

Translate this page into:
Using the Invisalign® system in conjunction with extraction for the treatment of Class II malocclusion with severe anterior crowding

*Corresponding author: Lionel Hui Bon Hoa, Invisalign Singapore Pte Ltd, Singapore. lhuibonhoa@aligntech.com
-
Received: ,
Accepted: ,
How to cite this article: Hui Bon Hoa L. Using the Invisalign® system in conjunction with extraction for the treatment of Class II malocclusion with severe anterior crowding. APOS Trends Orthod 2021;11(1):81-7.
Abstract
Clear aligners are a well-established alternative to conventional fixed orthodontic appliances for treating mild-to-moderate malocclusion. This case report details the successful treatment of a 14-year-old female patient with Class II malocclusion, crowding, and dental crossbite using extraction and the Invisalign® system. Achieving satisfactory anterior guidance by correcting the anterior crossbite and reducing the overjet and overbite was the primary treatment goal. Secondary treatment objectives included upper and lower midline alignment, leveling and alignment of arches, and achieving a Class I canine relationship for adequate canine guidance. Two sets of clear aligners were chosen; the first for alignment and the second for refinement. Extraction of teeth 14 and 24 were performed during the first aligner treatment phase, with space closure achieved by the distal movement of canine and posterior teeth mesialization. The second set of aligners refined the dentition by correcting the posterior open bite and extrusion of posterior teeth. Treatment duration was 13.5 months. By the end of treatment, the Invisalign system in conjunction with tooth extraction established an ideal overbite and overjet, corrected the crossbite, and achieved a Class I canine relationship with minimal disruption to the patient’s esthetic appearance. In addition, root axes were parallel and well controlled, despite extractions and space closure. Awareness of the dental biomechanics when clear aligners and extraction are used may be imperative for yielding successful outcomes for patients with Class II malocclusion and extractions.
Keywords
Class II malocclusion
Extractions
Crowding
Invisalign

INTRODUCTION
Malocclusion is a frequent occlusal trait observed among children and adolescents.[1-4] Severe deviations can prevent proper dentofacial development, leading to dental injury and impaired oral function.[5,6] Moreover, maligned dentition can negatively impact the emotional and social well-being of adolescents.[7,8] Children and adolescents cite esthetic reasons for seeking treatment for their malocclusion[9,10] and concurrent with rapid advancements in orthodontics, patients have been increasingly expecting treatment options to be both esthetic and comfortable.[11,12] Conventional orthodontic methods and devices such as braces, arch wires, and ligatures are associated with an unideal facial appearance[13] and may impede proper dental hygiene, leading to periodontal complications.[14,15] Moreover, the discomfort associated with fixed orthodontic appliances can impart a negative quality of life in adolescents.[16,17]
Since its approval by the Food and Drug Administration in 1998, the Invisalign® system by Align Technology, Inc. (San Jose, CA, USA) has now become an established esthetic alternative to conventional fixed orthodontic appliances.[18,19] Initially indicated for minor crowding and spacing, its continuous improvement and development of attachment designs such as SmartTrack, and auxiliaries such as Power Ridge and Precision Cut features, have expanded the capabilities of this device. According to the Invisalign® Tooth Movement Assessment Overview, the Invisalign system can accomplish significant tooth movement, ranging from 20° for molars to 45° for canine and premolars, root movements of 4 mm for anterior and posterior teeth, and extrusions and intrusions of 2.5 mm for anterior teeth.
Recent systematic reviews have demonstrated that the Invisalign system is a viable alternative to conventional orthodontic devices for the correction of mild-to-moderate malocclusion.[20,21] The Invisalign system has also demonstrated success in the treatment of extraction cases and complex malocclusions.[22-26] While recent enhancements in the Invisalign system have resulted in an overall improvement in mean accuracy, challenges still persist, like with brackets and wires, in achieving certain movements with this treatment modality.[27,28] Nevertheless, the transparency and comfort of the Invisalign system have been cited by patients as key advantages over conventional appliances.[29,30]
This case report details the successful correction of a Class II malocclusion, crowding, and dental crossbite with the Invisalign system in conjunction with extraction.
