

Translate this page into:
FOCA orthodontic diagnosis method: Facial, occlusal, cephalometric, and anamnesis analysis – Description of the method and instruments applied
 , Gabriela Letícia Clavisio Siqueira Machado1, Adriana Souza de Jesus1,, Renata Mayumi Kato1, Thales Lippi Ciantelli1, Patrícia Pigatto Schneider1
, Gabriela Letícia Clavisio Siqueira Machado1, Adriana Souza de Jesus1,, Renata Mayumi Kato1, Thales Lippi Ciantelli1, Patrícia Pigatto Schneider1

*Corresponding author: Adriana Souza de Jesus, Department of Orthodontics, UniCPO Sorocaba, Votorantim, São Paulo, Brazil. jesus.adrianasouza@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Pinto RO, Machado GLCS, Jesus AS, Kato RM, Ciantelli TL, Schneider PP. FOCA orthodontic diagnosis method: Facial, occlusal, cephalometric, and anamnesis analysis – Description of the method and instruments applied. APOS Trends Orthod. doi: 10.25259/APOS_187_2024
Abstract
Diagnosis is considered the determining step for success or failure in orthodontic treatment and must be performed considering heredity, individual characteristics, and the patient’s environment, both for corrective and interceptive orthodontics. To establish a sequence and associate relevant information that defines a treatment plan, the facial, occlusal, cephalometric, and anamnesis (FOCA) diagnostic method was created. This method is actively used by more than 3000 dentists and its instruments have already been shared with more than 110,000 dentists in Brazil and Latin America, through online events. This article aims to describe the methodology and instruments created for its application. The 13-step facial analysis guide, occlusal analysis in the transverse, vertical, and sagittal directions, as well as inter and intra-arch analysis, are described in this work. The anamnesis guide instrument highlights heredity, medical history, menarche, habits, trauma, tooth loss, breathing, speech changes, snoring, bruxism, and TMJ function deviations. The sequence of what to do with the information obtained through facial and occlusal analysis is described in this work: The elaboration of therapeutic goals, list of problems, alternative approaches, and final treatment sequence. The FOCA diagnostic method guarantees a disciplined approach to diagnosis and treatment planning. The systematization of information, as well as the implementation of technology in the diagnostic steps, justifies treatment decisions and leads the professional to more complete and assertive treatment plans.
Keywords
Diagnosis
Patient care planning
Cephalometry
Anamnesis

INTRODUCTION
Diagnosis and planning in orthodontics are considered the stage of orthodontic treatment that requires the greatest knowledge, time, and dedication from the professional. Over the years, we have witnessed an exponential sophistication of materials and instruments in orthodontics. As occlusion has become a realistic goal for treating many types of malocclusions, the need for a complete understanding of the patient’s diagnosis and treatment plan are prerequisites today.
For many years, the diagnosis was made solely based on cephalometric analysis. Strict standards depending on the inclination of the lower incisor, such as the Tweed Triangle reference,[1] led to a generation of orthodontists with practices focused on orthodontic extractions. The main limitations in focusing diagnosis on cephalometry are the differences between norms in different ethnic groups due to anatomical variations such as the position of the base of the skull, the difficult correlation with the patient’s esthetics, and errors when it is not performed digitally.[2,3]
With the introduction of facial diagnosis following the first studies by Arnett and Bergman,[4,5] the harmony and metrics of the face began to be taken into account as the first point to be considered in the treatment plan. Andrews also made a great contribution with his studies on Gall’s line in adult women and men, a reference line for planning and finalizing clinical cases in orthodontics. According to the author, the line must pass perpendicular to the ground, close to the glabella, and coincide with the most buccal surface of the upper incisor.[6]
The facial, occlusal, cephalometric, and anamnesis (FOCA) method, an acronym for FOCA, has been part of the Postgraduate Program in Orthodontics at UniCPO School since 2017. It is applied after acquiring complete patient documentation and performing rigorous clinical examinations as a step-by-step guide to diagnosing and treating patients. This method gained visibility after being disseminated in online Interceptive and Corrective Orthodontics events, to date with the participation of 110,000 dentists from Brazil and 22 countries in Latin, Central America, and Europe. The method is actively applied by 3250 students in the online improvement and extension courses and 150 students in the Specialization in Orthodontics and other postgraduate programs in Latin America. The methodology was applied to students of different levels, beginners in orthodontics, and experienced orthodontists. There is already information about the efficiency of the online education model for postgraduate teaching in orthodontics.[7]
The theoretical basis of the facial analysis is derived from the work of Arnett and Bergman, Adams et al., and Siécola et al. [5,6,8,9] The objective of the FOCA method is to systematize the diagnostic steps to guide the thinking of the orthodontist or orthodontics student to possibly arrive at the ideal treatment plan based on the list of problems, therapeutic goals, and treatment alternatives, and final treatment plan.
