

Translate this page into:
Evaluation of skeletal and dentoalveolar components in Syrian females with a gummy smile
Address for Correspondence: Dr. Amr Hayani, Faculty of Dentistry, University of Aleppo, Aleppo, Syria. E-mail: amhayany@hotmail.com
This article was originally published by Wolters Kluwer and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Objectives
The objective of this study was to investigate the dentoalveolar and skeletal components contributing to a gummy smile (G.S.) in Syrian females.
Materials and Methods
The G.S. group included 20 Syrian females, with an average age of 21.9 ± 3.9 years and a clinically diagnosed G.S. The control group included 20 Syrian females, with an average age of 22.05 ± 2.87 years and an acceptable smile. All subjects had Class I molar and canine relationships. Lateral cephalometric radiographs of all subjects were taken under similar conditions. Total cephalometric parameters measured included 11 angular measurements, 12 linear measurements and 7 ratios between the linear measurements.
Results
Statistically significant increases in the total anterior facial height, lower anterior facial height, dentoalveolar heights and facial diversion angles were observed in the G.S. group as opposed to the control group.
Conclusion
There was an obvious role played by the skeletal and dentoalveolar components in occurrence of a G.S. in Syrian females and these must be considered during orthodontic treatment planning.
Keywords
Gummy smile
skeletal and dentoalveolar components
Syrian female population

INTRODUCTION
Smile is an emotional facial expression of the human race that triggers positive reactions and helps people win friends and popularity. Acquiring a charming smile is one of the major reasons for which patients seek orthodontic care. The different components of smile change with age and such changes differ between males and females.[1] Gummy smile (G.S.), which is defined as the increased gingival exposure between the lower border of the upper lip and gingival margin during full smiling is considered unesthetic and a gingival display of more than 2 mm is thought to be undesirable.[2]
Excessive gingival display is prevalent in 10% of the population between the age of 20 and 30 years and is more common in women than in men.[3,4] The severity of this condition gradually decreases with age as a consequence of drooping of the upper and lower lips, which in turn leads to decreased maxillary incisor exposure and increased mandibular incisor exposure.[5,6] There is also evidence of sexual dimorphism in smile line frequency: “Low smile lines” are predominantly seen in males with a male:female ratio of 2.5:1 and “high smile lines” are predominantly seen in females with a male:female ratio of 2:1.[7] The study by Peck et al.[4] confirms these findings.
G.S. is a multifactorial problem and its etiology has been discussed in a considerable amount of literature. Excessive anterior maxillary height, hyperfunction of labial elevator muscles and excessive gingiva as a result of delayed passive eruption are thought to be three major causes.[7] Singer[8] explained the role of upper lip length in G.S. cases. Bishara[9] found G.S. cases with large interlabial gaps to have either short lips or excessive anterior vertical growth. Monaco et al.[10] classified G.S. based on its etiopathogenetic nature as Dento-gingival G.S., Muscular G.S., Dentoalveolar (skeletal) G.S. and mixed nature G.S.
A study by Peck et al.[11] noted that the biologic mechanism underlying the presence of a gingival smile line appeared to include several variables such as anterior vertical maxillary excess (by 2-3 mm), greater muscular capacity to raise the upper lip on smiling and other factors like excessive overjet, excessive interlabial gap at rest and excessive overbite. Wu et al.,[12] summarized the morphologic features determining the presence of a G.S. as skeletal malocclusion type, dentoalveolar heights and the ratio of the upper lip length to the anterior maxillary height.
The main objective of this study was to understand the various skeletal and dentoalveolar components in Syrian female patients with a G.S.
MATERIALS AND METHODS
Subjects
Post-pubertal subjects were chosen for the study so that there was no component of growth-related influence. The G.S. group consisted of 20 Syrian females. The following criteria were used in the selection of subjects:
All patients were adults (>18 years) and had full permanent dentition (except 3rd molars).
Dental Class I molar and canine relationships, simple minor crowding or spacing was accepted.
No history of trauma to the face, orthodontic treatment, maxillofacial or plastic surgery.
Absence of congenital anomalies, significant facial asymmetry, cleft lip or palate.
All patients complained of a G.S. and had a gingival display of more than 2 mm on average as noted during clinical examination.