PATIENT PROFILE AND DIAGNOSIS
A 14-year-old healthy female patient presented in November 2015. Her principal esthetic concern was the crowding of her upper anterior teeth. She had a mesofacial profile with a skeletal Class II relationship. Clinical examination, intraoral photographs, and radiographs revealed the following dental concerns: (1) Half cuspid Class II canine and molar relationship; (2) narrow upper arch; (3) 3 mm deviation to the left of the facial midline; (4) overjet and overbite of 4 mm; (5) anterior crossbite at tooth 22; (6) lower anterior teeth crowding of 4 mm; and (7) upright lower incisors [Figure 1]. No functional concerns were reported.
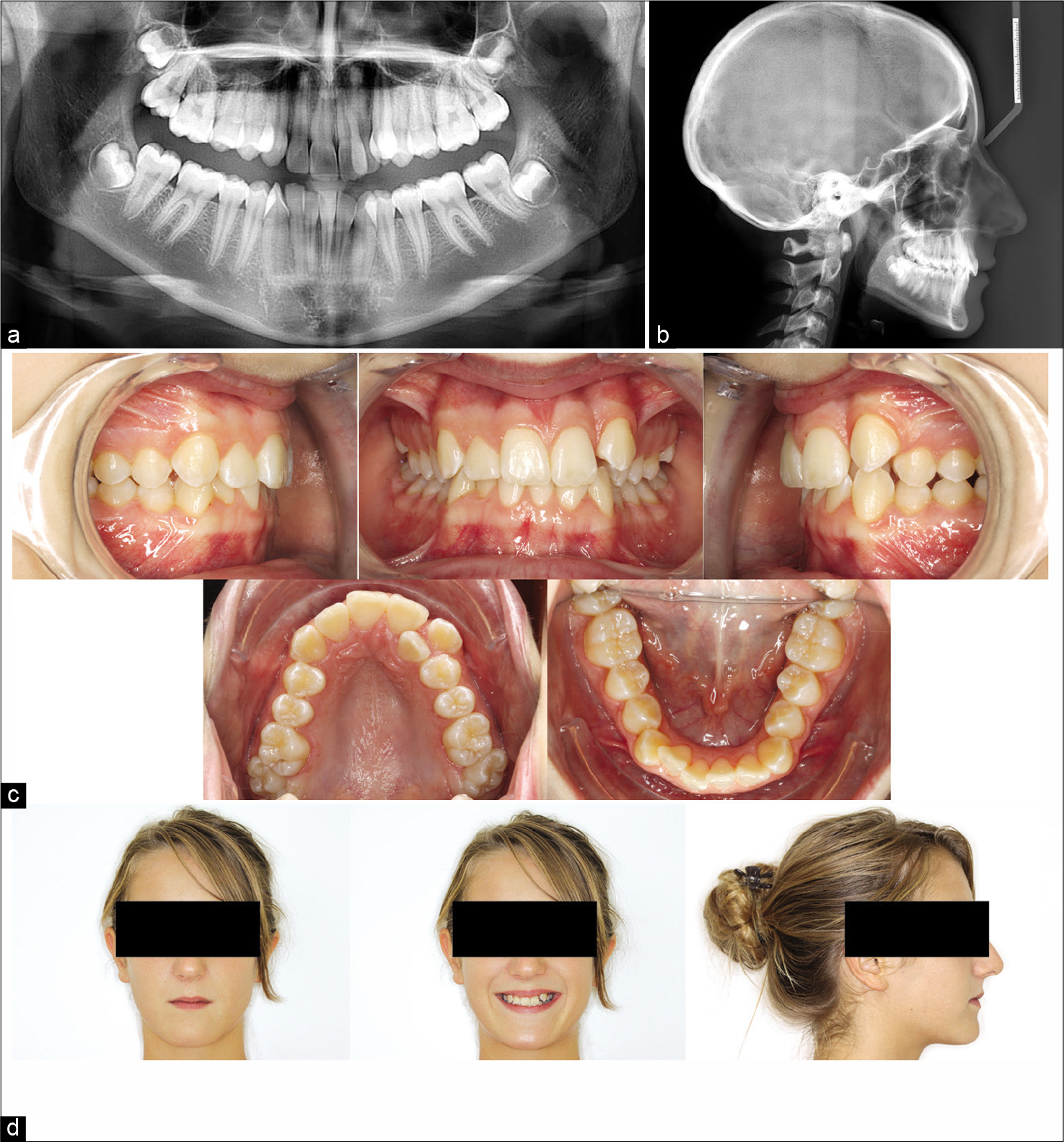
- Clinical examination of the initial dental status. Pre-treatment (a) panoramic radiograph, (b) lateral cephalogram, (c) intraoral photographs, and (d) extraoral photographs of the facial profile.
