

Translate this page into:
The role of impacted third molar angulation on the anterior crowding

*Corresponding author: Gökçenur Gökçe, Department of Orthodontics, Izmir Katip Celebi University, Izmir 35040, Turkey. dtggokce@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Gökçe G, Akan B, Veli I. The role of impacted third molar angulation on the anterior crowding. APOS Trends Orthod 2021;11(1):56-61.
Abstract
Objectives:
The aim of this study was to assess the role of impacted third molar angulation on the severity of anterior crowding.
Materials and Methods:
Panoramic radiographs and three-dimensional (3D) digital models of 45 patients satisfying the following inclusion criteria were selected for this study. To calculate the irregularity index of Little, the sum of the contact point displacements from the anatomical contact point to the contact point among the lower canine teeth was measured on 3D digital models. Little’s irregularity index was used to classify patients as having mild, moderate, or severe crowding. For intragroup variance, comparisons T test was used. The Spearman single rank correlation coefficients were used to analyze any correlation among degree of crowding and (a) third molar inclination to base of mandible, (b) third molar inclination to occlusal plane, and (c) third molar inclination to second molar inclination respectively.
Results:
There were no statistical differences found in all tested parameters (i.e., third molar inclination to mandibular plane, inclination of the third molars to occlusal plane, and inclination of the third molars to second molars) among three groups (P > 0.005).
Conclusion:
It can be deduced that no relationship obtains among the third molar inclination to base of mandible, third molar inclination to occlusal plane, third molar inclination to second molar inclination, and the level of anterior crowding.
Keywords
Anterior crowding
Third molars
İrregularity index
Panoramic radiography

INTRODUCTION
The lower anterior crowding is a problem that may affect of the population about esthetics or oral hygiene. It has been a topic of research from the point of both the etiology and treatment for many years by orthodontists. In many studies, the lower incisor teeth were identified as the most crowding teeth in the mouth. There are many factors affecting the lower anterior crowding. The etiologies of this were tooth arch size discrepancy,[1] inclination of incisors to become retrocline with age,[1] mesial drift, mandibular anterior growth development and remodeling, before eruption, tooth tissue discrepancy, occlusion, soft-tissue maturation, and mandibular third molars.[2]
Impaction of the third molar tooth is one of the clinical problems that dentists may face in orthodontic treatment of adolescent patients.[3] Third molars frequently follow the abortive eruption path and remain impacted due to insufficient dental arch and area. The percentage of third molar impaction shows up to be rising and variable in different populations.[4] Furthermore, after the maxillary third molar, the mandibular third molars are the most commonly impacted tooth.[4]
In the orthodontic literature, the role of mandibular third molars in the lower anterior crowding has been examined by many researchers and presented.[5] The most controversial point is whether third molars impaction conduced to the development of malocclusion or recurrence, particularly in the anterior region of the dental arch.[5] In spite of many publications, there is still no clear answer to the question of whether impacted third molar teeth cause anterior dental arch crowding.[5]
Hasegawa et al.[6] investigated the effect of mandibular third molar on the anterior crowding and the angulation of teeth in the mandibular lateral sections in Mongolian subjects using dental casts and panoramic and oblique cephalometric radiographs. Björk et al.[7] examined 243 cases using the parameters obtained from cephalometric radiographs to determine the relationship between the area available mandibular third molars. Niedzielska[8] evaluated the dental arches length and width to detect the probable effect of third molars on mandibular incisor crowding using panoramic radiographs and dental casts.
First, in 1961, Bergstrom and Jensen[9] analyzed the effect of the third molar in the dental arch dimensions and stated that these teeth may also cause crowding in the region of mandibular incisors. Vego[10] reported that the eruption of the third molar teeth exerted mesial force on the adjacent teeth with causing crowding in the anterior region. Similarly, Lindqvist[11] argued that the eruption of the third molar teeth causes crowding in the mandibular incisors region by force transmission. In addition, Laskin[12] reported that many clinicians claimed that impacted third molars created an anteriorly directed force and caused crowding of the mandibular incisors.
There is no consensus as to whether there is a cause-and-effect relationship among the existence of lower third molars and anterior crowding. Since the results of the studies in the literature were different from each other, we aimed in this study to evaluate the relationship among the inclination of impacted third molar on the severity of mandibular incisors. The null hypothesis was that the severity of crowding did not worsen with the increase in the angulation of the impacted molars.
