

Translate this page into:
Is there a relationship between transverse maxillary deficiency and sella turcica: A cephalometric analysis study?


*Corresponding author: Semiha Arslan, Department of Orthodontics, Faculty of Dentistry, Bolu Abant İzzet Baysal University, Bolu, Turkey. semmarslan@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Deniz Y, Arslan S. Is there a relationship between transverse maxillary deficiency and sella turcica: A cephalometric analysis study? APOS Trends Orthod 2021;11(2):116-22.
Abstract
Objectives:
The aim of this study was to investigate the dimensions and morphological variations of sella turcica and to test whether a relationship exists between sella turcica and transverse maxillary deficiency.
Materials and Methods:
The cephalometric radiographs of patients older than 17.99 years, which have been taken before the orthodontic treatment, and patient records were analyzed to investigate sella turcica dimensional and morphological analysis. Linear measurements of sella are as follows sella length, sella width, sellar area, sella height anterior, posterior, and median. The sella turcica morphological shape analysis was performed into six groups (normal sella turcica, oblique anterior wall, sella turcica bridge, double contour of floor, irregularities of the posterior part of the dorsum sella, and pyramidal shape of the dorsum sella). The width of the maxillary arch is measured by the digital caliper. Male participants with a maxillary width of less than 30.8 mm and a maxillary width of less than 31.1 mm in female patients in the first molar region were determined as a transverse maxillary deficiency. The mean dimensions of sella turcica and the relationship between cases with transverse maxillary deficiency and non-skeletal anomaly were compared using independent samples t-tests. The transverse maxillary deficiency and the sellar morphology relationship were compared using Chi-square test. Post hoc multiple comparisons and analyzes were performed at 95% confidence interval by Bonferroni correction.
Results:
The sella length measurements yielded higher values among the patients with transverse maxillary deficiency (P < 0.05). The normal sella morphology had quantitative superiority in patients without skeletal anomaly in comparison with transverse maxillary deficiency cases (P < 0.05). It was observed that the sella turcica bridge had a statistically superiority in patients with transverse maxillary deficiency (P < 0.05).
Conclusion:
The increased sellar measurement and sella turcica bridging, may provide knowledge about possible transverse maxillary deficiency.
Keywords
Cephalometric radiographs
Transverse maxilla deficiency
Sella turcica bridge

INTRODUCTION
The sella turcica is a depression located on the superior surface of the sphenoid bone, and the pituitary gland is located in the sella turcica. The sella turcica is of great significance in determining growth during and estimating the results of orthodontic treatment. Moreover, it is an important anatomical structure in the radiographic analysis of the neuro-cranial and craniofacial complex. The s-point, which plays an important role in the cephalometric analysis of dentofacial structures during orthodontic examinations, is located at the center of the sella turcica.[1]
In the previous studies, it was reported that the development of the pituitary gland and the development of the sella turcica are in close relationship and that any developmental deviation in the pituitary gland causes a similar deviation in the sella turcica.[2] The pituitary gland consists of the anterior lobe, the medial lobe, and the posterior lobe.[3] Growth hormone is released from the adenohypophysis located at the anterior segment of the sella turcica; thus, the anterior segment of the sella turcica is under the effects of the adenohypophysis gland, which influences the growth of the craniofacial regions.
Kjær reported that deviations in the posterior wall of the sella turcica may cause malformations in the brain, whereas deviations in the anterior wall may cause deviations in the frontonasal region.[2] Various studies have been carried out to compare frontonasal and maxillofacial growth with the morphology of the sella turcica.[4-6] Shrestha et al. reported a relationship between the length and anteroposterior width of the sella and Class I, Class II, and Class III malocclusions.[4]
Besides, a study comparing the sellar widths of patients receiving orthodontic treatment and those receiving surgical-orthodontic treatment reported that the sellar area was larger among the patients receiving surgical-orthodontic treatment.[5] Baidas et al. observed a relationship between the morphological characteristics and dimensions of the sella in Class I and Class II malocclusions.[6] However, no known study investigating the relationship between transverse maxillary deficiency and sella turcica dimensions has been conducted.
Thus, the aim of the present study was to determine how variations in the size and morphology of the sella turcica affect transverse maxillary deficiency cases. The null hypothesis of the present study was that there is no relationship between sella turcica dimensions, sella turcica morphology, and transverse maxillary deficiency.