TREATMENT OBJECTIVES
The principal objective was to achieve satisfactory anterior guidance by reducing the overjet and overbite and by correcting the anterior crossbite. Ancillary treatment goals included aligning the upper and lower midline, leveling and alignment of arches, and achieving a Class I canine relationship to allow adequate canine guidance.
TREATMENT PROGRESS
A treatment plan using the Invisalign system with two sets of clear aligners was chosen to achieve the patient’s treatment objectives. Due to severe anterior crowding and lack of space in the upper arch, extractions of teeth 14 and 24 were required. As the lower incisors were upright without much crowding, no extractions were performed in the lower arch, thereby enabling a Class I canine and Class II molar relationship. A ClinCheck® treatment plan (Align Technology, Inc. San Jose, CA, USA) was developed before commencing the orthodontic treatment using the Invisalign system. Following the simulated outcomes from the ClinCheck treatment plan, attachments were added to the following teeth: (1) A rectangular, horizontal, gingival, and beveled attachment on tooth 22 to control buccal movement, (2) optimized attachments on teeth 13 and 23 for axis control, and (3) conventional rectangular vertical attachments on teeth 15, 16, 25, and 26 to limit posterior mesialization [Figure 2a]. Extraction of teeth 14 and 24 was performed after commencing Invisalign treatment. The space closure following extraction was corrected by distal movement of the canine teeth and mesialization of the posterior teeth to achieve a Class II molar relationship [Figure 2b]. In addition, slight leveling was conducted on the lower arch. No overcorrection was performed during this treatment phase. The alignment stage was conducted using 37 upper and 19 lower aligners, each worn weekly for 9 months. The initial treatment phase yielded favorable outcomes, with the closure of extraction space, and achievement of teeth alignment [Figure 3]; however, a slight posterior open bite was observed (2 mm on the left and 1 mm on the right side).
