

Translate this page into:
Safe sites in the mandibular buccal shelf for orthodontic mini-screws: Tomographic study in different facial types
 , Rafael Gorghetto Domingos1,, Almir Lima Junior1, Jose Rino Neto1, João Batista de Paiva1
, Rafael Gorghetto Domingos1,, Almir Lima Junior1, Jose Rino Neto1, João Batista de Paiva1

*Corresponding author: Rafael Gorghetto Domingos, Department of Orthodontics and Pediatric Dentistry, School of Dentistry, University of São Paulo, São Paulo, Brazil. rafaelgolghetto@yahoo.com.br
-
Received: ,
Accepted: ,
How to cite this article: Ribeiro AC, Domingos RG, Lima A, Rino J, de Paiva JB. Safe sites in the mandibular buccal shelf for orthodontic mini-screws: Tomographic study in different facial types. APOS Trends Orthod. doi: 10.25259/APOS_79_2024
Abstract
Objectives:
The objective of this study was to verify safe sites on the mandibular buccal shelf (MBS) for extra-alveolar mini-screw insertion according to facial type.
Material and Methods:
In this retrospective study, 84 cone-beam computed tomography scans were equally divided into three groups according to the patient’s facial type: Group 1, hyperdivergent; Group 2, neutral; and Group 3, hypodivergent. The total buccal alveolar bone thickness was measured in five zones between the mesial root of the first molar and the distal root of the second molar, 3, 6, and 9 mm apical to the cementoenamel junction (CEJ).
Results:
MBS areas with adequate thickness for temporary anchorage device (TAD) insertion were as follows: Group 1, second molar distal root 9 mm from the CEJ; Group 2, second molar distal root 6 and 9 mm from the CEJ; and Group 3, second molar mesial root 9 mm from the CEJ and second molar distal root 6 and 9 mm from the CEJ.
Conclusion:
The safe zones on the MBS for TAD insertion were located on the distal root of the second molar, 9 mm from the CEJ, for all facial types. For neutral and hypodivergent patients, the site located on the second molar distal root, 6 mm from CEJ, was included; for hypodivergent patients, the site located on the second molar mesial root, 9 mm from the CEJ, was included.
Keywords
Corrective orthodontics
Orthodontic anchorage procedures
Cone-beam computed tomography

INTRODUCTION
Orthodontists consistently pursue accessories or techniques that provide reliable anchorage, and alternatives that reduce patient compliance. Temporary anchorage devices (TADs) were designed to optimize orthodontic treatment results by ensuring the desired tooth stabilization at several treatment stages.[1] The first TADs were inserted in the intra-alveolar area, which may interfere with certain treatment plans, particularly when mass movement in the sagittal direction is intended.[2] To resolve this problem in orthodontic mechanics, the installation of TADs in an extra-alveolar area was proposed. The placement of these devices in this region allows for the use of larger screws that can be inserted parallel to the axial inclination of the molars without interfering with the roots of the teeth that will be moved.[3]
For complete lower arch movement assisted by TADs, insertion in the mandibular buccal shelf (MBS) region is indicated. This area is located vestibularly to the lower molars, in front of the mandibular oblique line, and presents a dense cortical bone and suitable thickness for mini-screw installation. It has shown a high success rate and stability of these devices during orthodontic mechanics. The site between the first and second lower molars has been indicated as a safe site in the MBS for TAD insertion;[4] however, clinically, this location may present insufficient bone thickness for successful insertion or satisfactory primary stability in many cases. In a preliminary tomographic evaluation, a minimum total buccal bone thickness of 5 mm (from the root surface to the most vestibular point of the adjacent cortical bone) of the MBS was necessary for safe extra-alveolar mini-screw insertion.[5]
Based on the predominance of vertical or horizontal bone growth patterns, different facial types have been classified in the literature as hypodivergent, neutral, and hyperdivergent.[6,7] It creates distinct morphological characteristics, such as different mean bone thickness in the MBS area,[8] which can interfere with the procedure of TAD insertion. Studies performed using cone-beam computed tomography (CBCT) aimed at assessing the alveolar cortical plate have observed that hypodivergent patients have a higher dentoalveolar cortical thickness than hyperdivergent patients.[8-12]
As MBS is indicated for the insertion of extra-alveolar TADs, and each facial type presents specific morphologic bone aspects, this study was performed to verify the safe sites in this area for mini-screw insertion according to the patient’s facial type and the differences between each growth pattern concerning bone thickness in this region.
