

Translate this page into:
Dietary experiences during fixed orthodontic treatment

*Corresponding author: Sabarinath Prasad, Department of Orthodontics, Hamdan Bin Mohammed College of Dental Medicine, Mohammed Bin Rashid University, Dubai, United Arab Emirates. sabarinath.prasad@mbru.ac.ae
-
Received: ,
Accepted: ,
How to cite this article: En PL, SoYeon O, Nor NN, Mei L, Farella M, Prasad S. Dietary experiences during fixed orthodontic treatment. APOS Trends Orthod 2023;13:60-7.
Abstract
Objectives:
Orthodontists generally recommend avoidance of certain foods during fixed appliance (FA) treatment, based on anecdotal information. This study aimed to identify the dietary preferences and experiences of patients undergoing FA treatment as a step toward the preparation of evidence-based dietary guidelines.
Material and Methods:
Questionnaires regarding dietary preferences and experiences of patients undergoing FA treatment were applied to a convenience sample of 38 adolescents (12 M; 26 F). Open-ended responses were summarized and visualized in a world cloud generator. 5-point Likert and Visual Analog Scales (VAS) were used to record the closed-ended responses. Descriptive statistics and multivariate analysis of variance were used to analyze questionnaire findings.
Results:
Lollies, apples, and nuts frequently caused problems with FA. The most frequent reason for avoiding certain types of food was worry about appliance breakage, followed by pain and sensitivity. VAS scores indicated that toffee and caramel scored highest (65.1% F and 54.1% M) for discomfort followed by corn on the cob (64.4% F and 48.7% M) and apples (56.6% F and 55.3% M). VAS scores did not differ significantly between the sexes (P > 0.05). Nearly, a quarter of the sample reported that FA negatively affected their eating behaviors, causing pain and discomfort during eating. No sex differences (P > 0.05) were found for negative experiences with food.
Conclusion:
Dietary preferences and experiences of patients undergoing FA treatment were identified concerning a New Zealand diet profile. A future study with a larger sample size will help formulate evidence-based dietary guidelines during FA treatment.
Keywords
Diet
Orthodontics
Survey
Questionnaire
Fixed appliances

INTRODUCTION
Demand for orthodontic treatment has significantly increased[1] and fixed appliances (FA) are an integral part of comprehensive orthodontic treatment. Orthodontic treatment with FA entails lifestyle modifications and impacts the performance of routine daily activities, particularly eating.[2] FA tends to be more painful in comparison to removable appliances and pain during mastication has been reported by recall-based[3] and naturalistic assessment[4] studies. Pain can affect compliance[5] and is ranked high among the reasons for discontinuing orthodontic treatment.[3]
The discomfort, sensitivity, and/or pain on biting and chewing during orthodontic treatment with FA lead to alterations in food choices. Changes in the consistency of the food consumed are needed to manage pain during orthodontic treatment.[6] Diet modifications during orthodontic treatment also result in response to instructions given by orthodontists.[7] During FA treatment, dietary advice provided by orthodontists focus on avoiding breakages and minimizing pain/discomfort during treatment. Dietary instructions by orthodontists during FA treatment relate to the consistency and quality of food consumed with a recommendation to avoid “hard, chewy, and sticky food.” Orthodontists advise a soft diet in the immediate post-treatment stage to avoid pressure sensitivity leading to altered nutrient intake. The importance of providing dietary and nutritional guidance to patients undergoing orthodontic treatment has been emphasized in the past.[3,8] Although dietary guidelines listing foods to avoid and foods that can be consumed during FA treatment have been provided by orthodontic associations around the world,[9-11] data to support these guidelines are lacking. Significant variability in recommended diets and lack of existing data to support the evidence-based implementation of dietary guidelines has also been reported post-orthognathic surgery.[12] A clear understanding of patient experiences during eating and the kind of food that they avoid and consume is necessary to develop better dietary recommendations for patients undergoing FA treatment.
