

Translate this page into:
The hybrid approach: A solution to overcome unpredictable movements in clear aligner therapy


*Corresponding author: Luca Lombardo, Department of Orthodontics, University of Ferrara, Via Borsari, Ferrara, Emilia Romagna, Italy. dott.lulombardo@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Lombardo L, Albertini P, Siciliani G. The hybrid approach: A solution to overcome unpredictable movements in clear aligner therapy. APOS Trends Orthod 2020;10(2):72-7.
Abstract
The clear aligner system has been radically improved in many aspects: New materials, protocols, attachments, and auxiliaries were developed to improve biomechanics. Many movements remain unpredictable, outlining the limits of clear aligners treatment, but a hybrid approach, which combines clear aligners with fixed appliance, is an efficient treatment alternative. This approach significantly reduces overall treatment time and unpredictable movements. The aim of this article is to show the application of the hybrid approach for different types of movements.
Keywords
Clear aligners
Fixed appliances
Hybrid approach

INTRODUCTION
Clear aligners have become increasingly popular in recent years due to patients’ esthetic and comfort needs.
Young patients between the ages of 8 and 16 have a strong self-perception regarding smile esthetics and, therefore, not only adults require orthodontic treatment with the use of esthetic appliances.[1,2]
In the last years, the clear aligner system has been radically improved in many aspects: New materials, protocols, attachments, and auxiliaries were developed to improve biomechanics.
A careful patient selection is necessary since the clear aligners therapy is a valid alternative only for non-extraction cases, which fit in determined diagnostic parameters.[3]
For more severe cases, fixed appliances are needed since clear aligners therapy is less efficient.[4-6]
Recently, a meta-analysis has concluded that orthodontic treatment with aligners is associated with worse treatment outcome compared to fixed appliances in adult patients.[7]
The outcomes are closely related to the predictability of the planned dental movements.
The software to create aligners setup simulates any type of dental movement, even those achievable only with orthognathic surgery; therefore, planning the case requires attention.
The international scientific literature is very clear and agrees in describing which movements are achievable and which are unpredictable with clear aligners.[4-7]
The aligners accuracy is sufficient to resolve anterior crowding and molar distalization (2.5 mm), but inadequate for bodily expansion of the maxillary posterior teeth, canine and premolar rotational movements, extrusion of maxillary incisors, and in overbite control.[5]
Many movements remain unpredictable, outlining the limits of clear aligners treatment, which can be sometimes overcome only using fixed appliance, as extraction cases or severe malocclusions.