MATERIAL AND METHODS
For this retrospective study, 84 full-head CBCT scans were randomly selected from the Orthodontics and Odontopediatrics Department of FOUSP database. The included patients were aged between 18 and 40 years and had all mandibular permanent teeth erupted, no previous orthodontic treatment, no history of surgery or previous trauma in the mandibular area, satisfactory dental and periodontal conditions, and no clinical signs or symptoms of temporomandibular joint disease. This project was approved by the Research Ethics Committee of the School of Dentistry of FOUSP under protocol number 2.253.955.
The images were collected using a CBCT (I-CAT® Cone Beam 3-D Dental Imaging System, Imaging Sciences International, Hartefield, USA) with a 0.4 mm voxel resolution and evaluated in a specific software (Dolphin Imaging and Management Solutions, Chatsworth, CA, USA). The natural head position on these tomographic images was adjusted to coincide with the true horizontal plane[13] to reduce errors in head position during image acquisition. Therefore, each time these data were accessed, the head position remained the same. Subsequently, a two-dimensional lateral reproduction of the head was obtained from this scan for cephalometric tracing.
The Jarabak Index (the ratio of S-Go and N-Me)[6,7] was adopted to determine the facial type of each patient after cephalometric analysis and was then organized into three groups: Group 1, hyperdivergent facial type–prevalence of vertical vector of facial growth; Group 2, neutral facial type– neutral facial type: Balance of vertical and horizontal facial growth vectors; and Group 3, hypodivergent facial type– prevalence of horizontal vector of facial growth.
To evaluate the bone thickness on the MBS, the appraisal was performed bilaterally in axial slices at distances of 3 mm, 6 mm, and 9 mm apically from a reference line passing through the mesial and distal cementoenamel junction (CEJ) of the evaluated tooth [Figure 1a] at the following sites: (1) first molar mesial root, (2) first molar distal root, (3) between the first and second molars, (4) second molar mesial root, and (5) second molar distal root [Figure 1b]. The thickness