MATERIAL AND METHODS
This retrospective study design based on recorded data was approved by Bolu Abant İzzet Baysal University Clinical Research Ethics Committee (Decision No: 2019/269). Clinical findings and cephalometric analysis were used for patient selection for the study and control groups. In this retrospective study approach, the cephalometric radiographs, which had been taken before orthodontic treatment, and patient records of 372 patients receiving treatment at the Orthodontic Clinic of Bolu Abant İzzet Baysal University between January 2016 and April 2020 were analyzed. The inclusion criteria were as follows: (1) Older than 17.99 years (Apposition of the tuberculum sella and resorption of the posterior edge continue through the age of 16 to 18 years.[1,7,8] For this reason, patients aged ≥18 years were involved in the present study, (2) no history of orthognathic surgery, (3) no trauma in the head and neck region, (4) systemically healthy, (5) availability of cephalometric images suitable for analyzing sella measurement, and (6) cases with Class I occlusion.
The sample size was computed according to Alkofide’ study that used 60 radiographs for each group, by the ClinCalc post hoc power calculator (https://clincalc.com/stats/ samplesize.aspx).[9] The sample size established 63 participants for each group to detect a large effect size (d = 0.80) with a power of 85% and a two-sided significance level of 5%. Hence, 80 samples were taken in each group (study group and control group). The total sample size in the study was 160.
Features of cephalometric radiography
Pretreatment cephalometric images taken using the Vatech panoramic-cephalometric device (Vatech, PaX-Uni3D, Yongin, Republic of Korea) were used. The cephalometric radiographs of all the patients were taken by an experienced X-ray technician using the same device and the same standard method. All radiographs used in the present study had good radiological quality for showing the anatomy of the sella turcica and the craniofacial complex. The mid-sagittal magnification was 110%, and all images were calibrated using NIH before the linear measurements, after which the analyses were performed.
Transverse maxillary deficiency describing criteria
In the current study cases with Class I occlusion were included in the study, patients with Class II and Class III malocclusion were excluded from the study. Skeletal type classification into Class I, Class II or, Class III was based on the ANB, beta angle, and W angle. Parameters of Class I malocclusion type measured on cephalometric radiographs were based for ANB angle 0–4 degree,[9] for beta angle 27° and 35°,[10] and for W angle 51° and 56°.[11] The patients were grouped into the Class I group when at least two out of three of the parameters were defined as that.
For determination transverse maxillary deficiency, Howe et al.[12] procedure was used to measure trans-arch widths. Dental model measurements of cases with Class I occlusion made with a digital caliper for arch width predictions of the maxillary arch between the right and left antimeres of the first premolars and the first molars according to the indexes of Howe.[12] The values for the between the right and left antimeres of the first premolars are recorded on the palatal aspect at the cervical margin of the tooth on its point of greatest convexity; for the first molar, at the point on the cervical margin adjacent to the lingual Groove [Figure 1]. Female cases with transverse distance between the first premolar teeth of the upper jaw <22.8 mm and distance between the first molar teeth <30.8 mm; in male cases transverse distance between the first premolar teeth of the upper jaw <23.5 mm and distance between the first molar teeth <31.1 mm were included in the group with transverse maxillary deficiency malocclusion.
