

Translate this page into:
Comparative evaluation of the position of incisive canal and its proximity to the maxillary central incisor roots with different incisor inclinations – A CBCT study


*Corresponding author: Shefali Gupta, Department of Orthodontics and Dentofacial Orthopedics, Pacific Dental College and Hospital, Udaipur, Rajasthan, India. shefaligupta611@gmail.ocm
-
Received: ,
Accepted: ,
How to cite this article: Gupta S, Kothari B, Garg K, Shah S, Singh N. Comparative evaluation of the position of incisive canal and its proximity to the maxillary central incisor roots with different incisor inclinations – A CBCT study. APOS Trends Orthod. doi: 10.25259/APOS_141_2024
Abstract
Objectives:
The aim of this study was to evaluate and compare the incisive canal position and its proximity to maxillary central incisor roots at different incisor inclinations.
Material and Methods:
A 105 CBCT samples have been then divided into three groups on the basis of U1-SN and U1-NA when traced on lateral cephalogram into normal, proclined, and retroclined. Several linear measurements have been made in the axial plane at three different levels, that are palatal opening, mid-root level, and apex, in relation to the incisive canal. Angular measurements were also made in the sagittal plane.
Results:
A significant difference was found between the proximity of the maxillary right and left central incisor to the incisive canal in the proclined and retroclined group at the mid-root level and at the apex. There has been a major variation between the angles developed by the incisive canal to the palatal plane in all three groups. A significant correlation was also found between the angle formed by the incisive canal to the palatal plane and the tooth’s long axis to the palatal plane.
Conclusion:
The proclined group exhibits the shortest distance between the incisive canal and the incisors, implying the need for meticulous planning in Class II Division 1 and bimaxillary protrusion cases. This planning is crucial when aiming for extensive retraction and intrusion to prevent any contact with an incisive canal, thus reducing the root resorption risk.
Keywords
Incisive canal
Maxillary central incisor roots
Cone-beam computed tomography

INTRODUCTION
Orthodontic treatment involves intricate considerations of tooth movement and its potential impact on surrounding anatomical structures. Maxillary incisors play a crucial role in both esthetics and function, necessitating careful planning to achieve optimal results. Conventionally, orthodontic treatment plans have been guided by the concept of the “Envelope of Discrepancy,” delineating the range of possible tooth movements. However, the advent of temporary anchorage devices has expanded treatment possibilities, necessitating a re-evaluation of movement limitations.
Anatomical structures such as the cortical plates, tongue, lips, and periodontal apparatus impose constraints on orthodontic tooth movement, necessitating careful consideration to avoid iatrogenic damage. While conventional 2D imaging has limitations, cone-beam computed tomography (CBCT) offers invaluable 3D insights, enhancing diagnosis and treatment planning, especially in cases involving impacted teeth or bone deficiencies.
Root resorption is a significant concern during orthodontic treatment and can be influenced by various factors. The maxillary cortical plate and the incisive canal are important landmarks, with their proximity increasing the risk of root resorption, especially following anterior retraction. According to a case report by Imamura et al.,[1] a female patient with Angle Class II division 1 malocclusion experienced major resorption of root in her upper right central incisor post-orthodontic treatment. On examination using CBCT, it was observed that the right central incisor root which has been in contact with the incisive canal, potentially contributing to the occurrence of root resorption. Pan and Chen[2] evaluated the risk of contact between the incisive canal and maxillary central incisor roots using mini-implants and found a higher risk of contact in subjects with a decreased anteroposterior distance between the incisive canal and maxillary central incisor roots.
Recent studies have shed light on the inter-relationship between the incisive canal and upper central incisor roots, with various factors such as skeletal pattern, facial profile, and sex influencing the proximity of these structures. However, the impact of incisor inclination on this relationship remains underexplored. In addition, research by Vardimon et al.[3] has emphasized the importance of understanding the anatomical variations of the incisive canal to minimize the risk of root resorption during orthodontic treatment.
Therefore, our study aims to fill this gap by evaluating and comparing the position of the incisive canal relative to upper central incisor roots at different inclinations by analyzing CBCT scans of patients with varying incisor inclinations.