According to the literature, less experienced orthodontists have greater difficulty in recognizing the complexity of medium and high-complexity cases.[10] This deficit in diagnosis results in longer cases, with difficult resolution and changes in treatment plans.
The diagnostic sequence is known by orthodontic professionals, but it is rarely executed formally and rigorously due to the lack of organization of information and because it requires extensive time to go through all the stages. Applications, software, and artificial intelligence (AI) have been implemented to facilitate diagnosis and reduce the time dedicated mainly to cephalometric measurements and models.[11,12]
It is clear that the literature finds gaps related to detailed and didactic methods in the diagnosis and planning of clinical cases in orthodontics. For this reason, this work aims to describe the FOCA technique and the support instruments that were created to implement the method.
Obtaining the patient’s facial analysis
To perform a facial analysis of the patient, a clinical examination must first be conducted and photographs must be taken in the natural position of the head (NPH). The patient should look at the horizon with the pupils parallel to the ground. Years ago, facial analysis was carried out with the Frankfurt plane parallel to the ground, but we already know that the NPH is more faithful and presents fewer variations.[13]
In this work, we present the facial analysis guide [Part of Annex 1 and 2] which was divided into 13 steps. The objective of this instrument is to guide the orthodontist through the main structures of the face to reach the 13th point, the definition of the facial pattern. According to Siécola et al.,[9] individuals, regardless of their nationality, can be classified according to the subjective analysis of 5 facial patterns, which would be Pattern I, II, III, short face, and long face. Pattern I is considered the individual with a proportional maxilla and mandible without growth anomalies on the face. Pattern II presents a growth anomaly that may be due to mandibular retrusion (most common), maxillary protrusion, or a contribution from both. Pattern III is characterized by a mandibular protrusion (most common), maxillary retrusion, or contribution of both growth changes. The short-face patient presents a deficiency in the growth of the lower third of the face and can be classified as unbalanced brachyfacial. The long-face patient would be the opposite in terms of vertical facial growth and could be considered unbalanced dolichofacial.
The authors defend the subjective and non-metric facial analysis for the classification of the face pattern. However, due to the clinical difficulties encountered among orthodontics professionals, the authors of this work suggest classifying the pattern into 3 stages:
Drawing lines of orientation to guide the interpretation of the face
Patient evaluation on 12 facial structures in frontal and lateral views
After this analysis, determine the patient’s facial pattern, and in cases of Pattern II or III, whether there is an association with vertical problems. This sequence was suggested after we encountered difficulties mentioned by post-graduation students in orthodontics for subjective analysis and to guide the professional by reducing the possibility of error.
In all lateral photographs, two reference lines of the face are placed: The true vertical line (TVL) and Gall’s line [Figure 1].

- Image showing the true vertical line and Gall’s line in a patient with mandibular protrusion and maxillary retrusion.
The TVL is defined as a line passing through the subnasal point, perpendicular to the ground. It is used to evaluate the relationship between upper and lower lips, maxilla, and mandible and the relationship between Glabella, points A’ and B’ (deepest points of the maxilla and mandible marked in soft tissue). Gall’s line has already been described earlier in this article. Both have the aim of assisting in the evaluation of the anteroposterior position of the bone bases, assessing whether there is protrusion or not depending on the distance or coincidence between the maxillary and mandibular structures and the reference lines.[14]
In the lateral view, the nose implantation line is drawn, the line that goes from the corner of the orbit to the wing of the nose. Furthermore, the chin baseline, the neck contour line, and the lines define the nasolabial angle [Figure 2]. In the frontal analysis, the horizontal lines that establish the facial thirds are placed: the lowest line of the chin, the line of the base of the nose, the glabella line, and the line of the hair insertion. Only one vertical line is drawn in the frontal view, the vertical line that follows the references of the center between the eyebrows, the tip of the nose, and the center of the “cupid’s arch” [Figure 3].

- Image showing nose implantation line, chin baseline, neck contour, and nasolabial angle in a patient with mandibular protrusion and maxillary retrusion.
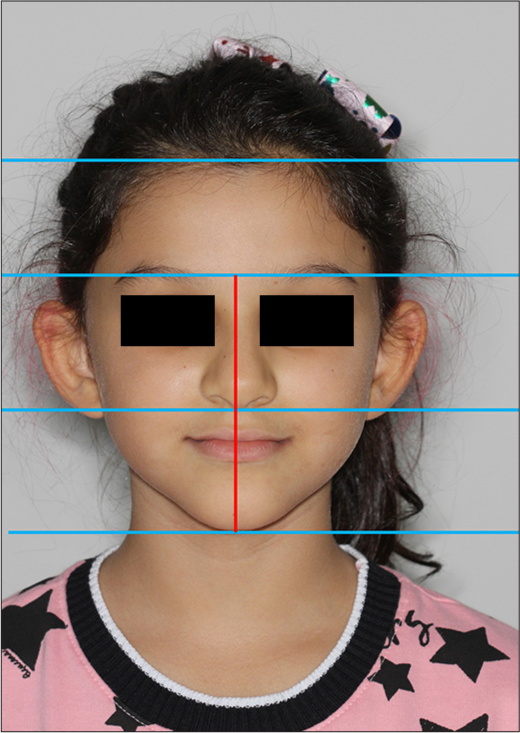
- Frontal image; the horizontal lines (blue lines) are drawn to evaluate the facial thirds and the vertical line (red line) to analyze facial asymmetry.
