

Translate this page into:
Perception of dental professionals and lay people to altered facial esthetics

*Corresponding author: Dr. Talat Al-Gunaid, Department of Orthodontics and Pediatric Dentistry, Faculty of Dentistry, Taibah University, P. O. BOX: 2898, Madinah, Kingdom of Saudi Arabia. Phone: +966-505354055. gunaid2000@hotmail.com
-
Received: ,
Accepted: ,
Abstract
Introduction
The aim of this study was to examine whether dental professionals and lay people group do agree in their perception of digitally altered facial components or not.
Materials and Methods
A frontal photograph of a Saudi young man was taken, imported, and digitally altered to a series of images of 16 photographs. Eyes, nose, mouth, and chin were altered gradually from the original photograph and were rotated 1°, 3°, and 5°. 225 raters (60 lay people, 41 orthodontists, 77 dentists, and 47 dental students) were invited and asked to evaluate the original and altered images using a visual analog scale.
Results
Lay people were less critical and gave higher ratings than dentists when evaluating rotated eyes of 5°. Orthodontists gave higher ratings than lay people and dental students at distinguishing of 1° of rotated nose. Orthodontists were less critical in rating larger alterations of the nose at 3° than lay people. Orthodontists were also less discriminating of minor alterations of the lips. They could not detect mouth rotation of 1° compared to lay people and dental students.
Conclusions
The results of this study underline the importance of developing an objective index to enumerate the magnitude of facial asymmetries.
Keywords
Dental professionals
Facial asymmetry
Perception

INTRODUCTION
Much attention has been devoted to facial harmony and attractiveness. Facial symmetry is also considered as an important factor in determining facial attractiveness. In our daily orthodontic practice, we often meet patients with facial asymmetry presented with asymmetric eyes, deviated nose or jaws. These patients are aware or unaware of their facial deformity. Therefore, it seems important for orthodontists, maxillofacial surgeons, and plastic surgeons to assess the position of all of these facial components before, during, and after orthodontic, orthognathic, and/or plastic surgery treatments.
Looking at the related literature, we can easily find many studies on facial esthetics that have either been based on lateral cephalometric radiographs or lateral facial photographs.[1-5] These studies did not take into account the fact that people view each other from the frontal view during face-to-face communication and this could influence the perception of facial attractiveness if used.[6,7] Several studies have investigated the impact of facial esthetics on overall facial attractiveness and reported that the relative positions of the nose, lips, and chin are significant soft tissue contributors to achieving a balanced facial profile,[8-11] and any alterations in one or more facial components are likely to be noticed by patients.[12,13]
Numerous studies have been conducted to assess the perception of facial attractiveness.[14-18] Some of them used boards of professionals,[15,16] panels of lay people,[14] or dual selections by both dental professionals and lay people.[17,18]
Romani et al.[19] raised the question “do orthodontists differ from lay people regarding their ability to detect differences in facial profile?.” Many authors have attempted to answer this question. Some of them reported that professionals and lay groups are in agreement,[20,21] whereas others suggested that the professional opinions regarding the evaluation of facial esthetics may not coincide with the perception and expectations of patients or lay people with various degrees of disagreement between groups.[7,18]
Meyer-Marcotty et al.[22] conducted a three-dimensional (3D) study to analyze the perception of facial asymmetry. They created a virtual 3D faces with various degrees of facial asymmetry with gradual alterations of different parts of the face. They invited three groups of raters (30 orthodontists, 30 maxillofacial surgeons, and 30 laymen). They concluded that the identification of asymmetry is independent of the profession of the raters and that laymen were able to detect asymmetries when located near the midline of faces.
The current study was designed to examine whether dental professionals and lay people groups agree in their perception of digitally altered facial components or not.
MATERIALS AND METHODS
A frontal photograph of a young man who met the following criteria was taken: Class I skeletal pattern, Class I molar and canine relationships, normal overjet and overbite, the absence of crowding, no previous orthodontic, orthognathic, or prosthodontic treatments, and no craniofacial deformities or trauma.
The photographic setup
The photographic setup consisted of a tripod supporting a digital camera (Canon ESO1100D, Tokyo, Japan) with a shutter speed of 1/60, relative aperture (f/4), effective pixels approximately 12.2 M, with canon lens (EF 50 mm F/1.8 ii). The subject was positioned on a line marked on the floor at a distance of 1 m from the camera. Adjustment of the tripod height allowed the optical axis of the lens to be in a horizontal position during the recording (natural head position).