MATERIALS AND METHODS
A power analysis using G * Power software (version 3.1.3; Franz Faul University, Kiel, Germany) revealed that to obtain a power of 80% and an alpha (a) of 0.05, a sample size of 15 per group was needed.[6] Hence, panoramic radiographs and three-dimensional (3D) digital models of 45 (25 females and 20 males) patients (age range 18.7–23.3 years, mean 20.7 years) were selected from the archive of the Department of Orthodontics at X University and divided into three groups according to severity of crowding (minimum, moderate, and severe). The inclusion criteria were Angle Class I molar relationship,[6] ANB angle between 0 and 5 degrees,[13] no caries or restoration in the mandibular teeth,[6] no history of previous orthodontic treatment,[6] complete mandibular dental arch (except third molars),[14] age at least 17 years,[6] all four third molars impacted,[6] good quality orthopantomograms, and plaster casts available.[14]
After the plaster models were scanned with a 3D model laser scanner (D250 3D Dental Scanner; 3Shape A/S, Copenhagen, Denmark), digital models were obtained. These models were then analyzed by one researcher (X.X.) using the 3Shape Orthoanalyzer program using the 3Shape Orthoanalyzer software (version 1.0; 3Shape A/S).
The total displacement of anatomic contact points among mandibular canines was measured on the digital models and the index of Little’s irregularity was calculated for each patient [Figure 1].[15] According to this index, the subjects were divided into three groups to Little’s index of irregularity: Minimum crowding, moderate crowding, and severe crowding. The irregularity index presented by Little[16] was assessed to mandibular incisor crowding by measure the total of displacements among canines. The sum of these five measurements showed the irregularity index score for each patient. In addition, scoring for each patient’s crowding was carried out according to Little’s irregularity index classified as mild (0–3 mm), moderate (4–8 mm), severe (>8 mm).[16]
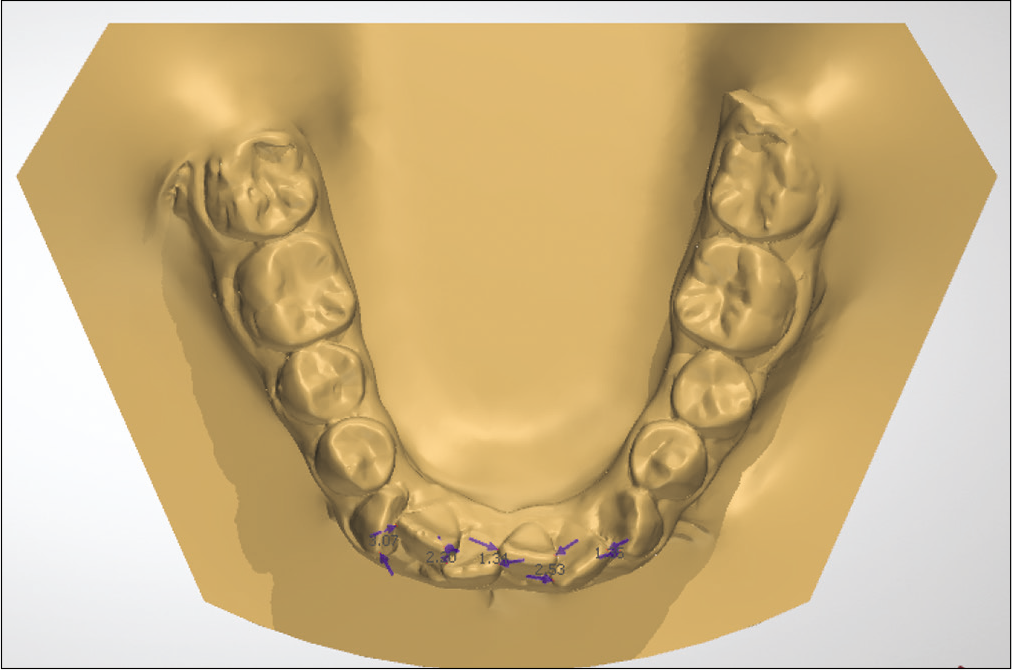
- Measurements of irregularity index on digital models. The blue arrows represent the linear displacement of the anatomic contact points of the anterior teeth.