MATERIAL AND METHODS
Retrospective research has been performed on the CBCT data of the maxillary anterior region, which were taken from the records of previous patients reported to the Department of Orthodontics and Dentofacial Orthopedics at Pacific Dental College and Hospital, Debari, Udaipur. The Institutional Review Board of Sai Tirupati University in Udaipur gave its approval to the study. No CBCT was taken just for research purposes. The size of the sample has been estimated by utilizing open EPI software. The estimation was based on Cho et al.[4] research, which revealed the need for 105 subjects in the current research.
The inclusion criteria were as follows: (1) age group 15– 25 years and (2) existence of pre-treatment lateral cephalogram and CBCT of good diagnostic quality. Exclusion criteria were as follows: (1) Impacted canine or any pathology present between the roots of the maxillary central incisor, (2) facial asymmetry, (3) history of previous orthodontic treatment, (4) large diastema, and (5) large midline shift.
Pre-treatment lateral cephalograms were manually traced and assessed to divide the subjects into three groups based on incisor inclination using two measurements, U1-SN and U1-NA, based on Steiner’s Analysis.
Three groups are divided as follows:
Group 1 NORMAL (U1-SN 100-108°, U1-NA 20-28°)
Group 2 PROCLINED (U1-SN >108°, U1-NA >28°)
Group 3 RETROCLINED (U1-SN<100°, U1-NA<20°)
Analysis was done on CBCT images using CS 3D Imaging Software (CareStream Health™, Rochester, New York).
The following measurements were made-In the sagittal plane, three levels were marked for measurements in an axial plane [Figure 1].
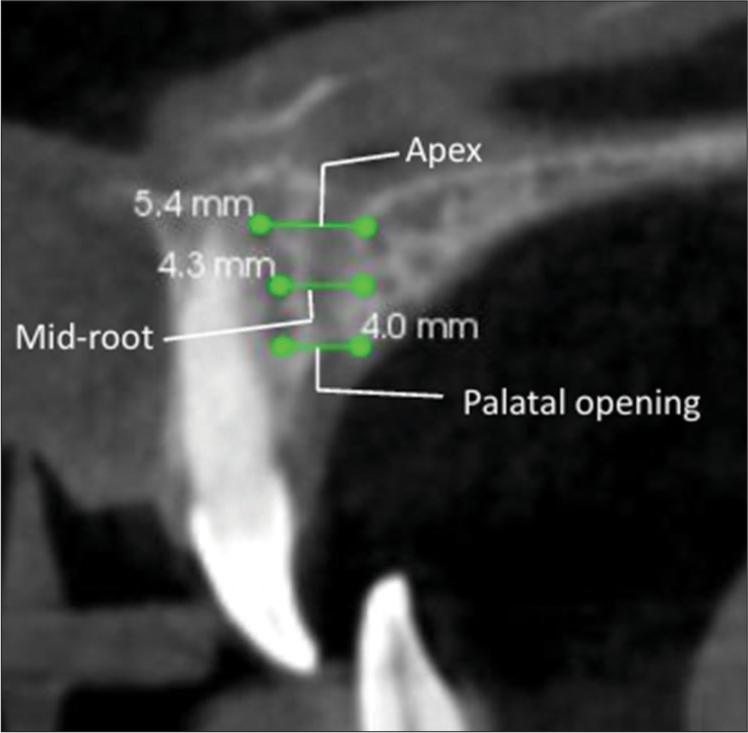
- Sagittal plane levels at palatal opening, mid root, and apex.
At the incisive canal palatal opening
At the mid-root level (between the incisive canal palatal opening to root apex)
At apex.
At all three levels of inter-root distance (IN), the distance between the right (IR) and left (IL) central incisor to the incisive canal and incisive canal width (D) was measured [Figure 2].
