

Translate this page into:
Cone-beam computed tomography assessment of bone quality and quantity following laser-assisted orthodontic tooth movement: A randomized controlled trial


*Corresponding author: Farah Yousry Eid, Department of Orthodontics, Faculty of Dentistry, Alexandria University, Alexandria, Egypt. farahyousry66@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Eid FY, Alansari RA. Cone-beam computed tomography assessment of bone quality and quantity following laser-assisted orthodontic tooth movement: A randomized controlled trial. APOS Trends Orthod. 2024;14:99-108. doi: 10.25259/APOS_188_2023
Abstract
Objectives:
Low-level laser therapy (LLLT) has been widely implemented in the acceleration of orthodontic tooth movement (OTM). However, the impact of LLLT on the alveolar bone changes accompanying OTM has not been comprehensively addressed in a clinical trial. Hence, the objective of this investigation was to perform a three-dimensional (3D) assessment of the impact of LLLT on the changes in bone quality (bone density), and quantity (bone thickness and volume) during the canine retraction stage of orthodontic treatment.
Material and Methods:
Twenty patients requiring maxillary first premolars’ extraction followed by canine retraction were recruited for this split-mouth study. Before the commencement of canine retraction, the maxillary arch in each of the enrolled subjects was randomly split into an “experimental” side, and a “control” side. In the experimental group, LLLT was performed on days 0, 3, 7, 14, and then every two weeks until the completion of the research duration (12 weeks). The employed diode laser was of 980 nanometers (nm) wavelength and a dosage of 8 joules per square centimeter (J/cm2), in a continuous mode. Canine distalization was accomplished using nickel-titanium closed-coil springs, with a force of 150 grams (g). Pre-retraction and post-retraction cone-beam computed tomography was performed to assess bone quality and quantity, in terms of alveolar bone density, thickness, and volume.
Results:
A statistically significant reduction in bone density and volume was found following canine retraction (P < 0.05) with and without LLLT application. For the total bone thickness, a statistically significant decrease was observed at both the coronal and mid-root levels of the maxillary canine (P < 0.05), whereas an insignificant change was reported at the apical level (P > 0.05) in both the studied groups. Furthermore, insignificant differences were documented in all the measured outcomes between the experimental and the control groups (P > 0.05).
Conclusion:
With the employed parameters in the present study, LLLT does not positively influence the changes in neither bone quality (bone density) , nor bone quantity (bone thickness and volume) accompanying OTM. Moreover, a significant reduction in bone density, in bone thickness (coronal and mid-root levels), as well as in bone volume accompanies canine distalization in both groups.
Keywords
Low-level laser therapy
Three-dimensional
Cone-beam computed tomography
Canine retraction
Orthodontic tooth movement
Bone density
Bone volume
Bone thickness

INTRODUCTION
Orthodontic tooth movement (OTM) is a complex procedure that has been described as an accommodative biological response to an external force interfering with the physiological balance of the dentofacial structures.[1] Orthodontic mechanical stimuli lead to remodeling and re-organization of the periodontal ligament, the alveolar bone, and the gingiva in order for successful OTM to take place.[1]
The effects of OTM on bone density are not well understood. Decrease,[2] increase,[3] and no change in bone density around orthodontically treated teeth have all been reported.[4] This may be attributed to the different types and magnitudes of orthodontic forces, leading to different remodeling responses.[5]
Acceleration of OTM and shortening of the orthodontic treatment duration have been the focus of orthodontists and patients.[6] This is due to the possibility that prolonged orthodontic treatment could result in unwanted complications.[7-9] Therefore, various procedures have been developed to accelerate OTM[10,11] including low-level laser therapy (LLLT).[12]
LLLT has biostimulatory effects ; it increases bone cell proliferation, accelerates bone metabolism,[13] and improves the aggregation of osteogenesis markers, resulting in an increase in bone density.[14,15] It has been investigated for the clinical purposes of acceleration of OTM,[16] amelioration of treatment-related pain,[17] as well as alveolar bone repair and improvement of bone regeneration.[18] However, the outcomes of LLLT vary greatly with the variation of different treatment parameters, including wavelength, output power, and energy density.[15] Furthermore, the impact of LLLT on alveolar bone changes accompanying OTM is not known. Alterations in bone quality and quantity provide clinicians with valuable information regarding whether LLLT accelerates bone remodeling, and the stability of the clinical results.
Lately, cone-beam computed tomography imaging (CBCT) has been used for assessing bone mineral tissues.[19] Despite the availability of several other non-invasive methods for bone assessment, they present challenges and drawbacks. Digital image analysis of microradiographs,[20] for example, cannot accurately reproduce the three-dimensional (3D) bone tissue structure.[2] Another example is, computed tomography scans;[21] their excessive radiation dose makes them unsuitable for repeated scanning over a short period of time.[2] CBCTs, on the other hand, can yield sufficient image quality with a relatively low radiation exposure, together with providing superior diagnostic value in comparison to the two-dimensional imaging techniques. Therefore, CBCTs have become the tools of choice for the assessment of different changes in the alveolar bone.[22]
Bone quality is commonly assessed through bone mineral density (BMD) using Hounsfield units (HU),[4,23] whereas bone quantity is assessed by measuring bone thickness and/or bone volume. Alterations in bone quality and quantity could provide clinicians with valuable information regarding the bone alterations for comparative purposes, within or between patients.[24] Nevertheless, the accuracy of these comparisons is largely dependent on the manipulation of a consistent CBCT hardware, analysis software, and imaging operation.[25]
Therefore, the present investigation aimed to assess the impact of LLLT on bone quality (alveolar bone density [ABD]) and quantity (alveolar bone thickness [ABT] and volume [ABV]), in a 3D manner throughout the canine retraction stage of orthodontic treatment using CBCT. The null hypothesis was that LLLT does not induce significant improvements in neither alveolar bone quality nor quantity, during OTM.
