

Translate this page into:
Simplified application of midpalatal miniscrew in the retreatment of a hyperdivergent case – A case report

-
Received: ,
Accepted: ,
How to cite this article: Lin SC, Thavarungkul R, Chen YP, Wang SH. Simplified application of midpalatal miniscrew in the retreatment of a hyperdivergent case – A case report. APOS Trends Orthod. doi: 10.25259/ APOS_6_2024
Abstract
Whole dentition intrusion and distalization poses great challenge in orthodontics due to complex mechanical design and possible anatomical limits. This case report illustrates the orthodontic retreatment of a class I hyperdivergent patient by the “high-pull palatal gear” (HPPG) technique and two mandibular miniscrews. The gummy smile was corrected and the profile was successfully improved through whole arch intrusion and distalization and subsequent forward rotation of the mandible.
Keywords
Temporary skeletal anchorage devices
Hyperdivergent
Retreatment
Whole arch intrusion
Whole arch distalization

INTRODUCTION
With the wide prevalence and acceptance of orthodontic treatment, there is an increasing trend for adult patients who received orthodontics in their adolescence seeking retreatment to further improve their dental alignment and facial profile.[1] For those who already have their premolars extracted in the prior treatment, the capacity of profile improvement would be limited. It often requires orthognathic surgery combined with cosmetic genioplasty to address the underlying skeletal problem and get the most improvement of chin projection.[2]
The “high-pull palatal gear” (HPPG) technique utilizes one single miniscrew placed at the palate to achieve whole maxillary dentition intrusion and distalization on rigid archwire. The HPPG technique was named after the high-pull headgear (HPHG) since they create a similar force vector. This case report illustrates the orthodontic retreatment of a Class I hyperdivergent patient with HPPG technique and two mandibular miniscrews to achieve bimaxillary intrusion and distalization. The successful counterclockwise rotation of the upper occlusal plane in turn facilitates the forward rotation of the mandible to achieve balance between smile and facial esthetics.
CASE REPORT
A 29-year-old female patient came to the clinic and asked for an orthodontic retreatment. She had her previous orthodontic treatment 10 years ago but was still bothered by the excessive gummy smile and protrusive lips. The clinical examination showed a convex lateral profile with mentalis muscle activity on lip closure. No obvious facial asymmetry was noted. Intro-oral photos and panoramic X-ray revealed missing of all four first premolars and third molars. The canine and molar relationships were Class II on the right side and Class I on the left side. The overjet was 6 mm and overbite was 4 mm, respectively [Figures 1 and 2].

- (a-c) Pretreatment facial photos. (d-h) Pretreatment intraoral photos.

- (a) Pretreatment panoramic radiograph, (b) lateral cephalogram, and (c) cephalometric tracing.
The cephalometric analysis revealed a Class I skeletal pattern with a high mandibular plane angle (SN-MP = 37.4°). The vertical disharmony resulted in the backward rotation of the pogonion, giving the patient a more retrognathic appearance in terms of facial esthetics. The labiolingual inclination of the upper incisors was normal while the lower incisors were proclined (U1-SN = 108.5° L1-MP = 102.4°) [Figure 2, and Table 1].
| Analysis | Taiwanese norms |
Pre- treatment |
Post- treatment |
|---|---|---|---|
| Skeletal | |||
| SNA (°) | 81.5±3.5 | 78.5 | 78.5 |
| SNB (°) | 77.7±3.2 | 73.9 | 74.8 |
| ANB (°) | 4.0±1.8 | 4.6 | 3.7 |
| SN-MP (°) | 33.0±1.8 | 37.4 | 34.3 |
| LAFH (mm) | 71.4±3.7 | 70 | 67.5 |
| Wits appraisal (mm) | −1.0±1.0 | 0.89 | −0.72 |
| Dental | |||
| U1-SN (°) | 108.2±5.4 | 108.5 | 100.8 |
| L1-MP (°) | 93.7±6.3 | 102.4 | 101.1 |
| Soft tissue | |||
| U Lip-Eline (mm) | −1.1±2.2 | 4.3 | 1.2 |
| L Lip-Eline (mm) | −0.5±2.5 | 5.8 | 1.9 |
LAFH: Lower anterior facial height, SNA: Sella-Nasion to A point angle, SNB: Sella-Nasion to B point angle, ANB: A point to B point angle, SNMP: Sella-Nasion to mandibular plane angle, U1-SN: Upper incisor to Sella-Nasion angle, L1-MP: Lower incisor to mandibular plane angle, U Lip-Eline: Upper lip to Eline, L Lip-Eline: Lower lip to Eline
TREATMENT OBJECTIVES
The treatment objectives included:
Obtain well-aligned dentition with bilateral Class I canine and molar solid occlusion
Attempt retraction in the sagittal dimension to reduce lip protrusion and also decrease the vertical dental height to correct the gummy smile, relieve the muscle strain, and enhance chin projection.
