selection process of included articles.
Critical analysis
Three independent investigators assessed the validity of the selected articles. The PRISMA and AMSTAR-2 guidelines were used to verify their quality. A calibration process was then performed, and a 90% concordance index was obtained.
All the evaluations were performed using the PRISMA checklist, which applied the identification, screening, selection, and inclusion phases from the guidelines using 27 questions. Then, the AMSTAR-2 guideline was applied to assess the quality of the articles, and four levels of quality were obtained: high, moderate, low, and critically low.
The risk of bias, classified as low, high, or undefined, was assessed for every single article. In addition, whether heterogeneity was reported was also established. A descriptive analysis of the main characteristics of the included revisions was carried out.
RESULTS
Quality assessment of systematic reviews and meta-analyses
Quality assessment of the ten included articles in this umbrella review is shown in [Table 1]. According to the AMSTAR-2 guideline, seven studies were classified as having moderate quality and 3 as low quality. According to the PRISMA guideline, the articles with the best scores were investigations performed by Nowrin et al.[4], Gandhi et al.[2], Yi et al.[37], and Fang X. et al.[38]. Out of the 27 items included in the PRISMA checklist, only one article matches all the criteria and the score is over 18 points. Besides, nine out of ten articles report high heterogeneity and the remaining article does not report it.
Quality assessment instruments reported in these studies are the Grading of Recommendations, Assessment, Development, and Evaluations, which was used in three articles; the Strengthening the Reporting of Genetic Association Studies statement in two articles; the Risk of bias in Non-randomized Studies-of Interventions tool in 1 study, the Methodological index for non-randomized studies index in 1 work, the Quality Assurance International certification in 1 article, the PRISMA guideline in 1 article, and the Methodologic Scoring System adopted by Roscoe et al. in 2015 in the remaining article.[6]
| Article | Prisma guideline information qualification | Amstar-2 guideline general quality | Heterogeneity | Quality assessment instrument used in the study |
|---|---|---|---|---|
| Shifat A Nowrina[4] Saidi Jaafarb Norma Ab Rahmana Rehana Basric Mohammad Khursheed Alamd Fazal Shahida 2018 |
24/27 | Low | CC vs. TT: p-value: 0.020 I2: 60.136 CT vs. TT: p-value: 0.019 I2: 60.371 CC + CT vs TT: p-value: 0.032 I2: 56.520 CC vs. CT + TT: p-value: 0.000 I2: 76.917 |
(STREGA) statement |
| Arwa Aldeeri, Lulu Alhammad, Amjad Alduham, Waad Ghassan, Sanaa Shafshak, Eman Fatani 2018 [5] | 18/27 | Moderate | NR | The Methodologic Scoring System Adopted from Roscoe MG et al, 2015.9[6] |
| Marina G. Roscoe, Josete B. C. Meira, and Paolo M. Cattaneo 2015[66] | 21/27 | Moderate | Heterogeneity in study design and treatment protocols | PRISMA 2009 checklist |