The photograph was imported and digitally altered to a series of images using Adobe Photoshop (version CS3; Adobe Systems, Inc., San Jose, CA, USA). The alterations involved eyes (E), nose (N), lips (L), chin (C), and eyes + nose + lips + chin (ENLC) and non-altered photograph (original photograph) [Figure 1]. A total of 27 photographs were obtained. Each variable such as eyes, nose, lips, and chin was altered gradually from the original photograph and was rotated 1° to a maximum of 5°. After the manipulation, a complete file was created and uploaded to Google drive.
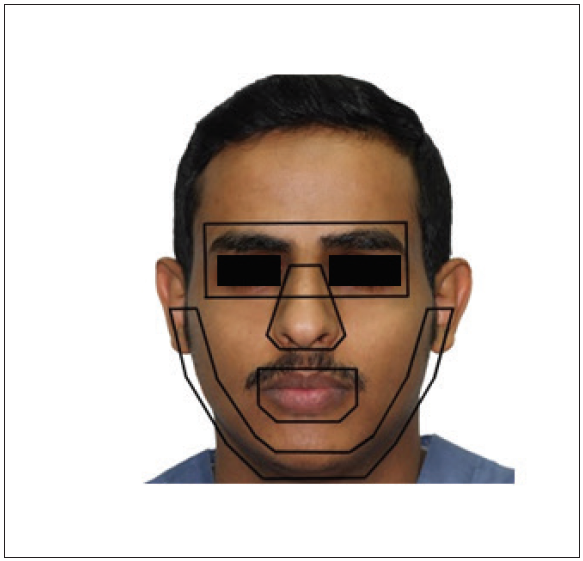
- Facial structures involved in this study.
Validation exercise
To examine the validity of the study, we administered a questionnaire to the ethical committee for final approval and invited 30 assessors to participate in evaluating the questionnaire and give their feedback about the following: Number of questions, questions’ clearness, grammatical mistakes, number of photos, and if the time were appropriate or not. The feedback from this exercise was to reduce the number of photos and to shorten the time required to answer the questionnaire so that the number of photos was reduced to 16 photos resulted in shorter time required to answer the questionnaire.
The questionnaire
A Google drive questionnaire template was used. This questionnaire consisted of two parts. The first part included demographic data regarding age, gender, nationality, level of education, profession, and years of experience and the second part included the evaluation of the rater’s perception of facial appearances from the frontal view of 16 photographs [Figure 2]. Different groups of raters were invited and were asked to evaluate the original and the altered images using a visual analog scale (VAS). On the VAS, each rater had the option to rate each photo from “very unattractive” to “very attractive.” The VAS score ranged from 0 to 5 points, with 0 being the minimum and 5 the maximum esthetic value. The total number of raters who took part in the study was 225 (60 lay people, 41 orthodontists, 77 dentists, and 47 dental students). Furthermore, the female-to-male ratio was 1.4:1.

- E 1: Rotated eyes of 1°, E 2: Rotated eyes of 3°, E 3: Rotated eyes of 5°, N 1: Inclined nose of 1°, N 2: Inclined nose of 3°, N 3: Inclined nose of 5°, L 1: Rotated lips of 1°, L 2: Rotated lips of 3°, L 3: Rotated lips of 5°, C 1: Rotated chin of 1°, C 2: Rotated chin of 3°, C 3: Rotated chin of 5°, eyes+nose+lips+chin (ENLC) 1: Rotated ENLC of 1°, ENLC 2: Rotated ENLC of 3°, ENLC 3: Rotated ENLC of 5°.
Statistical methods
Mean and standard deviation (SD) for each group of raters and comparisons between groups were done using one-way analysis of variance followed by Bonferroni post hoc test. All statistical analyses were done using the SPSS software (version 20, SPSS, IBM Corporation, USA). Our level of significance was set at P < 0.05.
ResultS
Table 1 shows the mean and SD of the scores for the four groups to altered eyes. No statistically significant differences were found between groups except that lay people were less critical and gave higher VAS ratings than dentists (P < 0.05) when evaluating rotated eyes of 5°.
| Variable | Lay people (n=60) | Orthodontists (n=41) | Dentists (n=77) | Dental students (n=47) | P value† | Bonferroni test |
|---|---|---|---|---|---|---|
| Mean±SD | Mean±SD | Mean±SD | Mean±SD | P value | ||
| Eyes (1°) | 2.58±1.37 | 3.20±0.84 | 2.82±1.21 | 2.57±1.16 | 0.05 | |
| Eyes (3°) | 2.38±1.42 | 2.37±1.11 | 2.13±1.17 | 2.13±0.88 | 0.48 | |
| Eyes (5°) | 1.80±1.46 | 1.73±1.23 | 1.17±1.19 | 1.47±1.16 | 0.020 | (Lay>Dent)* |
†Refers to ANOVA test, *P<0.05, SD: Standard deviation, VAS: Visual analog scale
Table 2 exhibits the comparison between groups to the altered nose. Significant differences were found in the altered nose of 1 and 3°. Orthodontists gave higher ratings than lay people and dental students at distinguishing of 1° of the rotated nose (P < 0.01) and the orthodontists were less critical in ratings larger alterations of the nose at level 3° than lay people (<0.05).