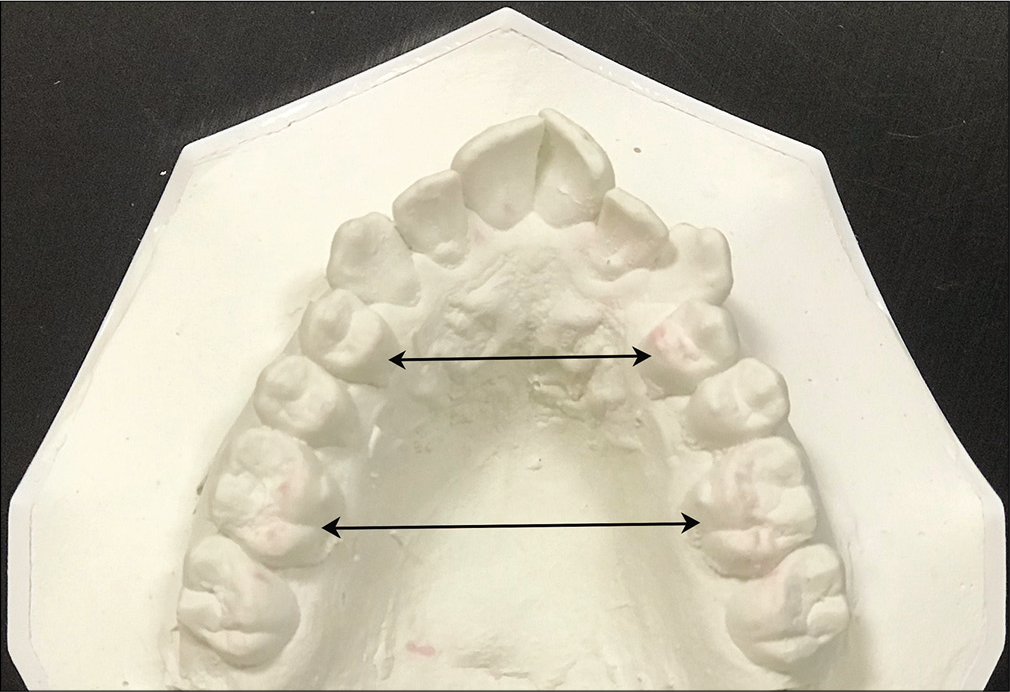
- Evaluation of transverse maxillary deficiency on dental model. The upper black arrow describes the transversal width between the cervical margins of the first premolars measured by the digital clipper, and the lower one describes the measured transversal distance between the first molars.
Class I cases without transverse maxillary deficiency determined with Howe’ index were included in the control group.
Cephalometric tracing of the sella turcica
Sella turcica morphology analysis
The morphological shape of the sella was classified by making use of the study carried out by Axelsson et al.[13] on regionally examining the tuberculum sella, dorsum sella, and sella floor. Axelsson et al.[13] classified sella turcica shape variations into six groups. These classifications were (1) normal sella turcica, (2) irregularity of the posterior wall of the sella turcica, (3) oblique anterior wall of the sella turcica, (4) double counter of the sella turcica floor, (5) sella turcica bridge, and (6) pyramidal shape of the sella turcica [Figure 2]. In the previous studies, relationships between the sellar bridges and malocclusions were reported. For this reason, when examining a class, attention was paid to ensure the samples had a single morphology. For instance, the cases having both a sellar bridge and irregularity at the posterior edge were excluded from the study.
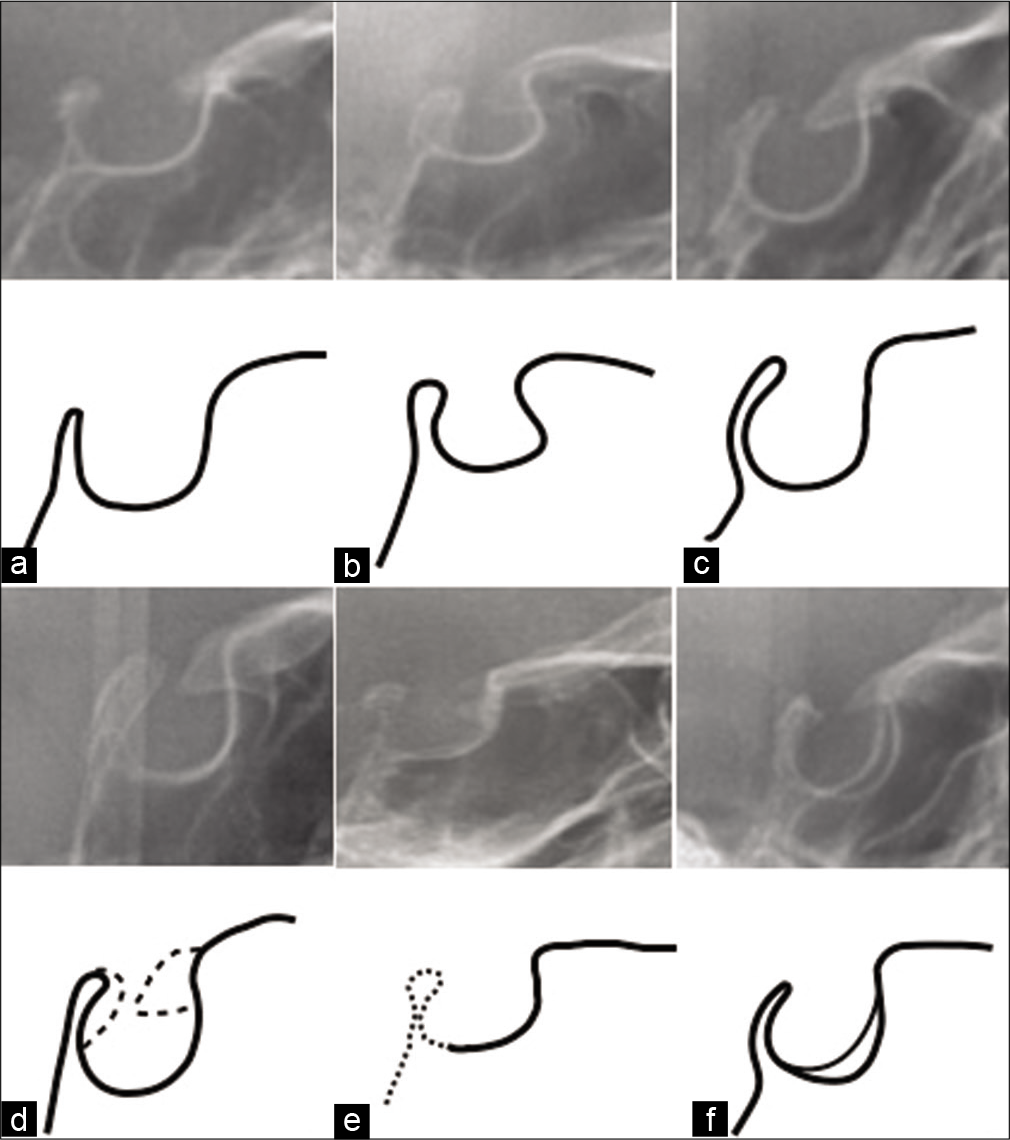
- Drawing and detailing of different morphological forms of sella turcica on cephalometric radiographs (a) normal sella turcica, (b) oblique anterior wall of the sella turcica, (c) pyramidal shape of sella turcica, (d) sella turcica bridge, (e) irregularity of the posterior wall of the sella turcica, (f) double counter of the sella turcica floor.
Sella turcica dimensional analysis
The dimensional analysis (length, depth, and diameter) of the sella turcica was performed by relying for reference on the study carried out by Andredaki et al.[14] who examined the sella turcica of 184 healthy Greek individuals. According to the results obtained by Andredaki et al.,[14] the linear measurements of the sella were as follows:
Sella length: The distance from the tuberculum sella to the posterior clinoid process
Sella width: The largest antero-posterior dimension. Sella width was measured from the posterior to the anterior of the sella, parallel to the Frankfort plane
Sella height anterior: The vertical height of the anterior sella was measured from the tuberculum sella to the sella floor, perpendicular to the Frankfort plane
Sella height posterior: The vertical height of the posterior sella was measured from the posterior clinoid process to the sella floor, perpendicular to the Frankfort plane
Sella height median: The vertical height of median area of sella was measured from the sella floor to a point midway between posterior clinoid process and tuberculum sella, perpendicular to the Frankfort plane
Sellar area: This was measured by joining a line from the posterior clinoid process to the tuberculum sella.
All radiographs were evaluated by an oral radiologist who has 10 years’ experience and an orthodontist under semi-dark lighting conditions. The 50 cephalometrics were selected randomly (Excel 15.0 Microsoft, Redmond, WA, USA) and re-evaluated 2 weeks after the first evaluations under the same conditions to determine intra-observer and inter-observer reliability.
Statistical analysis
Statistical analyses were performed using IBM Statistical Package for the Social Sciences version 21. The mean dimensions of the sella turcica and the relationship between the two groups were compared using an independent samples t-test. The relationship between gender and the dimensions of the sella turcica was also examined using the independent samples t-test. A Chi-square test was used to compare the relationship between transverse maxillary deficiency and sellar morphology. Post hoc multiple comparisons and analyses were performed using the Bonferroni correction at a 95% confidence interval. Coherence between the original and repeated measurements was examined using Cohen’s kappa coefficient. Cohen’s kappa analyses were interpreted as 0.00–0.10 being no agreement, 0.10–0.40 being poor agreement, 0.41–0.60 being moderate agreement, 0.61–0.80 being good agreement, and 0.81–1.00 is very good agreement. The statistical significance level was accepted as P < 0.05.