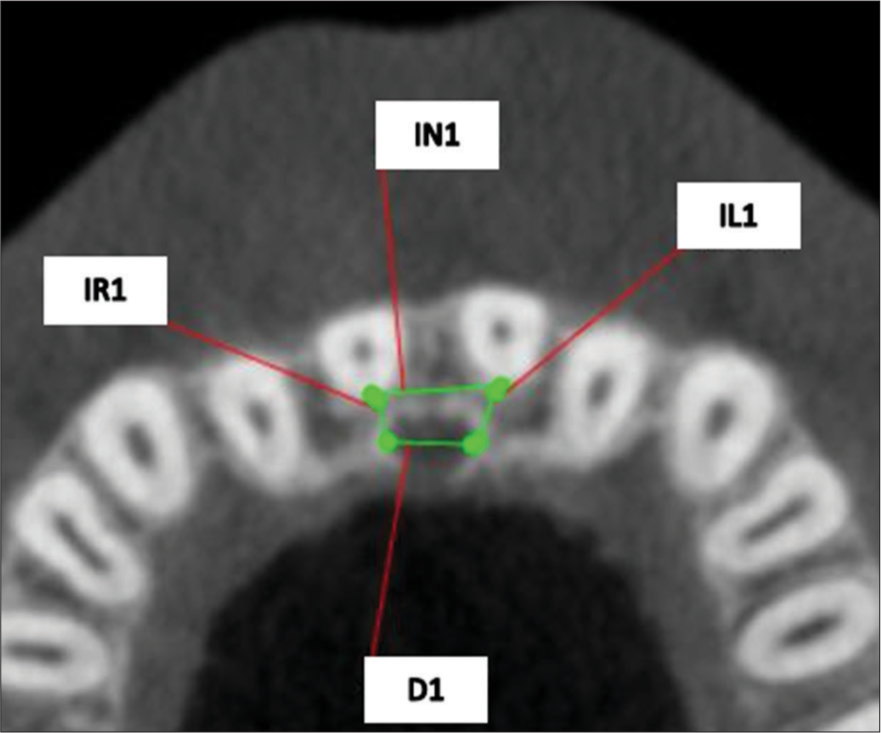
- Various measurements done in axial plane. IN: Inter-root distance, IR: Distance between incisive canal to right central incisor, IL: Distance between incisive canal to left central incisor, D: Width of incisive canal.
In the sagittal plane, the angle formed by the incisive canal to the palatal plane (A1), tooth-long axis to the palatal plane (A2), and incisive canal length (L) were measured [Figure 3].
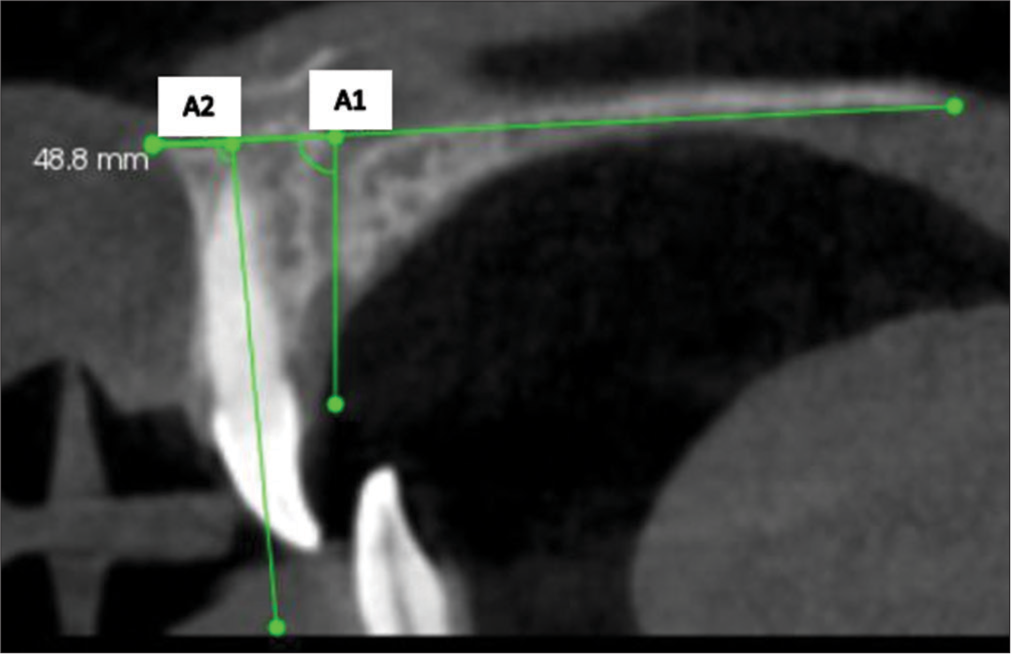
- Angular measurements. A1: Angle formed by palatal plane to incisive canal A2: Angle formed by palatal plane to long axis of the tooth.