TREATMENT ALTERNATIVES
To genuinely address the skeletal discrepancies, the ideal treatment plan should be a two-jaw orthognathic surgery: Maxillary Le-Fort I impaction and mandibular BSSO forward rotation in conjunction with an advancement genioplasty. Somehow the patient refused the surgical approach.
The treatment plan was then settled as bimaxillary whole arch intrusion and distalization by temporary skeletal anchorage devices (TSADs).
TREATMENT PROGRESS
0.018 slot self-ligating brackets (Clippy, Tomy Inc., Tokyo, Japan) were bonded. After initial leveling and alignment of both arches, the archwires were changed to 0.017 × 0.025 stainless steel wires in the fifth month. One palatal miniscrew (A1-P, stainless steel, 1.5 × 8 mm, Bio-Ray Biotech Instrument Co., Taipei, Taiwan) was installed at the anterior portion of T zone.[3] Intrusive distalization force was delivered from the maxillary lateral incisors. In the mandibular arch, bilateral TSADs (AbsoAnchor, PH1413-06, Dentos Inc., Daegu, South Korea) were installed between the lower second premolars and first molars to apply intrusive distalization force in the lower arch [Figure 3].

- (a) The line of force lies in front of the center of resistance of upper dentition; therefore, total intrusion and counterclockwise rotation of the upper dentition could be achieved. (b and c) Mechanical design: Intrusive distalization of upper dentition by high-pull palatal gear technique. Intrusive distalization of lower dentition by bilateral apically-positioned mini-screws. (d-h) Intraoral photos at the 8th month of active treatment. CR (T): Center of resistance of the total dentition. Purple arrow: the line of force from lateral incisors to mid-palatal screw. Red arrows: the intrusive force applied on rigid stainless archwire, resulting the counterclockwise rotation of upper occlusal plane relative to the total center of resistance CR(T). Green eyelets: the force of elastic chain applied on lateral incisors. Yellow area: the protective resin on the palatal screw to reduce irritation. Red arrow: line of force application from the laterals to mid-palatal screw. Red eyelets: the intrusive force applied by the elastic chain attached on the apically-positioned mandibular miniscrews. HPPG: High-pull palatal gear.
The gummy smile was gradually improved as treatment progressed [Figure 4]. All appliances were removed after 26 months of active treatment. Upper and lower Essix retainers were delivered. The patient was instructed to wear the retainers full-time for the first 6 months and shift to night-time wearing thereafter.