| Francesco Tarallo, Claudio Chimenti, Giordano Paiella, Massimo Cordaro and Michele Tepedino 2019[7] | 20/27 | Low | Heterogeneity in the studies | Quality Assessment Instrument (QAI) |
| Vaibhav Gandhi , Shivam Mehta, Marissa Gauthier, Jijian Mu, Chia-Ling Kuo, , Ravindra Nanda and Sumit Yadav 2020[2] |
27/27 | Moderate | Heterogeneity among studies was modeled by a the effect of a random study in the mixed-effects meta-regression model | Methodological index for non-randomized studies (MINORS) |
| Aikaterini Samandara, Spyridon N Papageorgiou, Ioulia Ioannidou-Marathiotou, Smaragda Kavvadia-Tsatala, Moschos A Papadopoulos 2018[3] | 23/27 | Moderate | P<0.10 | Grading of Recommendations, Assessment, Development and Evaluations (GRADE) Downs and Black checklist |
| Scott Derek Currell, , Andrew Liaw, A y Alan Nimmo 2019[1] | 21/27 | Moderate | NR | Grading of Recommendations, Assessment, Development and Evaluations (GRADE) |
| Hatem A. Alhadainy, Carlos Flores, Jacqueline Crossman 2016[13] | 18/27 | Low | P<0,05; I2=69%). Because I2was 69%, a random effects model was performed that showed a funnel plot with asymmetric distribution of the included studies | Grading of Recommendations, Assessment, Development and Evaluations (GRADE) |
| Jianru Yi, Meile Li y Zhihe Zhao 2019[37] |
23/27 | Moderate | (I2> 50%) The hypothesis test was set at p<0.05 | STREGA statement |
| Xuanwei Fang, Rui Qi, Chufeng Liu 2019[38] | 22/27 | Moderate | Chi2= 17,14 df= 12 (P=0,14) I2= 30% |
Grading of Recommendations, Assessment, Development and Evaluations (GRADE) |
CC: Control, TT: Treated, STREGA: Strengthening the reporting of genetic association studies, PRISMA: Preferred Reporting Items for Systematic Reviews and Meta-Analysis, NR: Not reported
Cochrane evaluation of individual studies identified sources of bias [Table 2] and assessed the presence of a prism algorithm, the report of interobserver evaluation, and the presence of a funnel plot in each study. The results of this study showed that all investigations exposed the use of the prism algorithm, resulting in a low risk of selection bias. Assessment of interobserver concordance was reported in all articles, leading to a low risk of bias. Due to the presence of a funnel plot, only two studies showed a low risk of report bias, and it was undefined or unclear in the remaining articles as some doubts about the results arose.
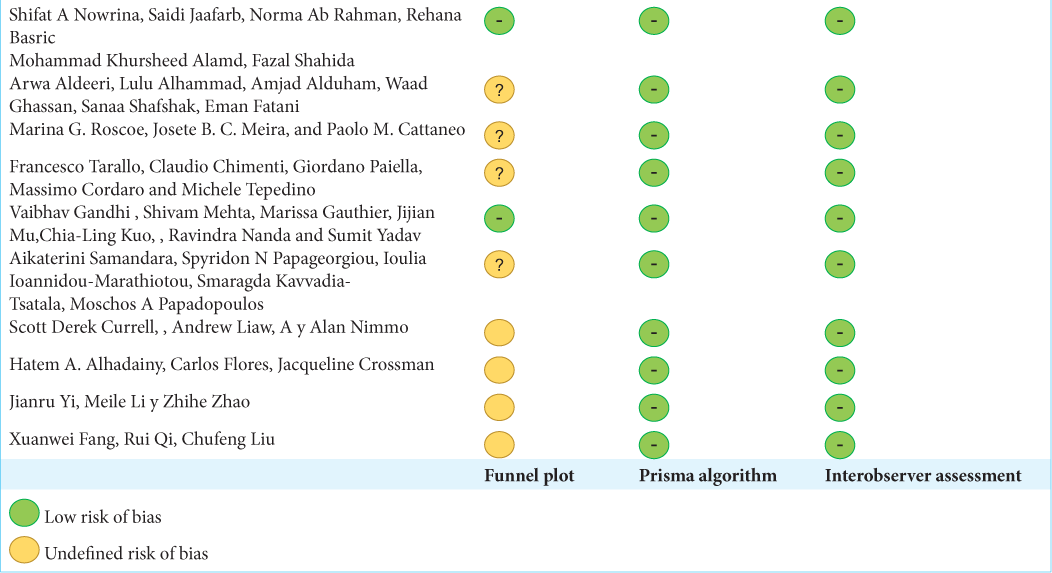 |
With the purpose of reducing systematic errors, possible bias in the included articles was identified. Due to the high variability among ethnic groups, a selection bias may be found in genetic studies, as genotypes vary according to ethnicity. Samples of fewer than 100 patients were considered a potential bias. The difference in precision among radiographies and measurement and quantification methods was also considered a measurement bias. The absence of control groups, lack of high-quality prospective studies, non-homogeneity at the GCF collection time, different methods to collect this fluid, and measurement of applied force magnitude were other biases.