RESULTS
After excluding the images not meeting the inclusion criteria, the images of 80 patients (47 females and 33 males) in the study group and 80 patients (54 females and 26 males) in the control group were included in the present study. The kappa values were found to be between 0.78 and 1.00 for various image artifacts. Based on these values, good or very good agreement was found for intra-observer and inter-observer reliability.
After examining the relationship between gender and sellar dimensions using an independent samples t-test, it was determined that the sellar length was at a higher level among the males (P < 0.05). However, it was also found that the mean values of sellar width, sellar height anterior and media, and sellar area were at higher levels among the males, but without statistically significant differences (P > 0.05). The Chi-square analysis revealed no significant relationship between gender and transverse maxillary deficiency (P > 0.05) [Table 1].
| Female | Male | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| n | Mean±Std. Deviation | Std. Error Mean | Range | n | Mean±Std. Deviation | Std. Error mean | Range | P-value* | |
| Sella width | 101 | 10.5±1.79 | 0.70 | 6.3–13.9 | 59 | 11.2±1.61 | 1.25 | 5.7–14.1 | 0.561 |
| Sella length | 101 | 8.29±1.93 | 0.20 | 4.3–12.7 | 59 | 9.02±1.72 | 0.22 | 4.8–12.8 | 0.022* |
| Sella height ant | 101 | 7.29±1.58 | 0.16 | 4.0–14.3 | 59 | 7.59±1.59 | 0.21 | 3.3–9.8 | 0.273 |
| Sella height post. | 101 | 7.64±1.65 | 0.52 | 5.2–12.1 | 59 | 7.40±1.25 | 0.16 | 4.0–10.0 | 0.716 |
| Sella height med. | 101 | 7.32±1.59 | 0.16 | 4.7–11.9 | 59 | 7.39±1.21 | 0.16 | 4.7–13.0 | 0.783 |
| Sellar area | 101 | 9.55±2.08 | 0.22 | 7.3–16.4 | 59 | 10.9±1.43 | 1.08 | 5.9–14.0 | 0.140 |
Using the independent samples t-test to examine the relationship between sellar measurements and transverse maxillary deficiency, it was determined that the sellar length yielded higher values among the patients with transverse maxillary deficiency (P < 0.05) [Table 2]. Similarly, the relationship between sellar morphology and transverse maxillary deficiency was compared using crosstabs, and the intragroup differences were analyzed using post hoc multiple analyses with Bonferroni correction. It was thereby determined that normal sellar morphology has quantitative superiority in patients without any skeletal anomaly (P < 0.05). It was also observed that the sella turcica bridge had a statistical superiority in patients with transverse maxillary deficiency (P < 0.05) [Table 3]. No difference was found between females and males after examining the relationship between gender and sellar morphology using Chi-square analysis (P > 0.05) [Table 4].
| Transverse Maxillary Deficiency | Non-skeletal anomaly | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| n | Mean±Std. Deviation | Std. Error mean | Range | n | Mean±Std. Deviation | Std. Error mean | Range | P-value* | |
| Sella width | 80 | 10.96±1.79 | 0.98 | 5.7–13.9 | 80 | 10.64±1.61 | 0.85 | 6.3–14.1 | 0.802 |
| Sella length | 80 | 8.91±1.73 | 0.20 | 4.3–12.8 | 80 | 8.23±1.97 | 0.23 | 4.8–12.8 | 0.029* |
| Sella height ant | 80 | 7.49±1.39 | 0.16 | 4.0–9.8 | 80 | 7.32±1.76 | 0.20 | 3.3–14.3 | 0.524 |
| Sella height post. | 80 | 7.42±1.40 | 0.16 | 5.2–12.1 | 80 | 7.67±1.25 | 0.62 | 4.0–11.5 | 0.707 |
| Sella height med. | 80 | 7.45±1.29 | 0.15 | 4.8–11.9 | 80 | 7.24±1.59 | 0.18 | 4.7–13.9 | 0.398 |
| Sellar area | 80 | 9.87±1.69 | 0.19 | 6.3–16.4 | 80 | 10.27±1.43 | 0.86 | 5.9–15.4 | 0.653 |
| Transverse Maxillary Deficiency | Non-skeletal anomaly | P-value* | |
|---|---|---|---|
| Normal sella turcica | 25a | 41b | 0.001 |
| Oblique anterior wall | 7a | 4a | |
| Sella turcica bridge | 22a | 5b | |
| Pyramidal shape of the dorsum sella | 7a | 11a | |
| İrregularities of the posterior part of the dorsum sella | 13a | 15a | |
| Double countor of floor | 6a | 4a | |
| Total | 80 | 80 |
| Female | Male | P-value* | |
|---|---|---|---|
| Normal sella turcica | 43a | 23a | 0.791 |
| Oblique anterior wall | 5a | 6a | |
| Sella turcica bridge | 17a | 11a | |
| Pyramidal shape of the dorsum sella | 6a | 5a | |
| İrregularities of the posterior part of the dorsum sella | 17a | 9a | |
| Double countor of floor | 13a | 5a | |
| Total | 101 | 59 |
DISCUSSION