was horizontally measured[5,9-12] at each of these sites, from the midpoint of the root to the most vestibular point of the adjacent alveolar cortical bone. To measure the distance on the site located between the first and second molars, a line was drawn from the distal root of the first molar to the mesial root of the second molar, and the thickness from the midpoint of this line to the most vestibular point of the adjacent cortical bone was measured. All measurements were done by the same radiologist, experienced in CBCT assessments.
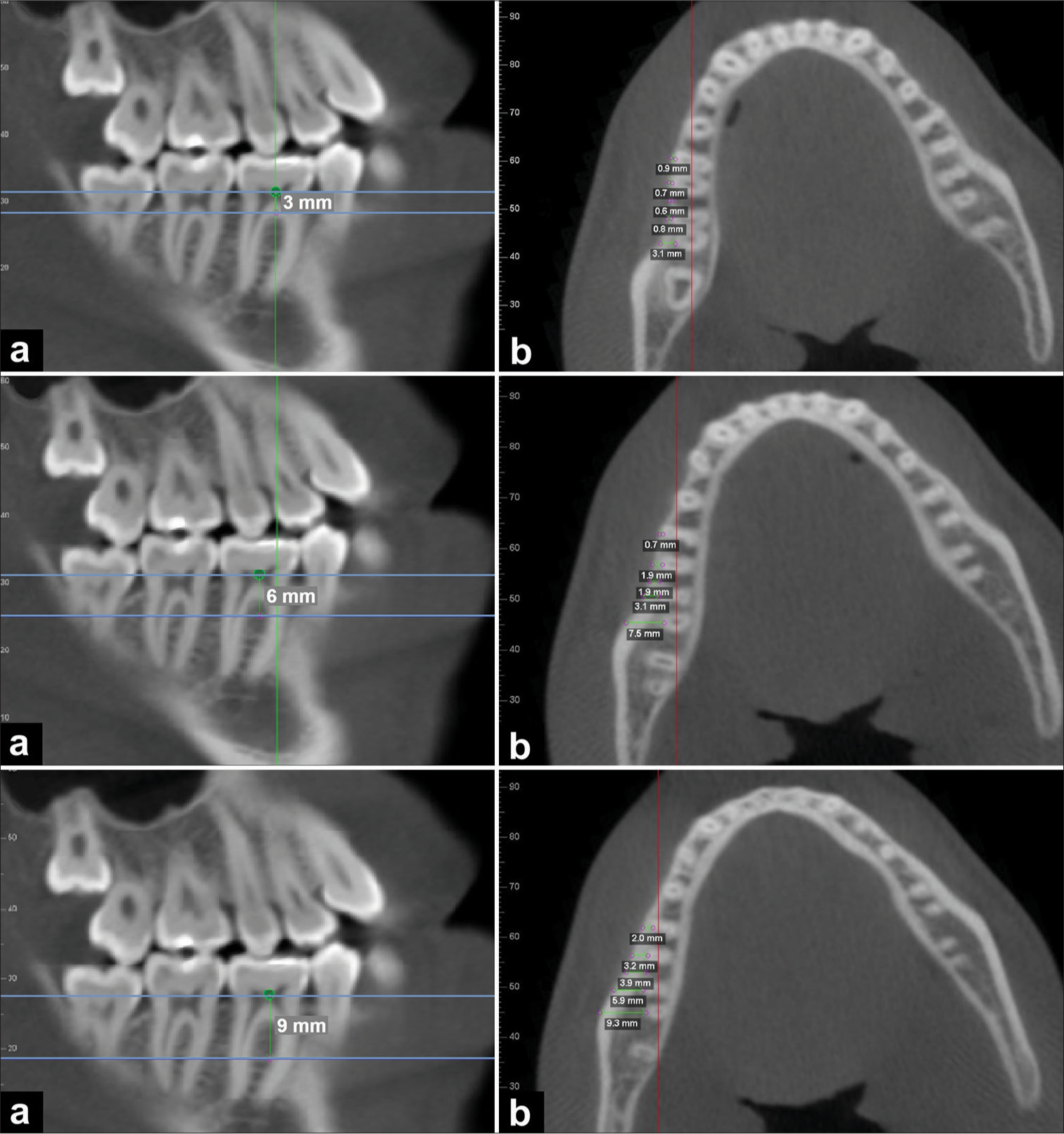
- (a) Sagittal tomographic image with markings at 3 mm, 6 mm, and 9 mm apical from the cementoenamel junction (b) and axial slice at the respective markings.
Statistical analysis
The analysis was performed using IBM SPSS for Windows (version 20.0) with a significance level of 5%. A preliminary assay was performed on 30 tomographic images (ten of each facial type) and indicated that a sample of 28 scans in each group was essential to achieve a power of 80% and alpha = 0.05. The ages of the patients were described using means and standard deviations and compared between facial types using analysis of variance (ANOVA), followed by Bonferroni’s multiple comparisons if the results were significant. The patients’ sex was described using absolute and relative frequencies, and the association between facial types was verified using the Chi-square test. The bone thickness measurements were described separately for each group using means and standard deviations with 95% normal intervals for all parameters. Differences between the bone measurement sites for each facial type were compared using repeated-measures ANOVA, followed by Bonferroni’s multiple comparison test. The interclass correlation coefficients were estimated with 95% confidence intervals to evaluate method error. This was determined for part of the sample, and the differences between measurements were calculated using Dahlberg’s formula.[14,15]
RESULTS
The primary results showed no statistically significant mean difference in the ages of the patients between the three groups (P = 0.947) and no correlation between sex and facial type (P = 0.651).