Main characteristics of reports
The main characteristics of articles included in this umbrella review compared different clinical and molecular variables that increase the risk of developing EARR during the orthodontic treatment. Out of ten investigations, four were performed in Asia, two in North America, one in South America, two in Europe, and one in Oceania.
Most investigations are randomized controlled clinical trials performed in human subjects under orthodontic treatment of about to begin one. Sample size was established according to each investigation and most works only include 3D diagnostic aids. For qualitative studies (systematic reviews), the minimum number of included studies was 2, and the maximum was 30. For quantitative studies (meta-analysis), the minimum number of included studies was 3, and the maximum was 16.
As for age, the minimum age to participate in the studies was 8 years, and the maximum was 75 years. Only six papers reported gender information, and more females than males were included. Diagnostic aids ranged from lateral cephalograms, panoramic, occlusal radiographs, periapical radiographs, and scanning electron microscopy. However, 80% of the authors preferred the CBCT as the measurement method due to its high precision. Samples from GCF were obtained using filter papers, paper strips, and micropipettes, and analyses were performed using techniques such as Taqman, Ncoi sequencing, and enzyme-linked immunosorbent assay (ELISA) immunoassays, among others. Only two types of orthodontic appliances were reported (clear dental aligners or fixed orthodontic appliances). For the volumetric measurement of the EARR, the following methods were reported: linear measurements, radiometric, millimeters, and voxel 3D. Four studies classified EARR as light, moderate, and severe. As for biological factors, one study analyzed ethnicity and found a higher prevalence in Caucasian and Hispanic populations than in Asians. As for patient type (children, adolescents, or adults), the most severe form of EARR was found more frequently in adults than adolescents [Table 3]. Immunological factors were referred to as variables such as genetic polymorphism expression and the presence of cytokines, ILs, RANK, OPG, dentin phosphoprotein (DPP), dentin sialoprotein (DSP), and alkaline phosphatase (ALP), among other biomarkers. All these factors and the main conclusions are summarized in [Table 4].
| Article | Average age | Gender | Radiographies | Treatment type | Root resorption quantification method |
|---|---|---|---|---|---|
| Association between genetic polymorphisms and external apical root resorption: A systematic review and meta-analysis | 8.0-55.4 years | NR | Lateral cephalogram, panoramic, CBCT, occlusal, periapical | "Treatment type" confounding factor was not considered | Radiographic analysis |
| Association of Orthodontic Clear Aligners with Root Resorption Using Three-dimension Measurements: A Systematic Review |
8.3-33.7 years | NR | CBCT, micro computerized tomography | Orthodontic treatment with transparent aligners (Invisalign and ClearSmile®). Light load (25 g) and heavy load (225 g) | Volumetric measurement |
| Association of orthodontic force system and root resorption: A systematic review | 10.2-41.8 years | 66% females 43% males | Periapical | 12 split-mouth studies assessed the influence of load level on OIIRR in premolars. Except the study by Harry and Sims, the remaining studies compared a light (25g) with a heavy load (225g), light torque (2.5°) with heavy torque (15°), and light distal inclination (2.5°) with heavy distal inclination (15°) as the most studied, followed by intrusion | Volumetric measurements and histologic analyses |
| Biomarkers in the gingival crevicular fluid used to detect root resorption in patients undergoing orthodontic treatment: a systematic review | 9.0-44.0 years | 73% females 27% males | Panoramic | 2 split-mouth studies, one in canines and one in premolars. 5 clinical trials with control group. Studies with GCF collection during and after orthodontic treatment to verify the presence of ERR biomarkers | Low, moderate and severe; cytokine measurement with GCF collection |
| Comparison of external apical root resorption with clear aligners and pre-adjusted edgewise appliances in non-extraction cases: a systematic review and meta-analysis |
10.0-75.0 years | 65% females 35% males | Panoramic, periapical, CBCT | Treatment with Invisalign and Smart Track aligners and Roth and MBT prescriptions for fixed orthodontic treatment | Radiometric measurements in millimeters |