Once performed the appropriate guidelines on the face, the facial analysis instrument can be used in 13 steps. In the instrument created “facial analysis guide,” subtitles help to indicate the standard of normality and the changes that must be brought together to form the list of problems.
Obtaining the patient’s occlusal analysis
The patient’s first occlusal analysis is performed clinically by visualizing the occlusion in maximum intercuspation (MI) and manipulating the patient in centric relation (CR). At this point, we detect clinical signs of normality of the temporomandibular joint and functional deviations, and the difference between CR and MI should not exceed 1 mm.[15] If there are fulcrums in the occlusion or double bite that exceed the reference value, whether or not accompanied by pain, a cone beam computed tomography (CBCT) examination of the patient is recommended to assess the integrity of the condyles cortical, symmetry, and volume. Thus, the authors eliminated the need to set up the case in an articulator, as we visualized the position of the condyle in the glenoid fossa on the CBCT examination and recorded the points of premature contact of the occlusion in CR with complementary intraoral photographs.
The patient’s occlusal analysis must be developed by observing intraoral photographs and digital or physical models. Occlusal analysis is performed in two different ways, the first seeking to classify malocclusions and the second seeking to obtain numbers on intra- and inter-arch analyses. The analysis of the diagnostic models follows the transverse, vertical and sagittal order (TVS). This is performed so that the orthodontist does not fail to classify any of the dimensions independently.
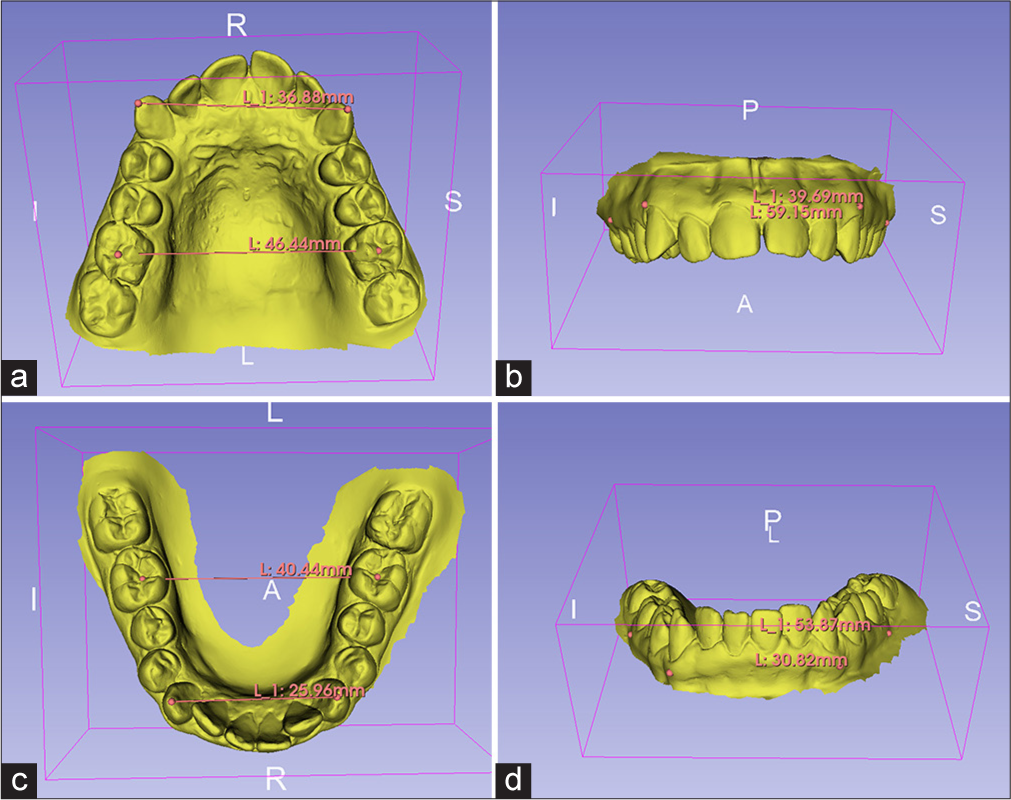
In the transverse view, the malocclusion can be evaluated as adequate, unilateral, or bilateral posterior crossbite and Brodie bite. At this point, measures can be taken in the inter-molar and inter-canine regions to serve as support in the future to define the therapeutic approach. The following are recommended [Figure 4]: Linear measurement between the center of the central groove of the upper and lower molars, the tip of the cusps of the upper and lower canines, the most buccal portion of the bone in the region of the molars and canines to assess whether the transverse discrepancy is slight (until 2 mm), moderate (between 2 and 4 mm), or severe (>4 mm difference between the upper and lower arches).