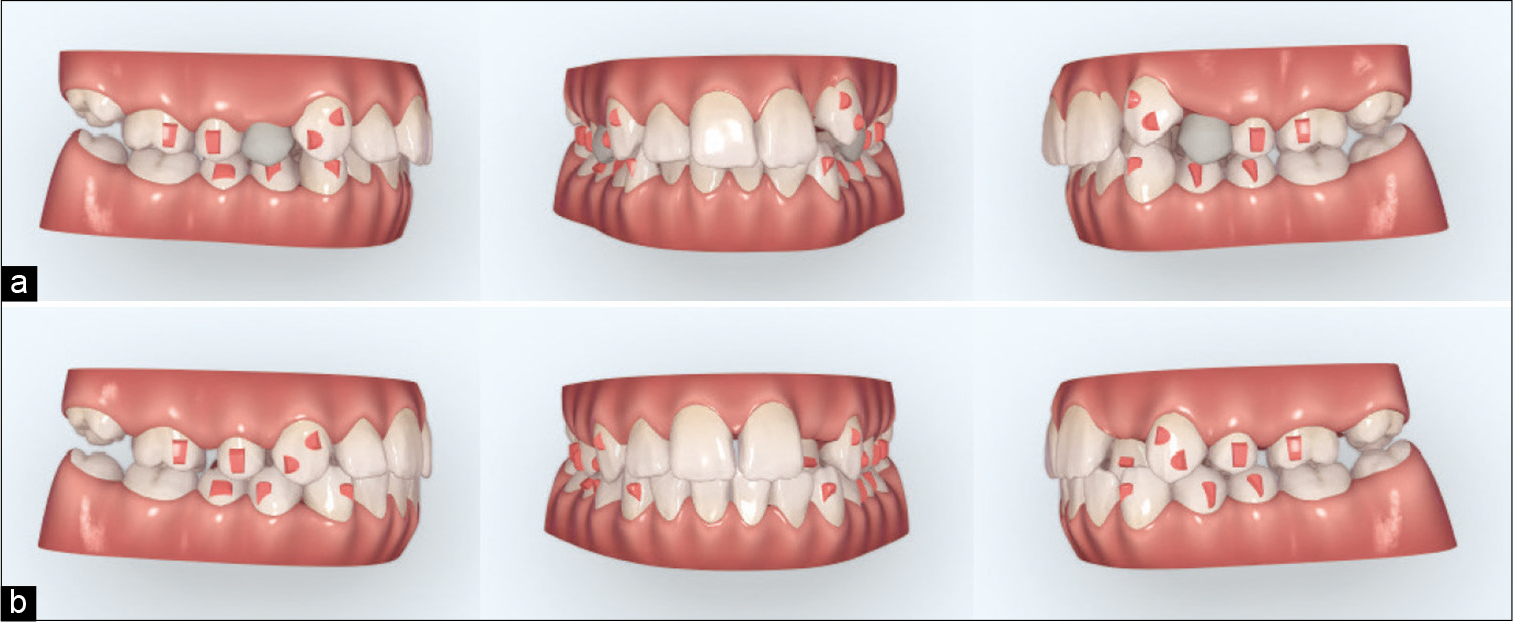
- ClinCheck treatment plan for alignment stage (a) before and (b) after extraction. Attachments are represented as red squares.

- (a) Intra- and (b) extraoral photographs after the alignment stage.
A second ClinCheck treatment plan was developed, and based on those results, additional aligners were employed, with two conventional horizontal attachments on teeth 15 and 25 [Figure 4]. During this 4.5-month course, 14 upper and 15 lower aligners were worn weekly. At the end of this refinement phase, posterior teeth were extruded and posterior open bite was corrected.

- ClinCheck treatment plan for the refinement stage. Red squares represent attachments and blue lines represent Power Ridges.
TREATMENT ALTERNATIVES
The principal treatment alternative discussed with the patient was non-extraction with expansion, maxillary distalization, and interproximal reduction. This approach would have yielded a broader upper arch with a broader smile (i.e., no black triangles), and a less retrusive profile. Disadvantages of this treatment alternative would have involved the risk of proclined upper incisors, longer duration of treatment, and the potential of not achieving the desired treatment goals and, thus, necessitating the extraction of teeth 18 and 28. The benefits and shortcomings of using buccal and lingual brackets were also discussed with the patient. However, since the patient’s concerns were also to do with esthetics and comfort, she was pleased to know that the clear aligner system could be used to achieve her treatment objectives.
TREATMENT RESULTS
Post-treatment results after 13.5 months of treatment demonstrated that the patient’s treatment objectives were met [Figure 5]. After the two treatment stages, ideal overbite and overjet were established, a Class I canine and Class II molar relationship was achieved, and crossbite was corrected. Overall, the patient’s smile was improved after the treatment.