| Evaluation of orthodontically induced external root resorption following orthodontic treatment using cone beam computed tomography (CBCT): a systematic review and meta-analysis | 11,4 - 26,6 years | 37,7% males 62,3% females | CBCT | Fixed orthodontic treatment, anterior maxillary intrusion or rapid maxillary expansion | Changes in length and volume |
| Orthodontic mechanotherapies and their influence on external root resorption: A systematic review | 12,3 - 20, 9 years | NR | Computerized tomography, SEM, periapical, CBCT | 3 studies assessed continuous and intermittent forces with different force magnitudes and follow-up periods. All the studies used a split-mouth design with fixed orthodontic brackets bonded to the premolars | Volumetric measurement |
| Orthodontic-induced External Root Resorption of Endodontically Treated Teeth: A Meta-analysis | 12,8 - 34,5 years | NR | CBCT, periapical, panoramic, lateral cephalogram | Fixed orthodontic treatment on vital and non vital teeth | Linear measurement of the EARR |
| Root resorption during orthodontic treatment with self-ligating or conventional brackets: a systematic review and meta-analysis | 12 - 30 years | 40,6% males 59,4% females | CBCT, periapical | Self-ligation and conventional fixed orthodontic treatment | Volumetric measurement |
| Root resorption in orthodontic treatment with clear aligners: A Systematic Review and Meta-Analysis | 12- 58 years | 40% males 60% females | CBCT, periapical, panoramic | Fixed orthodontic treatment vs aligners | Volumetric measurement |
CBCT: Cone beam computed tomography, SEM: Scanning electron microscopy, NR: Not reported, GCF: Gingival crevicular fluid
| Category | Factor | Description | Article |
|---|---|---|---|
| Mechanical factors | |||
| Force magnitude | Under the same mechanical stress, many subjects exhibit low and some severe ERR | 1 | |
| there are positive correlations between ERR and continuous forces | 3 | ||
| there is a positive correlation between ERR and an increase in the orthodontic force magnitude regardless of force direction | 7 | ||
| Treatment duration | The higher the treatment time, the higher the root resorption | 3 | |
| a pause in dental movement is beneficial to reduce ERR | 3,7,10 | ||
| a reduction in root resorption was observed in patients who received orthodontic treatment in two phases | 7 | ||
| Movement direction or type | Buccal inclination was associated with ERR in the Bucco cervical and linguoapical regions | 3 | |
| buccal root torque was associated with ERR in the Bucco apical and palatocervical regions | 3 | ||
| distal inclination was associated with ERR in the distal aspect of the apical and middle thirds and in the mesial aspects in the cervical third | 3 | ||
| extrusion movement was associated with increased resorption on the distal surfaces | 3 | ||
| There are positive correlations between ERR and intrusive forces | 3.7 | ||
| Type of orthodontic device | Transparent aligners do not reduce the risk of developing ERR, although the incidence and severity might be reduced | 2.1 | |
| similar results are observed when patients are treated with light forces using aligners or brackets | 3 | ||
| teeth subjected to super elastic NITI arch wires show higher ERR | 3 | ||
| differences were not found in the prevalence or severity of ERR when straight-wire appliances were compared with standard appliances | 7 | ||
| class-II elastics is a risk factor for ERR | 8 | ||
| meta-analysis results suggest that self-ligating brackets are better than conventional brackets at protecting maxillary central incisors against ERR | 9 | ||
| Biologic factors | |||
| Age | No age predilection was found | 2 | |
| Race | ERR is higher in Caucasians and Hispanics than Asians | 2 | |
| Gender | Proportion of ERR cases was higher in females than males | 8 | |
| No predilection of ERR for males or females | 2 | ||
| Tooth type | The highest root resorption was found on the maxillary lateral incisors followed by maxillary central incisors and canines | 2,6,8 | |
| The highest ERR was observed in the anterior maxilla followed by the anterior mandible, posterior mandible and posterior maxilla | 6 | ||
| Root morphology | Root morphology (abnormal shape, long and narrow roots) is associated with ERR | 8 | |
| Provious extractions | Orthodontic treatment involving extractions are more associated with reduction in root size | 6 | |
| Dental extraction to resolve severe dental crowding may be considered a risk factor for ERR | 10 | ||
| Pulp vitality | An increase in ERR in endodontically treated teeth after orthodontic treatment was not observed | 8 | |