To determine whether the sella turcica region has an abnormal appearance, it is necessary to define what a normal morphological image is. The previous studies offered different evaluations regarding the morphology of the sella turcica. In the 1920s, Camp classified the shape of a normal sella into circular, oviform, and flat.[15] Teal used a similar classification, but also took the posterior wall and floor of the dorsum sella and anterior wall into consideration.[16] MeyerMarcotti et al. categorized it into arc, shallow, and J-shape.[17] In their study on individuals with Down syndrome between childhood and adulthood, Russell and Kjær categorized the morphology of the sella turcica into three subclasses: Almost normal sella, deviation of the anterior wall of the sella, and deviation of the floor of the sella.[18]
Axelsson et al.[13] examined and classified sella turcica morphologies in terms of six subclasses. In their study, which was carried out on healthy Norwegian individuals, they determined sellar morphologies with normal sella turcica, pyramidal shape, oblique anterior wall of the sella turcica, sella turcica bridge, double contour of the sella turcica, and irregularity of the posterior part of the dorsum sella. Besides, they reported normal sellar morphology in 71% of males and 65% of females. Moreover, they observed obliquity of the anterior wall more frequently among males and a sella turcica bridge along with irregularity of the posterior part of the dorsum sella more frequently among females.
Researchers have disagreed whether the anterior and posterior walls of the sella turcica have different embryologic origins and, as a result, whether the anterior and posterior parts should be regarded separately.[19] The pituitary gland consists of three parts: The anterior lobe (adenohypophysis), the middle lobe, and the posterior lobe (neurohypophysis).[3] Growth hormone is, however, secreted from the adenohypophysis. Hence, the anterior segment of the sella turcica is under the effects of adenohypophysis, which influences the growth of the craniofacial regions. Since the anterior part of the sella turcica is under the effects of the adenohypophysis gland, it is thought that deviations in growth should mainly influence the anterior part of the sella.[13,20,21] In this study, no relationship was observed between the anterior height of the sella, obliquity in the anterior part of the sella, and transverse maxillary deficiency.
The present study was carried out on a limited number of patients using plain radiography, and it is necessary to expand the dataset and to conduct examinations using three-dimensional imaging to more thoroughly investigate the relationship between transverse maxillary deficiency and maxillofacial growth.
In addition to the effects of genetic factors on sellar morphology, researchers have also postulated that environmental factors have a significant effect on morphology. In their study carried out on monozygotic twins, Townsend et al. reported that the dimensions of the sella turcica depended on environmental factors as well as genetic factors.[22] In their study on monozygotic twins and non-twin individuals, Jacobsen et al. reported that the dimensions of the sella turcica were somewhat similar and somewhat different among the twin pairs.[23] To achieve more precise results in future studies, it is recommended to examine the relationship between sellar measurements and maxillofacial development by considering the medical records and general health status of the participating individuals.
The relationship between sella turcica bridging with craniofacial anomalies and skeletal malocclusion has been reported in many studies.[5,17,24-27] In the present study, individuals having single sellar morphology were included in the study. For this reason, the number of study group participants was significantly limited. In this study, which was carried out according to the classifications made by Axelsson et al.[13] one of the sellar morphologies was the sellar bridge, which was observed in 22 patients in the study group and five patients in the control group. A relationship was found between sellar bridge and transverse maxillary deficiency, which is a skeletal anomaly (P < 0.05). However, the relationship between transverse maxillary deficiency and sellar bridge has not yet been reported in the literature.