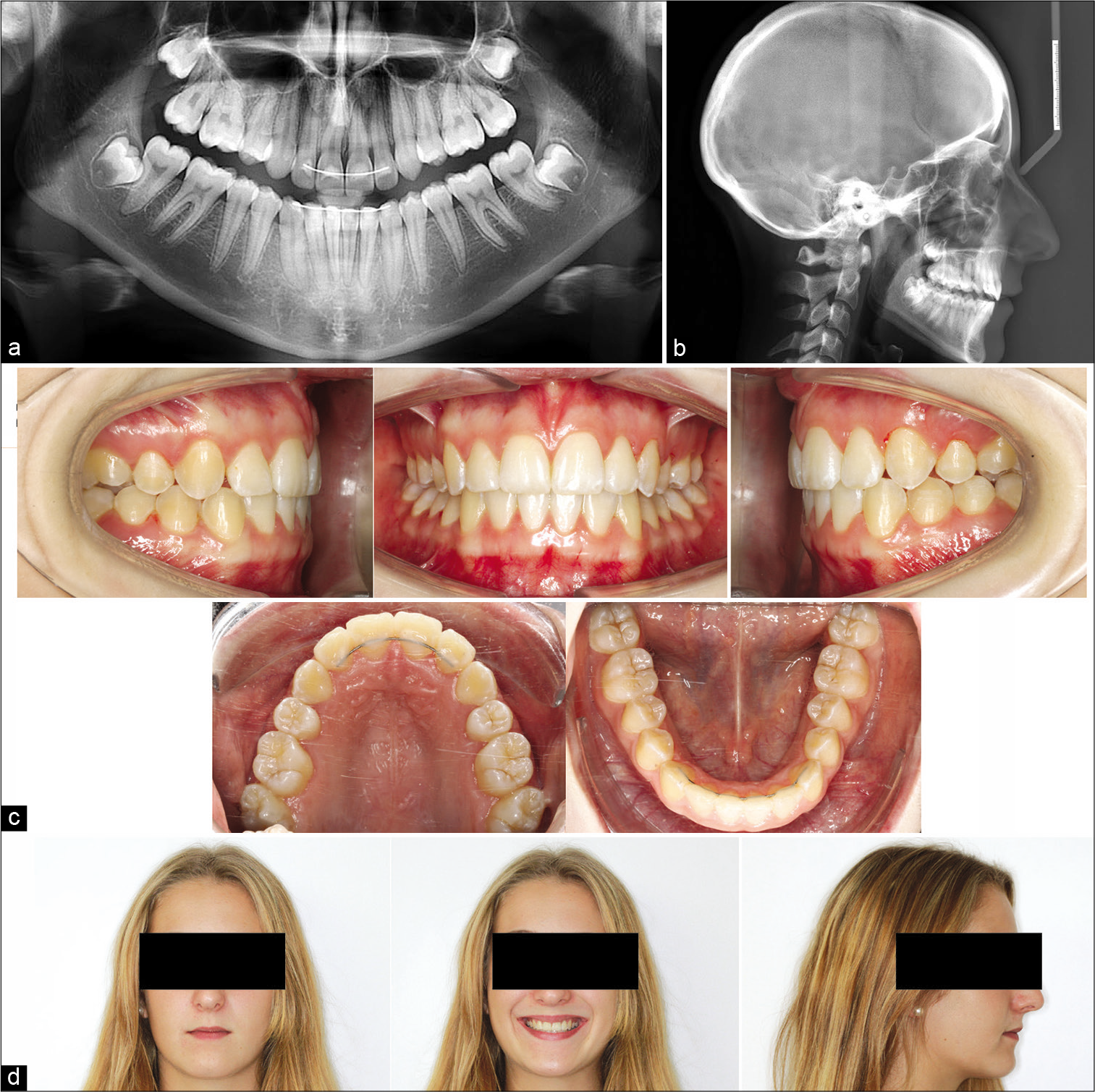
- Clinical examination of the post-treatment dental status. Post-treatment (a) panoramic radiograph, (b) lateral cephalogram, (c) intraoral photographs, and (d) extraoral photographs of the facial profile.