Questionnaire surveys are a valuable tool to gain insight into the preferences, opinions, and experiences of subjects in a quick and cost-effective manner. In the past, questionnaire studies have provided valuable information regarding patient experiences at various stages of orthodontic treatment.[13-16] Questionnaires are helpful in gathering baseline data which can then be used to formulate evidence-based guidelines. With this in mind, a questionnaire survey was conducted to identify dietary preferences and experiences during FA treatment from a patient perspective.
MATERIAL AND METHODS
Ethical approval for this study was obtained from the University of Otago Human Ethics Committee Reference H20/062.
An anonymous and self-administered questionnaire was used to collect data on perceptions of different types of food from subjects undergoing orthodontic treatment with FA. Patients were recruited over 1 month from the active patient list of the Orthodontic Department, Faculty of Dentistry, University of Otago and were included if they were aged between 12 and 18 years of age and currently undergoing FA treatment. All patients recruited had upper and lower metal brackets (Mini Master® American Orthodontics, slot size 0.018”) bonded using light cure adhesive resin (3M, Transbond™ XT). Patients were excluded if they were in the first 2 weeks of FA treatment, had mental impairment, or were unable to complete the questionnaire.
A convenience sample of 55 patients (age 15.4 ± 1.6 years) who attended orthodontic appointments was invited to participate in the study. Informed consent was obtained from all the patients or caregivers. Out of the 55 patients surveyed, 38 were eligible and participated in the computer-based survey that was administered in the patient waiting area. Patients were also allowed to opt-out of the survey at any time.
The survey [Appendix 1-3] consisted of both open-ended and closed-ended questions and covered various aspects of patient experience, comfort level, difficulties encountered, and limitations imposed while eating different food items during FA treatment. The food items selected for the questionnaire were based on the recommendations made by several orthodontists at the University of Otago, and on common food items listed in the national food survey of New Zealanders.[17]
The questionnaire included five parts: Demographic information about the patients, limitations imposed by food type, experiences during eating, level of discomfort with different foods, and open-ended questions. For the closed-ended survey questions, Visual Analog Scales (VAS) and 5-point Likert scales recorded participant ratings. VAS marked on a 0–100 scale ranging from 0 (least) to 100 (worst) were used to rate how patients felt about the severity of limitations imposed by food type and level of discomfort with different foods. 5-point Likert scales were used to record the negative experiences of patients during eating with FA.
Participant responses to the open-ended questions were qualitatively analyzed in a word cloud generator. Responses for the food items that caused breakages, discomfort, pain, and staining were pooled. Descriptive words such as “hard,” “chewy,” and “sticky” were excluded from the word cloud.
Data were recorded as the mean ± standard deviation, or number, and percentage. Data analysis was performed using the Statistical Package for the Social Sciences (version 22.0; SPSS Inc., IL, USA) with an alpha value of 0.05. Multivariate analysis of variance was used for comparing sample means.
RESULTS
[Table 1] shows the sociodemographic characteristics of the 38 patients who were surveyed. The majority were females and of New Zealand (NZ) European ethnicity.
| Sex (n, %) | Male Female |
12 (32%) 26 (68%) |
| Ethnicity (n, %) | NZ European Maori/Pacific Others |
32 (84%) 3 (8%) 3 (8%) |
The level of limitation imposed [Figure 1] was the least (<10% VAS) with food that did not require chewing and minimal (<20% VAS) with shredded food items. A limitation associated with hard food, sticky food, and food requiring biting on front teeth was high (around 40–50% of VAS), with no difference reported between genders (P > 0.05).