Studies on sellar size have been carried out since the 1950s.[1,7,8,13,28] It is thought that the dimensional measurements of the sella might be affected by various factors, such as individual variations, gender, age, skeletal patterns, and various anomalies. However, in their studies, Yassir et al.[29] and Alkofide[9] reported that there was no statistically significant difference between girls and boys in terms of dimensional measurements. Moreover, Axelsson et al.[13] found no difference between the genders in terms of depth and diameter; however, they did report that the sellar length among the boys was statistically significantly longer than among the girls at ages 12, 15, and 18. In contrast with this result, Francis[30] reported that the sellar dimensions were found to be larger among the girls as compared to the boys.
In their study carried out on healthy Nepalese individuals aged between 18 and 30 years, Shrestha et al.[4] found no statistically significant differences between the age groups or between the genders. In this study carried out on individuals older than 17.99 years, the number of female individuals was superior to the male individuals in the control group. Although it has been thought that this superiority might statistically influence the results, it was reported in previous studies that there was no statistically significant difference other than sellar length between the genders.[4] The differences between the results obtained in the previous studies might be related to the ethnic origin of the population being examined, genetic and environmental conditions, and the cephalometric radiography method used.
Besides the teeth, the neural crest cells also play a role in the development and formation of the sella turcica. Similar to the development of teeth, the anterior segment of the sella turcica is mainly formed by the neural crest cells.[2] This similarity in embryological origin has directed researchers toward examining the relationship between dental and skeletal anomalies and the sella turcica. For example, Leonardi et al. reported a relationship between sellar bridge and dental anomalies.[25] In their study, Baidas et al.[6] compared Class I and Class II cases using linear measurements of sellar size and found no statistically significant differences. They reported that the sellar width was wider among the Class II individuals and narrower among the Class I individuals. For their part, in a study examining variations in sellar size among Classes I, II, and III individuals, Shrestha et al. reported that both length and anterior-posterior width were in the order of Class III, Class I, and Class II.[4] Ali et al. showed that the frequency of sellar bridging was significantly higher in subjects with canine impaction.[31] Controversly, Ortiz et al. reported that there was no statistically important relationship between palatal canine impaction with sellaturcica bridging in their study conducted by 3D CBCT.[32]
In the present study, which examined sellar differences between patients with transverse maxillary deficiency and patients with no skeletal anomaly, it was determined that patients with transverse maxillary deficiency had longer sellar length.
The most important limitation of the present study is that it was carried out using only two-dimensional cephalometric graphs. This method prevents the obtaining of the actual anatomical measurements of the sella turcica. Another limitation of the study is that the measurements and assessments were performed by a single observer, which limited the ability to specify the morphological shapes of the sella turcica and determine sella turcica bridging. Studies carried out using three-dimensional graphs or cadavers might yield more reliable results for comparing sella turcica morphology and maxillofacial skeletal defects. Besides, the fact that the study was conducted on a subpopulation presents another limitation.
CONCLUSION
The present study determined that cephalometric radiography is a method that can be very effectively used to examine the dimensions of the sella turcica
The null hypothesis of the present study – that no relationship would be found between transverse maxillary deficiency and size and morphology of the sella turcica – was rejected
Sella turcica length was longer in patients with transverse maxillary deficiency
The frequency of sella turcica bridging was higher in patients with transverse maxillary deficiency versus those with no skeletal anomaly
Sella turcica length was longer in the males in this study, but gender did not influence on the other dimensions of the sella turcica.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Cranial base development: A follow-up x-ray study of the individual variation in growth occurring between the ages of 12 and 20 years and its relation to brain case and face development. Am J Orthod. 1955;41:198-225.
- [CrossRef] [Google Scholar]
- Orthodontics and foetal pathology: A personal view on craniofacial patterning. Eur J Orthod. 2009;32:140-7.
- [CrossRef] [PubMed] [Google Scholar]
- Imaging the sella and parasellar region. Neuroimaging Clin N Am. 2005;15:203-19.
- [CrossRef] [PubMed] [Google Scholar]
- The morphology and bridging of the sella turcica in adult orthodontic patients. BMC Oral Health. 2018;18:45.
- [CrossRef] [PubMed] [Google Scholar]
- Bridging and dimensions of sella turcica in subjects treated by surgical-orthodontic means or orthodontics only. Angle Orthod. 2005;75:714-8.
- [Google Scholar]
- Association of sella turcica bridging with palatal canine impaction in skeletal Class I and Class II. Clin Cosmet Investig Dent. 2018;10:179-87.