The patient was satisfied and highly motivated throughout the procedure. Furthermore, she was provided fixed and removal retainers (Vivera®, Align Technology, Inc., San Jose, CA, USA) for life to prevent relapse and to maintain dental position.
DISCUSSION
Clear aligners, such as the Invisalign system, address the esthetic concerns associated with conventional methods while still maintaining efficacy, especially in less severe cases of malocclusion.[20,21] This case demonstrated the successful use of the Invisalign system to correct complex anterior crowding and skeletal Class II malocclusion in conjunction with extraction. By treatment end, ideal overbite and overjet were established, crossbite was corrected, and a Class I canine relationship was achieved with minimal disruption to the patient’s esthetic appearance during treatment. Moreover, root axes were well controlled and parallel, despite the extractions and space closure procedures.
The ClinCheck treatment plan is not only an important tool for assessing a treatment approach but also facilitates the monitoring of treatment progress. While the ClinCheck program helps in designing the treatment plan, clinicians should be aware of the biomechanical basis of the treatment and should plan to mitigate the risk of undesirable outcomes. However, few studies have recommended overcorrection using the Invisalign system, citing the lack of root control.[31-33] In this case, an overcorrection of the lower incisor intrusion and more labial root torque on the upper incisors could have been added at the first ClinCheck treatment plan to avoid the posterior open bite. Furthermore, when the second ClinCheck plan was developed, the posterior open bite could have been corrected using bond buttons and vertical elastics without the use of additional aligners. Alternatively, mesial attachments on the buccal side of tooth 16 and 26 could have improved the closure of the posterior bite. InvisalignG6 for first premolar extractions has been designed to improve therapeutic outcomes of bimaxillary protrusion or severe crowding.[34] However, InvisalignG6 protocol was not applicable for this case since more than 2 mm (G6, maximum anchorage) and even more than 5 mm (G6+, moderate anchorage) of posterior mesialization was required to achieve Class II molar relationship.
While the use of the clear aligner system with tooth extraction has yielded satisfactory outcomes, the apparent “tight smile” could be a cause for concern. Indeed, this outcome may have been circumvented by opting for a non-extraction treatment option with conventional methods.[35-37] However, for this case, the extent of crowding was considerable and required space for the distalization of canines to achieve a Class I canine relationship. Few studies have reported the successful treatment of complex cases with clear aligners, and robust evidence through randomized controlled trials is lacking.[24-26] While the Invisalign system can be used to treat most malocclusions, complex cases such as a severe deep bite or mesialization of molars may require auxiliaries, such as temporary anchorage devices or segmental wires.[38,39]
CONCLUSION
This case report demonstrated that the Invisalign system, in conjunction with extraction, corrected complex anterior crowding and moderate malocclusion in a teenage female patient and yielded satisfactory outcomes. The treatment was also non-invasive and thus promoted a high degree of compliance.
Acknowledgments
The author acknowledges the patient for granting her consent to be included in this case report. Editorial assistance was provided by Isuru Wijesoma from MediTech Media (Singapore), which was funded by Align Technology, Inc., in accordance with Good Publication Practice (GPP3) guidelines.
Declaration of patient consent
The author certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Editorial assistance was funded by Align Technology, Inc. The sponsor had no role in the design, analysis, interpretation of the study, and the decision to submit the report for publication.
Conflicts of interest
The author is currently employed by a subsidiary of Align Technology, Inc. However, the views and opinions expressed in this publication are independent and based on the author’s own experiences as an Invisalign provider and do not purport to reflect the views or opinions of Align Technology, Inc., and/or any of its affiliates. The analysis shared in this publication and the presentation of case material herein does not imply any expression of guarantee on case outcomes by the author or Align Technology, Inc. Furthermore, editorial assistance was funded by Align Technology, Inc. The sponsor had no role in the design, analysis, interpretation of the study, and the decision to submit the report for publication.