Statistical analysis
The statistical analysis has been made by utilizing Statistical Package for the Social Sciences software. A descriptive statistical analysis was conducted for every parameter. Analysis of Variance, or one-way analysis of variance, was employed to compare the groups. Tukey’s post hoc test has been employed for conducting intergroup comparisons. Pearson correlation was also utilized to check the association among the angles formed with the palatal plane. At P < 0.05, the values appeared to be significant. A single examiner conducted each measurement.
RESULTS
The patient’s average age was 18.5 years in all three groups [Table 1]. The distance between the incisive canal and the right and left central incisor was not statistically significant when measured at the palatal opening. However, it was found to be significant at the level of mid-root and at apex [Figures 4 and 5]. The mean distance has been found to be more in retroclined group compared to proclined group. There have been no statistically significant variations in comparing the distance among the right and left central incisor with incisive canal in all three groups as well as overall subjects. The width of the incisive canal decreased from palatal opening to apex, but no statistically significant variations have been observed [Tables 2 and 3]. There was a statistically significant variation among the angle created by the incisive canal to the palatal plane in all three groups, with the proclined group having the least angle. A positive correlation was also found between the angle formed by the incisive canal to the palatal plane and the angle created by the tooth’s long axis to the palatal plane in proclined, retroclined, and overall subjects [Table 4]. The incisive canal length also changed substantially among the groups, with retroclined having the shortest length. There were no significant variations among the inter-root distance of all three groups, but it increased from palatal opening to apex.
| Normal | Proclined | Retroclined | |
|---|---|---|---|
| Age | 18.3±3.16 | 18.5±3.97 | 18.5±4.25 |
| Male | 18 | 14 | 21 |
| Female | 17 | 21 | 14 |
| Normal | Proclined | Retrolined | P-value | |
|---|---|---|---|---|
| IR1 | 3.26±0.94 | 3.67±3.79 | 3.02±0.87 | 0.488 |