| No difference was found in the degree of ERR between endodontically treated teeth vs contralateral vital teeth | 8 | ||
| Endodontic treatment in males exhibited a significant increased ERR | 8 | ||
| Molecular factors | Expression of genetic polymorphisms | IL-1B (+3954) polymorphism is considered a promising gene to predict ERR | 1 |
| Patients who are homozygous for allele 1 of the IL-1B (+3954) gene have a 95% probability of developing ERR > 2mm | 1 | ||
| Cytokines | Levels of IL-4, IFN-γ and GMCSF are higher in light ERR cases | 4 | |
| Dentin matrix protein (DMP - 1) is not a useful biomarker because it is not possible to differentiate between its physiological and pathological activities | 4 | ||
| Dentin phosphoprotein (DPP) is a relatively useful biomarker for ERR diagnosis | 4 | ||
| RANKL concentration in the GCF is higher in patients with light and severe ERR | 4 | ||
| There are higher concentrations of DPP, DSP and IL-6 in patients with severe ERR | 4 | ||
| Overall alkaline phosphatase (ALP) activity increased with higher rates of tooth movement at 150 g of force | 4 | ||
| Cytokine levels are different depending on sampling sites and occurring time | 4 |
EARR: External apical root resorption, ERR: External root resorption, NITI: Nickel titanium, IL-1B: Interleukin-1beta, IFN: Interferon, GM-CSF: Granulocyte macrophage colony-stimulating factor, GCF: Gingival crevicular fluid, DSP: Dentin sialoprotein, DPP: Dentin phosphoprotein, DMP: Dentin matrix protein
DISCUSSION
Due to the absence of pathognomonic signs, EARR is casually detected in routine panoramic radiographs. However, underestimating its severity may lead to permanent loss of important root structure since other risks patients are subjected to from their biological background, their interaction with the environment, and factors related to the mechanics employed in orthodontic treatment are mostly unknown. Results presented in this umbrella review may be used as a foundation to develop more solid investigations on this topic.
In 2019, Currel et al.[1] analyzed the degree of root resorption in teeth subjected to orthodontic treatment considering mechanical factors such as type of device and orthodontic force magnitude and direction. It was found that continuous forces increase EARR regardless of magnitude and direction. Bracket type, ligation, and archwire sequence did not influence the severity of EARR.[1]
In 2019, Samandara reported that root shortening is significantly increased after orthodontic therapy and confirmed that heavy forces, extractions, and anterior teeth with abnormal root morphology are factors that increase the prevalence and severity of this condition. Similar results are reported by Fernandes stating that orthodontic therapy with extractions increases the risk of EARR by 70% and also considering other variables, such as increased overjet and long dilacerated roots.[3,39]
Harris et al.,[40] Barbagallo et al.,[27] Cheng et al.,[25] and Paetyangkul et al.[36] concurred that there is a directly proportional relationship between force and EARR and that the type of orthodontic movement is a significant mechanical factor as forces intensify on certain areas of the root according to the orthodontic action. For instance, pressure accumulates on the root apex during intrusion movements, thus increasing the risk of EARR in that zone. During extrusion movements, EARR is more frequently found on the cervical third toward the mesial and distal, which are the areas where pressure accumulates. However, it is important to mention that extrusion movements have 4 times lower resorption probabilities than intrusions.[41]
The type of appliance used in the orthodontic treatment is another variable that may influence the behavior of the root resorption process. Conventional brackets have been compared with self-ligating ones to determine whether significant differences are found between both bracket types in the incidence of EARR . Yi J. et al.[37] established that self-ligating systems may produce lighter forces during aligning movements since no ligature is needed, which may produce a protective effect for maxillary central incisors that are most vulnerable. However, Aras et al. concluded that it is not possible to suggest the superiority of one system over another due to the lack of investigations that follow solid methodologies to identify the exact differences between both systems. [37,42]