The control group consisted of 20 Syrian females, selected in the same manner as the G.S. group except for the last criterion. All subjects in the control group had a normal acceptable smile.
Lateral cephalometric radiographs of all the subjects were taken under same exposure conditions with teeth in maximal intercuspation, the Frankfort horizontal (FH) plane parallel to the floor and the soft-tissue objectively judged to be unstrained. The reference points used are shown in Figure 1.

- The reference points used in the study. Na: The most anterior point of nasofrontal suture in midsagittal plane, S: Midpoint of bony crypt of sellaturcica, Pt: Pterygo-Maxillary fissure a landmark at the 11 O’clock position of the mid-planed contour of the pterygo-mandibular fissure, Go: The bisection of the angle formed by tangents to the posterior border of the ramus and the inferior border of the mandible, Me: The most inferior point on the symphysis of the mandible, Po: The superior margin of the external auditory meatus, Or: The lowest point on the inferior margin of the orbit, Ans: Anterior nasal spine The most anterior point of palate, Pns: Posterior nasal spine Posterior tip of the palatal bone, Gn: The most anterior inferior point of the chin, A: The most concave in anterior contour of maxillary alveolar process in midsagittal plane between supradental and anterior nasal spine, B: The deepest midline point on the mandible between infradental and pogonion, U1: The tip of the crown of the upper central incisor, L1: The tip of the crown of the central lower incisor, UM6: The tip of the mesial cusp of the upper first molar, LM6: The tip of the mesial cusp of the lower first molar
All cephalometric radiographs were traced manually on acetate sheets by one author in order to eliminate inter-examiner variability. 11 angular and 12 linear measurements were constructed for skeletal and dento-alveolar analysis in addition to 7 ratios between the linear measurements [Figures 2, 3 and 4].
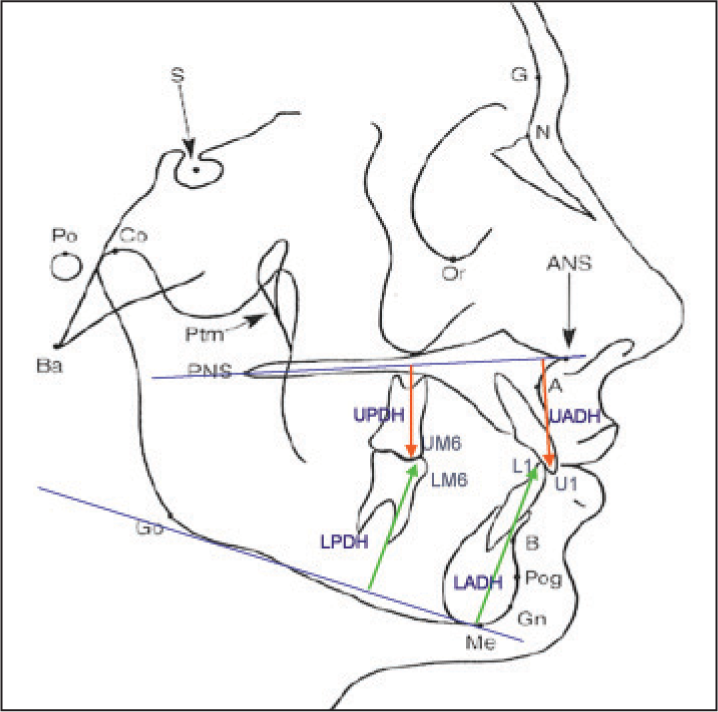