| IL1 | 3.22±0.8 | 3.04±0.98 | 3.12±0.83 | 0.709 |
| D1 | 3.5±0.9 | 3.27±1.08 | 3.63±1.25 | 0.392 |
| IN1 | 7.37±1.33 | 7.22±1.7 | 7.32±1.16 | 0.9 |
| IR2 | 3.68±1.23 | 3.23±0.99 | 3.73±1.09 | 0.048* |
| IL2 | 3.71±1.22 | 3.18±1.17 | 3.98±1.08 | 0.016* |
| D2 | 3.32±0.97 | 3.2±0.98 | 3.43±1.31 | 0.669 |
| IN2 | 7.31±1.46 | 7.12±1.6 | 7.23±1.4 | 0.392 |
| IR3 | 4.03±1.67 | 3.48±1.29 | 4.39±1.45 | 0.004* |
| IL3 | 4.06±1.45 | 3.4±1.34 | 4.39±1.29 | 0.011* |
| D3 | 3.25±0.97 | 3.11±1.24 | 3.57±1.54 | 0.312 |
| IN3 | 7.29±1.62 | 7.13±1.64 | 7.3±1.86 | 0.899 |
| A1 | 75.25±7.59 | 71.0±8.19 | 76.7±10.66 | 0.023* |
| L | 11.76±2.82 | 11.7±2.43 | 10.0±2.51 | 0.007* |
P<0.05 – Significant Test applied – ANOVA. IN: Inter-root distance, IR: Distance between right central incisor to incisive canal, IL: Distance between left central incisor to incisive canal, A1: Angle formed between incisive canal to palatal plane, L: Length of incisive canal, D: Width of incisive canal, 1: Palatal opening, 2: Mid-root level, 3: Apex, *significant
| IN2 | IR2 | IL2 | D2 | IN3 | IR3 | IL3 | D3 | A1 | L | |
|---|---|---|---|---|---|---|---|---|---|---|
| Normal vs. Proclined | 0.854 | 0.212 | 0.144 | 0.892 | 0.925 | 0.278 | 0.114 | 0.895 | 0.118 | 0.995 |
| Normal vs. Retroclined | 0.976 | 0.982 | 0.588 | 0.897 | 0.999 | 0.565 | 0.575 | 0.549 | 0.766 | 0.015* |
| Proclined vs. Retroclined | 0.942 | 0.041* | 0.013* | 0.642 | 0.908 | 0.032* | 0.009* | 0.297 | 0.022* | 0.02* |
P<0.05 – significant Test applied – Tuckey’s post hoc. IN: Inter-root distance, IR: Distance between right central incisor to incisive canal, IL: Distance between left central incisor to incisive canal, A1: Angle formed between incisive canal to palatal plane, L: Length of incisive canal, D: Width of incisive canal, 1: Palatal opening, 2: Mid-root level, 3: Apex, *significant
| r-value | P-value | |
|---|---|---|
| Normal | −0.11 | 0.531 |
| Proclined | 0.46 | 0.006* |
| Retroclined | 0.45 | 0.007* |
| Overall | 0.40 | <0.001* |
Test applied – Pearson correlation, *significant
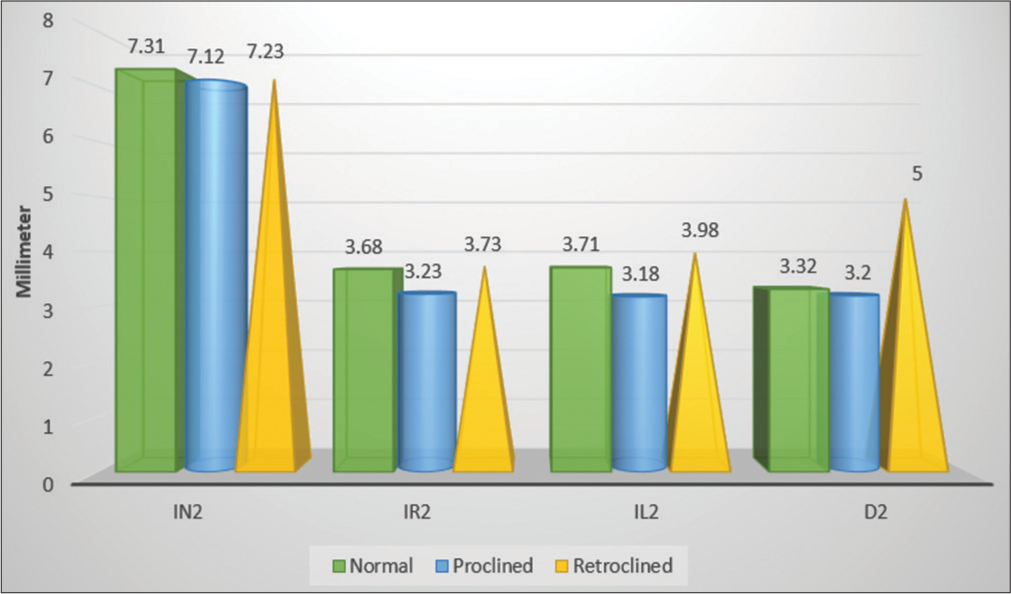
- Evaluation of inter-root distance (IN2), proximity of right (IR2) and left (IL2) maxillary central incisor roots to incisive canal and width of incisive canal (D2) at mid-root level in different incisor inclinations.