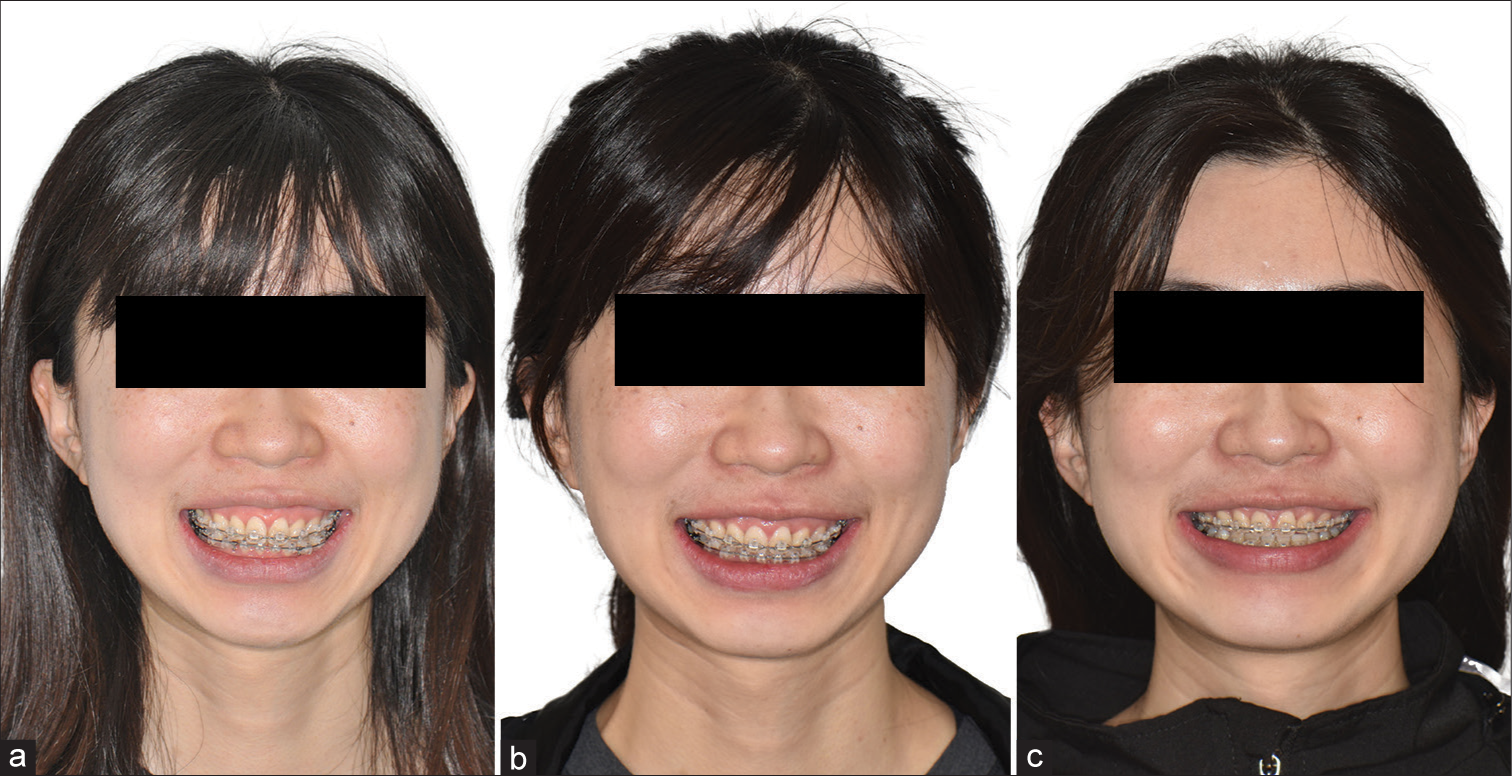
- Gummy smile was gradually improved by high-pull palatal gear technique at the (a) 5th, (b)10th and (c)18th month of active treatment.
TREATMENT RESULTS
Bilateral Class I canine and molar occlusion were established. The bimaxillary whole arch intrusion and distalization were successfully achieved. As a result, the gummy smile and mentalis strain were resolved considerably. The counterclockwise rotation of the upper occlusal plane, in turn, facilitated the forward rotation of the mandible. The patient had a pleasing smile with better chin projection after treatment [Figure 5].

- (a-c) Post-treatment facial photos. (d-h) Post-treatment intraoral photos.
No obvious root resorption was noted in the post-treatment panoramic X-ray. The mandibular plane angle was decreased by 3.1° (SN-MP from 37.4° to 34.3°), therefore improved the chin projection, and relieved the mentalis strain [Figure 6].