MATERIAL AND METHODS
Study design
The study was a randomized controlled trial (RCT) with a split-mouth design, with one side being the experimental side, and the contralateral side being the control side.
Study subjects
Twenty patients (8 males, and 12 females) participated in the study, with the age ranging from 15 to 20 years (mean age = 18 ± 1.2 years). The sample size was computed to be 18 patients (36 sides) with an 80% power, and increased to 20 patients (40 sides) to compensate for possible drop-outs over the follow-up period.[26] It was calculated using MedCalc Statistical Software version 19.0.5 (MedCalc Software bvba, Ostend, Belgium; https://www.medcalc.org; 2019). Yoshida et al.[27] reported estimates of BMD at different time points that that were used to calculate mean (standard deviation [SD]) BMD at three months using an extrapolation equation. The calculated mean (SD) difference in BMD between irradiated and non-irradiated sides = 239.65 (30.29) mg/cm3 and 95% confidence interval (CI) = 223.99, 255.31.
Ethical approval has been granted by the Institutional Review Board of the Faculty of Dentistry (IRB: 00010556–IORG: 0008839). Manuscript Ethics Committee number 0631– 02/2023. Patients were recruited from the outpatient clinic in the Department of Orthodontics. Consecutive subjects with the following inclusion criteria were recruited: (1) An indication for extraction of the maxillary first premolars, (2) absence of systemic and or chronic conditions, (3) no former orthodontic treatment, and (4) satisfactory oral hygiene and periodontal health. All subjects signed written informed consents after being thoroughly informed about the procedure and their rights. This study was conducted in accordance with the ethical principles of the Declaration of Helsinki.
Patients’ preparation
Recruited participants were prepared for fixed appliance treatment. The medical and dental history were documented, along with gathering customary orthodontic records (intraoral and extraoral photographs, radiographs, and dental models). Oral hygiene reinforcement was also confirmed before the initiation of orthodontic treatment. Fixed straight wire appliances with Roth prescription, and 0.022” × 0.028” slots were bonded in all patients. Subsequently, they were referred for extraction of the maxillary first premolars. Leveling and alignment were then commenced and considered achieved when a 0.016” × 0.022” stainless steel archwire was engaged passively in all the bracket slots of the maxillary teeth.
Randomization
As per the study’s split-mouth design, one side of the maxilla in each patient was randomly assigned to be the “experimental” side, whereas the other side was assigned to be the “control” side using a computer-generated randomization code (Microsoft, Inc, Redmond, WA, USA).
Canine retraction
Canine retraction on the experimental and control sides was accomplished by closed-coil springs made of nickel-titanium (NiTi), bilaterally extending between the hooks on the canine bracket and on the molar tube, with 150 g of force being applied, as assessed using a force gauge. The employed force was inspected every three weeks. Pre-retraction and post-retraction CBCTs were acquired for all the enrolled participants.
Low-level laser administration
A diode laser (Wiser; Doctor Smile-Lambda Spa, Brendola, Italy) was administered to emit continuous infrared (IR) radiation with a power output of 100 mW, and a wavelength of 980 nm. The plane wave optical fiber (AB 2799; Doctor Smile-Lambda Spa, Brendola, Italy) released a beam spot size of 1 cm2 using the flat top handpiece. The experimental side was irradiated by deploying the optical fiber tip against the middle third of the maxillary canine root, where the irradiation could also extend to the entire root length. Moreover, the flat top handpiece was held at a 1.5 cm distance, as per manufacturer instructions, for 8 seconds [Figure 1]. The total energy density administered per episode was 8 J/cm2 (1 J/cm2/s). Precautions to laser implementation were taken in advance, where protective eyewear that had been supplied by the manufacturer specific for the employed wavelength, had been used by the patient as well as the operator.

- The optical fiber tip of the laser device held against the maxillary canine root, at a 1.5 cm distance, as per manufacturers’ recommendation.
Each participant was treated on the experimental side with LLLT in the above-described manner, on days 0, 3, 7, 14, and every two weeks thereafter, over the 12-week research duration. As a blinding measure for the participating subjects, the laser beam was positioned passively against the control sides, yielding a placebo effect. However, the nature of the intervention precluded blinding of the operator at this stage. A flowchart illustrating the research design is represented in [Figure 2], summarizing the procedures of the study.

- Research design flowchart summarizing the study procedures. CBCT: Cone Beam Computed Tomography, LLLT: Low-level laser therapy, NiTi: nickel-titanium, ABD: alveolar bone density, ABT: alveolar bone thickness, ABV: alveolar bone volume.
Outcome measurements
All the measured alveolar bone changes over the 12-week observational period were assessed from the pre- and post-canine retraction CBCT scans of the maxillary arch only to limit the radiation exposure. CBCTs over the given study period are also justified by their low radiation dose resulting from the relatively small field of view (FOV) employed.[12,28,29] The CBCTs were acquired using the same +CBCT machine (J. Morita R100 Cone beam 3D Imaging System; MFG Corp., Kyoto, Japan). The FOV of the scan was 100 × 50 mm (Width × Height). The volumes were reconstructed with a 0.160 mm isometric voxel size. Furthermore, the voltage of the tube was 90 Kilovoltage peak (kVp) and 8 mA, with an exposure time of 20 s.