In alternative, the innovative concept of hybrid approach implies the use of partial fixed appliances combined with clear aligners.
The aim of this article is to show the application of the hybrid approach for different types of movements, which would be unpredictable with the application of clear aligners only.
ROTATIONS CORRECTION
The ability to rotate teeth strongly depends on the tooth anatomy and how the pressure points grip the tooth.
In literature, the accuracy of clear aligners is described as inadequate to derotate canines and premolars.[5]
Rounded teeth are the most difficult teeth to control with aligners (1/3 of that predicted), unlike the upper incisors, which are easier to rotate due to the greater mesiodistal width and to the flatter shape.[4,6]
The hybrid approach, especially on the most difficult teeth to derotate, consists of a fixed partial lingual appliance to obtain greater movement predictability, a reduction in the number of attachments in esthetic areas and a limited number of clear aligners.
The first step of this procedure is to place lingual tubes on the rotated teeth and on the adjacent teeth; then, an accurate impression is necessary to simulate the presence of a lingual archwire in the setup and to keep the physical space under the clear aligners (F22; Sweden and Martina, Due Carrare, PD, Italy) [Figure 1].
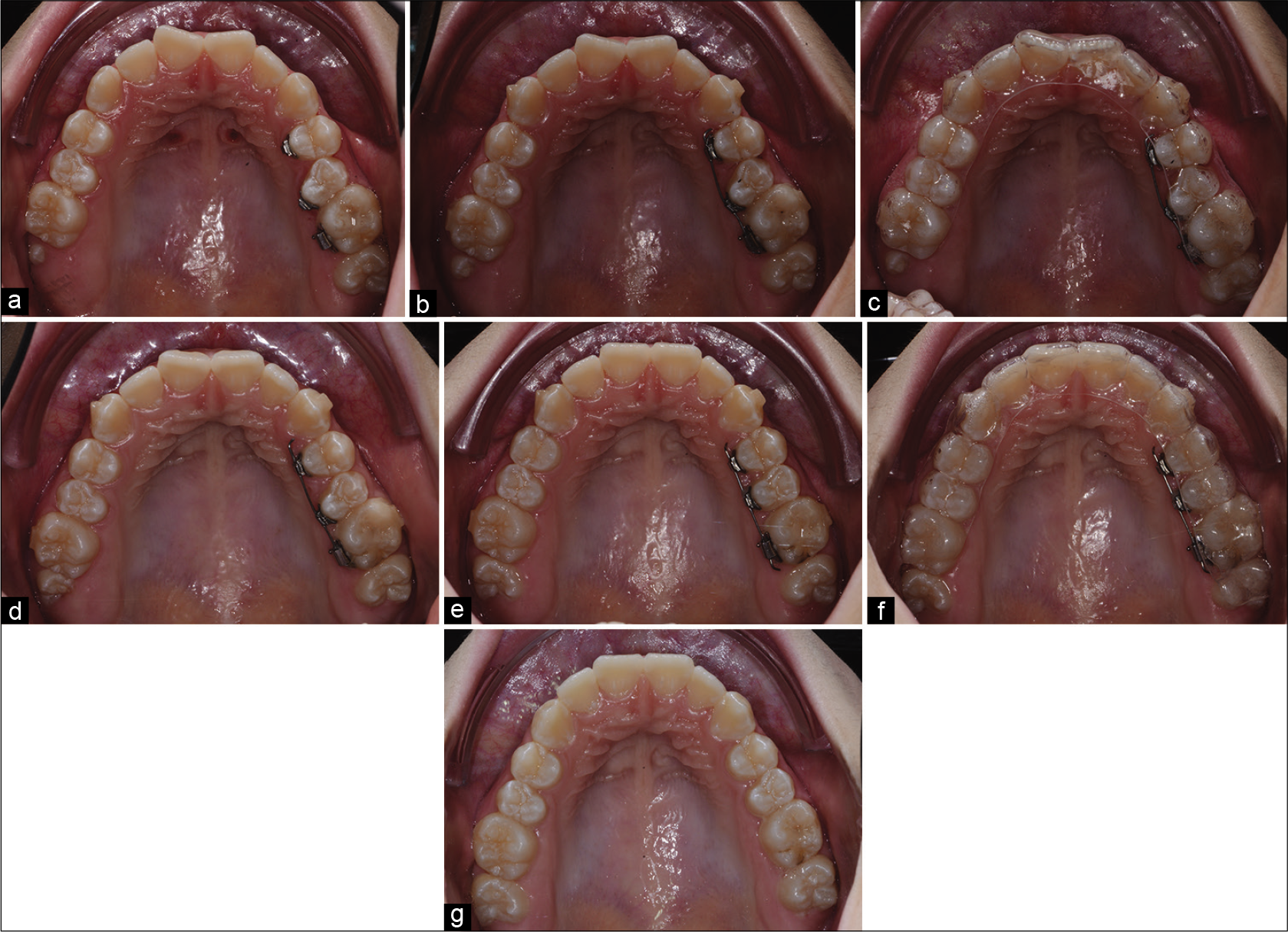
- Rotations correction: (a) Lingual tubes placed on the rotated teeth and on the adjacent teeth followed by impressions; (b and c) beginning of the hybrid treatment with clear aligners combined with a 0.013 CuNiTi archwire insertion in lingual tubes; (d) 2 months later, the clear aligners continue to follow the CuNiTi archwire expression; (e and f) 4 months from the beginning, the rotation is corrected; (g) final result.
F22 aligners completely envelope the partial fixed lingual appliances and follow the CuNiTi archwires expression [Figure 1].
TRANSVERSAL CORRECTION
In literature, the bodily transverse expansion with clear aligners is not predictable and the setup tends to overestimate bodily expansion movements.[5,8]
The transverse dimensions increase is often due to tipping movement of the teeth, even if bodily expansion movements were planned.[8]
In fact, when a transverse diameter expansion with dental tipping is necessary, due to an excessively negative inclination of the posterior teeth, only clear aligners are ideal; however, as in most cases, when a bodily expansion is needed, only clear aligners are no longer sufficient.
For these reasons, the hybrid approach consists of a phase, before F22 clear aligners treatment, with rapid palatal expander with or without miniscrews, depending on the patient age.
In adult patients, the expansion supported by miniscrews improves the bodily movements [Figure 2].