Panoramic radiographs were obtained with an orthopantomograph machine using standardized techniques OP 300 (Instrumentarium Imaging, Tuusula, Finland). The magnification of the device is ×1.3. The radiographs were analyzed by a single observer.
While determining the impaction of third molar, panoramic radiographs were used. If the tooth was not completely erupt and the apical closure was not completed on the radiographs, this case was considered impacted.[15] Two-dimensional radiographic measurements of the impacted third molars in the mandible were taken on both sides and the average value of each side was evaluated. Measurements on the dental arch carried out as follows:
Angle of the third molar tooth relative to the base of the mandible (Angle A) [Figure 2].[17]
Mesioangular angulation of the third molars (the angle formed among the second and third molars drawn through the midpoint of the occlusal surface and root furcation) (Angle B) [Figure 2].[4]
The third molar to the second molar inclination (Angle C) [Figure 2].[17]
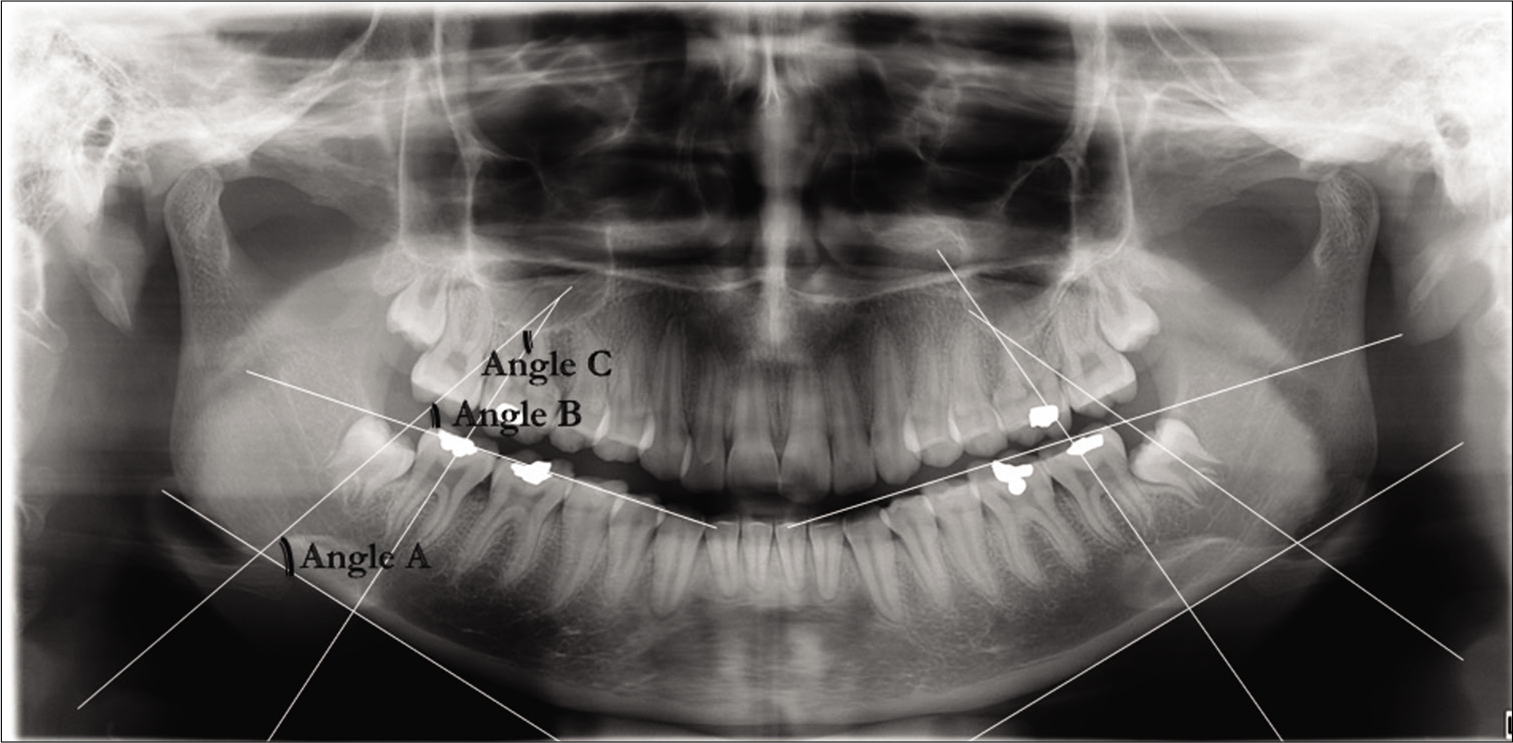
- Measurements on the panoramic radiographs: third molar to base of mandible (angle A), mesioangular angulation of the third molar (angle B), third molar to second molar inclination (angle C)
Statistical analysis
All statistical analyses were applied with the Statistical Package for the Social Sciences (SPSS 22.0 for Windows; Chicago, USA). The normality assumption was satisfied across the groups for the three dependent variables with test of Shapiro–Wilk. The Levene’s test for variance homogeneity test was applied to the data. The group variances were homogeneous for all three variables. The statistical assessment was performed using parametric tests. Comparison of groups were performed using a multivariate analysis of variance (MANOVA) with dependent variables. Arithmetic mean and standard deviation values were calculated and reported in tables.