The following measurements were obtained on both sides of the mouth in each patient using different modules on the OnDemand3D™ App software (Cybermed Inc., Seoul, Korea).
ABD
The ABD was measured through the 3D Module of the OnDemand3D™ App. CBCT area sections were selected approximately 2 mm from the alveolar crest, with an axial slice thickness of 2.5 mm. Gray scale density values or HUs were then measured at four regions around the maxillary canine: mesial, distal, buccal, and palatal, and an average value was consequently calculated for assessment of overall ABD surrounding each maxillary canine root [Figure 3].
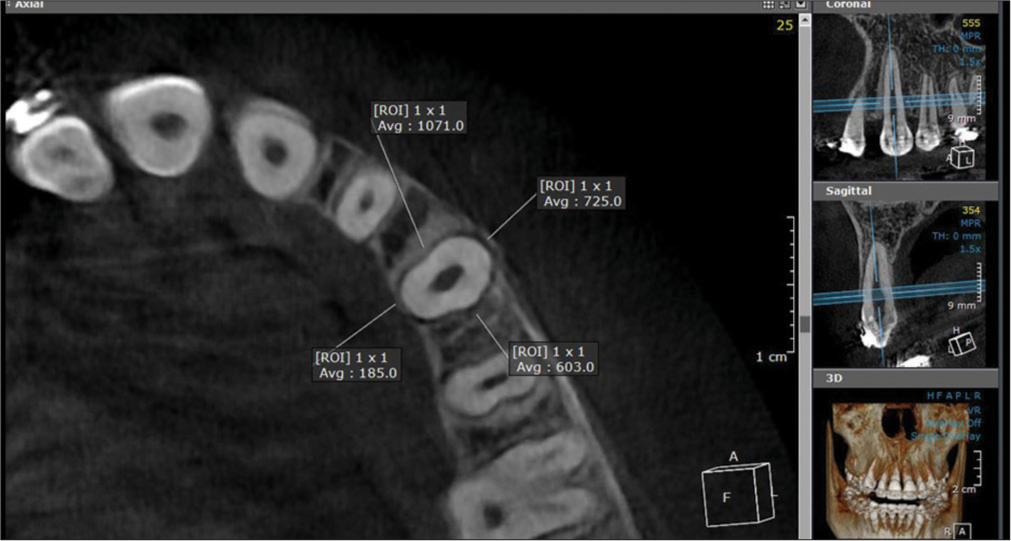
- Evaluation of alveolar bone density from cone-beam computed tomography area sections, 2 mm from the alveolar crest. Grey scale density values were measured at four regions around the maxillary canine: mesial, distal, buccal, and palatal (3D Module, OnDemand3D™ App software). ROI: Region of Interest.
ABT
Utilizing the 3D Module of the OnDemand3D™ App software, the focal trough was adjusted to allow the labiolingual slicing/sectioning of the maxillary canine parallel to the long axis of the root, with an axial slice thickness of 0.01 mm. The buccal bone thickness (BBT) and the palatal bone thickness (PBT) were measured at three levels along the canine root, including the coronal, the mid-root, and the apical levels [Figure 4]. Both the BBT and the PBT were added together to calculate the total ABT at each of the assessed levels.
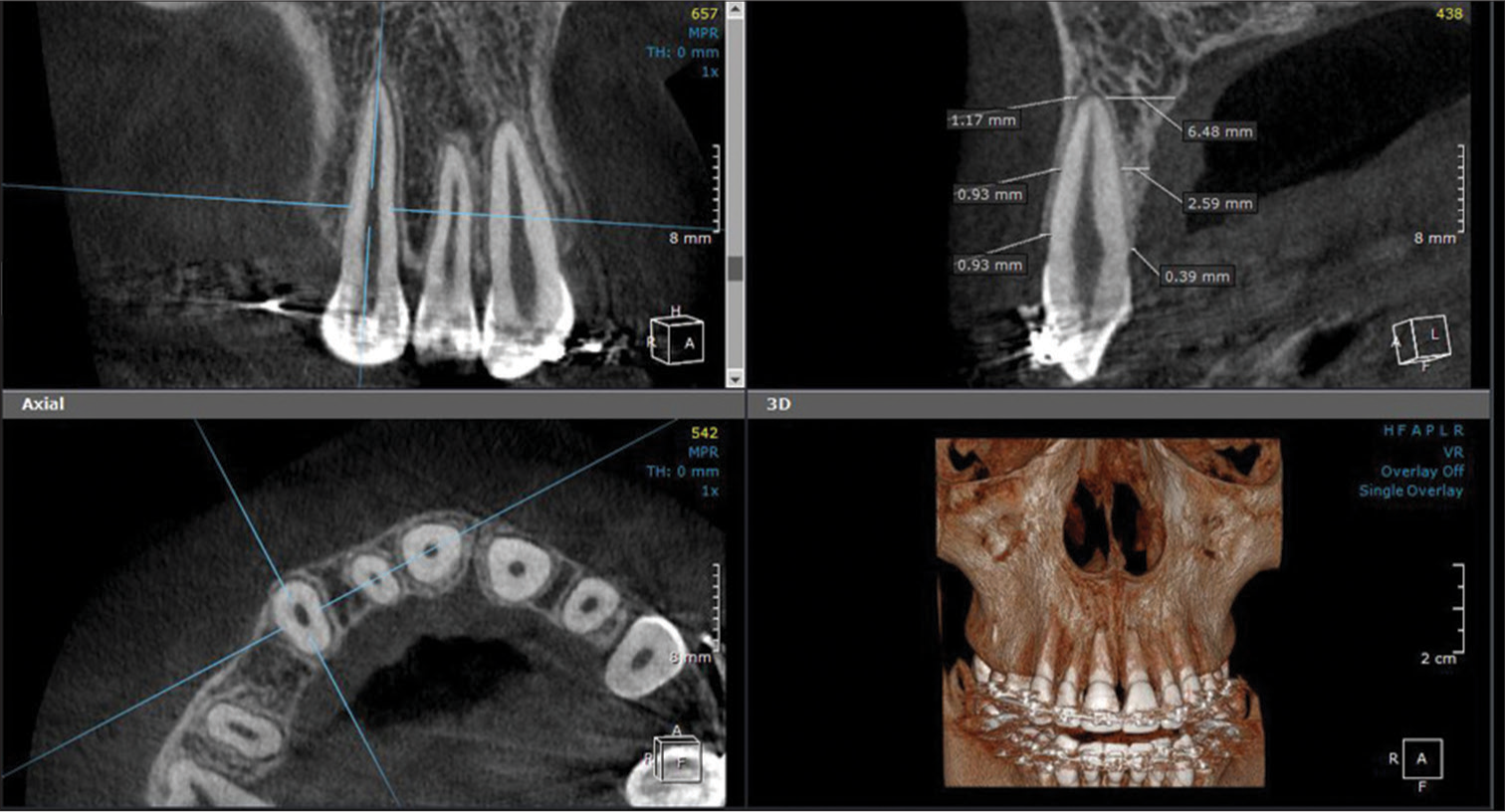
- Assessment of alveolar bone thickness on both the buccal and palatal sides of the maxillary canine, at three levels along the canine root: coronal, mid-root, and apical (3D Module, OnDemand3DTM App software).