- Cephalometric measurements used in the study (dentoalveolar height measurements). Upper anterior dental height (UADH): The perpendicular length of a line dropped from U1 to palatal plane, upper posterior dental height (UPDH): The perpendicular length of a line dropped from UM6 to palatal plane, UADH/UPDH: The ratio between upper anterior dento-alveolar height and upper posterior dento-alveolar height, lower anterior dental height (LADH): The perpendicular length of a line dropped from L1 to mandible plane, lower posterior dental height (LPDH): The perpendicular length of a line dropped from LM6 to mandible plane, LADH/LPDH: The ratio between lower anterior dento-alveolar height and lower posterior dento-alveolar height
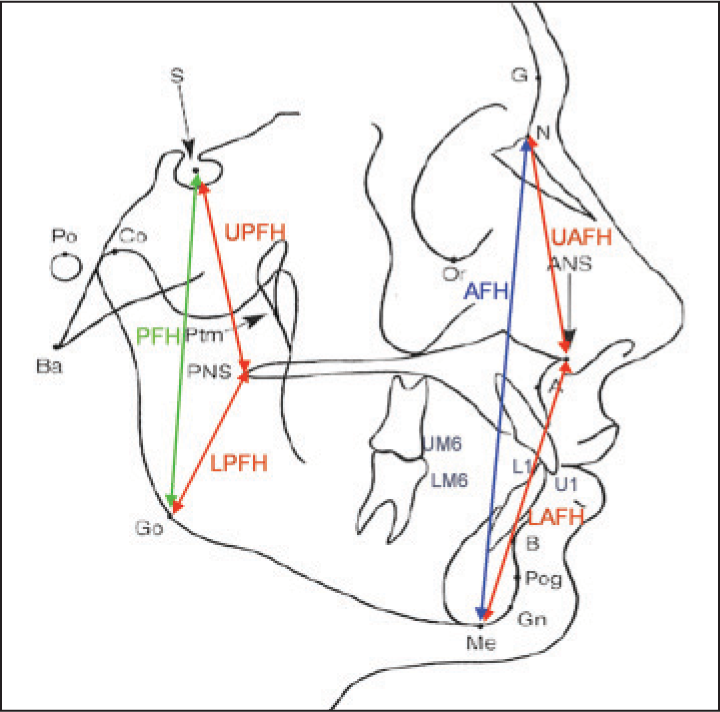
- Cephalometric measurements used in the study (facial height measurements). Upper anterior facial height: The distance between N and ANS, Lower anterior facial height: The distance between ANS and Me, Anterior facial height: The distance between N and Me, Upper posterior facial height: The distance between S and PNS, Lower posterior facial height: The distance between PNS and Go, Posterior facial height: The distance between S and Go
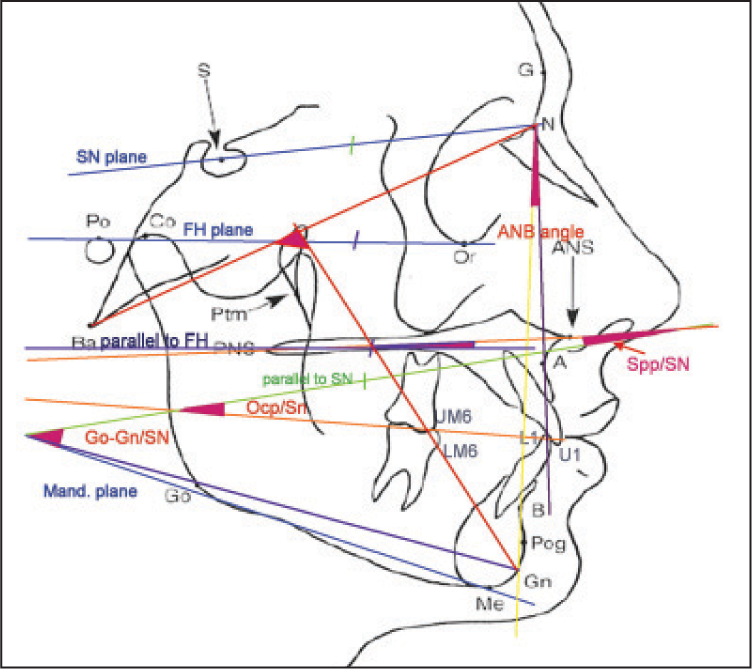
- Cephalometric angular measurements used in the study Facial axis angle: The lower posterior angle formed by Ba-Na and Pt-Gn, Spp/SN: The angle between palatal plane and SN plane, Ocp/ SN: The angle between occlusal plane and SN, Go-Gn/SN: The angle between mandibular plane and SN plane, Spp/FH: The angle between palatal plane and FH, FMA: The angle between mandibular Plane and FH, SNA: The angle between SN line and NA line, SNB: The angle between SN line and NB line, ANB: The difference between SNA and SNB angle. U1-NA (degree): The angle between upper incisal axis and NA line, U1 to NA (mm): The distance from is perpendicular to NA line, L1-NB (degree): The angle between lower incisal axis and NB line, L1 to NB (mm): The distance from ii perpendicular to NB line
Reliability
A random selection of 8 cephalometric radiographs (20% of the total sample) was retraced by the same investigator to evaluate intraexaminer error in tracing and measuring. These duplications were performed a minimum 1 month after the first tracing. The method error was calculated using paired sample tests and paired sample correlations. The method error was considered to be negligible.