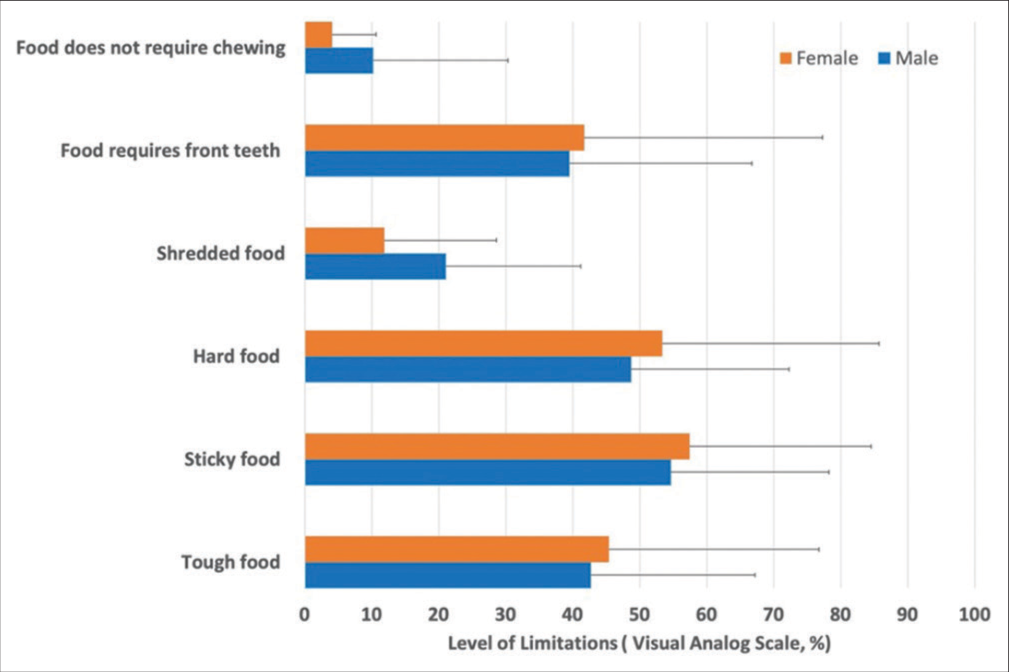
- Visual analogue scales scores for severity of limitations associated with hard food, sticky food, and food requiring biting on front teeth.
The 5-point Likert scale showed [Figure 2] that up-to a quarter of the surveyed patients always/often experienced negative feelings; with pain and discomfort being the two most frequent negative experiences while eating. No significant gender differences were found regarding negative experiences with food (P > 0.05).
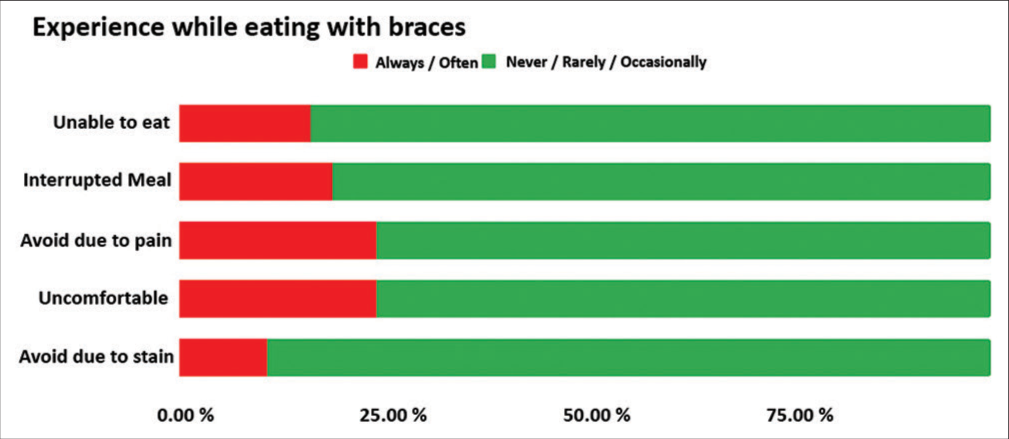
- 5-point Likert scale responses for negative experiences with food.
With FA, most discomfort (>50% VAS) was experienced while eating toffee and caramel, hard lollies, apples, steak and corn on the cob. Raw carrots, nuts, and muesli bars also led to discomfort but to a lesser extent (average VAS scores > 30%) [Figure 3]. FA-friendly food (average VAS scores <10%) included fish and chips, hot chips, pasta, noodles, and boiled eggs. Female patients experienced more discomfort among the food items mentioned in the questionnaires than males, but the difference was not statistically significant, except for roasted chicken (P = 0.047).