Regarding molecular factors, articles suggest that EARR has an important genetic component. Homozygous patients for allele 1 of IL-1B exhibit 5–6 times higher risk of developing EARR >2 mm than other groups. Data show that allele 1 in the IL-1B gene, known for reducing the production of IL-1 cytokine, significantly increases the risk of resorption. In addition, it has been suggested that EARR is a complex condition influenced by many different factors that are important to know to understand the contribution of environmental factors, such as habits and biomechanics.[4,43]
The search for EARR biomarkers intensified after finding dentin specific proteins (DPP-and DSP) that are byproducts found in the GCF, even though such proteins are not routinely released within the periodontal ligament space. ELISA immunoassays were analyzed by James et al. and later confirmed by Balducci et al.,[44,45] who identified and quantified these proteins in patients under orthodontic treatment. Dentin matrix protein-1 (DMP-1) was found in large quantities in the GCF as it is eliminated from bone and dentin during resorption processes. However, based on the results of the current work, DMP-1 is not dentin-specific, and its presence may be explained not only because of EARR but also due to the remodeling process during the orthodontic movement. As such, it is not an adequate biomarker of this condition as it is not possible to differentiate between its normal and pathological activities. Likewise, DSP protein was found in control groups, so no consensus is reached in the scientific literature to classify them as exact molecular biomarkers of EARR as they are not exclusive of dentin and are expressed in the osseous tissue. Their presence in the GCF may be explained by physiological remodeling processes, which are increased in patients under orthodontic treatment.[43,46]
Perinetti et al. assessed the activity of ALP in the GCF to evaluate its utility in the diagnosis of EARR during orthodontic treatment. These authors observed a significantly higher ALP activity in tension sites compared to compression zones, which increases as the force increases. However, this finding only reflects the biological activity of such compound in the periodontium during the dental movement and must be further studied, as proposed by Tarallo et al. in 2019.[7,33,47]
As for dental pulp status and root resorption, Alhadainy et al. and Huzar et al. concurred that the endodontic treatment does not seem to increase root resorption as no significant differences are found between vital and endodontically-treated teeth.[13,48]
CONCLUSION
Different factors or individual characteristics are paramount to define the risk of root resorption. The dental professional must carry out a comprehensive medical record of patients, including their background, to make the best treatment decision possible.
Biomarkers such as I-1B, I-6, I-4 ILs, and DPP are potential indicators of root resorption, and such molecules might be used to establish the individual risk and/or reach an early diagnosis of EARR to reduce the negative impact of this condition on orthodontic treatments.
Ethical approval
Institutional Review Board approval is not required.
Declaration of patient consent
Patient’s consent was not required as there are no patients in this study.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- Orthodontic mechanotherapies and their influence on external root resorption: A systematic review. Am J Orthod Dentofacial Orthop. 2019;155:313-29.
- [CrossRef] [Google Scholar]
- Comparison of external apical root resorption with clear aligners and pre-adjusted edgewise appliances in non-extraction cases: A systematic review and meta-analysis. Eur J Orthod. 2021;43:15-24.
- [CrossRef] [Google Scholar]
- Evaluation of orthodontically induced external root resorption following orthodontic treatment using cone beam computed tomography (CBCT): A systematic review and meta-analysis. Eur J Orthod. 2019;41:67-79.
- [CrossRef] [Google Scholar]
- Association between genetic polymorphisms and external apical root resorption: A systematic review and meta-analysis. Korean J Orthod. 2018;48:395-404.
- [CrossRef] [Google Scholar]
- Association of orthodontic clear aligners with root resorption using three-dimension measurements: A systematic review. J Contemp Dent Pract. 2018;19:1558-64.
- [CrossRef] [Google Scholar]
- Association of orthodontic force system and root resorption: A systematic review. Am J Orthod Dentofacial Orthop. 2015;147:610-26.
- [CrossRef] [Google Scholar]
- Biomarkers in the gingival crevicular fluid used to detect root resorption in patients undergoing orthodontic treatment: A systematic review. Orthod Craniofac Res. 2019;22:236-47.