- Linear measurements for transverse evaluation TVS (transverse, vertical, and sagittal) analysis. (a) Intermolar and intercanine distances in the upper arch. (b) Most buccal bone portion in the region of upper molars and canines. (c) Intermolar and intercanine distances in the lower arch. (d) Most buccal bone portion in the region of lower molars and canines.
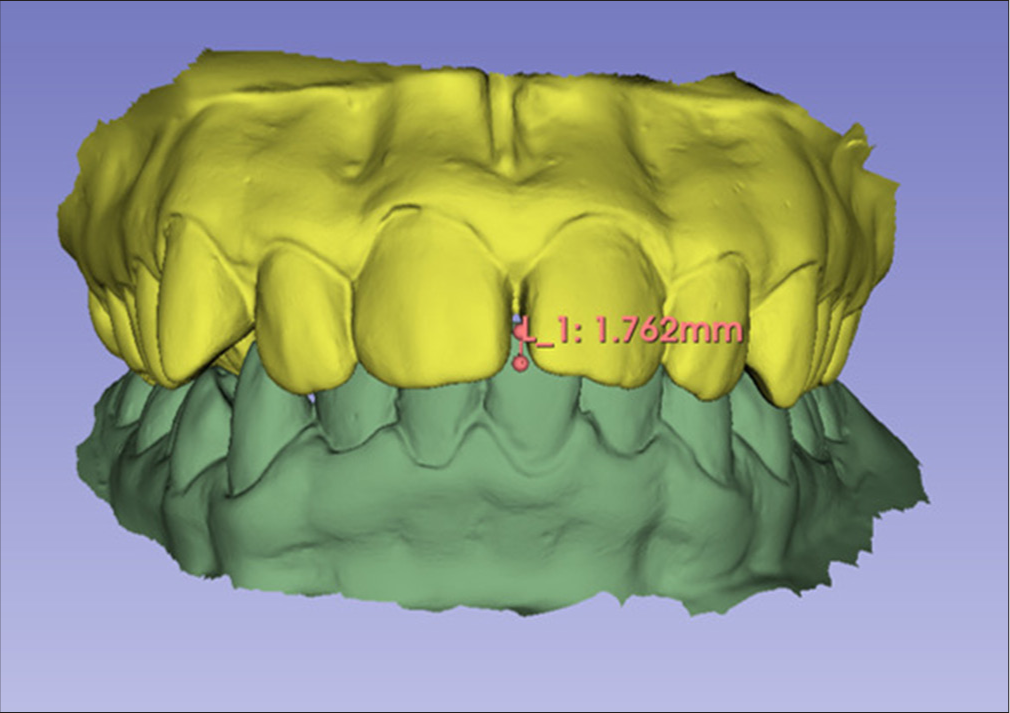
Vertical analysis of dental arches [Figure 5] performed with models in occlusion, classifying the patient as having adequate overbite (2 mm between upper and lower incisors), deep bite (+2 mm), reduced overbite or edge-to-edge bite (between 0 and 1 mm), and anterior open bite (−1 mm).
- Linear measurements for vertical evaluation or overbite TVS (transverse, vertical, and sagittal) analysis.
The sagittal analysis of dental arches is performed by evaluating the molar relationship in permanent dentition and the canine relationship in mixed dentition. The canine relationship is chosen for the first phases of development due to stability in the dental exchange stage and due to greater fidelity to the patient’s facial pattern. At this stage, the patient is classified into dental Class I, II, or III, and regarding severity, 1/4, ½, ¾, or complete.
In the case of patients with permanent dentition, Class II is classified about the upper incisors (division 1 for proclined incisors and division 2 for lingualized central and proclined lateral incisors or lingualized central and lateral incisors). Class II and Class III are also classified regarding symmetry, being considered a subdivision when it presents Class II or III on one side and Class I on the opposite side, with the side of the malocclusion being nominated as a subdivision followed by its corresponding side, right or left.
Intra and inter-arch analysis, which aims to record numerical data on crowding and discrepancy between the upper and lower arch, can be done manually or digitally, using physical or digital models. There are no differences between measurements using the two types of models, as long as they are performed carefully by the orthodontist.[16]
This analysis can be easily performed using new technologies such as the Smartooth cell phone application (for iOS system) or OrthoCalc (for Android and iOS systems). In both applications, individual measurements of the dental equator from 2nd molar to 2nd molar in the upper and lower arches and the measurement of the bone base from the mesial of the first molars are carried out. In physical models using a compass and ruler and in digital models using free software, the authors suggest Autodesk Meshmixer or 3D Slicer.