References
- Global distribution of malocclusion traits: A systematic review In: Dental Press J Orthod. Vol 23. 2018. p. :1-10.
- [CrossRef] [PubMed] [Google Scholar]
- Sci Rep. 2018;8:4716-25.
- [CrossRef] [PubMed] [Google Scholar]
- Prevalence of malocclusion and orthodontic treatment need in children and adolescents in Bogota, Colombia. An epidemiological study related to different stages of dental development. Eur J Orthod. 2001;23:153-67.
- [CrossRef] [PubMed] [Google Scholar]
- Prevalence of malocclusion in Italian schoolchildren and orthodontic treatment need. Eur J Paediatr Dent. 2013;14:314-8.
- [Google Scholar]
- Exploring the impact of malocclusion and dentofacial anomalies on the occurrence of traumatic dental injuries in adolescents. Angle Orthod. 2017;87:816-23.
- [CrossRef] [PubMed] [Google Scholar]
- Impact of malocclusion and dentofacial anomalies on the prevalence and severity of dental caries among adolescents. Angle Orthod. 2015;85:1027-34.
- [CrossRef] [PubMed] [Google Scholar]
- The impact of malocclusion on the quality of life among children and adolescents: A systematic review of quantitative studies. Eur J Orthod. 2015;37:238-47.
- [CrossRef] [PubMed] [Google Scholar]
- Effect of malocclusion on the self-esteem of adolescents. J Orthod Sci. 2017;6:123-8.
- [CrossRef] [PubMed] [Google Scholar]
- A systematic review of individual motivational factors in orthodontic treatment: Facial attractiveness as the main motivational factor in orthodontic treatment. Int J Dent. 2014;2014:938274.
- [CrossRef] [PubMed] [Google Scholar]
- Patient and parent motivation for orthodontic treatment-a questionnaire study. Eur J Orthod. 2010;32:447-52.
- [CrossRef] [PubMed] [Google Scholar]
- Clear Aligners Market Size, Share and Industry Analysis by Patient Age Group (Teenager, Adults), by End-User (Hospitals, Dental and Orthodontic Clinics) and Regional Forecast 2019-2026. Available from: https://www.fortunebusinessinsights.com/industry-reports/clear-aligners-market-101377 [Last accessed on 2020 Sep]
- [Google Scholar]
- Trends or evidence: What do orthodontists want to rely on? In: Dental Press J Orthod. Vol 24. 2019. p. :7-8.
- [CrossRef] [Google Scholar]
- Assessment of perceived orthodontic appliance attractiveness. Am J Orthod Dentofacial Orthop. 2008;133:S68-78.
- [CrossRef] [PubMed] [Google Scholar]
- Impact of dental neglect score on oral health among patients receiving fixed orthodontic treatment: A cross-sectional study. J Int Soc Prev Community Dent. 2016;6:120-4.
- [CrossRef] [PubMed] [Google Scholar]
- The effect of orthodontic therapy on periodontal health: A review of the literature. Int J Dent. 2014;2014:585048.
- [CrossRef] [PubMed] [Google Scholar]
- Discomfort associated with fixed orthodontic appliances: Determinant factors and influence on quality of life In: Dental Press J Orthod. Vol 19. 2014. p. :102-7.
- [CrossRef] [PubMed] [Google Scholar]
- Great expectations: What do patients expect and how can expectations be managed? J Orthod. 2013;40:112-7.
- [CrossRef] [PubMed] [Google Scholar]
- Esthetic orthodontic treatment using the Invisalign appliance for moderate to complex malocclusions. J Dent Educ. 2008;72:948-67.