- [CrossRef] [Google Scholar]
- Effect of orthodontic forces on cytokine and receptor levels in gingival crevicular fluid: A systematic review. Prog Orthod. 2014;15:65.
- [CrossRef] [Google Scholar]
- External apical root resorption concurrent with orthodontic forces: The genetic influence. Acta Odontol Scand. 2017;75:280-7.
- [CrossRef] [Google Scholar]
- Diagnosis of external root resorption in orthodontics. Rev Nacion Odontol. 2012;8:62-75.
- [Google Scholar]
- Root resorption, treatment time and extraction rate during orthodontic treatment with self-ligating and conventional brackets. Head Face Med. 2014;10:2.
- [CrossRef] [Google Scholar]
- Orthodontic-induced external root resorption of endodontically treated teeth: A meta-analysis. J Endod. 2019;45:483-9.
- [CrossRef] [Google Scholar]
- Root resorption during orthodontic treatment: causes and recommendations for action. Cient Dent. 2011;8:61-70.
- [Google Scholar]
- Evaluation of root resorption after comprehensive orthodontic treatment using cone beam computed tomography (CBCT): A meta-analysis. BMC Oral Health. 2018;18:116.
- [CrossRef] [Google Scholar]
- Effect of orthodontic force magnitude on cytokine networks in gingival crevicular fluid: A longitudinal randomized split-mouth study. Eur J Orthod. 2019;41:214-22.
- [CrossRef] [Google Scholar]
- Physical properties of root cementum: Part 17. Root resorption after the application of 2.5° and 15° of buccal root torque for 4 weeks: A microcomputed tomography study. Am J Orthod Dentofacial Orthop. 2011;139:e353-60.
- [CrossRef] [Google Scholar]
- A radiographic comparison of apical root resorption after orthodontic treatment with 3 different fixed appliance techniques. Am J Orthod Dentofacial Orthop. 2000;118:262-73.
- [CrossRef] [Google Scholar]
- Physical properties of root cementum: Part 22. Root resorption after the application of light and heavy extrusive orthodontic forces: A microcomputed tomography study. Am J Orthod Dentofacial Orthop. 2012;141:e1-9.
- [CrossRef] [Google Scholar]
- Physical properties of root cementum: Part 25. Extent of root resorption after the application of light and heavy buccopalatal jiggling forces for 12 weeks: A microcomputed tomography study. Am J Orthod Dentofacial Orthop. 2015;147:738-46.
- [CrossRef] [Google Scholar]
- Comparison of the intrusion effects on the maxillary incisors between implant anchorage and J-hook headgear. Am J Orthod Dentofacial Orthop. 2008;133:654-60.
- [CrossRef] [Google Scholar]
- Changes in the physical properties of human premolar cementum after application of 4 weeks of controlled orthodontic forces. Eur J Orthod. 2006;28:313-8.
- [CrossRef] [Google Scholar]
- A randomized clinical trial of the effectiveness of 0.018-inch and 0.022-inch slot orthodontic bracket systems: Part 3-biological side-effects of treatment. Eur J Orthod. 2019;41:154-64.
- [CrossRef] [Google Scholar]
- Physical properties of root cementum: Part 11. Continuous vs intermittent controlled orthodontic forces on root resorption. A microcomputed-tomography study. Am J Orthod Dentofacial Orthop. 2009;136:8.e1-8. discussion 8-9
- [CrossRef] [Google Scholar]
- Effect of continuous versus intermittent orthodontic forces on root resorption: A microcomputed tomography study. Angle Orthod. 2018;88:733-9.
- [CrossRef] [Google Scholar]
- Physical properties of root cementum: Part 18. The extent of root resorption after the application of light and heavy controlled rotational orthodontic forces for 4 weeks: A microcomputed tomography study. Am J Orthod Dentofacial Orthop. 2011;139:e495-503.
- [CrossRef] [Google Scholar]
- Physical properties of root cementum: Part 10. Comparison of the effects of invisible removable thermoplastic appliances with light and heavy orthodontic forces on premolar cementum. A microcomputed-tomography study. Am J Orthod Dentofacial Orthop. 2008;133:218-27.