Statistical analysis
All statistical analyses were performed using SPSS (Statistical Package for Social Sciences) version 17 (SPSS Inc., Chicago, IL, USA). The descriptive statistics, mean values and standard deviations (SD) were calculated for age and each measurement. The sample showed normal distribution according to the Anderson–darling test. Therefore, the independent samples’ t-test was used to evaluate the difference between the groups and compare the mean differences of each cephalometric measurement between the groups. Statistical significance was set at P < 0.05.
RESULTS
The mean and SD of age and amount of the gingival exposure for the G.S. group and the control group are shown in Tables 1 and 2.
| Group | Mean age (years) | SD | Sample size (n) |
|---|---|---|---|
| G.S group | 21.9 | 3.9 | 20 |
| Control group | 22.05 | 2.87 | 20 |
G.S – Gummy smile; SD – Standard deviation
| Variable | G.S group | Control group | Significance | |||||
|---|---|---|---|---|---|---|---|---|
| Mean | SD | n | Mean | SD | n | P value | Sig. | |
| Gingival exposure | 5.12 | 1.35 | 20 | 0.40 | 0.59 | 20 | 0.000 | *** |
Sig – Significance; ***P < 0.001. G.S – Gummy smile; SD – Standard deviation
The mean and SD of the cephalometric measurements (linear, angular and ratio measurements) for the G.S. group and the control group are shown in Tables 3, 4 and 5 respectively.
| Variable | G.S group | Control group | Significance | Reliability n = 8 | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | n | Mean | SD | n | P Value | Sig. | t | r | |
| UADH | 35.00 | 1.91 | 20 | 30.95 | 4.04 | 20 | 0.000 | *** | 1 | 0.99 |
| UPDH | 28.45 | 2.76 | 20 | 25.85 | 2.87 | 20 | 0.006 | ** | 0.35 | 0.98 |
| LADH | 48.60 | 2.43 | 20 | 44.35 | 3.31 | 20 | 0.000 | *** | 1 | 0.98 |
| LPDH | 38.35 | 2.90 | 20 | 36.35 | 2.90 | 20 | 0.036 | * | 0.59 | 0.98 |
| I/NA mm | 7.92 | 3.09 | 20 | 5.70 | 1.75 | 20 | 0.009 | ** | 0.59 | 0.95 |
| i/NB mm | 9.62 | 2.66 | 20 | 7.10 | 2.63 | 20 | 0.009 | ** | 0.59 | 0.98 |
| UPFH | 50.10 | 2.75 | 20 | 48.40 | 3.28 | 20 | 0.084 | * | 1 | 0.98 |
| LPFH | 49.30 | 4.47 | 20 | 49.40 | 4.22 | 20 | 0.942 | NS | 0.68 | 0.98 |
| PFH | 83.45 | 4.90 | 20 | 82.80 | 6.22 | 20 | 0.716 | NS | 0.59 | 0.99 |
| UAFH | 58.10 | 3.82 | 20 | 56.15 | 3.04 | 20 | 0.083 | * | 1 | 0.99 |
| LAFH | 81.15 | 5.23 | 20 | 72.65 | 5.76 | 20 | 0.000 | *** | 0.35 | 0.99 |
| AFH | 135.40 | 7.35 | 20 | 126.10 | 5.31 | 20 | 0.000 | *** | 0.17 | 0.99 |
Sig – Significance; *P < 0.05; **P < 0.01; ***P < 0.001; NS – Not significant; UADH – Upper anterior dental height; UPDH – Upper posterior dental height; LADH – Lower anterior dental height; LPDH – Lower posterior dental height; UPFH – Upper posterior facial height; LPFH – Lower posterior facial height; PFH – Posterior facial height; LAFH – Lower anterior facial height; UAFH – Upper anterior facial height; AFH – Anterior facial heights
| Variable | G.S group | Control group | Significance | Reliability n = 8 | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | n | Mean | SD | n | P Value | Sig. | t | r | |
| I/NA° | 23.80 | 6.18 | 20 | 22.05 | 4.86 | 20 | 0.326 | NS | 0.28 | 0.98 |