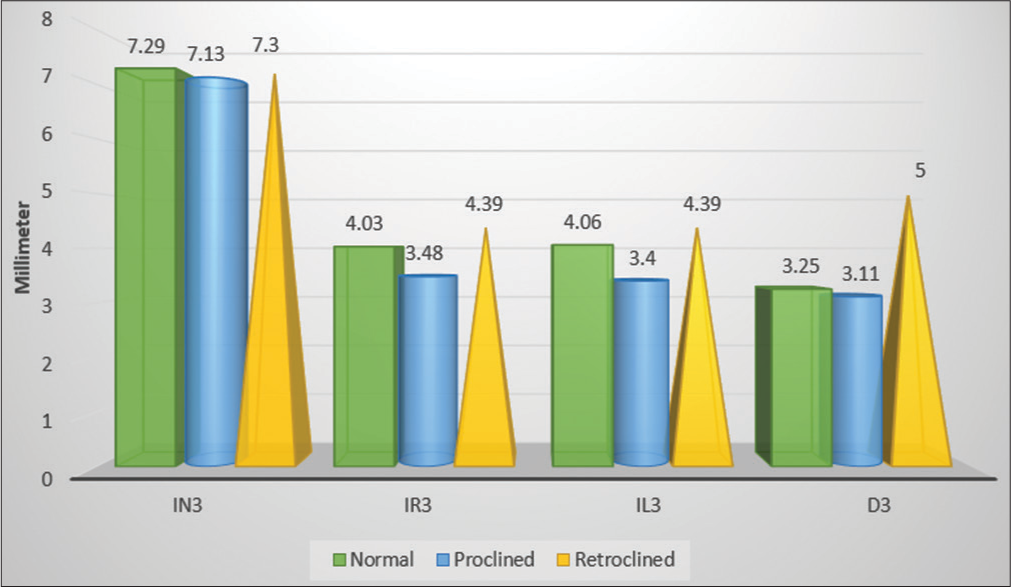
- Evaluation of inter-root distance (IR3), proximity of right (IR3), and left (IL3) maxillary central incisor roots to incisive canal and width of incisive canal (D3) at apex in different incisor inclinations.
DISCUSSION
In our study, we evaluated the distance between the incisive canal and the right and left central incisors at different incisor inclinations. We observed that at the palatal opening, there were no statistically significant differences in the distance from the incisive canal to the right and left central incisors across all three tooth inclinations. Similarly, Cho et al.,[4] who evaluated the relative position of the incisive canal to the maxillary incisor roots in individuals with Class I skeletal and dental malocclusion, also found no significant differences at the palatal opening.
Gull et al.[5] conducted a study on the Indian population with Class I skeletal and dental malocclusion using CBCT and reported findings at the palatal opening that were consistent with our results. Khurana et al.[6] studied subjects with Class I malocclusion in the Newark population and also found no significant difference in the proximity of the central incisors to the incisive canal at the palatal opening.
In contrast, Lobsang et al.[7] divided their subjects into three groups based on skeletal growth patterns and found a significant difference in the distance at the palatal opening, with the shortest distance observed in the Class II group. Although our study did not reveal significant variations, we did observe the shortest distance in the proclined group. It is important to note that Lobsang’s study categorized subjects based on skeletal malocclusion (ANB angle, witts appraisal) rather than incisor inclination. Given that Class II malocclusion includes two divisions, we assume that Lobsang et al.[7] likely focused on Class II Division 1 characterized by proclined anterior teeth. Proclined incisors can result in the roots being more centrally located within the alveolar bone, which could explain the shorter distance observed between the incisive canal and the central incisors in their study as well as in our study but not significantly in the present study.
At the mid-root level, we observed a significant variation in the distance between the incisive canal and the central incisors when comparing the proclined and retroclined groups, with the proclined group showing a shorter distance. This finding contrasts with the studies by Cho et al.,[4] Gull et al.,[5] and Khurana et al.,[6] where no significant difference was reported. This discrepancy may be attributed to the fact that their studies only assessed subjects with skeletal Class I malocclusion. In contrast, Lobsang et al.[7] found a significant difference, with the Class II pattern showing the shortest distance. We assume this might be due to the presence of proclined incisors in the Class II group, as their study categorized subjects based on skeletal malocclusion rather than incisor angulation, leading us to infer that the results could be related to the proclined group. Another important factor to consider is that the treatment planning of extraction is based on incisor inclination and soft-tissue consideration rather than skeletal malocclusion. Therefore, the division of subjects based on incisor inclination along with skeletal malocclusion is more beneficial rather than skeletal malocclusion alone.