- Visual analogue scales scores for the levels of discomfort on eating different food items.
Lollies followed by apples and nuts were the main food items that patients associated with breakage of FA components. This was consistent with food items that were reported to be uncomfortable to eat with FA. Meat in particular was reported to be painful to eat by a majority of patients followed by lollies. Despite this, the steak came in fifth on the list of food items for the level of discomfort. Interestingly, many patients did not avoid food items that increased the likelihood of causing staining. Patients reported that chewing gum got stuck in the FA components leading to breakage. However, an almost equal number of patients also felt that chewing gum did not negatively affect FA treatment. Similarly, no significant differences were seen between patients that avoided and did not avoid eating with the front teeth while on FA treatment. A world cloud was used to visually summarise the frequency of food items that patients considered as FA- unfriendly [Figure 4].

- Word cloud depicting the words used most frequently in the survey. Font size correlates with the greater frequency of the word used in the survey, while word location in the image is random.
DISCUSSION
While undergoing orthodontic treatment with FA, diet is restricted typically to reduce pain/discomfort and to minimize the likelihood of appliance breakages. For this, orthodontists recommend “soft food,” without detailed specifications regarding the foods to consume or to avoid. Orthodontic associations provide dietary guidelines, advising the avoidance of chewy (caramels, chewing gum, beef jerky, and bagels); hard (peanuts, ice chips, hard lollies, and pork cracklings), and crunchy food (like chips, apples, and carrots) for the duration of FA treatment.
To the best of our knowledge, this is the first study to investigate dietary preferences and experiences of subjects undergoing FA treatment using a combination of open- and closed-ended measures.
Adolescent subjects were chosen in this study because a majority of patients undergoing orthodontic treatment with FA fall in this age group. Only patients who were on FA longer than 2 weeks were included in the study as pain intensity has been shown to gradually decline after this period.[18] Being the first study of its kind, no studies were available to estimate the needed sample size and power for this study. Convenience sampling was used as a relatively fast and inexpensive way for gathering initial explorative data. Hence, a relatively small number of patients (n = 38) were included that were skewed toward the female gender (70%). This is not surprising as most often it is young females who seek orthodontic treatment, probably because of higher aesthetic demands.[19] Although no statistically different differences were seen between genders, the general trend was that female subjects experienced greater pain/discomfort with the food items that were not FA-friendly. This is consistent with findings from the literature on orofacial pain and temporomandibular disorders,[20,21] although it must be acknowledged that there is only limited understanding of the mechanisms behind these gender-based differences.
The validity of findings is largely dependent on how representative the responding sample is of the source population. Due to the relatively small number of patients and over representation of females, caution should be exercised in generalizing the findings of the present study. Future studies with more patients and gender- and aged-matched control groups will be helpful to improve study generalizability and increase the validity of this study.
Although patients who responded to the survey were diverse and representative of orthodontic patients; most were of NZ European ethnicity [Table 1]. The food items chosen for the questionnaire were based on the normal diet of NZ adolescents outlined in the National Food Survey NZ.[17] Again, the generalizability of results may be limited due to dietary variations between different ethnic groups and nationalities.[22]
Open-ended questions helped gain better insights and provide more detail regarding the feelings, and opinions of subjects undergoing FA treatment with the qualitative data permitting capturing information of interest. From the open ended questions in this study, most adolescents undergoing FA treatment avoided certain types of food due to reasons including fear of breaking their braces; followed by teeth sensitivity and pain, worry of food entrapment in-between the appliance, and difficulty while eating. One also mentioned that “Because they were recognized by the information provided to me as specifically bad for braces.” Word clouds are simple visual tools that represent word frequency with more common terms within the responses being analyzed appearing as larger in the image generated.[23,24] However, word clouds should be interpreted with certain caveats as they often fail to group words that have the same or similar meaning. Due to the focus only on single word frequency, they also do not identify phrases, reducing context.