After entering the data into the applications, a data report is generated with the model discrepancy, Bolton discrepancy (6–6 and 3–3), or Moyers discrepancy for mixed dentition. If these data are out of the normal range, they must be transferred to the problem list.
Obtaining the patient’s cephalometric analysis
As the method presents a detailed analysis of the face, cephalometry at this stage serves as a supporting instrument for the numerical understanding of the patient’s most important characteristics.
It is known that cephalometry has greater data fidelity when measurements are carried out digitally. In addition, it reduces the dentist’s working time drawing the analyses. For this reason, software was also implemented to facilitate the diagnostic method. There are paid software such as Dolphin, Dentofacial Planner, and Radiocef[17] or free software such as Webceph, BlueSky Plan, and Blender. In some software, there are already tools for detecting cephalometric points using AI, which only have to be modified to the exact position by the operator.[12]
The three pillars of analysis of the FOCA method are anteroposterior analysis of the bone bases, vertical growth visualization measurements, and linear and angular position of the upper and lower incisors. From these 3 pillars, their respective normality criteria are also considered. As this method was created to be applied to the Latin American population, we sought references of normality from Brazilian or Latin American individuals. The measurements of pillars 1, 2, and 3 are illustrated in [Figure 3].
Pillar 1: Sagittal analysis of the bone bases
SNA, the angle formed by the points S, N, and A that defines the sagittal relationship of the maxilla with the skull base, first described by Downs (Norm: 82°).
SNB, the angle formed by points S, N, B that defines the sagittal relationship of the mandible with the skull base, first described by Downs (Norm: 80°).
N Perp A, the linear distance between point A and the N-perp line, the line leaving point N, perpendicular to the Frankfurt plane, first described by McNamara. Defines the sagittal relationship of the maxilla with the base of the skull (Norm: 0–1 mm).[18]
N Perp Pog, the linear distance between point B and the N- perp line, the line leaving point N, perpendicular to the Frankfurt plane, first described by McNamara. Defines the sagittal relationship of the mandible with the base of the skull, (Norm: −4–0 mm).[18]
Wits, points A and B must be projected perpendicularly onto the functional occlusal plane, and the distance between them, AO and BO, respectively, is measured. When AO is ahead of BO, the measurement is positive; when BO is ahead of AO, the measurement is negative. Defines the sagittal relationship of the maxilla and mandible (Norm: −1 ± 2mm).[19]
Pillar 2: Analysis of incisor position
1.NA, the angle formed between the line that passes through the axis of the upper central incisor and the NA line. Defines the degree of buccal inclination of these teeth (Norm: 23º).
1. NB, the angle formed between the line that passes through the axis of the lower central incisor and the NB line. Defines the degree of buccal inclination of these teeth (Norm: 25º).
1-NA, horizontal linear distance between the NA line and the most prominent point of the upper incisor. Defines the degree of protrusion of the upper incisor (Standard 4 mm).
1-NB, horizontal linear distance between the NB line and the most prominent point of the lower incisor. Defines the degree of protrusion of the lower incisor (Norm 4 mm).
Pillar 3: Vertical analysis of the growth pattern
FMA, the angle formed between the Frankfurt plane, traced by points Porion (Po), Orbitale (Or) and the mandibular plane, defined by points Gonion (Go), Menton (Me). Defines growth in the patient’s vertical direction (Norm 25°), first described by McNamara.[18]
If these data are out of normality, they will be transferred to the problem list.
If the orthodontist is already used to working with a different analysis from the measurements presented in this work, he or she will only select the variables related to the 3 pillars of the analysis of his or her preference. If these data are out of normality, they will be transferred to the problem list.
Anamnesis: Obtaining patient history data
The anamnesis guide [Annex 1 and 2] of the FOCA method was created as an assessment tool, considering information that can be complementary or decisive for the treatment plan. Two different guides are used, one for interceptive orthodontics, this being a more complete version, and a guide for corrective orthodontics. Below, we will present the most complete version of this instrument:
Common points of interest and family environment. It is already known that patients with a good relationship with the orthodontist tend to be more collaborative with the use of appliances, accessories, and oral hygiene. At this point in the anamnesis, it is possible to establish meeting points and connections with the patient, improving communication from the beginning. The time invested in establishing relationships with patients will be less than necessary to correct potential problems.[20] Another important point is the family structure. If the school period is full-time, if the parents are divorced, or if the child stays with grandparents part-time. All these points are defined in interceptive orthodontics as whether the treatment will be with removable or fixed appliances.
Heredity: At this point consider information related to facial growth, growth anomalies such as Pattern II, III, short or long face, and asymmetries. You should also ask about dental anomalies in the family.