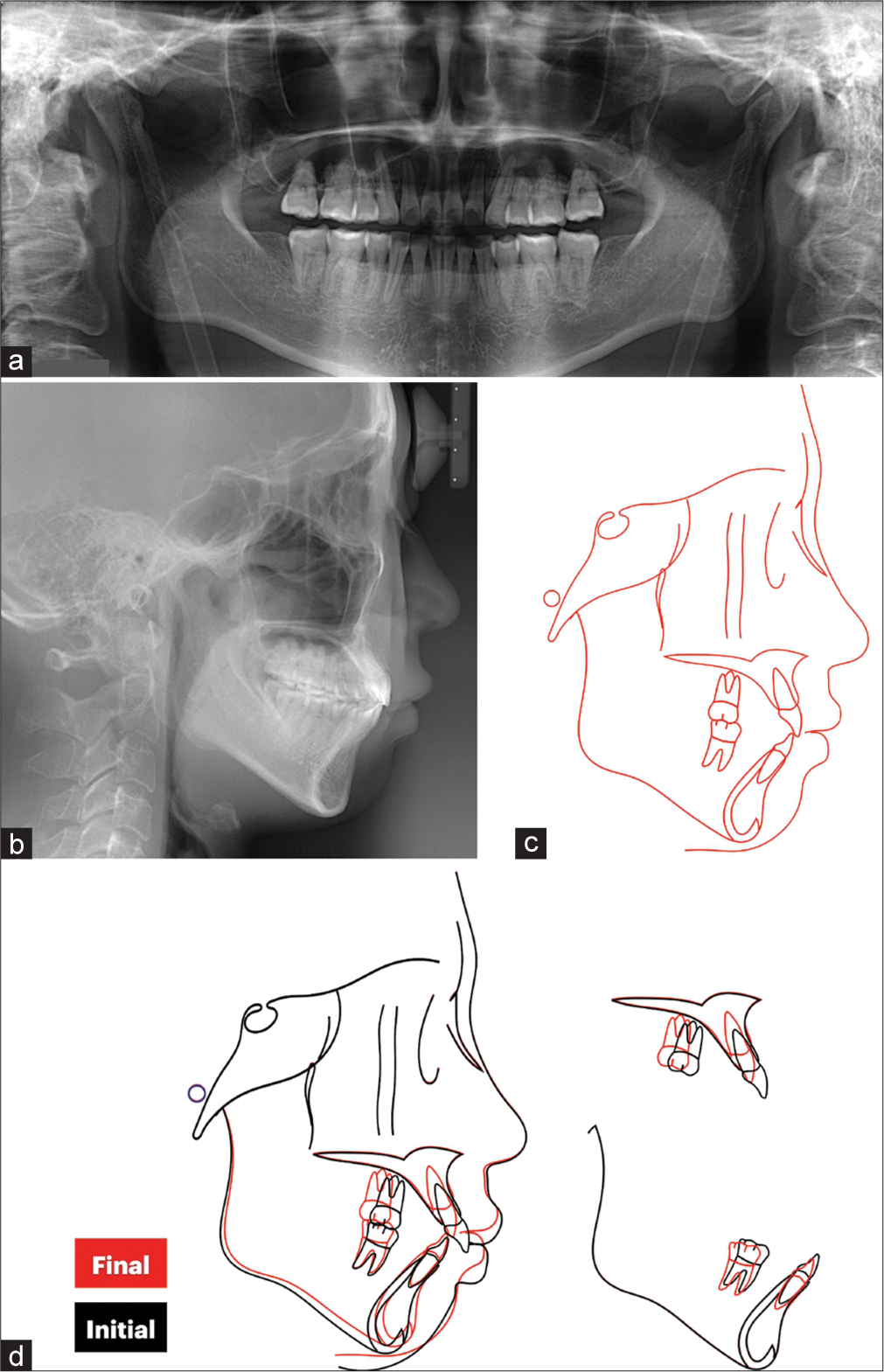
- (a) Posttreatment panoramic radiograph, (b) posttreatment lateral cephalogram, (c) cephalometric tracing and (d) cephalometric superimposition showed the intrusive distalization of both arches.
Post-retention 15 months follow-up showed stable occlusion and harmonious profile [Figure 7].

- (a-c) Post retention 15 months follow-up facial photos. (d-h) Post retention 15 months follow-up intraoral photos.
An authorization for the photo release was obtained from the patient.