Masticatory forces in the posterior region are heavy and relatively hard food requires greater masticatory effort. These forces when transferred by the hard food to the impinging bracket may account for discomfort during eating and bracket failure. All subjects in this study were treated with the same FA and bonding system and different operators represented by postgraduate students, who add to variability in response.[25] Interestingly, researchers have found differences in bracket failure rates among different malocclusion types.[26] The effect of malocclusion on mastication is equivocal. Systematic reviews have concluded that only severe malocclusions can decrease masticatory performance[27] and also that it is not entirely possible to either support or deny the influence of specific dental/skeletal malocclusion traits on masticatory performance.[28] However, investigating bracket failure rates according to the type of malocclusion or whether the failure was operator- or patient-related was not within the scope of this study and may be an area for future research.
VAS and 5-point Likert scales are useful tools to assess a patient’s subjective experience or perception of a variety of clinical phenomena[29,30] including diet and eating.[3,31,32] This study revealed that most patients with FA, regardless of gender, reported a high level of discomfort when eating foods such as apples, sticky food like caramel or toffee, corn on the cob, and hard lollies. In comparison to that, foods that were associated with low levels of discomfort were white bread, hot chips, pasta, fish and chips, noodles, and boiled eggs while eating with FA. Reassuringly, the findings from this study generally support the Australian Society of Orthodontics[9] recommendations to avoid chewy foods such as caramels, chewing gum, beef jerky, and bagels, hard foods such as peanuts, hard lollies, and pork crackling, and crunchy foods such as chips, apples, and carrots for orthodontic patients.
CONCLUSION
Dietary preferences and experiences of patients undergoing FA treatment were identified concerning an NZ diet profile. The foods that scored high for discomfort were somewhat consistent with the foods identified by patients as non-braces friendly due to reasons of causing breakage, and pain, staining, and discomfort. While the present study offers substantial insight into the foods that can be FA-friendly and those that are not concerning the New Zealander diet profile, further research using a bigger sample size, a wider range of food, and food textures is required. Development, implementation, and evaluation of dietary guidelines would be the next logical step that will help in providing orthodontists with the resources needed to confidently manage dietary advice for patients undergoing FA treatment.
Acknowledgments
We wish to thank Honorary Associate Professor Winsome Parnell from the Department of Human Nutrition, University of Otago, Dunedin for her help in the development of the survey questions
Declaration of patient consent
Institutional Review Board (IRB) permission obtained for the study.
Conflicts of interest
There are no conflicts of interest.
Financial support and sponsorship
Nil.
References
- Who needs orthodontic treatment? Who gets it? and who wants it? Br Dent J. 2015;218:99-103.
- [CrossRef] [PubMed] [Google Scholar]
- Impacts on daily performances related to wearing orthodontic appliances. Angle Orthod. 2008;78:482-6.
- [CrossRef] [PubMed] [Google Scholar]
- Pain, masticatory performance and swallowing threshold in orthodontic patients. Dent Press J Orthod. 2013;18:117-23.
- [CrossRef] [PubMed] [Google Scholar]
- Ecological momentary assessment of pain in adolescents undergoing orthodontic treatment using a smartphone app. Semin Orthod. 2018;24:209-16.
- [CrossRef] [Google Scholar]
- Pain and discomfort during orthodontic treatment: Causative factors and effects on compliance. Am J Orthod Dentofacial Orthop. 1998;114:684-91.
- [CrossRef] [PubMed] [Google Scholar]
- Orthodontic pain: From causes to management--a review. Eur J Orthod. 2007;29:170-9.
- [CrossRef] [PubMed] [Google Scholar]
- A qualitative study of the early effects of fixed orthodontic treatment on dietary intake and behaviour in adolescent patients. Eur J Orthod. 2012;34:432-6.
- [CrossRef] [PubMed] [Google Scholar]
- Effects of orthodontic treatment on nutrient intake. Am J Orthod Dentofacial Orthop. 1997;111:554-61.