| Variable | Lay people (n=60) | Orthodontists (n=41) | Dentists (n=77) | Dental students (n=47) | P value† | Bonferroni test |
|---|---|---|---|---|---|---|
| Mean±SD | Mean±SD | Mean±SD | Mean±SD | P value | ||
| Nose (1°) | 2.75±1.34 | 3.46±0.98 | 3.06±1.13 | 2.66±1.17 | 0.005 | (Ortho>Lay)**, (Ortho>Stud)** |
| Nose (3°) | 2.62±1.46 | 3.34±0.99 | 2.88±1.27 | 2.64±1.05 | 0.02 | (Ortho>Lay)* |
| Nose (5°) | 2.52±1.56 | 2.85±1.17 | 2.27±1.22 | 2.19±1.08 | 0.06 |
†Refers to ANOVA test, *P<0.05, **P<0.01, SD: Standard deviation, VAS: Visual analog scale
As for lips alterations, the post hoc test showed that orthodontists were less discriminating of minor alterations of the lips. They could not detect mouth rotation of 1° compared to lay people (P < 0.01) and dental students (P < 0.05) [Table 3].
| Variable | Lay people (n=60) | Orthodontists (n=41) | Dentists (n=77) | Dental students (n=47) | P value† | Bonferroni test |
|---|---|---|---|---|---|---|
| Mean±SD | Mean±SD | Mean±SD | Mean±SD | P value | ||
| Lips (1°) | 2.73±1.36 | 3.49±0.87 | 3.01±1.13 | 2.77±1.13 | 0.007 | (Ortho>Lay)**, (Ortho>Stud)* |
| Lips (3°) | 2.90±1.36 | 3.24±0.92 | 3.08±1.07 | 2.72±1.04 | 0.14 | |
| Lips (5°) | 2.70±1.39 | 2.95±0.97 | 2.75±1.23 | 2.49±1.14 | 0.37 |
†Refers to ANOVA test, *P<0.05, **P<0.01, SD: Standard deviation, VAS: Visual analog scale
Table 4 shows the comparison between groups to the altered chin. No statistically significant differences were found between groups.
| Variable | Lay people (n=60) | Orthodontists (n=41) | Dentists (n=77) | Dental students (n=47) | P value† |
|---|---|---|---|---|---|
| Mean±SD | Mean±SD | Mean±SD | Mean±SD | ||
| Chin (1°) | 2.32±1.52 | 2.37±1.07 | 2.03±1.41 | 2.02±1.19 | 0.11 |
| Chin (3°) | 2.67±1.43 | 2.88±0.98 | 2.88±1.28 | 2.53±1.04 | 0.43 |
| Chin (5°) | 2.15±1.40 | 2.39±1.05 | 2.32±1.21 | 2.15±1.12 | 0.65 |
†Refers to ANOVA test, SD: Standard deviation, VAS: Visual analog scale
Table 5 exhibits the comparison between groups to altered ENLC. Lay people and dental students were significantly better than orthodontists at distinguishing a minor discrepancy of 1° alteration (P < 0.01).
| Variable | Lay people (n=60) | Orthodontists (n=41) | Dentists (n=77) | Dental students (n=47) | P value† | Bonferroni test |
|---|---|---|---|---|---|---|
| P value | ||||||
| Mean±SD | Mean±SD | Mean±SD | ||||
| ENLC (1°) | 2.42±1.46 | 3.41±0.77 | 2.80±1.13 | 2.53±1.21 | 0.001 | (Ortho>Lay)**, (Ortho>Stud)** |
| ENLC (3°) | 2.13±1.49 | 2.22±0.96 | 2.13±1.19 | 1.96±1.38 | 0.80 | |
| ENLC (5°) | 1.47±1.45 | 1.32±1.29 | 1.13±1.26 | 1.15±1.38 | 0.47 |
ENLC refers to: Eyes+Nose+Lips+Chin, †Refers to ANOVA test, **P<0.01, SD: Standard deviation, VAS: Visual analog scale
No statistically significant differences were found between groups when rating original photo [Table 6].