[Table 1] describes the mean values and respective standard deviations of the patients in Group 1 (hyperdivergent). All measurements showed statistically significant differences between the evaluated sites (P <0.001). The measurements at the site located at the second molar distal root, 9 mm from the CEJ, were > 5 mm.
| Variable | Distance from CEJ | P | ||
|---|---|---|---|---|
| 3 mm | 6 mm | 9 mm | ||
| First molar mesial root, right side | 0.38±0.39 | 0.38±0.48 | 1.16±0.80 | <0.001 |
| First molar distal root, right side | 0.46±0.46 | 1.03±0.97 | 2.09±1.46 | <0.001 |
| Between first and second molars, right side | 0.56±0.83 | 1.71±1.27 | 3.30±1.65 | <0.001 |
| Second molar mesial root, right side | 1.09±1.18 | 2.85±1.99 | 4.48±1.99 | <0.001 |
| Second molar distal root, right side | 2.6±1.91 | 4.64±2.25 | 6.14±1.61 | <0.001 |
| First molar mesial root, left side | 0.29±0.31 | 0.46±0.58 | 1.01±0.97 | <0.001 |
| First molar distal root, left side | 0.41±0.53 | 1.04±1.24 | 1.98±1.65 | <0.001 |
| Between first and second molars, left side | 0.71±0.90 | 1.48±1.59 | 3.06±1.84 | <0.001 |
| Second molar mesial root, left side | 1.24±1.23 | 2.52±1.88 | 4.45±2.00 | <0.001 |
| Second molar distal root, left side | 2.74±2.52 | 4.79±2.15 | 6.21±1.88 | <0.001 |
ANOVA with repeated measurements. ANOVA: Analysis of variance, TAD: Temporary anchorage device, MBS: Mandibular buccal shelf, CEJ: Cementoenamel junction. Gray cells indicate the site with sufficient bone thickness for TAD installation in the MBS.
[Table 2] describes the mean values and standard deviations for Group 2 (neutral). All measures differed significantly between sites (P < 0.001). The measurements in the second molar distal root, 6 and 9 mm from the CEJ, showed values > 5 mm. [Table 3] describes the mean values and standard deviations of the participants in Group 3 (hypodivergent). All measures differed significantly between sites (P < 0.001). Measurements of the second molar mesial root, 9 mm from the CEJ, and the second molar distal root, 6 and 9 mm from the CEJ, showed values > 5 mm.
| Variable | Distance from CEJ | P | ||
|---|---|---|---|---|
| 3 mm | 6 mm | 9 mm | ||
| First molar mesial root, right side | 0.28±0.33 | 0.53±0.57 | 1.34±1.01 | <0.001 |
| First molar distal root, right side | 0.55±0.68 | 1.44±0.98 | 2.71±1.29 | <0.001 |
| Between first and second molars, right side | 0.85±1.06 | 2.10±1.16 | 3.61±1.30 | <0.001 |
| Second molar mesial root, right side | 1.13±1.15 | 2.99±1.45 | 4.83±1.49 | <0.001 |
| Second molar distal root, right side | 3.23±2.15 | 5.43±1.85 | 6.60±1.43 | <0.001 |
| First molar mesial root, left side | 0.23±0.38 | 0.38±0.57 | 0.91±0.92 | <0.001 |
| First molar distal root, left side | 0.43±0.59 | 1.06±1.04 | 2.36±1.50 | <0.001 |
| Between first and second molars, left side | 0.74±1.00 | 1.85±1.36 | 3.44±1.47 | <0.001 |
| Second molar mesial root, left side | 1.19±1.33 | 2.84±1.95 | 4.91±1.86 | <0.001 |
| Second molar distal root, left side | 2.80±2.18 | 5.16±1.94 | 6.64±1.71 | <0.001 |
ANOVA with repeated measurements. ANOVA: Analysis of variance, TAD: Temporary anchorage device, MBS: Mandibular buccal shelf, CEJ: Cementoenamel junction. Gray cells indicate the site with sufficient bone thickness for TAD installation in the MBS.