RESULTS
Sex distribution and descriptive statistics including means and standard deviations for all data are listed in [Table 1]. According to the results, there was no significant difference among the subgroups.
| n | Mean | Standard error | 95% confidence interval | P | |||
|---|---|---|---|---|---|---|---|
| Male | Female | Lower bound | Upper bound | ||||
| Third molar to base of mandible | 20 | 25 | 60.625 | 1.786 | 57.021 | 64.229 | 0.657 |
| Third molar to occlusal plane | 20 | 25 | 45.381 | 1.722 | 41.906 | 48.856 | 0.360 |
| Third molar to second molar inclination | 20 | 25 | 24.418 | 1.631 | 21.127 | 27.709 | 0.089 |
| ANB angle | 20 | 25 | 2.800 | 1.892 | 0.600 | 5.000 | 0.078 |
NS: P>0.05, P<0.05
[Table 2] summarizes the comparisons among the three crowding conditions across three situations of lower third molar position.
| Minimum crowding | Moderate crowding | Severe crowding | F | P | Partial eta squared | ||||
|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | ||||
| Third molar to base of mandible | 62.95 | 11.66 | 59.49 | 12.1 | 59.44 | 12.17 | 0.425 | 0.657 | 0.2 |
| Third molar to occlusal plane | 48.11 | 11.87 | 45.95 | 10.07 | 42.08 | 12.57 | 1.047 | 0.36 | 0.47 |
| Third molar to second molar inclination | 19.74 | 8.22 | 24.75 | 9.37 | 28.77 | 14.27 | 2.566 | 0.89 | 0.109 |
Multivariate test (Pilla’s trace) [F(6. 82)=1.018, P=0.419, partial −ɳ2=0.069]
Based on the severity of the malocclusion, the third molar inclination to mandibular plane was found to be 62.95 ± 11.66, 59.49 ± 12.1, and 59.44 ± 12.17, respectively. Furthermore, the third molar inclination to occlusal plane was found to be 49.11 ± 11.87 in minimum crowding group, 45.95 ± 10.07 in moderate crowding group, and 42.08 ± 12.57 in severe crowding group. Finally, inclination of the third molars to the second molars was 19.74 ± 8.22 in minimum crowding group, 24.75 ± 9.37 in moderate crowding group, and 28.77 ± 14.27 in severe crowding group.
According to the results shown in [Table 2], no statistically significant changes were found in all tested parameters (i.e., third molar inclination to mandibular plane, inclination of the third molars to occlusal plane, and inclination of the third molars to second molars) among three groups (P > 0.005).
Based on these results, the null hypothesis of this study was accepted. In other words, the angulation of the third molars had no effects on lower anterior crowding.
DISCUSSION
The effect of the third molar impaction and position on lower anterior crowding has been the subject of interest by many investigators, especially orthodontists, for many years.[18] Evaluating the presence and angulation of the third molars are important for orthodontists when planning retention procedure. After orthodontic treatment, stability is an also important issue. There is no consensus in the literature as to whether third molars cause anterior crowding or contribute to instability of orthodontic results. So that, the aim of this study is to determine whether the impacted lower third molar teeth can affect the lower anterior crowding.