| Variable | Lay people (n=60) | Orthodontists (n=41) | Dentists (n=77) | Dental students (n=47) | P value† |
|---|---|---|---|---|---|
| Mean±SD | Mean±SD | Mean±SD | Mean±SD | ||
| Normal | 2.70±1.43 | 3.20±1.05 | 2.99±1.24 | 2.64±1.17 | 0.09 |
†Refers to ANOVA test, SD: Standard deviation, VAS: Visual analog scale
DISCUSSION
Perception of facial esthetics has been investigated to a great extent. Many investigators have attempted to assess, rank, and classify faces on the basis of their attractiveness using panels of laypersons,[14,23] panels of specialists,[15,16,24] or both specialists and laypersons.[1,12,17,18]
It was reported that including both perceptions of specialists and lay people could give better idea of what most orthodontic patients would desire from surgical orthodontic treatment and/or plastic surgery to achieve because what is pleasant or attractive to the specialists - based on their experience or training - might not agree with what our patients or other inexperienced persons think are beautiful.[4,14]
In the present study, a large number of raters from different ages, occupations, ethnic groups, and educational backgrounds were invited to participate in this study (lay people, orthodontists, dentists, and dental students) because we hoped and expected that their overall judgment would reveal a more comprehensive social perception of esthetics.
Several reports have reported that young people usually are not aware of taking the decision toward orthodontic treatment.[25-27] For this reason and in an attempt to minimize the influence of such factors on subjective esthetic judgment, the raters included in this study were 18 years old or older.
A comparison between groups to altered eyes showed that lay people were less critical and gave higher VAS ratings than dentists when evaluating rotated eyes of 5°. This finding is partially in line with that of Soh et al.[15] in that the perception of esthetics by laypersons should not significantly correlate with that of dental professionals.
As for nose, lips, and ENLC alterations, orthodontists were unexpectedly less critical than lay people and dental students at distinguishing minor or moderate alterations of 1 and 3° rotations. Evidence suggests that midface is crucial in judgments of symmetry as most people focus on the area of the eyes, nose, and mouth.[28] The finding of the present study is in line with that of Meyer-Marcotty et al.[22,28] who reported that increased facial asymmetry near the midline of the face resulted in a more negative evaluation of the face in direct face-to-face interactions, suggesting that the midfacial area is crucial during facial perception.[29]
On the other hand, these findings can be speculated that the orthodontists place their main focus during treatment planning on the anteroposterior dimension so that their eyes and minds are always directed toward this specific dimension. Moreover, orthodontists take several factors into their consideration during diagnosis and treatment planning such as the limits to which the therapeutic choice should be extended, the effects of growth, and these certainly will affect their overall assessment and esthetic outcome. A plausible explanation why orthodontists were “less discriminating of minor alterations of the nose and mouth rotation than lay people and dental students could be that, orthodontists having encountered many patients in real-life situations may be more tolerant to asymmetries and imperfections (knowing how much time and effort it takes in clinical settings to correct the minute flaws) and hence rated them less critically than other two groups. Not because they were “unable to detect” but because they did detect it and thought it did not look that unattractive and considered it to be acceptable since VAS asks them to rate “attractiveness.” Moreover, lay people do not usually see themselves from a lateral perspective; the frontal perspectives of the face and the smile are more familiar to the patients and dental students than the lateral view during daily face-to-face communication. These results confirm that frontal perspectives of the face and the smile are more “familiar” to patients than the lateral view. Due to these factors, a difference does exist between orthodontists and patients’ in their evaluations of frontal asymmetries.[28,29]
Despite the limited power of the present investigation due to the limited literature to support or contradict these findings and the possibility that online questionnaires could affect the overall assessment. However, we observed perceptible inconsistency between how the patients perceived facial asymmetrical faces and how others perceived them and this study highlights the problem of the subjective assessment of the facial morphology. It also underlines the importance of developing an objective index to enumerate the magnitude of facial asymmetries.
According to these findings, it is of great importance for better orthodontic diagnosis and treatment planning to sit with the patients or parents, expose them to their frontal and lateral photographs, taking their perception into account, showing possible treatment results, and trying to make their perceptions as close to the orthodontists as possible. This sharing and close relationship of perceptions will enhance the treatment planning and result in more realistic motivations and expectations.[2]
CONCLUSIONS
The results of this study underline the importance of developing an objective index to enumerate the magnitude of facial asymmetries.
ACKNOWLEDGMENTS
The authors would like to express their deep gratitude and appreciation to Dr. Hussam AL Oufi, College of Dentistry, Taibah University, for participating in this study and for his time and support.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- A comparative assessment of the perception of Chinese facial profile esthetics. Am J Orthod Dentofacial Orthop. 2005;127:692-9.