ABV
Using the In2Guide Module of the OnDemand3D™ App software, the threshold was adjusted twice, once for the teeth alone, and another time for the teeth and the bone together, and the thresholds were set individually for each case. The two resultant exported 3D Model Stereolithographic files from each scan were subsequently imported into Materialise Magics 3D Print Suite software (Materialise, Belgium), where a cutting tool was manipulated to cut around the maxillary canine root border to an approximate depth of 2–3 mm parallel to the root surface [Figure 5]. A Boolean operation was then carried out for each canine, where the volume of the canine was subtracted from the overall volume of the cut area to determine the bone volume solely. This calculation was automatically performed by the employed software.
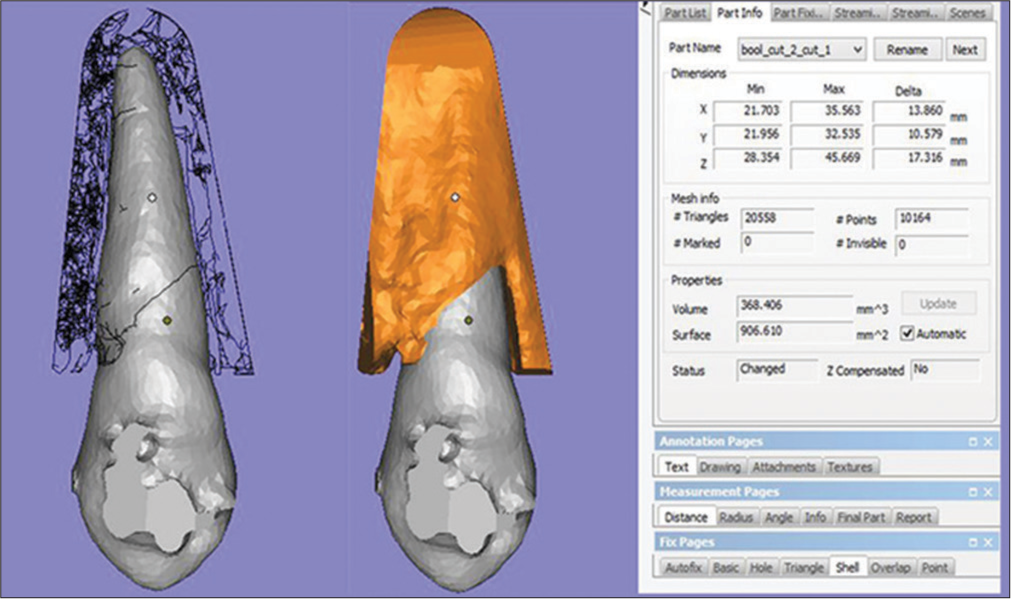
- Measurement of alveolar bone volume (ABV) after cutting at a depth of 2–3 mm around the canine root border. A Boolean operation was then carried out for calculation of ABV (Materialise Magics 3D Print Suite software).
Operators and a statistician were blinded to the experimental and control sides during measurements and data analysis, respectively.
Intra-examiner and inter-examiner reliability
At first, one researcher performed all the measurements. The same researcher and another calibrated independent researcher repeated the whole analysis on nine patients selected arbitrarily two weeks later to test intra- and inter-examiner reliability. The Intraclass Correlation Coefficient (ICC)[30] ranged between 0.89 and 0.98, indicating excellent reliability.
Statistical analysis
Normality was checked for all variables using descriptive statistics, plots (Q-Q plots and histogram), and normality tests. All the data showed normal distribution, so means and SDs were calculated. Percent change was calculated using the following equation:
Comparisons between the experimental and control sides and between pre- and post-retraction values were executed using paired samples t-test, with the calculation of mean difference and 95% CIs. Significance was set at P < 0.05. Data analysis was done using IBM Statistical Package for the Social Sciences SPSS for Windows (Version 26.0).
RESULTS
The initially recruited research sample (n = 20) successfully completed the study period of 12 weeks. Moreover, all the acquired CBCT scans were accounted for.