In our study, unlike most studies in the literature,[6,8,11] the samples were divided into three groups according to LII as minimum, middle, and severe crowding. Patients with dental and skeletal Class I according to the ANB angle and patients with all third molar teeth impacted were included in the study. Thus, standardization was tried to be achieved among patient subgroups.
Many different radiographic imaging systems have been used in the literature to evaluate the relationship between the third molar angulation and the degree of anterior crowding.[19] Conventional cross-sectional tomography and computed tomography (CT) methods for three-dimensional (3D) evaluation of the inclination of the impacted lower third molar and its relationship with the second molar are useful. Cone-beam computed tomography (CBCT) presents an innovation of tomographic imaging systems for dentistry. This system provides high-resolution and low radiation dose as an alternative to CT.[19] CBCT is used as a diagnostic tool in dentistry, especially in the extraction of impacted teeth, provides detailed information about the angulation of mandibular 3rd molar teeth and their relationship with adjacent teeth.[20]
Although clinicians agree that CT is advantageous in many dental practices, they do not prefer to use it routinely because of its additional radiation exposure and high cost. CT is not required if the 3D relationship among the mandibular second and the third molar angulation could accurately predict with analysis on panoramic radiography. On the other hand, there are few studies comparing tomography with panoramic radiography.[20] Furthermore, there are many studies used panoramic or lateral cephalometric radiography for evaluation of angulation of the impacted mandibular third molar in the literature. These radiographies are routinely used for orthodontic treatment or diagnosis. By this means, radiation dose imparted to patients is lower than CT.
Arai et al.[19] reported that angular differences between superimposed images may cause clinicians to make incorrect measurements on the third molar angulation during lateral cephalograms. However, Kamegai[21] concluded that due to the fact that the lateral segment was parallel to the film with 45° oblique lateral cephalograms, the third molar, and tooth in the lateral segment gave a more accurate projection and more preferable appearance. Haavikko et al.[22] evaluated the angulation of the third molars on panoramic radiographs and reported that there was no significant difference between the left and right sides. Hence, we decided to use panoramic radiographs both the left and right side to determine the angulation of the third molars as Hasegawa et al.[6] and Elsey and Rock[23] did.
The use of three-dimensional digital models is increasing day by day in dentistry. There are many studies in the literature comparing linear dental anatomical measurements attained from digital and plaster models.[20] Many authors reported no differentiation among linear measurements on plaster and digital models. Alcan et al.[24] evaluated the effects of conventional measures taken with alginate on the digital model accuracy and reported that digital orthodontic models are as reliable as conventional models and can be used safely in orthodontic clinics.
According to Ledyard’s[25] measurements made on lateral cephalometric X-rays, the development of the retromolar region continued until the age of 16. Therefore, eruption of the third molar teeth is unlikely to continue after this age. Hence, in the present study, the inclusion criteria were patients should be at least 17 years old.
Many factors play a role in the lower anterior crowding. These factors are; decreased arch length, increased tooth dimensions and atypical form, decreased intercanine distance anatomical features of the contact points of adjacent teeth and growth changes in the mandible occurring.[14] It is still unclear whether the third molar teeth have any effect on the alignment of the anterior teeth. According to the survey study of Laskin,[12] approximately 65% of the participants advocated the idea that the 3rd molar teeth cause anterior crowding. Bishara[3] stated that it is difficult to prove the theory that the third molars apply force to the anterior teeth. Conversely, Zachrisson[26] claimed that late mandibular anterior crowding was caused by insufficient space for the development of the 3rd molar tooth. The researcher showed the reason for the crowding in adolescent and young adults as the force directed mesially by the 3rd molar tooth. Hattab et al.[4] investigated the arch dimensions of the cases with erupted and impacted mandibular third molars and they observed that the most important factor causing the third molar impaction was an insufficient retromolar area. According to Niedzielska,[8] when there is not enough space which is available in the dental arches, the 3rd molar teeth can lead to anterior crowding, however, when sufficient space is available, these teeth can erupt in the normal position and do not cause any changes in the angulation and position of other teeth. Harradine et al.[27] and Richardson[28] reported a correlation among the impacted third molars and anterior lower crowding. Similarly, Schwarze,[29] Bergstrom and Jensen,[9] and Sheneman[30] indicated that the presence of third molars was associated with severe anterior crowding.