- [CrossRef] [PubMed] [Google Scholar]
- Diet While Having Orthodontic Treatment. Available from: https://www.aso.org.au/diet-while-having-orthodontic-treatment [Last accessed on 2022 May 01]
- [Google Scholar]
- Teeth and Brace-friendly Food and Drink. Available from: https://www.bos.org.uk/portals/0/Public/docs/PILs/foodanddrinkapril2013.pdf [Last accessed on 2022 May 01]
- [Google Scholar]
- Life During Orthodontic Treatment. Available from: https://www.3.aaoinfo.org/blog/parent-s-guide-post/life-during-orthodontic-treatment [Last accessed on 2022 May 01]
- [Google Scholar]
- Review of diet protocols following orthognathic surgery and analysis of postoperative weight loss. Cleft Palate Craniofac J. 2022;0
- [CrossRef] [PubMed] [Google Scholar]
- Impact of malocclusion on adolescents' oral health-related quality of life. Gen Dent. 2016;64:e1-5.
- [Google Scholar]
- Development of the Malocclusion Impact Questionnaire (MIQ) to measure the oral health-related quality of life of young people with malocclusion: Part 2-cross-sectional validation. J Orthod. 2016;43:14-23.
- [CrossRef] [PubMed] [Google Scholar]
- Impact of the onset of fixed appliance therapy on adolescents' quality of life using a specific condition questionnaire: A cross-sectional comparison between male and female individuals. J Orthod. 2019;46:195-204.
- [CrossRef] [PubMed] [Google Scholar]
- Psychometric validation of a pre-existing questionnaire used to measure patient satisfaction following orthodontic treatment in a UK population. J Orthod. 2021;48:231-40.
- [CrossRef] [PubMed] [Google Scholar]
- 2016 New Zealand Total Diet Study. 2018. Wellington: Ministry for Primary Industries; Available from: https://www.mpi.govt.nz/dmsdocument/43177-2016-NZ-Total-Diet-Study-with-Appendices-report [Last accessed on 2022 May 01]
- [Google Scholar]
- The pain experience and psychological adjustment to orthodontic treatment of preadolescents, adolescents, and adults. Am J Orthod Dentofacial Orthop. 1991;100:349-56.
- [CrossRef] [PubMed] [Google Scholar]
- Does gender make a difference in orthodontics? A literature review. Orthod Fr. 2018;89:157-68.
- [CrossRef] [PubMed] [Google Scholar]
- Summary of findings from the OPPERA baseline case-control study: Implications and future directions. J Pain. 2011;12(11 Suppl):T102-7.
- [CrossRef] [PubMed] [Google Scholar]
- Increasing gender differences in the prevalence and chronification of orofacial pain in the population. Pain. 2020;161:1768-75.
- [CrossRef] [PubMed] [Google Scholar]
- Associations between dietary patterns, socio-demographic factors and anthropometric measurements in adult New Zealanders: An analysis of data from the 2008/09 New Zealand Adult Nutrition Survey. Eur J Nutr. 2018;57:1421-33.
- [CrossRef] [PubMed] [Google Scholar]
- Experiences of individuals concerning combined orthodontic and orthognathic surgical treatment: A qualitative twitter analysis. Med Princ Pract. 2018;27:227-35.
- [CrossRef] [PubMed] [Google Scholar]
- A retrospective survey of the causes of bracket-and tube-bonding failures. Angle Orthod. 2017;87:111-7.
- [CrossRef] [PubMed] [Google Scholar]
- A comparative clinical trial of a compomer and a resin adhesive for orthodontic bonding. Angle Orthod. 2000;70:233-40.
- [Google Scholar]
- The influence of malocclusion on masticatory performance. A systematic review. Angle Orthod. 2010;80:981-7.
- [CrossRef] [PubMed] [Google Scholar]
- Effect of malocclusion on jaw motor function and chewing in children: A systematic review. Clin Oral Investig. 2022;26:2335-51.
- [CrossRef] [PubMed] [Google Scholar]
- A critical review of visual analogue scales in the measurement of clinical phenomena. Res Nurs Health. 1990;13:227-36.