The effect of LLLT on ABD
Changes in ABD values in the two groups are presented in [Table 1]. There was a statistically significant reduction in the ABD values on both sides between pre- and post-treatment, with a 14.64 ± 2.93% reduction on the experimental side and a 15.05 ± 3.04% decrease on the control side. On comparing the ABD changes post-treatment between the two studied groups, insignificant differences have been found (P = 0.07).
| Experimental | Control | Difference | 95% CI | P-value 1 | |
|---|---|---|---|---|---|
| Mean (SD) | |||||
| Pre-retraction | 657.44 (119.91) | 647.30 (111.36) | 10.14 (41.36) | −9.22, 29.49 | 0.29 |
| Post-retraction | 563.83 (117.50) | 552.32 (109.79) | 11.52 (34.01) | −4.40, 27.43 | 0.15 |
| Percent change | −14.64 (2.93) | −15.05 (3.04) | 0.42 (0.96) | −0.03, 0.86 | 0.07 |
| P-value 2 | <0.001* | <0.001* | |||
SD: Standard deviation, CI: Confidence interval, HU: Hounsfield unit. Paired samples t-test was used. P-value 1: Comparison between the experimental and control sides, P-value 2: Comparison of pre-and post-retraction values within each group. *Statistically significant difference at P<0.05
The effect of LLLT on ABT
Changes in the total ABT at the three assessed levels along the maxillary canine root post-retraction in both groups are displayed in [Table 2]. In both the studied groups, significant decreases in the total ABT at the coronal level (−10.26 ± 12.64% in the laser group, and −16.36 ± 13.10% in the control group), and the mid-root level (−7.85 ± 14.69% in the laser group, and −10.11 ± 18.29% in the control group) have been noted. In contrast, there were no significant differences in the total ABT post-treatment at the apical level of the maxillary canine root on both the laser (−0.78 ± 0.51%), and the control sides (−1.43 ± 0.39%). Nevertheless, comparisons between the two sides showed insignificant differences between them in the total ABT at all the evaluated levels (P > 0.05) after canine distalization.
| Experimental | Control | Difference | 95% CI | P-value 1 | |
|---|---|---|---|---|---|
| Mean (SD) | |||||
| Pre-retraction | |||||
| Coronal | 1.31 (0.45) | 1.26 (0.37) | 0.05 (0.26) | −0.08, 0.17 | 0.44 |
| Mid-root | 3.05 (1.11) | 2.83 (1.04) | 0.22 (0.85) | −0.18, 0.62 | 0.26 |
| Apical | 6.45 (1.60) | 6.07 (1.61) | 0.38 (1.20) | −0.18, 0.94 | 0.17 |
| Post-retraction | |||||
| Coronal | 1.18 (0.45) | 1.04 (0.31) | 0.14 (0.31) | −0.004, 0.28 | 0.06 |
| Mid-root | 2.77 (1.00) | 2.48 (0.96) | 0.28 (0.70) | −0.05, 0.61 | 0.09 |
| Apical | 6.40 (1.59) | 5.99 (1.59) | 0.42 (1.18) | −0.13, 0.96 | 0.13 |
| Percent change | |||||
| Coronal | −10.26 (12.64) | −16.36 (13.10) | |||
| Mid-root | −7.85 (14.69) | −10.11 (18.29) | |||
| Apical | −0.78 (0.51) | −1.43 (0.39) | |||
| P-value 2 | |||||
| Pre-vs. Post- | |||||
| Coronal | 0.001* | <0.001* | |||
| Mid-root | 0.02* | 0.01* | |||
| Apical | 0.14 | 0.15 | |||
SD: Standard deviation, CI: Confidence interval, Paired samples t-test was used. P-value 1: Comparison between the experimental and control sides, P-value 2: Comparison of pre-and post-retraction values within each group. *Statistically significant difference at P<0.05
The effect of LLLT on ABV
The calculated changes in ABV in both groups are depicted in [Table 3]. On the experimental and control sides, there was a statistically significant decrease in the ABV around the maxillary canine after its distalization (15.97 ± 4.26% on the experimental side, and 16.59 ± 4.29% on the control side). There were no statistically significant differences in the post-treatment ABV values between the two groups (P = 0.13).
| Experimental | Control | Difference | 95% CI | P-value 1 | |
|---|---|---|---|---|---|
| Mean (SD) | |||||
| Pre-retraction | 648.75 (130.58) | 638.78 (121.63) | 9.97 (56.90) | −16.66, 36.60 | 0.44 |
| Post-retraction | 546.31 (116.50) | 533.29 (106.31) | 13.02 (41.85) | −6.57, 32.61 | 0.18 |
| Percent change | −15.97 (4.26) | −16.59 (4.29) | 0.62 (1.78) | −0.21, 1.45 | 0.13 |
| P-value 2 | <0.001* | <0.001* | |||
SD: Standard deviation, CI: Confidence interval. Paired samples t-test was used. P-value 1: Comparison between the experimental and control sides, P-value 2: Comparison of pre-and post-retraction values within each group. *Statistically significant difference at P<0.05.
DISCUSSION
The main purpose of this study was to investigate the 3D alveolar bone changes induced by LLLT after the canine retraction stage of orthodontic treatment. Based on the recorded outcomes of the present study, the null hypothesis has been accepted, since the application of LLLT accompanying canine retraction has not induced significant improvements neither in bone quality, nor in bone quantity.