| i/NB° | 31.85 | 6.29 | 20 | 27.45 | 6.55 | 20 | 0.037 | * | 0.73 | 0.99 |
| SNA° | 80.50 | 4.14 | 20 | 80.95 | 3.42 | 20 | 0.710 | NS | 1 | 1 |
| SNB° | 76.00 | 3.75 | 20 | 77.65 | 2.83 | 20 | 0.125 | NS | 1 | 0.99 |
| ANB° | 4.50 | 1.60 | 20 | 3.30 | 1.45 | 20 | 0.018 | * | 1 | 0.96 |
| Ocp/SN | 19.40 | 4.15 | 20 | 17.45 | 5.43 | 20 | 0.210 | NS | 1 | 0.99 |
| Spp/SN | 9.45 | 3.88 | 20 | 9.85 | 3.42 | 20 | 0.732 | NS | 0.08 | 0.99 |
| Spp/FH | 3.00 | 3.56 | 20 | 1.25 | 3.10 | 20 | 0.107 | NS | 0.17 | 0.99 |
| GoGn/SN | 38.85 | 5.56 | 20 | 30.95 | 4.62 | 20 | 0.000 | *** | 0.38 | 0.68 |
| FMA | 27.20 | 4.50 | 20 | 21.20 | 4.00 | 20 | 0.000 | *** | 0.35 | 0.99 |
| Facial axis | 82.75 | 4.19 | 20 | 87.80 | 3.22 | 20 | 0.000 | *** | 0.17 | 0.99 |
Sig – Significance;*P < 0.05; ***P < 0.001; NS – Not significant; G.S – Gummy smile; SD – Standard deviation; FMA – Frankfort’s mandibular plane angle
| Variable | G.S group | Control group | Significance | Reliability n = 8 | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | n | Mean | SD | n | P Value | Sig. | t | r | |
| LAFH/UAFH | 1.400 | 0.096 | 20 | 1.299 | 0.147 | 20 | 0.015 | * | 0.59 | 0.98 |
| PFH/AFH | 0.617 | 0.040 | 20 | 0.656 | 0.036 | 20 | 0.003 | ** | 0.52 | 0.99 |
| UADH/AFH | 0.258 | 0.011 | 20 | 0.245 | 0.027 | 20 | 0.045 | * | 0.91 | 0.98 |
| LADH/AFH | 0.359 | 0.014 | 20 | 0.351 | 0.018 | 20 | 0.155 | NS | 0.89 | 0.96 |
| UADH/UPDH | 1.237 | 0.097 | 20 | 1.198 | 0.098 | 20 | 0.212 | NS | 0.65 | 0.94 |
| UADH/LADH | 0.720 | 0.031 | 20 | 0.697 | 0.073 | 20 | 0.209 | NS | 0.85 | 0.97 |
| LADH/LPDH | 1.270 | 0.055 | 20 | 1.222 | 0.057 | 20 | 0.01 | * | 0.57 | 0.94 |
Sig – Significance; *P < 0.05; **P < 0.01; NS – Not significant; G.S – Gummy smile; SD – Standard deviation; LAFH – Lower anterior facial height; UAFH – Upper anterior facial height; AFH – Anterior facial heights; PFH – Posterior facial heights; UADH – Upper anterior dental height; LADH – Lower anterior dental height; UPDH – Upper posterior dental height; LPDH – Lower posterior dental height
Table 3 demonstrated that females with a G.S. had significantly more protruded incisors (upper and lower) in comparison with the control group (P < 0.01). Vertically, all the measurements sho wed a significant increase, indicating greater dento-alveolar heights in the G.S. group (P < 0.05).
The skeletal facial height measurements also showed a significant increase in the G.S. group (P < 0.05), with an exception of two measurements, i.e., the total posterior and lower posterior facial heights (PFHs), which showed small differences which weren’t statistically significant (P > 0.05). As shown in Table 4, the mean of ANB angle in females with a G.S. was 4.5° which significantly differed from the mean of ANB angle (3.3°) in the control group (P < 0.05). Furthermore, the mandibular plane angles measured between the FH and cranial base Sella-Nasion (SN), were significantly larger in females with the G.S. than the control group (P < 0.001).
The facial axis was more divergent in the G.S. group in comparison with the control group (P < 0.001).