- [CrossRef] [PubMed] [Google Scholar]
- Five-point scales outperform 10-point scales in a randomized comparison of item scaling for the Patient Experiences Questionnaire. J Clin Epidemiol. 2011;64:200-7.
- [CrossRef] [PubMed] [Google Scholar]
- Techniques for the experimental measurement of human eating behaviour and food intake: A practical guide. Int J Obes Relat Metab Disord. 1995;19:361-75.
- [Google Scholar]
- Development and validation of the general dietary behavior inventory (GDBI) in scope of international nutrition guidelines. Nutrients. 2021;13:1328.
- [CrossRef] [PubMed] [Google Scholar]
Appendix 1: Open-ended questions.
| Questions |
|---|
| Is/are there any food(s) that have caused your braces to break? If yes, please list them below What are the food(s) that were recommended by your dentist/ orthodontist to be eaten during treatment with braces? |
| What are the recommended food(s) you were told by your dentist/orthodontist to avoid or be careful of during treatment with braces? |
| What food(s) do you feel uncomfortable to eat with braces on? List the food(s) that have caused pain while eating with braces on Do you find yourself avoiding eating with your front teeth? (Y/N) If yes, list them Why do you avoid certain type(s) of food? |
| List the food(s) that have caused staining of your braces List the food(s) that have caused breakage of your braces while eating |
| How does chewing gum affect your braces? Do you notice yourself enjoying chewing gum/avoiding chewing gum? If so, why? |
Appendix 2: Closed-ended questions.
| Questions with Visual Analogue Scales responses | |
| 1 | How much does biting with your front teeth bother you? |
| 2 | How bothered are you when biting or chewing fresh apple? |
| 3 | How bothered are you when biting or chewing corn on the cob? |
| 4 | How bothered are you when chewing or biting steak? |
| 5 | How bothered are you when biting or chewing muesli bars? |
| 6 | How bothered are you when biting or chewing nuts? |
| 7 | How bothered are you when biting or chewing popcorn? |
| 8 | How bothered are you when biting or chewing hard lollies? |
| 9 | How bothered are you when biting or chewing sticky food like caramel and toffee? |
| 10 | How bothered are you when eating roasted chicken? |
| 11 | How bothered are you when eating ice-cream? |
| 12 | How bothered are you when eating scones? |
| 13 | How bothered are you when eating hot chips? |
| 14 | How bothered are you when eating biscuits? |
| 15 | How bothered are you when eating cereal? |
| 16 | How bothered are you when eating raw carrots? |
| 17 | How bothered are you when eating chocolate? |
| 18 | How bothered are you when eating ice cubes? |
| 19 | How bothered are you when eating white bread? |
| 20 | How bothered are you when eating mixed grain bread? |
| 21 | How bothered are you when eating hamburger? |
| 22 | How bothered are you when eating boiled egg |
| 23 | How bothered are you when eating dry biscuits? |
| 24 | How bothered are you when eating noodles? |
| 25 | How bothered are you when eating pasta? |
| 26 | How bothered are you when eating fish and chips? |
| Questions#with 5-point-Likert scale responses | |
| 1 | Have you avoided eating certain types of food because it causes pain since you started wearing braces? |
| 2 | Have you avoided eating certain types of food because it causes staining on your braces? |
| 3 | Have you avoided eating certain types of food because it causes discomfort while wearing braces? |
| 4 | Have you had interrupted meals because of the problems with your braces? |
| 5 | Have you been unable to eat with your braces because of problems with them? |
| 6 | Have you found it uncomfortable to eat any food because of your braces? |
Non-applicable (NA) was the response recorded to a question if the food was not compatible with patients dietary requirements #Always ( ) Often ( ) Occasionally ( ) Rarely ( ) Never ( ) responses
Appendix 3: Limitations experienced with fixed appliances.
| Questions with Visual Analogue Scales responses |
| Chew tough food |
| Chew sticky food |
| Chew hard food |
| Chew chicken |
| Eat anything that uses the front teeth |
| Eat soft food that does not require any chewing |