The implemented study design in the current trial was a randomized controlled trial (RCT), since RCTs are contemplated as the benchmark for the analysis of intervention efficiency.[31] In addition, the split-mouth design reduced the confounding effects of inter-subject variability, with the participants serving as their own controls, also reducing the number of participants needed.[32]
The employed laser device was a Diode laser semiconductor (Doctor Smile-Lambda Spa, Italy), administered at a wavelength of 980 nm as per manufacturer recommendation, to achieve the required biostimulatory result. This recommendation might go back to the fact that in the ultraviolet to the near IR spectrum, shorter wavelengths result in minimal tissue penetration (200–600 nm), whereas longer absorption wavelengths (650– 1200 nm) bring about heavier tissue penetration.[33]
Another factor influencing the therapeutic and biostimulatory impact of LLLT is the dosage or the energy density. The energy density used in this study was 8 J/cm2, which is a comparable dosage to that employed in several other investigations.[12,28] However, a vast array of administered laser energy densities have been documented, ranging from low dosages[12] to higher ones.[34] In the present work, the employed energy density was delivered using the flat top handpiece, where the beam spot size was 1 cm2. A direct correspondence has been recorded between the diameter of the applied laser beam, and the penetration depth , that consequently validates the use of the flat top handpiece in this investigation.[33] A similar single laser dose administration with a large beam spot size has been employed by Caccianiga et al.[35] with leveling and alignment, as well as by Eid et al.[12] during canine retraction.
CBCTs were imperative for the assessment of both bone quality and quantity; thus, they were performed by the enrolled subjects both pre- and post-retraction. It is to be noted that in addition to the remarkable diagnostic superiority of CBCTs, both the intraobserver and interobserver reliability of CBCT measurements have been advocated.[36] Therefore, CBCT scans have been the tools of choice for the evaluation of alveolar bone changes by several investigators.[37,38] The CBCT scans used for measurements in the present study were all performed with consistent parameters (+CBCT machine, FOV, voxel resolution, voltage, and exposure time). Moreover, all the comparisons regarding the assessed bone changes were carried out on the same subjects and tooth areas, but at distinct treatment timings, all of which maximized the accuracy of the employed CBCTs as evaluation tools.[39]
Assessment of bone quality in the current research involved the assessment of the ABD of the maxillary canine pre- and post-retraction, from the obtained CBCT scans. ABD was measured in HU values , which are the commonly employed units for the measurement of bone density as evident in the literature.[4,40] The present study results showed a significant reduction in ABD after canine retraction, with and without laser application. Multiple factors were reported to influence bone density, including occlusal forces, dietary habits, and body weight.[41-43] Nevertheless, over the course of the study, there were no remarkable alterations neither in body weight nor in the dietary habits adopted by any of the enrolled subjects. However, the reduction in ABD accompanying OTM has been repeatedly reported in the literature, in both clinical and animal studies,[39,44] which could be attributed to the fact that the immature or the recently created bone is less dense and has lower mineralization in comparison with older bone.[44] Moreover, in the study by Hsu et al.,[44] a 24% reduction in ABD has been reported after seven months of orthodontic treatment , which is considered relative to our approximate 15% ABD reduction in only three months of treatment.
This study also found a slightly higher ABD in the irradiated group in comparison to that in the non-irradiated group after canine retraction, but this difference did not attain the level of statistical significance. This slight ABD difference could be attributed to the biostimulatory effect of LLLT that has been known to impact the bone remodeling process,[12,27] although it was not reflected clinically or statistically in the current trial. Similar outcomes have been reported in another investigation by Hsu et al.,[45] where insignificant differences have been registered in bone density with and without laser application accompanying OTM. In contrast, Yoshida et al.[27] documented a significant increase in bone density with low-energy laser irradiation in comparison to the non-irradiated group with OTM. However, the laser parameters employed in their study, in terms of dosage and wavelength were unlike those used in this study, which makes direct comparisons quite conflicting.
This is common in LLLT, where the divergence in the employed parameters documented in the literature greatly affects the results, making outcome comparisons quite difficult.
Bone quantity evaluation was investigated through the analysis of both ABT and ABV. Regarding ABT, our findings documented a statistically significant decrease in the total ABT at the coronal and mid-root levels along the maxillary canine root following its distalization on the laser and control sides. However, an insignificant reduction was found at the apical level. A direct correlation was established between the possible changes in the axial inclination of the teeth over the course of orthodontic treatment and the corresponding changes in the ABT,[37,46] especially at the cervical and mid-root levels, which is in accordance with the current findings. Therefore, this theory could possibly provide a plausible explanation for the significant changes perceived in the total ABT, in both groups. On another note, the insignificant differences in the total ABT between the laser and the control groups at all levels indicate that the biostimulatory impact of LLLT was rather negligible. Since no prior investigations were carried out to test the influence of LLLT on ABT; unfortunately, outcomes of the present study could not be compared to others.
Regarding ABV, a pattern similar to that observed with ABD was documented in ABV. A statistically significant reduction in the ABV was observed in both the laser and the control groups after canine retraction, with insignificant differences being observed upon comparing both groups to each other. Our outcomes are in accordance with those by Verna et al.,[47] where they observed a significant reduction in alveolar bone fraction (bone volume/total volume) around the teeth after orthodontic treatment, in a histological study on rats on both the compression and the tension sides. They explained their findings through the pressure-tension theory , that advocates bone deposition in the tension area. However, the newly formed bone in the tension region is inadequately mineralized and relatively fragile. Furthermore, Banse and Devogelaer[48] have stated that bone density is closely related to bone fraction or bone volume; therefore, the findings by Verna et al.[47] could also provide a possible elaboration on our findings regarding the drop in ABD in both study groups. Although ABV was slightly higher in the irradiated group in comparison to the nonirradiated group, this difference was found to be insignificant, pertaining to the relatively weak impact of laser biostimulation on the bone remodeling process accompanying OTM.