Medical history: At this point, we ask about the patient’s general health status, hormonal imbalances, and drug use. Drug interactions with orthodontic movement can occur with the use of anti-inflammatories, corticosteroids, estrogens, and bisphosphonates, among others. According to the literature, to have an impact on tooth movement, the dose must be high the period of action very long, and the application must be local.[21]
Menarche: Girls who have already experienced menarche are always on the growth curve before the peak ends. The average age of menarche is 12.59 years (minimum age = 9.9, maximum age = 16.2).[22]
Habits: Investigate sucking habits, biting nails, and objects, in case of a positive answer, we can intervene in the persistence of these habits.
Trauma and tooth loss: This can cause delayed eruption, retained teeth, and the need for traction. Side effects in occlusion such as loss of vertical dimension, extrusion, and mesial inclination of molars. Trauma in childhood may also be related to episodes of articular disc displacement.
Oral or nasal breathing and snoring symptoms: At this step, the tone and posture of the lips should be observed at rest; as well as the quality and dryness of enamel and gums. Mouth-breathing patients may experience gum inflammation and bleeding due to direct air contact with the mucosa. On lateral teleradiography, the patient may present signs of obstruction due to adenoid hypertrophy, radiographically identified by the increase in volume in the posterior wall of the nasopharynx.[23] It is possible to perform respiratory tests in the office, such as the “swallow of water” technique. For this purpose, the patient is asked to fill the mouth with water. The orthodontist must observe the patient for approximately 3 min to detect whether the corner of the lip is passive or responding to the stimulus of effort to keep the water in the mouth. If the patient keeps the corner of the lip at rest, without effort, it is considered that their nasal airflow is normal. If, on the contrary, the patient spits out the water or makes a great effort to keep it in the mouth, it is suspected that there is some degree of nasal obstruction and it is recommended to refer the patient to the otorhinolaryngologist. If the patient passes the test but still presents mouth breathing, there is a need to refer him to a speech therapist with the main objective of improving lip tone.[24] The patient’s complaints, associated with clinical signs of obstruction or normal breathing, must be considered to decide between the need for expansionist treatment protocols or those involving mandibular protrusion.
Speech changes: Related to anterior open bite and anterior tongue pressure.[24]
Bruxism and TMJ changes: Bruxism is characterized by several combined signs and symptoms, such as tooth wear or fractures, dental marks in soft tissues, temporomandibular disorders, headaches, and behavioral and sleep disorders. The orthodontist should be concerned when there is wear on the crowns of permanent teeth, which can direct treatment considering the signs and symptoms.[25] It is worth mentioning that bruxism is a risk factor for TMJ disorders in children and adults.[26] The most common findings in patients with TMJ disorders are restriction of mouth opening, clicking, and hyperalgesia, which generally occurs when applying pressure to the chewing muscles or TMJ. Isolated muscle pain, disc displacement with and without reduction, degenerative pathologies, and subluxation are common clinical conditions in the population.[27] At the sign of any of these pathologies, the orthodontist should not begin orthodontic treatment before muscle pacification or recorticalization of the degenerative process. These findings can also influence the definition of orthodontic mechanics, always avoiding the use of intermaxillary elastics or fixed propulsors to avoid tension in the TMJ region.
Integration of obtained data
At this stage, the list of problems, therapeutic goals, treatment alternatives, and the final stages of treatment are established.
The list of problems is performed taking into account all aspects of facial, occlusal, cephalometry analysis, and anamnesis data. It is assumed that if the orthodontist has a problem, he must find a solution. To do this, he separately describes the standard deviations found in the examinations.
Therapeutic goals are made based on the patient’s limitations such as growth pattern, according to Siécola et al.,[9] what is possible to achieve and what is impossible to expect through orthodontic camouflage. Other limitations may also be imposed by periodontal conditions, tooth loss, and general health problems that may bring limitations concerning treatment expectations. The therapeutic goals also must be described considering the patient’s reality in terms of conduct, personality, and psychological state.[28]
Alternatives should always be considered before determining the sequence, presenting the pros and cons of each possible treatment. To this end, variations are explained to the patient concerning the final stability of the case, cost-benefit, esthetic effects on the face, functional benefits, the option to rehabilitate with a prosthesis/implant or close prosthetic spaces orthodontically, and treatment time. The final treatment plan is made in the last stage, after the entire diagnostic process, dividing the case into phases. In the case of interceptive treatments, the current treatment is predicted and the need for monitoring until the end of growth and a possible second corrective intervention requiring further examinations is explained to the patient. In corrective treatments, the phases are divided into alignment and leveling, transverse, vertical, sagittal correction, closure of spaces in case of extractions, finishing, and containment.