| Variable | Distance from CEJ | P | ||
|---|---|---|---|---|
| 3 mm | 6 mm | 9 mm | ||
| First molar mesial root, right side | 0.49 ± 0.60 | 0.91 ± 0.81 | 1.81 ± 1.13 | <0.001 |
| First molar distal root, right side | 0.98 ± 0.83 | 1.79 ± 1.44 | 3.26 ± 1.72 | <0.001 |
| Between first and second molars, right side | 0.79 ± 0.74 | 2.17 ± 1.00 | 3.95 ± 1.34 | <0.001 |
| Second molar mesial root, right side | 1.31 ± 1.57 | 3.41 ± 1.82 | 5.26 ± 1.58 | <0.001 |
| Second molar distal root, right side | 3.26 ± 2.30 | 5.55 ± 2.12 | 6.92 ± 1.73 | <0.001 |
| First molar mesial root, left side | 0.33 ± 0.39 | 0.64 ± 0.68 | 1.5 ± 1.09 | <0.001 |
| First molar distal root, left side | 0.46 ± 0.58 | 1.26 ± 1.10 | 2.78 ± 1.66 | <0.001 |
| Between first and second molars, left side | 0.50 ± 0.57 | 1.69 ± 1.16 | 3.51 ± 1.27 | <0.001 |
| Second molar mesial root, left side | 0.99 ± 1.02 | 2.78 ± 1.45 | 5.16 ± 1.65 | <0.001 |
| Second molar distal root, left side | 2.44 ± 2.13 | 5.24 ± 1.70 | 6.72 ± 1.48 | <0.001 |
ANOVA with repeated measurements. ANOVA: Analysis of variance, TAD: Temporary anchorage device, MBS: Mandibular buccal shelf, CEJ: Cementoenamel junction. Gray cells indicate the site with sufficient bone thickness for TAD installation in the MBS.
DISCUSSION
Anchorage is invariably a critical factor in obtaining satisfactory orthodontic treatment results. Over the years, new strategies have been proposed to improve effectiveness. Skeletal anchorage has emerged to achieve this goal. TADs have been widely incorporated into orthodontic treatment to expand the limits of tooth movement and reduce the need for patient compliance.[1-4] The selection of the insertion site is primarily based on planned biomechanics and anatomy; however, the facial type may influence the anatomical characteristics of the installation area. Bone thickness is an important anatomical factor during the insertion of an orthodontic screw, and several studies have used CBCT to assess bone quality and quantity to determine the most favorable position.[4,5,8-12,16,17]
The MBS has become a frequent site of insertion of TADs in the lower arch. This region is a secure location for the installation of extra-alveolar TADs due to its cortical bone density and total bone thickness, offering clinical advantages over interradicular insertion.[3,4,8] In MBS, the screw is inserted parallel to the long axis of the molar to avoid contact with the roots during installation and dental movement, with success rates of over 90% and excellent results.[3] Therefore, it is prudent to evaluate the total buccal bone thickness (including cancellous and cortical bone)[5,9-12,17] so that the TAD can be completely inserted into the bone to avoid touching the dental roots.
Safe TAD installation in the MBS requires a minimum buccal bone thickness of 5 mm, as stated in a previous study[5] that assessed this region vertically on the first and second molars at 6 and 11 mm apical to the CEJ; however, the results were not correlated with the patient’s facial type. Our study evaluated patients of the three facial types in the region of the first and second lower molars at distances of 3, 6, and 9 mm apical to the CEJ. The reference point is usually measured either from the alveolar bone crest[4,10,11] or the CEJ.[5,9,12,16,17] Our assessment used the CEJ as a reference to avoid possible interferences concerning eventual bone losses affecting alveolar crest heights, which could negatively interfere with the results.
Differences were found in vestibular alveolar bone thickness among the facial types. In the hyperdivergent group [Table 1], a minimum buccal bone thickness of 5 mm was observed bilaterally at the distal root of the second molar, 9 mm from the CEJ [Figure 2a]. In the neutral group [Table 2], the measurements in the second molar distal root bilaterally presented sufficient buccal bone thickness at 6 mm, as similarly reported in a previous study,[5] and 9 mm apical to the CEJ [Figure 2b]. In the hypodivergent group [Table 3], in addition to the second molar distal root, at 6 and 9 mm from the CEJ, the site located on the mesial root of the second molar, 9 mm apical to the CEJ, also presented a sufficient buccal bone thickness for safe TAD installation on the MBS [Figure 2c]. These results are comparable to those of another study[4] that evaluated CBCT scans of class III patients, in which the authors did not mention the facial type; however, patients with class III malocclusion tend to present a hypodivergent growth pattern with a large mandible,[18] which may justify the similar result found in Group 3 of our study. Only the site in the second molar distal root 9 mm from the CEJ was common to the three groups due to its safety for TAD installation, similar to the results of other studies[9-12,16,17] that assessed the MBS.