With regard to the skeletal linear measurement ratios [Table 5], the PFH/anterior facial height (AFH) ratio in the G.S. group showed a significant decrease (P < 0.001), whereas the lower anterior/upper anterior facial height ratio (LAFH/UAFH) was significantly larger than the control group (P < 0.05).
The dentoalveolar linear measurement ratio (lower anterior/ lower posterior dentoalveolar height ratio, [LPDH]) showed a significant increase in the G.S. group (P < 0.05).
The relationship between the skeletal and dentoalveolar measurements (upper anterior dentoalveolar height [UADH] to the total AFH ratio) showed a significant increase in the G.S. group (P < 0.05).
DISCUSSION
The present study investigated the various dentoalveolar and skeletal components contributing to a G.S. in Syrian females. The subjects were considered as belonging to the “G.S. group” after a clinical examination, in which the amount of gingival exposure during a posed smile was noted. A posed smile is the voluntary expression made when introduced to someone and it is repeatable; studies have found little difference among numerous consecutive photographs of posed smiles by the same individuals.[13,14] The selected study sample showed a gingival display that measured more than 2 mm in the posed smile at the right central incisor (as directly measured by a ruler).[15] We considered 2 mm and more of gingival exposure as a criterion to define the G.S. group, based on previous studies, which have reported normal amounts of gingival exposure during smile. Some studies say that the upper lip must coincide with the gingival margin during the smile.[16,17] Viazis mentions that 0-2 mm of gingival exposure is normal.[18] Other studies have reported that it is acceptable to see less than 2 mm of the gingiva during the smile.[15,19,20]
When the measurements made on lateral cephalograms in the two groups were compared, differences in the AFH, PFH between the two groups were seen. There was a statistically significant increase in the AFH in the G.S. group (P < 0.001), but there was no statistically significant difference in PFH between the groups. The results also identify a significant decrease in PFH/AFH ratio in the G.S. group, (P = 0.003), which suggests that females with a G.S. had greater AFH in comparison with the control group. This result was in accordance with that of Wu et al., who identified the craniofacial features of adolescents with a G.S.[12]
The significant increase in AFH in the G.S. group was a result of the increase in both the upper and LAFHs with a highly significant increase in the LAFH (P < 0.001). This significant increase in the LAFH led to a significant increase in LAFH/UAFH ratio (P < 0.05) in the G.S. group. Bishara, in his study, has reported that any increase in the lower facial height may result in a lip-apart posture and an excessive gingival display on a full smile.[9]
The maxillo-mandibular relation as represented by the angle ANB was significantly larger in the G.S. group (P < 0.05). This may be a result of the increase in all the linear and angular measurements in the vertical dimension which indicated to posterior rotation of the mandible and retrusion of the point B.
With regard to dentoalveolar differences, this study has demonstrated a significant increase in the anterior and posterior upper dentoalveolar heights in the G.S. group (P < 0.01). Peck et al.,[11] Wu et al.,[12] and Mackley[21] in their studies, have found similar results, with G.S. cases showing an increase in the upper anterior dentoalveolar height (of about 2-3 mm). The lower dentoalveolar height also was significantly larger in the G.S. group than in the control group (P < 0.05). A study by Wu et al. found that the LPDH was significantly smaller in the G.S. group,[12] and this may be due to the difference in the reference mandibular plane they used to measure the lower dento-alveolar heights. The reference mandibular plane in Wu’s study was defined by Gn and Go points (as described by Steiner),[12] whereas in this study the reference mandibular plane was defined by the tangential line from menton to the lower border of the mandible (as described by downs).
The anterior dentoalveolar heights were larger than the posterior dentoalveolar heights, particularly in the mandible (P = 0.01). This might have contributed to the increased posterior rotation of the mandible in the G.S. group. The ratio between the UADH and the total AFH (P < 0.05) also was increased in the G.S. group. This result and all of the dentoalveolar measurements mentioned above, suggested that the females with the G.S. in this study had a general increase in the dentoalveolar heights as a compensation for LAFH increase and this was in agreement with Janson et al. study[22] which reported a significant increase in common dentoalveolar heights in patients who had an increase in lower facial height.
With regard to the dental variables, the lower incisors in relation to NB line were more protruded in G.S. cases (P < 0.05). This may be caused as a dental compensation for the increased ANB angle in females with the G.S.