- [CrossRef] [PubMed] [Google Scholar]
- Patients’ self-perception of dentofacial attractiveness before and after exposure to facial photographs. Angle Orthod. 2011;81:517-24.
- [CrossRef] [PubMed] [Google Scholar]
- Influence of lower facial height changes on frontal facial attractiveness and perception of treatment need by lay people. Angle Orthod. 2010;80:1159-64.
- [CrossRef] [PubMed] [Google Scholar]
- Soft-tissue cephalometric norms in yemeni men. Am J Orthod Dentofacial Orthop. 2007;132:e7-14.
- [CrossRef] [PubMed] [Google Scholar]
- Facial profile preferences among various layers of Turkish population. Angle Orthod. 2004;74:640-7.
- [PubMed] [Google Scholar]
- The influence of different facial components on facial aesthetics. Eur J Orthod. 2002;24:1-7.
- [CrossRef] [PubMed] [Google Scholar]
- The influence of dental to facial midline discrepancies on dental attractiveness ratings. Eur J Orthod. 1999;21:517-22.
- [CrossRef] [PubMed] [Google Scholar]
- Anthropometrics and art in the aesthetics of women’s faces. Clin Plast Surg. 1987;14:599-616.
- [PubMed] [Google Scholar]
- Growth changes in the soft tissue facial profile. Angle Orthod. 1990;60:177-90.
- [PubMed] [Google Scholar]
- Rating of facial attractiveness. Community Dent Oral Epidemiol. 1992;20:214-20.
- [CrossRef] [PubMed] [Google Scholar]
- The influence of dentofacial appearance on the social attractiveness of young adults. Am J Orthod. 1985;87:21-6.
- [CrossRef] [Google Scholar]
- The influence of lower face vertical proportion on facial attractiveness. Eur J Orthod. 2005;27:349-54.
- [CrossRef] [PubMed] [Google Scholar]
- Professional assessment of facial profile attractiveness. Am J Orthod Dentofacial Orthop. 2005;128:201-5.
- [CrossRef] [PubMed] [Google Scholar]
- Ethnic differences in the soft tissue profile of Korean and European-American adults with normal occlusions and well-balanced faces. Angle Orthod. 2002;72:72-80.
- [PubMed] [Google Scholar]
- Soft-tissue cephalometric norms in Chinese adults with esthetic facial profiles. J Oral Maxillofac Surg. 1992;50:1184-9.
- [CrossRef] [Google Scholar]
- Perceptions of dentofacial morphology by laypersons, general dentists, and orthodontists. J Am Dent Assoc. 1979;98:209-12.
- [CrossRef] [PubMed] [Google Scholar]
- Evaluation of horizontal and vertical differences in facial profiles by orthodontists and lay people. Angle Orthod. 1993;63:175-82.
- [PubMed] [Google Scholar]
- The perception of optimal profile in African Americans versus white americans as assessed by orthodontists and the lay public. Am J Orthod Dentofacial Orthop. 2000;118:514-25.
- [CrossRef] [PubMed] [Google Scholar]
- Three-dimensional perception of facial asymmetry. Eur J Orthod. 2011;33:647-53.
- [CrossRef] [PubMed] [Google Scholar]
- Soft tissue cephalometric norms in Japanese adults. Am J Orthod Dentofacial Orthop. 2000;118:84-9.
- [CrossRef] [PubMed] [Google Scholar]
- Soft tissue profile in anatolian Turkish adults: Part II. Comparison of different soft tissue analyses in the evaluation of beauty. Am J Orthod Dentofacial Orthop. 2002;121:65-72.
- [CrossRef] [PubMed] [Google Scholar]
- Clinical longitudinal standards for height and height velocity for North American children. J Pediatr. 1985;107:317-29.
- [CrossRef] [Google Scholar]
- Longitudinal study of dental arch widths at four stages of dentition. Angle Orthod. 1972;42:387-94.
- [PubMed] [Google Scholar]
- Dimensional changes of the dental arches: Longitudinal study from birth to 25 years. Am J Orthod. 1964;50:824-42.
- [CrossRef] [Google Scholar]
- Impact of facial asymmetry in visual perception: A 3-dimensional data analysis. Am J Orthod Dentofacial Orthop. 2010;137:e1-8.
- [CrossRef] [PubMed] [Google Scholar]
- An appraisal of three methods of rating facial deformity in patients with repaired complete unilateral cleft lip and palate. Cleft Palate Craniofac J. 2003;40:530-7.
- [CrossRef] [Google Scholar]