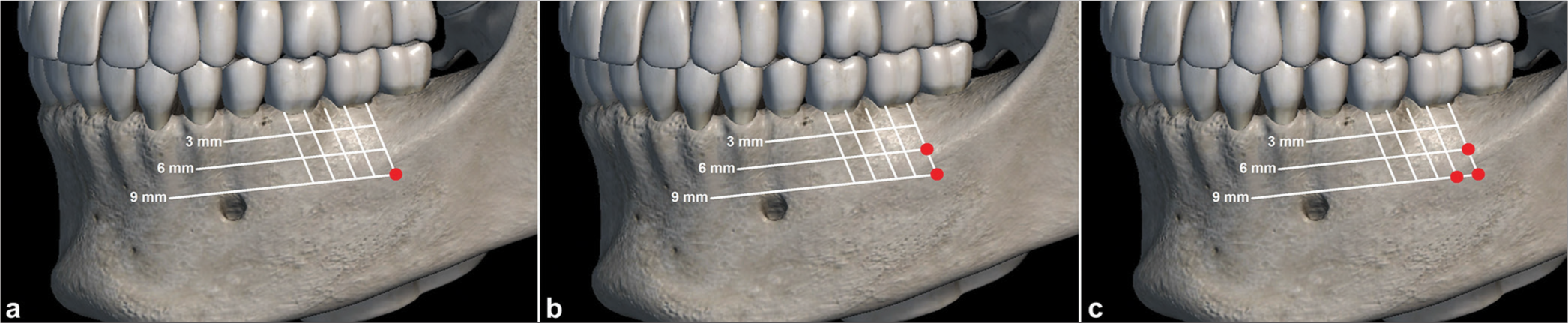
- Safe sites for mandibular buccal shelf mini-screw insertion. (a) Hyperdivergent patients; (b) neutral patients; (c) and hypodivergent patients.
In Group 1 (hyperdivergent), the sites situated on the second molar mesial root 9 mm from the CEJ and on the second molar distal root 6 mm from the CEJ presented almost sufficient bone thickness for safe TAD installation, with an increased standard deviation. The same was observed in Group 2 on the mesial root of the second molar 9 mm from the CEJ. This characteristic indicates that, in some patients in these groups, these three sites may be considered safe for TAD installation in the MBS; however, individual tomographic evaluation[16] is required for confirmation.
Bone assessment in the MBS region showed a progressive increase in thickness toward the second molar area and apical direction in the three groups [Tables 1-3], regardless of the facial type, and these differences were statistically significant at the sites observed. Similarly, this characteristic was described previously in studies using CBCT scans, and a pattern of increased bone thickness in the MBS during the evaluation of the lower and posterior regions was also observed.[5,16] Hypodivergent patients present with greater cortical and spongy bone thickness than hyperdivergent patients, regardless of their malocclusion classification.[8-12] Our study also observed a tendency for higher values in hypodivergent patients, considering that Group 3 showed a greater number of safe sites for TAD insertion in the MBS. It is important to remember that we assessed the total buccal alveolar bone thickness instead of dividing it into cortical and spongy bone [8-12,17] pretending to provide sites with adequate bone thickness for TAD installation, as this area usually presents a suitable cortical bone thickness for primary TAD stability.
A critical question is about the sites located 9 mm from the CEJ because, at this distance, there is a chance of the movable mucosa being penetrated or the mucogingival junction being touched.[3,19] Although this may cause concerns, the success rates of extra-alveolar TADs inserted into the attached gingiva or movable mucosa are similar.[3,19] Orthodontists should consider using longer screws when the insertion site is in the movable mucosa; this will be useful throughout the treatment once the active head remains out of the mucosa. Since this area may be difficult to reach, contra-angle motorized instruments should be helpful to ensure the correct TAD angulation.
As the assessment of alveolar bone thickness is delicate, CBCT scans should be performed with a reduced field of view (FOV); therefore, the voxel size decreases, and the image quality improves. This study was conducted with the existing tomographic images performed in a larger FOV and following the “As Low As Reasonably Achievable” principle, which produced a voxel size of 0.4 mm. This voxel size was appropriate for these appraisals, as observed in previous studies.[20]
An appropriate placement site is essential for stability. This study evaluated the buccal bone thickness in the MBS to determine safe areas for its insertion; however, the orthodontist should be attentive to other factors that may influence the stability of these screws.