The angular measurements suggesting vertical relationships like the FMA angle (Frankfort’s mandibular plane angle), Gonion-Gnathion to SN plane and the facial axis; have indicated a vertical growth pattern (P < 0.001) in G.S. cases. The significant increase in the LAFH and LAFH/UAFH ratio in the G.S. group seems to have contributed to the increase in these angular measurements. Singer[8] and Wu et al.[12] have reported similar increases in the angle between the mandibular plane and cranial base (P < 0.05) in G.S. cases, whereas, Peck et al.[11] reported that even though this angle was larger in G.S. cases it wasn’t significantly different from non-G.S. cases (P > 0.05).[11] This may be due to the difference in the mean age of the subjects in their study, which was 15.5 years, while in our study, the mean age was 21.5 years.
This study has shown an insignificant difference between the groups (P > 0.05) in relation to the inclination of the occlusal and palatal planes w.r.t the cranial base (Ocp/SN, Spp/SN). This suggests that the inclination of the maxilla was not a contributing factor in the occurence of a gummy smile. Peck et al.[11] and Wu et al.[12] confirmed this result in their studies through the insignificant difference in this measure (P > 0.05).
CONCLUSIONS
The cephalometric features of Syrian females with a G.S. can be summarized as follows:
Skeletal class II malocclusion and increased vertical growth pattern.
Increase in total AFH.
Decrease in the ratio of PFH/AFH.
Posterior rotation of the mandible.
No slanting of the palatal plane.
General increase in the dentoalveolar heights, especially the upper anterior dentoalveolar height.
Proclination of the lower incisors.
All the points mentioned above led to the conclusion that skeletal and dentoalveolar components had an obvious role in causing a G.S., and these points must be considered during orthodontic treatment planning in such cases.
Source of Support:
Nil.
Conflict of Interest:
None declared.
References
- The influence of maxillary gingival exposure on dental attractiveness ratings. Eur J Orthod. 2002;24:199-204.
- [Google Scholar]
- Some vertical lineaments of lip position. Am J Orthod Dentofacial Orthop. 1992;101:519-24.
- [Google Scholar]
- Dynamic smile analysis: Changes with age. Am J Orthod Dentofacial Orthop. 2009;136:310.e1-10.
- [Google Scholar]
- Textbook of Orthodontics. Philadelphia, Pennsylvania: W.B. Saunders Company; 2001. p. :561-76.
- Gummy smile: Clinical parameters useful for diagnosis and therapeutical approach. J Clin Pediatr Dent. 2004;29:19-25.
- [Google Scholar]
- Classification and craniofacial features of gummy smile in adolescents. J Craniofac Surg. 2010;21:1474-9.
- [Google Scholar]
- Dynamic smile visualization and quantification: Part 2. Smile analysis and treatment strategies. Am J Orthod Dentofacial Orthop. 2003;124:116-27.
- [Google Scholar]
- Esthetic factors involved in anterior tooth display and the smile: Vertical dimension. J Clin Orthod. 1998;32:432-45.
- [Google Scholar]
- Soft tissue cephalometric analysis for orthognathic surgery. J Oral Surg. 1980;38:744-51.
- [Google Scholar]
- The diagnosis and treatment of the gummy smile. Compend Contin Educ Dent. 1997;18:757-62. 764
- [Google Scholar]
- Soft-tissue evaluation In: Viazis AD, ed. Atlas of Orthodontics Principles and Clinical Applications. Philadelphia: W.B. Saunders Company; 1993. p. :49-57.
- [Google Scholar]
- Facial keys to orthodontic diagnosis and treatment planning — Part II. Am J Orthod Dentofacial Orthop. 1993;103:395-411.
- [Google Scholar]
- Orthodontics and orthognathic surgery in the combined treatment of an excessively “gummy smile”. N Z Dent J. 1999;95:53-4.
- [Google Scholar]
- An evaluation of smiles before and after orthodontic treatment. Angle Orthod. 1993;63:183-9.
- [Google Scholar]
- Variation in maxillary and mandibular molar and incisor vertical dimension in 12-year-old subjects with excess, normal, and short lower anterior face height. Am J Orthod Dentofacial Orthop. 1994;106:409-18.
- [Google Scholar]