On the contrary, we found no correlation between impacted third molar presence with anterior crowding. Similar to our results, other researchers found no significant influence of the third molars on anterior crowding.[31,32] In addition, Bishara[3] stated that the third molars had no considerable effect on the crowding of the mandibular anterior teeth. van der Schoot et al.[33] evaluated the relationship between dental crowding and the presence of third molars. They reported that the presence of third molars did not have a significant effect on the development of late anterior crowding. Karasawa et al.[34] aimed to reveal a correlation between the presence of third molars and mandibular incisor crowding in a cross-sectional study in a large group of 300 subjects. Investigators observed no correlation among maxillary or mandibular third molars and the anterior crowding.
The degree of third molar angulation is also considered to be associated with third molar impaction and anterior crowding.[18] Elsey and Rock[23] examined angular and linear measurements of lower third molars on panoramic radiograms of 30 patients to investigate whether mandibular premolar extraction had an effect on the eruption of the third molar teeth. Researchers reported that premolar teeth extraction reduces the mesial angulation of the third molar teeth by 7°. Saysel et al.[35] also promoted the idea that orthodontic treatment containing premolar extraction showed an improvement of mandibular third molars angulation relative to the occlusal plane. However, they did not evaluate the right and left sides separately. Hasegawa et al.[6] claimed that there was no significant relationship between the angulation of teeth relative to the mandibular plane and Little’s irregularity index. In similarly, we found that there was not statistically significant difference among severity of crowding and mandibular third molar angulation.
Bishara[3] stated that it is difficult to prove the theory that the third molars apply force to the anterior teeth. Conversely, Zachrisson[26] claimed that late mandibular anterior crowding was caused by insufficient space for the development of the 3rd molar tooth. The researcher showed the reason for the crowding in adolescent and young adults as the force directed mesially by the 3rd molar tooth. Hattab et al.[4] investigated the arch dimensions of the cases with erupted and impacted mandibular third molars and they observed that the most important factor causing the third molar impaction was an insufficient retromolar area.
The different results of these studies lead to a lack of consensus on the role of third molars in anterior crowding. The data obtained from our study showed that there was no relationship among the inclination of mandibular third molar teeth and degree of anterior crowding. This result agrees with the studies which not confirm the relation among mandibular third molar angulation and anterior crowding.
Limitations
According to the results of the power analysis performed before the study, although including at least 15 patients in each group was sufficient for the accuracy of the results of the study, a larger sample size may provide more accurate results. In addition, in our study, we worked on two-dimensional orthopantomograph images, since it would not be ethical to take CBCT recording, especially in minimal crowding cases. Hence, this issue constituted the limitation of our study.
CONCLUSION
There is no definite conclusion about the role of third molar teeth in the formation of anterior crowding. Our results do not support a cause-and-effect relationship among the variables. Hence, the third molar extraction is not essential to avoid anterior tooth crowding or post-orthodontic relapse.
Declaration of patient consent
Patient’s consent not required as patients identity is not disclosed or compromised.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Factors that affect the alignment of the mandibular incisors: A longitudinal study. Am J Orthod. 1973;64:248-57.
- [CrossRef] [Google Scholar]
- The great eights debate: Do the mandibular third molars affect incisor crowding? A review of the literature. Dent Update. 1993;20:242-6.
- [Google Scholar]
- Third molars: A dilemma! Or is it? Am J Orthod Dentofacial Orthop. 1999;115:628-33.
- [CrossRef] [Google Scholar]
- Radiographic evaluation of mandibular third molar eruption space. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1999;88:285-91.
- [CrossRef] [Google Scholar]
- The role of mandibular third molars on lower anterior teeth crowding and relapse after orthodontic treatment: A systematic review. Sci World J. 2014;2014:615429.
- [CrossRef] [PubMed] [Google Scholar]
- Influence of third molar space on angulation and dental arch crowding. Odontology. 2013;101:22-8.
- [CrossRef] [PubMed] [Google Scholar]
- Mandibular growth and third molar impaction. Acta Odontol Scand. 1956;14:231-72.
- [CrossRef] [Google Scholar]
- Third molar influence on dental arch crowding. Eur J Orthod. 2005;27:518-23.