CONCLUSION
After evaluating the results obtained in this study, the sites that can be considered secure for the insertion of MBS mini-screws are the second molar distal root 9 mm apical from the CEJ in hyperdivergent facial type patients, the second molar distal root 6 mm and 9 mm apical from the CEJ in neutral facial type patients, and the second molar mesial root 9 mm apical from the CEJ and the second molar distal root 6 mm and 9 mm apically from the CEJ in hypodivergent facial type patients.
Acknowledgments
The authors would like to acknowledge CAPES for providing a scholarship for the PhD degree of Annelise Nazareth Cunha Ribeiro, MSc.
Ethical approval
The research/study approved by the Institutional Review Board at Ethics Committee of FOUSP, number 2.253.955, dated September 01, 2017.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- Effectiveness of orthodontic miniscrew implants in anchorage reinforcement during en-masse retraction: A systematic review and meta-analysis. Am J Orthod Dentofacial Orthop. 2017;151:440-55.
- [CrossRef] [Google Scholar]
- Primary failure rate for 1680 extra-alveolar mandibular buccal shelf mini-screws placed in movable mucosa or attached gingiva. Angle Orthod. 2015;85:905-10.
- [CrossRef] [Google Scholar]
- 3D cortical bone anatomy of the mandibular buccal shelf: A CBCT study to define sites for extra-alveolar bone screws to treat Class III malocclusion. Int J Orthod Implantol. 2016;41:74-82.
- [Google Scholar]
- Bone and cortical bone thickness of mandibular buccal shelf for mini-screw insertion in adults. Angle Orthod. 2017;87:745-51.
- [CrossRef] [Google Scholar]
- Technique and treatment with light wire and edge wise appliances (2nd ed). St. Louis: Mosby; 1972.
- [Google Scholar]
- Cortical bone thickness of the alveolar process measured with cone-beam computed tomography in patients with different facial types. Am J Orthod Dentofacial Orthop. 2013;143:190-6.
- [CrossRef] [Google Scholar]
- Mandibular buccal shelf and infrazygomatic crest thicknesses in patients with different vertical facial heights. Am J Orthod Dentofacial Orthop. 2020;158:349-56.
- [CrossRef] [Google Scholar]
- Assessment of the mandibular buccal shelf for orthodontic anchorage: Influence of side, gender and skeletal patterns. Orthod Craniofac Res. 2021;24:83-91.
- [CrossRef] [Google Scholar]
- Buccal bone thickness of posterior mandible for microscrews implantation in molar distalization. Ann Anat. 2022;244:151993.
- [CrossRef] [Google Scholar]
- Bone thickness and height of the buccal shelf area and the mandibular canal position for miniscrew insertion in patients with different vertical facial patterns, age, and sex. Angle Orthod. 2023;93:185-94.
- [CrossRef] [Google Scholar]
- Head orientation in CBCT-generated cephalograms. Angle Orthod. 2009;79:971-7.
- [CrossRef] [Google Scholar]
- Anatomic assessment of the mandibular buccal shelf for miniscrew insertion in white patients. Am J Orthod Dentofacial Orthop. 2018;153:505-11.
- [CrossRef] [Google Scholar]
- Evaluation of mandibular buccal shelf characteristics in the Colombian population: A cone-beam computed tomography study. Korean J Orthod. 2021;51:23-31.
- [CrossRef] [Google Scholar]
- Skeletal components of Class III malocclusions and compensation mechanisms. J Oral Rehabil. 2008;35:629-37.
- [CrossRef] [Google Scholar]
- Comparison of the failure rate for infrazygomatic bone screws placed in movable mucosa or attached gingiva. Int J Orthod Implantol. 2017;47:96-106.
- [Google Scholar]
- Accuracy and reliability of tooth and root lengths measured on cone-beam computed tomographs. Am J Orthod Dentofacial Orthop. 2010;137:S100-8.
- [CrossRef] [Google Scholar]