- [CrossRef] [Google Scholar]
- Cellular, molecular, and tissue-level reactions to orthodontic force. Am J Orthod Dentofacial Orthop. 2006;129:469.e1-32.
- [CrossRef] [Google Scholar]
- Kinetics of interleukin-6 and chemokine ligands 2 and 3 expression of periodontal tissues during orthodontic tooth movement. Am J Orthod Dentofacial Orthop. 2012;142:494-500.
- [CrossRef] [Google Scholar]
- Longitudinal changes in gingival crevicular fluid after placement of fixed orthodontic appliances. Am J Orthod Dentofacial Orthop. 2011;139:735-44.
- [CrossRef] [Google Scholar]
- Effects of continuous and interrupted orthodontic force on interleukin-1beta and prostaglandin E2 production in gingival crevicular fluid. Am J Orthod Dentofacial Orthop. 2004;125:168-77.
- [CrossRef] [Google Scholar]
- A preliminary investigation of short-term cytokine expression in gingival crevicular fluid secondary to high-level orthodontic forces and the associated root resorption: Case series analytical study. Prog Orthod. 2017;18:23.
- [CrossRef] [Google Scholar]
- The monitoring of gingival crevicular fluid volume during orthodontic treatment: A longitudinal randomized split-mouth study. Eur J Orthod. 2012;34:109-13.
- [CrossRef] [Google Scholar]
- Lingual orthodontic treatment duration: Performance of two different completely customized multi-bracket appliances (Incognito and WIN) in groups with different treatment complexities. Head Face Med. 2014;10:46.
- [CrossRef] [Google Scholar]
- Periodontal parameters and cervical root resorption during orthodontic tooth movement. J Clin Periodontol. 2008;35:501-6.
- [CrossRef] [Google Scholar]
- Physical properties of root cementum: Part 16. Comparisons of root resorption and resorption craters after the application of light and heavy continuous and controlled orthodontic forces for 4, 8 and 12 weeks. Am J Orthod Dentofacial Orthop. 2011;139:e279-84.
- [CrossRef] [Google Scholar]
- Root resorption during orthodontic treatment with self-ligating or conventional brackets: A systematic review and meta-analysis. BMC Oral Health. 2016;16:125.
- [CrossRef] [Google Scholar]
- Root resorption in orthodontic treatment with clear aligners: A systematic review and meta-analysis. Orthod Craniofac Res. 2019;22:259-69.
- [CrossRef] [Google Scholar]
- Predisposing factors for external apical root resorption associated with orthodontic treatment. Korean J Orthod. 2019;49:310-8.
- [CrossRef] [Google Scholar]
- Apical root resorption in patients treated with comprehensive orthodontics. J Tenn Dent Assoc. 2001;81:30-3.
- [Google Scholar]
- Root resorption due to orthodontic treatment using self-ligating and conventional brackets: A cone-beam computed tomography study. J Orofac Orthop. 2018;79:181-90.
- [CrossRef] [Google Scholar]
- Genetic predisposition to external apical root resorption. Am J Orthod Dentofacial Orthop. 2003;123:242-52.
- [CrossRef] [Google Scholar]
- Evaluation of osteocalcin and pyridinium crosslinks of bone collagen as markers of bone turnover in gingival crevicular fluid during different stages of orthodontic treatment. J Clin Periodontol. 1998;25:492-8.
- [CrossRef] [Google Scholar]
- Biological markers for evaluation of root resorption. Arch Oral Biol. 2007;52:203-8.
- [CrossRef] [Google Scholar]
- Protein biomarkers of external root resorption: A new protein extraction protocol. Are we going in the right direction? Dental Press J Orthod. 2014;19:62-9.
- [CrossRef] [Google Scholar]
- Alkaline phosphatase activity in gingival crevicular fluid during human orthodontic tooth movement. Am J Orthod Dentofacial Orthop. 2002;122:548-56.
- [CrossRef] [Google Scholar]
- A comparison of the degree of external root resorption between endodontically treated and its vital contra lateral teeth after orthodontic treatment. IJFCM. 2019;3:27-31.
- [CrossRef] [Google Scholar]