- [CrossRef] [PubMed] [Google Scholar]
- Extraction of third molars in cases of anticipated crowding in the lower jaw. Am J Orthod. 1982;81:130-9.
- [CrossRef] [Google Scholar]
- Evaluation of the third molar problem. J Am Dent Assoc. 2006;82:824-8.
- [CrossRef] [PubMed] [Google Scholar]
- Steinernorms in Children 13-16 Years of Age in Ankara with Normal Occlusions, Thesis Ankara, Turkey: Ankara University; 1976.
- [Google Scholar]
- Effect of the lower third molars on the lower dental arch crowding. Stomatologija. 2006;8:80-4.
- [Google Scholar]
- Prediction of mandibular third-molar impaction in adolescent orthodontic patients. Am J Orthod Dentofacial Orthop. 2006;130:47-55.
- [CrossRef] [PubMed] [Google Scholar]
- The irregularity index: A quantitative score of mandibular anterior alignment. Am J Orthod. 1975;68:554-63.
- [CrossRef] [Google Scholar]
- Panoramic radiographic predictors of mandibular third molar eruption. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2006;102:154-8.
- [CrossRef] [PubMed] [Google Scholar]
- Role of third molars in orthodontics. World J Clin Cases. 2015;3:132-40.
- [CrossRef] [PubMed] [Google Scholar]
- Development of a compact computed tomographic apparatus for dental use. Dentomaxillofac Radiol. 1999;28:245-8.
- [CrossRef] [PubMed] [Google Scholar]
- Reliability of panoramic radiography in evaluating the topographic relationship between the mandibular canal and impacted third molars. J Am Dent Assoc. 2004;135:312-8.
- [CrossRef] [PubMed] [Google Scholar]
- Studies on the position of canines, premolars and molars by forty-five degrees oblique cephalometric roentgenography. Jpn J Orthod. 1973;32:23-46.
- [Google Scholar]
- Predicting angulational development and eruption of the lower third molar. Angle Orthod. 1978;48:39-48.
- [Google Scholar]
- Influence of orthodontic treatment on development of third molars. Br J Oral Maxillofac Surg. 2000;38:350-3.
- [CrossRef] [PubMed] [Google Scholar]
- The relationship between digital model accuracy and time-dependent deformation of alginate impressions. Angle Orthod. 2009;79:30-6.
- [CrossRef] [PubMed] [Google Scholar]
- A study of the mandibular third molar area. Am J Orthod Dentofacial Orthop. 1953;39:366-73.
- [CrossRef] [Google Scholar]
- Mandibular third molars and late lower arch crowding-the evidence base. World J Orthod. 2005;6:180-6.
- [Google Scholar]
- The effect of extraction of third molars on late lower incisor crowding: A randomized controlled trial. Br J Orthod. 1998;25:117-22.
- [CrossRef] [PubMed] [Google Scholar]
- Late lower arch crowding: The aetiology reviewed. Dent Update. 2002;29:234-8.
- [CrossRef] [PubMed] [Google Scholar]
- The influence of third molar germectomy-a comparative long-term study In: Transactions of the Third International Orthodontic Congress, Held in London 1973. Missouri: Mosby; 1975. p. :551-62.
- [Google Scholar]
- Third Molar Teeth and their Effect upon the Lower Anterior Teeth: A Survey of Forty-Nine Orthodontic Cases Five Years after Band Removal. In: MSD Thesis. United States: St. Louis University; 1968.
- [CrossRef] [Google Scholar]
- The effect of removal of all third molars on the dental arches in the third decade of life. Cranio. 1996;12:23-7.
- [CrossRef] [PubMed] [Google Scholar]
- The influence of mandibular third molars on mandibular anterior teeth. Am J Orthod. 1962;48:786-7.
- [CrossRef] [Google Scholar]
- Clinical relevance of third permanent molars in relation to crowding after orthodontic treatment. J Dent. 1997;25:167-9.
- [CrossRef] [Google Scholar]
- Crosssectional study of correlation between mandibular incisor crowding and third molars in young Brazilians. Med Oral Patol Oral Cir Bucal. 2013;18:e505-9.
- [CrossRef] [PubMed] [Google Scholar]
- The effects of first premolar extractions on third molar angulations. Angle Orthod. 2005;75:719-22.
- [Google Scholar]