Interestingly, Al-Rokhami et al.[9] examined the relationship between maxillary dentoalveolar protrusion in patients with different facial growth patterns and the position of the upper central incisor roots relative to the incisive canal. They found a significant difference based on facial pattern and sex. Although our study did not specifically stratify subjects based on facial patterns or sex, these factors likely influence the anteroposterior distance from the incisive canal to the maxillary incisors at the mid-root level.
It’s important to note that contact between the maxillary incisors and the incisive canal is often observed in cases involving enmasse retraction, such as in bimaxillary protrusion and Class II Division 1 malocclusion cases. In addition, factors like incisor torque should also be considered, as this can significantly impact the root movement, which, in turn, can affect the distance between the incisive canal and the central incisors. This was also stated by Kuc et al.[8] in his systemic review.
Previous studies by Khurana et al.,[6] Cho et al.,[4] Gull et al.,[5] and Al-Rokhami et al.[9] observed that the root apex was located farther from the midline plane compared to the most lateral border of the incisive canal. As a result, these studies did not investigate the “distance from the incisive canal to the apex of the upper central incisors.” However, in our research, we found significant variations in the anteroposterior distance between the incisive canal and the maxillary central incisor roots, with the proclined group showing a shorter distance than the retroclined group. Similarly, Lobsang et al.[7] found that Class II subjects had shorter distances, which we assume to be particularly relevant to Class II Division 1 malocclusion.
Ishii et al.[10] explored maxillofacial morphology concerning vertical and anteroposterior skeletal patterns and noted that the left central incisor was closer to the incisive canal, although no significant differences were found between males and females. While our study did not stratify patients according to sex, vertical growth pattern, or facial pattern, it is evident that these factors may also influence the anteroposterior distance between the incisive canal and the maxillary central incisors. This suggests that future research could benefit from considering these variables to better understand the variations in this distance.
In this investigation, we observed a significant variation in the angle formed by the incisive canal relative to the palatal plane, with the proclined group exhibiting the smallest angle, followed by the normal group and the retroclined group. In addition, we found a significant moderate positive correlation between the incisive canal angle to the palatal plane and the tooth axis to the palatal plane in proclined, retroclined, and overall subjects. However, a weak negative correlation was observed in the normal group. These findings align with a study by Linjawi and Margalani,[11] where CBCT was used to assess the incisor/palatal plane angle, incisive canal/palatal plane angle, palatal alveolar bone width at the apex, the width of the incisive canal, inter-root width at the apex, and the level of the incisive canal relative to the incisor apex. Their study also found a positive correlation between the angles of the incisive canal and the incisor to the palatal plane, indicating that as tooth angulation increases, so does the angulation of the incisive canal. This correlation suggests an increased risk of contact during retraction procedures, particularly in more proclined teeth.
Ongprakobkul et al.[12] further evaluated pre- and post-retraction CBCT scans and found that the association between the incisive canal’s angulation and the tooth’s angulation emphasizes the need for close monitoring of the distance between the incisive canal and maxillary central incisors in subjects undergoing anterior retraction. It is likely that the author is addressing Class II Division 1 malocclusion due to the inclusion criteria of upper premolar extraction, which is commonly performed in Class II Division 1 cases. This assumption is based on the fact that Ongprakobkul et al.[12] appear to have selected subjects based on the specific treatment modality used, which often involves upper premolar extractions in cases of Class II Division 1 malocclusion.
The incisive canal width has been calculated as the distance among the two most lateral points of the incisive canal where we found an insignificant difference, but the width decreased from palatal opening to apex.
Previous studies were done by Al-Rokhami et al.,[9] Cho et al.,[4] and Lobsang et al.[7] have measured two inter-root distances that are (1) the distance between the posterior-most point of upper incisor roots and (2) the distance among most medial points of incisor roots and where the posterior distance decreased from palatal opening to the apex and the medial distance increased from palatal opening to apex. Although our study focused on posterior distance but found no significant difference between the normal, proclined, and retroclined groups. Al-Rokhami et al.[9] found that the average, as well as lower facial groups, had more inter-root distance than the high facial angle. The thicker alveolar bone may lead to increased inter-root distance in brachyfacial or low-angle cases than in dolichofacial or high-angle cases.