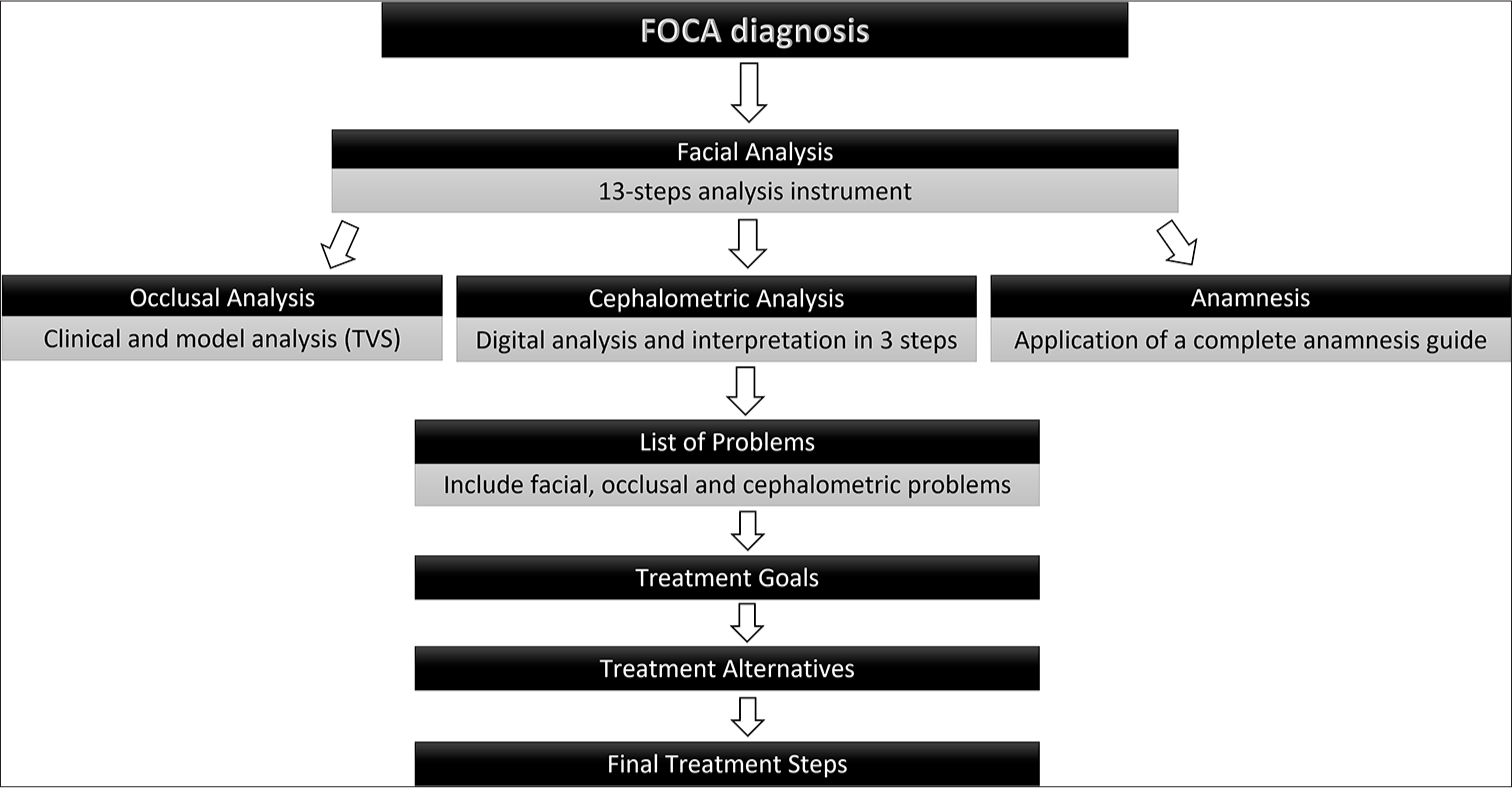
- Sequence of the facial, occlusal, cephalometric, and anamnesis (FOCA) diagnostic method. TVS: Transverse, vertical, and sagittal
The FOCA methodology [Figure 6] allows the orthodontist or orthodontic student to guide the diagnostic thinking to the detailed treatment plan in an orderly and detailed way. The method is easy to execute and can be applied in private practices and postgraduation centers. Future experimental studies are needed using the method to obtain statistical data investigating the quality of recognition of medium and high-complexity cases based on the application of the described instruments.
CONCLUSION
The FOCA diagnostic method and the instruments created for its implementation are a resource for systematizing the patient’s relevant information to create a more assertive treatment plan with the harmony of the face as the main therapeutic goal.
Ethical approval
Institutional Review Board approval is not required.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirms that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship Nil.
References
- The diagnostic facial triangle in the control of treatment objectives. Am J Orthod Dentofac Orthop. 1969;55:651-67.
- [CrossRef] [PubMed] [Google Scholar]
- How important are lateral cephalometric radiographs in orthodontic treatment planning? Am J Orthod Dentofac Orthop. 2011;139:175-81.