Limitations of the study
The present study has certain limitations, such as the lack of assessment regarding the effects of LLLT on the alveolar bone on the completion of orthodontic treatment. As a result, it is suggested that future research endeavors extend beyond the canine retraction phase. This expansion will enable a comprehensive understanding of the modifications occurring in the bone structure by the conclusion of the entire orthodontic process. Besides, expanding future research to include studying bone microstructure could shed more light on the nature of the qualitative changes taking place in the alveolar bone during OTM. Furthermore, it is important to note that the operator was not blinded during the experimental phase, potentially introducing a bias. Nonetheless, measures were taken to mitigate this bias. Patient allocation to the different groups was randomized, and operators were blinded during the measurement and statistical analysis phases, effectively reducing the potential for bias.
When analyzing the data of patients ranging from 15 to 20 years old, it can be challenging to separate the effects of growth-related changes from those resulting from orthodontic treatment and LLLT. Even though a split-mouth design with intra-individual control was used, this can still confound the interpretation of the study’s findings and make it challenging to draw definite conclusions about the reported findings.
CONCLUSION
LLLT with the parameters employed in this study does not elicit any significant improvement neither in bone quality (ABD), nor in bone quantity (ABT, and ABV) around the maxillary canine throughout its retraction phase during orthodontic treatment.
A significant reduction in the ABD, ABT (coronal and mid-root levels), as well as in the ABV occurs with OTM.
Ethical approval
Ethical approval has been granted by the Institutional Review Board of the Faculty of Dentistry, Alexandria University, Egypt (IRB: 00010556–IORG: 0008839). Manuscript Ethics Committee number 0631– 02/2023. This study was conducted in accordance with the ethical principles of the Declaration of Helsinki.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- Biomechanics and mechanics In: Contemporary Orthodontics. Vol 3. St Louis: Mosby; 2000. p. :300-5.
- [Google Scholar]
- Does orthodontic treatment affect the alveolar bone density? Medicine (Baltimore). 2016;95:e3080.
- [CrossRef] [PubMed] [Google Scholar]
- In vivo microcomputed tomography evaluation of rat alveolar bone and root resorption during orthodontic tooth movement. Angle Orthod. 2013;83:402-9.
- [CrossRef] [PubMed] [Google Scholar]
- The role of orthodontic tooth movement in bone and root mineral density: A study of patients submitted and not submitted to orthodontic treatment. Med Sci Monit. 2012;18:Cr752-7.
- [CrossRef] [PubMed] [Google Scholar]
- The rate and the type of orthodontic tooth movement is influenced by bone turnover in a rat model. Eur J Orthod. 2000;22:343-52.
- [CrossRef] [PubMed] [Google Scholar]
- Products, procedures… or a pipe dream? a reality check on the game called" accelerated orthodontics"! APOS Trends Orthod 2015. ;. ;5:53-5.
- [CrossRef] [Google Scholar]
- Evidence-based care in orthodontics and periodontics: A review of the literature. J Am Dent Assoc. 1999;130:521-7.
- [CrossRef] [PubMed] [Google Scholar]
- White spot lesions: Biomaterials, workflows and protocols. Semin Orthod. 2023;29:68-78.
- [CrossRef] [Google Scholar]
- Contemporary orthodontic workflows: A panacea for efficiency? Semin Orthod. 2023;29:1-3.
- [CrossRef] [Google Scholar]
- The development of submucosal injection of platelet rich plasma for accelerating orthodontic tooth movement and preserving pressure side alveolar bone. APOS Trends Orthod. 2016;6:5-11.
- [CrossRef] [Google Scholar]
- Interdental osteotomies induce regional acceleratory phenomenon and accelerate orthodontic tooth movement. J Oral Maxillofac Surg. 2014;72:19-29.
- [CrossRef] [PubMed] [Google Scholar]
- A randomized controlled trial evaluating the effect of two low-level laser irradiation protocols on the rate of canine retraction. Sci Rep. 2022;12:10074.
- [CrossRef] [PubMed] [Google Scholar]
- Low-power laser irradiation improves histomorphometrical parameters and bone matrix organization during tibia wound healing in rats. J Photochem Photobiol B. 2003;70:81-9.
- [CrossRef] [PubMed] [Google Scholar]
- Assessing accelerated tooth movement techniques on their own catabolic merits: A review. J World Fed Orthod. 2018;7:122-7.
- [CrossRef] [Google Scholar]
- Efficacy of photobiomodulation on accelerating bone healing after tooth extraction: A systematic review. Lasers Med Sci. 2019;34:685-92.
- [CrossRef] [PubMed] [Google Scholar]
- Comparison of rate of orthodontic tooth movement in adolescent patients undergoing treatment by first bicuspid extraction and en-mass retraction, associated with low level laser therapy in passive self-ligating and conventional brackets: A randomized controlled trial. Int Orthod. 2020;18:412-23.
- [CrossRef] [PubMed] [Google Scholar]
- Efficiency of low-level laser therapy in reducing pain induced by orthodontic forces. Photomed Laser Surg. 2012;30:460-5.
- [CrossRef] [PubMed] [Google Scholar]
- Effects of low-energy laser irradiation on bone remodeling during experimental tooth movement in rats. Lasers Surg Med. 2000;26:282-91.
- [CrossRef] [Google Scholar]
- CBCT in orthodontics: Assessment of treatment outcomes and indications for its use. Dentomaxillofac Radiol. 2015;44:20140282.