- Transversal correction: (a and b) Initial photographs show the transverse diameter reduction in an adult patient; (c and d) beginning of the hybrid treatment with RPE supported by miniscrews; (e and f) end of expansion phase and impressions performed for a clear aligners phase; (g and h) clear aligners phase; (i and j) clear aligners refinement phase; (k and l) end of hybrid treatment and RPE remotion.
SAGITTAL CORRECTION – CLASS II
In literature, a bodily distalization of 2.2 mm is possible to achieve, planning 0.25 mm of movement per step and asking the patients to wear aligners 14 days each.[9]
This amount of distalization is sufficient to correct at most a half cusp Class II relationship.
However, to minimize loss of anchorage, hybrid approach consists of intermaxillary elastics applied on sectional archwires or Carriere Motion, and in cases, where a greater sagittal correction is required, it consists of TADs appliances, such as pendulum on miniscrews [Figures 3 and 4].

- Moderate sagittal correction: (a) Initial photographs show a molar Class II relationship on the right side in an adult patient; (b) beginning of the hybrid treatment with Carriere Motion and clear aligners; (c and d) once the desired sagittal correction is obtained, the F22 clear aligners are used for the case finishing; (e) final result.

- Severe sagittal and transversal correction: (a-c) Initial photographs show a molar Class II relationship on the left side and transverse diameter reduction in an adult patient; (d-f) beginning of the hybrid treatment with RPE/pendulum supported by miniscrew and F22 clear aligners; (g-i) once the desired sagittal and transversal correction are obtained, (j-l) the F22 clear aligners are used for the easier case; (m-o) case refinement; (p-r) final result.
Upper wisdom teeth might be extracted to take advantage of the regional acceleratory phenomenon.
Once the desired sagittal correction is obtained, the F22 clear aligners are used for the case finishing [Figures 3 and 4].
SAGITTAL CORRECTION – CLASS III
In literature, there is no evidence about lower arch distalization movement and upper arch mesialization movement.
The sagittal correction of mild Class III can be obtained with the intermaxillary elastic combined with clear aligners, but sometimes this solution is not resolutive.
For these reasons, the hybrid approach consists of a phase before clear aligners with hybrid or traditional rapid palatal expander combined with facemask [Figure 5].

- Sagittal correction: (a-c) Initial photographs show a Class III malocclusion in a young patient; (d-f) beginning of the early treatment with traditional RPE combined with facemask; (g-i) early treatment is finished; since the sagittal correction was not sufficient, (j-l) an hybrid treatment with RPE supported by miniscrews combined with facemask and F22 clear aligners was performed; (m-o) once the desired sagittal correction is obtained, (p-r) the F22 clear aligners are used for the case refinement; (s-u) final result.
Once the desired sagittal correction is obtained, the clear aligners are used for the case finishing [Figure 5].
VERTICAL CORRECTION
In literature, pure intrusion and extrusion movements are unpredictable with clear aligners and proclination or retroclination is clinically planned to mask vertical problems.[10,11]
However, this type of correction is allowed when the amount of vertical correction is very limited.
The upper incisors intrusion is described as the most unpredictable movement with clear aligners, especially in severe deep bite malocclusions, and a bite opening of 1.5 mm could be obtained due to lower incisors proclination rather than true bodily intrusion.[11,12]
Furthermore, extrusion movements are unpredictable and only 29.6% of the movements planned in the setup are achieved at the end of clear aligners treatment. However, there is an increasing evidence that aligners are effective in open bite cases, obtaining a significant amount of incisor palatal tipping and extrusion.[13] The difficulty in achieving pure extrusion is likely due to the poor grip of the aligners on the teeth.
If the vertical correction is limited to few teeth, the hybrid approach consists of fixed partial lingual appliances with different heights of the tubes, to facilitate the movements planned [Figure 6]. The position of lingual tubes depends on the difference in height between the interested teeth and the adjacent teeth; then, an accurate impression is necessary to simulate the presence of a lingual archwire in the setup and to keep the physical space under the F22 clear aligners [Figure 6].