- [CrossRef] [PubMed] [Google Scholar]
- Comparison of craniofacial characteristics of typical chinese and caucasian young adults. Eur J Orthod. 2011;33:205-11.
- [CrossRef] [PubMed] [Google Scholar]
- Cephalometric soft tissue facial analysis. Am J Orthod Dentofacial Orthop. 1999;116:373-89.
- [CrossRef] [PubMed] [Google Scholar]
- Facial keys to orthodontic diagnosis and treatment planning. Part I. Am J Orthod Dentofac Orthop. 1993;103:299-312.
- [CrossRef] [PubMed] [Google Scholar]
- AP Relationship of the maxillary central incisors to the forehead in adult white females. Angle Orthodontist. 2008;78:662-9.
- [CrossRef] [PubMed] [Google Scholar]
- Teleorthodontics education model for orthodontic residents: A preliminary study. J Telemed Telecare. 2023;1:13-23.
- [Google Scholar]
- Anteroposterior relationship of the maxillary central incisors to the forehead in adult white males. Orthodontics (Chic). 2013;14:e2-9.
- [CrossRef] [PubMed] [Google Scholar]
- Subjective facial analysis and its correlation with dental relationships. Dental Press J Orthod. 2017;22:87-94.
- [CrossRef] [PubMed] [Google Scholar]
- Perceptions of orthodontic case complexity among orthodontists, general practitioners, orthodontic residents, and dental students. Am J Orthod Dentofacial Orthop. 2017;151:335-41.
- [CrossRef] [PubMed] [Google Scholar]
- Perceptions of orthodontic residents toward the implementation of dental technologies in postgraduate curriculum. BMC Oral Health. 2023;23:625.
- [CrossRef] [PubMed] [Google Scholar]
- Artificial intelligence in orthodontics and orthognathic surgery: A bibliometric analysis of the 100 most-cited articles. Head Face Med. 2023;19:1-11.
- [CrossRef] [PubMed] [Google Scholar]
- Natural position of the head: Review of two-dimensional and three-dimensional methods of recording. Br J Oral Maxillofac Surg. 2016;54:233-40.
- [CrossRef] [PubMed] [Google Scholar]
- Evaluation of aesthetic anteroposterior position of maxillary incisors in patients with extraction treatment using facial reference lines. J Int Med Res. 2019;47:2951-60.
- [CrossRef] [PubMed] [Google Scholar]
- Dentofacial characteristics in orthodontic patients with centric relation-maximum intercuspation discrepancy. Angle Orthod. 2014;84:939-45.
- [CrossRef] [PubMed] [Google Scholar]
- Reliability of Bolton analysis evaluation in tridimensional virtual models. Dental Press J Orthod. 2015;20:72-7.
- [CrossRef] [PubMed] [Google Scholar]
- Rev Dent Press Ortod Ortop Facial. 2006;11:44-54.
- [CrossRef] [Google Scholar]
- A method of cephalometric evaluation. Am J Orthod Dentofacial Orthop. 1984;86:449-69.
- [CrossRef] [PubMed] [Google Scholar]
- The “Wits” appraisal of jaw disharmony. Am J Orthod Dentofacial Orthop. 1975;67:125-38.
- [CrossRef] [PubMed] [Google Scholar]
- Perceived orthodontist behaviors that predict patient satisfaction, orthodontist-patient relationship, and patient adherence in orthodontic treatment. Am J Orthod Dentofacial Orthop. 1996;110:370-7.
- [CrossRef] [PubMed] [Google Scholar]
- The influence of medication on orthodontic tooth movement: a critical review of the literature. Rev Dent Press Ortod Ortop Facial. 2005;10:122-30.
- [CrossRef] [Google Scholar]
- BMI at menarche and timing of growth spurt and puberty in polish girls-longitudinal study. Anthropol Anz. 2019;76:37-47.
- [CrossRef] [PubMed] [Google Scholar]
- Evaluation of lateral cephalometric radiography as a mean of diagnosing adenoids hypertrophy. Rev Dent Press Ortod Ortop Facial. 2009;14:83-91.
- [CrossRef] [Google Scholar]
- Guidelines proposal for clinical recognition of mouth breathing children. Dental Press J Orthod. 2015;20:39-44.
- [CrossRef] [PubMed] [Google Scholar]
- Bruxism in children: What do we know? Narrative Review of the current evidence. Eur J Paediatr Dent. 2023;24:207-10.
- [Google Scholar]
- Bruxism: A summary of current knowledge on aetiology, assessment and management. Oral Surg. 2020;13:358-70.
- [CrossRef] [Google Scholar]
- The evolution of TMD diagnosis: Past, present, future. J Dent Res. 2016;95:1093-101.
- [CrossRef] [PubMed] [Google Scholar]
- A full diagnostic process for the orthodontic treatment strategy: A documented case report. Dent J (Basel). 2020;8:41.
- [CrossRef] [PubMed] [Google Scholar]