- [CrossRef] [PubMed] [Google Scholar]
- The cranial base; the postnatal development of the cranial base studied histologically on human autopsy material. Acta Odontol Scand. 1974;32:57-71.
- [Google Scholar]
- Normal and abnormal growth of the mandible. A synthesis of longitudinal cephalometric implant studies over a period of 25 years. Eur J Orthod. 1983;5:1-46.
- [CrossRef] [PubMed] [Google Scholar]
- The shape and size of the sella turcica in skeletal Class I, Class II, and Class III Saudi subjects. Eur J Orthod. 2007;29:457-63.
- [CrossRef] [PubMed] [Google Scholar]
- A new approach of assessing sagittal discrepancies: The Beta angle. Am J Orthod Dentofacial Orthop. 2004;126:100-5.
- [CrossRef] [PubMed] [Google Scholar]
- A new approach of assessing sagittal dysplasia: The W angle. Eur J Orthod. 2013;35:66-70.
- [CrossRef] [PubMed] [Google Scholar]
- An examination of dental crowding and its relationship to tooth size and arch dimension. Am J Orthod. 1983;83:363-73.
- [CrossRef] [Google Scholar]
- Post-natal size and morphology of the sella turcica. Longitudinal cephalometric standards for Norwegians between 6 and 21 years of age. Eur J Orthod. 2004;26:597-604.
- [CrossRef] [PubMed] [Google Scholar]
- A cephalometric morphometric study of the sella turcica. Eur J Orthod. 2007;29:449-56.
- [CrossRef] [PubMed] [Google Scholar]
- Normal and pathological anatomy of the sella turcica as revealed by roentgenograms. AJR Am J Roentgenol. 1924;12:143-56.
- [Google Scholar]
- Morphology of the sella turcica in Axenfeld-Rieger syndrome with PITX2 mutation. J Oral Pathol Med. 2008;37:504-10.
- [CrossRef] [PubMed] [Google Scholar]
- Postnatal structure of the sella turcica in down syndrome. Am J Med Genet. 1999;87:183-8.
- [CrossRef] [Google Scholar]
- Sella turcica morphology and the pituitary gland-a new contribution to craniofacial diagnostics based on histology and neuroradiology. Eur J Orthod. 2012;37:28-36.
- [CrossRef] [PubMed] [Google Scholar]
- The adenohypophysis and the cranial base in early human development. J Craniofac Genet Dev Biol. 1995;15:157-61.
- [Google Scholar]
- Axial skeleton and pituitary gland in human fetuses with spina bifida and cranial encephalocele. Pediatr Pathol Lab Med. 1996;16:909-26.
- [CrossRef] [PubMed] [Google Scholar]
- Epigenetic influences may explain dental differences in monozygotic twin pairs. Aust Dent J. 2005;50:95-100.
- [CrossRef] [PubMed] [Google Scholar]
- The morphology of the sella turcica in monozygotic twins. Twin Res Hum Genet. 2009;12:598-604.
- [CrossRef] [PubMed] [Google Scholar]
- A sella turcica bridge in subjects with severe craniofacial deviations. Eur J Orthod. 2000;22:69-74.
- [CrossRef] [PubMed] [Google Scholar]
- A sella turcica bridge in subjects with dental anomalies. Eur J Orthod. 2006;28:580-5.
- [CrossRef] [PubMed] [Google Scholar]
- Sella turcica bridging as a predictor of Class II malocclusion-an investigative study. J Stomatol Oral Maxillofac Surg. 2018;119:482-5.
- [CrossRef] [PubMed] [Google Scholar]
- Relation between bridging and dimensions of sella turcica and skeletal anomaly. J Fac Dent Atatürk Univ. 2009;19:177-80.
- [Google Scholar]
- Roentgen standards fo-size of the pituitary fossa from infancy through adolescence. Am J Roentgenol Radium Ther Nucl Med. 1957;78:451-60.
- [Google Scholar]
- Size and morphology of sella turcica in Iraqi adults. Al Mustansiria Dent J. 2010;7:23-30.
- [Google Scholar]
- Association between sella turcica bridging and palatal canine impaction. Am J Orthod Dentofacial Orthop. 2014;146:437-41.
- [CrossRef] [PubMed] [Google Scholar]
- A CBCT investigation of the Association between sella-turcica bridging and maxillary palatal canine impaction. Biomed Res Int. 2018;2018:4329050.
- [CrossRef] [PubMed] [Google Scholar]