- Vertical correction: (a and b) Initial photographs show an anterior open bite in an adult patient; (c and d) beginning of the hybrid treatment with F22 clear aligners combined with a 0.013 CuNiTi archwire insertion in lingual tubes, which were placed at different height to facilitate the planned movements; (e and f) case refinement after CuNiTi archwire complete expression; (g and h) final result.
The aligners completely envelope the partial fixed lingual appliances and follow the CuNiTi archwires expression [Figure 6].
However, the vertical malocclusions could be related to different problems and the diagnosis remains the essential object to choose the correct treatment plan.
CONCLUSIONS
Hybrid approach using clear aligners combined with partial fixed appliances is an efficient treatment alternative to avoid unpredictable movements. Moreover, this approach significantly reduces overall treatment time without a marked increase in cost.
Declaration of patient consent
Patient’s consent not required as patients identity is not disclosed or compromised.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Children's perceptions of smile esthetics and their influence on social judgment. Angle Orthod. 2016;86:1050-5.
- [CrossRef] [PubMed] [Google Scholar]
- Dynamic evaluation of anterior dental alignment in a sample of 8-to 11-year-old children. Int Orthod. 2012;10:177-89.
- [CrossRef] [PubMed] [Google Scholar]
- Predictability of orthodontic movement with orthodontic aligners: A retrospective study. Prog Orthod. 2017;18:35.
- [CrossRef] [PubMed] [Google Scholar]
- Efficacy of clear aligners in controlling orthodontic tooth movement: A systematic review. Angle Orthod. 2015;85:881-9.
- [CrossRef] [PubMed] [Google Scholar]
- Clinical effectiveness of invisalign orthodontic treatment: A systematic review. Prog Orthod. 2018;19:37.
- [CrossRef] [PubMed] [Google Scholar]
- How well does invisalign work? A prospective clinical study evaluating the efficacy of tooth movement with invisalign. Am J Orthod Dentofacial Orthop. 2009;135:27-35.
- [CrossRef] [PubMed] [Google Scholar]
- Treatment outcome with orthodontic aligners and fixed appliances: A systematic review with meta-analyses [published online ahead of print. Eur J Orthod. 2019;2019:cjz094.
- [CrossRef] [PubMed] [Google Scholar]
- The predictability of transverse changes with invisalign. Angle Orthod. 2017;87:19-24.
- [CrossRef] [PubMed] [Google Scholar]
- Maxillary molar distalization with aligners in adult patients: A multicenter retrospective study. Prog Orthod. 2016;17:12.
- [CrossRef] [PubMed] [Google Scholar]
- A systematic review of the accuracy and efficiency of dental movements with invisalign. Korean J Orthod. 2019;49:140-9.
- [CrossRef] [PubMed] [Google Scholar]
- Accuracy of clear aligners: A retrospective study of patients who needed refinement. Am J Orthod Dentofacial Orthop. 2018;154:47-54.
- [CrossRef] [PubMed] [Google Scholar]
- Management of overbite with the invisalign appliance. Am J Orthod Dentofacial Orthop. 2017;151:691-9e2.
- [CrossRef] [PubMed] [Google Scholar]
- Cephalometric evaluation of adult anterior open bite non-extraction treatment with invisalign. Dental Press J Orthod. 2017;22:30-8.
- [CrossRef] [PubMed] [Google Scholar]