- [CrossRef] [PubMed] [Google Scholar]
- Lower incisor extraction treatment with the Invisalign system. J Clin Orthod. 2002;36:95-102.
- [Google Scholar]
- Clinical effectiveness of Invisalign® orthodontic treatment: A systematic review. Prog Orthod. 2018;19:37-60.
- [CrossRef] [PubMed] [Google Scholar]
- A comparison of treatment effectiveness between clear aligner and fixed appliance therapies. BMC Oral Health. 2019;19:24.
- [CrossRef] [PubMed] [Google Scholar]
- Invisalign treatment of lower incisor extraction cases. Aust Orthod J. 2016;32:82-7.
- [Google Scholar]
- Lower incisor extraction treatment with the Invisalign® technique: Three case reports. J Orthod. 2015;42:33-44.
- [CrossRef] [PubMed] [Google Scholar]
- Four-premolar extraction treatment with Invisalign. J Clin Orthod. 2006;40:493-500.
- [Google Scholar]
- Surgical-orthodontic treatment using the Invisalign system. J Clin Orthod. 2008;42:237-45.
- [Google Scholar]
- Comparing outcomes in orthognathic surgery using clear aligners versus conventional fixed appliances. J Craniofac Surg. 2019;30:1488-91.
- [CrossRef] [PubMed] [Google Scholar]
- How well does Invisalign work? A prospective clinical study evaluating the efficacy of tooth movement with Invisalign. Am J Orthod Dentofacial Orthop. 2009;135:27-35.
- [CrossRef] [PubMed] [Google Scholar]
- Has Invisalign improved? A prospective follow-up study on the efficacy of tooth movement with Invisalign. Am J Orthod Dentofacial Orthop. 2020;158:420-5.
- [CrossRef] [PubMed] [Google Scholar]
- Motivation, acceptance and problems of Invisalign patients. J Orofac Orthop. 2005;66:162-73.
- [CrossRef] [PubMed] [Google Scholar]
- Discomfort associated with Invisalign and traditional brackets: A randomized, prospective trial. Angle Orthod. 2017;87:801-8.
- [CrossRef] [PubMed] [Google Scholar]
- Influence of attachments and interproximal reduction on the accuracy of canine rotation with Invisalign. A prospective clinical study. Angle Orthod. 2008;78:682-7.
- [CrossRef] [Google Scholar]
- Invisalign® treatment in the anterior region: Were the predicted tooth movements achieved? J Orofac Orthop. 2012;73:365-76.
- [CrossRef] [PubMed] [Google Scholar]
- A systematic review of the accuracy and efficiency of dental movements with Invisalign®. Korean J Orthod. 2019;49:140-9.
- [CrossRef] [PubMed] [Google Scholar]
- Align Technology, I. Introducing Invisalign G6. Discover New Possibilities. Available from: http://www.invisalign-g6.com/enxa [Last accessed on 2020 Sep]
- [Google Scholar]
- How accurate is Invisalign in nonextraction cases? Are predicted tooth positions achieved? Angle Orthod. 2017;87:809-15.
- [CrossRef] [PubMed] [Google Scholar]
- Nonextraction treatment of a skeletal Class III malocclusion. Am J Orthod Dentofacial Orthop. 2009;136:736-45.
- [CrossRef] [PubMed] [Google Scholar]
- Class II malocclusion nonextraction treatment with growth control In: Dental Press J Orthod. Vol 19. 2014. p. :113-22.
- [CrossRef] [PubMed] [Google Scholar]
- Effect of clear aligner therapy on the buccolingual inclination of mandibular canines and the intercanine distance. Angle Orthod. 2016;86:10-6.
- [CrossRef] [PubMed] [Google Scholar]
- Outcome assessment of Invisalign and traditional orthodontic treatment compared with the American board of orthodontics objective grading system. Am J Orthod Dentofacial Orthop. 2005;128:292.
- [CrossRef] [PubMed] [Google Scholar]