As a result, it is important to pay close attention to proximity among the “incisive canal and the maxillary central incisors,” particularly in cases involving proclined teeth like Class II Division 1. Bimaxillary protrusion and in cases with high anchorage demand where mini-screw or mini-implant assisted retraction is carried out.
There are various limitations to the study that should be considered. First, the small number of samples can limit the generalization of the findings. In addition, unequal representation of male and female subjects limits the ability to understand potential differences based on age and sex fully. Further research with larger and more diverse participant groups is necessary to strengthen correlations and broaden the scope of understanding in this area.
CONCLUSION
There has been a significant difference between the distance of the incisive canal to the upper central incisor roots at the mid-root level and at the apex in proclined and reclined groups.
A moderate positive correlation between the angle formed by the incisive canal to the palatal plane and the long axis of the tooth to the palatal plane in proclined, retroclined, and overall subjects.
Class II Division 1 and bimaxillary protrusion cases need to be meticulously evaluated as they usually have proclined incisors, which can lead to shorter distance among incisive canal as well as upper central incisor roots that might lead to resorption of root in case of contact with incisive canal during intrusion and retraction.
Ethical approval
The research/study approved by the Institutional Review Board at Sai Tirupati University, Udaipur, Rajasthan, number STU/IEC/2022/129, dated October 20, 2022.
Declaration of patient consent
Patient’s consent not required as patients identity is not disclosed or compromised.
Conflicts of interest
There are no conflicts of Interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- Unilateral maxillary central incisor root resorption after orthodontic treatment for Angle Class II, division 1 malocclusion with significant maxillary midline deviation: A possible correlation with root proximity to the incisive canal. Korean J Orthod. 2020;50:216-26.
- [CrossRef] [PubMed] [Google Scholar]
- Contact of the incisive canal and upper central incisors causing root resorption after retraction with orthodontic mini-implants: A CBCT study. Angle Orthod. 2019;89:200-5.
- [CrossRef] [PubMed] [Google Scholar]
- Correlation between the axis of the central incisor, nasal floor, and depth of the anterior maxilla. Am J Orthod Dentofac Orthop. 1991;100:511-6.
- [CrossRef] [PubMed] [Google Scholar]
- Morphologic evaluation of the incisive canal and its proximity to the maxillary central incisors using computed tomography images. Angle Orthod. 2016;86:571-6.
- [CrossRef] [PubMed] [Google Scholar]
- Evaluation of morphologic features and proximity of incisive canal to the maxillary central incisors using cone beam computed tomography. IOSR J Dent Med Sci. 2018;17:46-50.
- [Google Scholar]
- Cone beam computed tomographic-based retrospective study on Newark population for the assessment of distance between incisive canal and maxillary central incisors: Clinical implications. Indian J Dent. 2020;31:175-9.
- [CrossRef] [PubMed] [Google Scholar]
- Incisive canal and its propinquity to maxillary central incisors in various sagittal growth patterns: A CBCT study. Int J Adv Res. 2023;11:337-47.
- [CrossRef] [Google Scholar]
- The assessment of the rank of Torque control during incisor retraction and its impact on the resorption of maxillary central incisor roots according to incisive canal anatomy-systematic review. J Clin Med. 2023;12:2774.
- [CrossRef] [PubMed] [Google Scholar]
- Proximity of upper central incisors to incisive canal among subjects with maxillary dentoalveolar protrusion in various facial growth patterns: A CBCT analysis. Angle Orthod. 2022;92:529-36.
- [CrossRef] [PubMed] [Google Scholar]
- Factors associated with the proximity of the incisive canal to the maxillary central incisor. Appl Sci. 2023;13:6899.
- [CrossRef] [Google Scholar]
- Relationship between maxillary central incisors and incisive canal: A cone-beam computed tomography study. Folia Morphol. 2022;81:458-63.
- [CrossRef] [PubMed] [Google Scholar]
- Morphometric and volumetric analysis of the proximity between the incisive canal and maxillary central incisors during anterior retraction: A retrospective cone-beam computed tomography study. Angle Orthod. 2023;93:159-67.
- [CrossRef] [PubMed] [Google Scholar]