- [CrossRef] [PubMed] [Google Scholar]
- Quantitative determination of alveolar bone density using digital image analysis of microradiographs. Anat Anz. 1990;170:171-9.
- [Google Scholar]
- Quantitative computed tomography-based finite element analysis predictions of femoral strength and stiffness depend on computed tomography settings. J Biomech. 2015;48:153-61.
- [CrossRef] [PubMed] [Google Scholar]
- Can dental cone beam computed tomography assess bone mineral density? J Bone Metab. 2014;21:117-26.
- [CrossRef] [PubMed] [Google Scholar]
- Three-D imaging of dental alveolar bone change after fixed orthodontic treatment in patients with periodontitis. Int J Clin Exp Med. 2015;8:2385-91.
- [Google Scholar]
- Deriving Hounsfield units using grey levels in cone beam CT: A clinical application. Dentomaxillofac Rradiol. 2012;41:500-8.
- [CrossRef] [PubMed] [Google Scholar]
- Deriving Hounsfield units using grey levels in cone beam computed tomography. Dentomaxillofac Radiol. 2010;39:323-35.
- [CrossRef] [PubMed] [Google Scholar]
- Medical statistics at a glance (3rd ed). West Sussex, UK: John Wiley and Sons; 2009.
- [Google Scholar]
- Low-energy laser irradiation accelerates the velocity of tooth movement via stimulation of the alveolar bone remodeling. Orthod Craniofac Res. 2009;12:289-98.
- [CrossRef] [PubMed] [Google Scholar]
- The influence of two photobiomodulation protocols on orthodontically induced inflammatory root resorption (a randomized controlled clinical trial) BMC Oral Health. 2022;22:221.
- [CrossRef] [PubMed] [Google Scholar]
- Cone beam computed tomography: Basics and applications in dentistry. J Istanb Univ Fac Dent. 2017;51:S102-21.
- [CrossRef] [PubMed] [Google Scholar]
- A guideline of selecting and reporting intraclass correlation coefficients for reliability research. J Chiropr Med. 2016;15:155-63.
- [CrossRef] [PubMed] [Google Scholar]
- Randomized controlled trials-an indispensible part of clinical research. Dtsch Ärztebl Int. 2011;108:661.
- [CrossRef] [Google Scholar]
- Split-mouth designs in orthodontics: An overview with applications to orthodontic clinical trials. Eur J Orthod. 2013;35:783-9.
- [CrossRef] [PubMed] [Google Scholar]
- Five parameters you must understand to master control of your laser/light-based devices. Aesthet Surg J. 2013;33:1059-64.
- [CrossRef] [PubMed] [Google Scholar]
- Effects of different wavelengths of low-level laser therapy on orthodontically induced inflammatory root resorption in rats investigated with micro-computerized tomography. Am J Orthod Dentofacial Orthop. 2021;159:e245-51.
- [CrossRef] [PubMed] [Google Scholar]
- Does low-level laser therapy enhance the efficiency of orthodontic dental alignment? Results from a randomized pilot study. Photomed Laser Surg. 2017;35:421-6.
- [CrossRef] [PubMed] [Google Scholar]
- Accuracy and reliability of cone-beam computed tomography measurements: Influence of head orientation. Am J Orthod Dentofacial Orthop. 2011;140:157-65.
- [CrossRef] [PubMed] [Google Scholar]
- A quantitative three-dimensional comparative study of alveolar bone changes and apical root resorption between clear aligners and fixed orthodontic appliances. Prog Orthod. 2023;24:6.
- [CrossRef] [PubMed] [Google Scholar]
- Evaluation of maxillary canine root and maxillary bone thickness and density in patients with displaced maxillary canines: A cone-beam tomography study. Am J Orthod Dentofacial Orthop. 2022;162:318-30.
- [CrossRef] [PubMed] [Google Scholar]
- Effects of orthodontic tooth movement on alveolar bone density. Clin Oral Investig. 2012;16:679-88.
- [CrossRef] [PubMed] [Google Scholar]
- Quantitative evaluation of bone density using the Hounsfield index. Int J Oral Maxillofac Implants. 2006;21:290-7.
- [Google Scholar]
- Occupational sitting and low hip mineral density. Calcif Tissue Int. 1998;62:47-50.
- [CrossRef] [PubMed] [Google Scholar]
- The effect of osteoporosis on periodontal status, alveolar bone and orthodontic tooth movement. A literature review. J Int Acad Periodontol. 2007;9:77-84.
- [Google Scholar]
- The effect of altered bone metabolism on orthodontic tooth movement. Am J Orthod. 1981;80:256-62.
- [CrossRef] [PubMed] [Google Scholar]
- Bone density changes around teeth during orthodontic treatment. Clin Oral Investig. 2011;15:511-9.
- [CrossRef] [PubMed] [Google Scholar]
- 970 nm low-level laser affects bone metabolism in orthodontic tooth movement. J Photochem Photobiol B Biol. 2018;186:41-50.
- [CrossRef] [PubMed] [Google Scholar]
- Changes in alveolar bone thickness due to retraction of anterior teeth. Am J Orthod Dentofacial Orthop. 2002;122:15-26.
- [CrossRef] [PubMed] [Google Scholar]
- Histomorphometric study of bone reactions during orthodontic tooth movement in rats. Bone. 1999;24:371-9.
- [CrossRef] [PubMed] [Google Scholar]
- Does peripheral quantitative computed tomography ignore tissue density of cancellous bone? J Clin Densitom. 2002;5:403-10.
- [CrossRef] [PubMed] [Google Scholar]