DISCUSSION
For those patients who underwent extraction as part of their prior orthodontic treatment, the retreatment could be difficult in terms of profile improvement. It often requires orthognathic surgery in conjunction with advancement genioplasty to correct the gummy smile and achieve a harmonious chin profile in the hyperdivergent cases.[2] In recent years, with the rapid developments of TSADs, whole arch intrusion and distalization could be a valid alternative treatment modality.[4]
When considering the TSADs insertion sites, the buccal miniscrews could be readily used without extra attachments at the palatal side. However, when placing miniscrews at the buccal alveolus interdentally, the miniscrews could possibly contact dental roots during insertion. Besides, screws inserted on the attached gingiva or mucogingival junction often create a line of force lower than the center of resistance of the upper dentition, causing a clockwise rotation of the upper arch and deepening the overbite. The narrow inter-radicular distance also limits the capacity for distalization,[5] the miniscrews might interfere with dental roots and hinder further tooth movement. Orthodontists must identify when the miniscrews need relocation during treatment, which requires superior clinical experience and skill.
The miniscrews inserted at the infrazygomatic crest lie outside of the distalization path. Somehow the miniscrews might be inserted on non-keratinized gingiva and have a higher chance for soft-tissue inflammation or even covering of the screw head. Many times, the line of force is still below the center of resistance of the upper arch, therefore induces a clockwise rotation of the occlusal plane.[6] The interference between upper and lower dentition subsequently leads to a backward rotation of the mandible, which is unfavorable for the hyperdivergent patients. Class II elastics would cause the extrusion of upper incisors and worsen the gummy smile, steepen the occlusal plane, and increase the mentalis strain, all exacerbate the vertical disharmony [Figure 8].
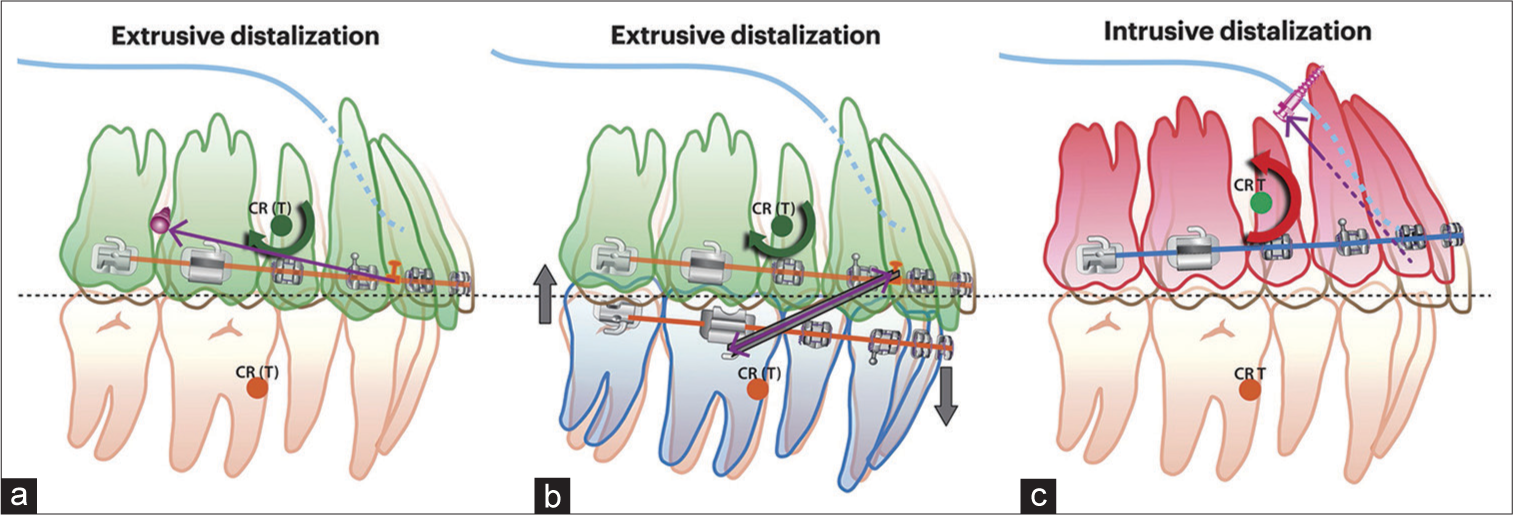
- Different vertical effect and occlusal plane change of extrusive and intrusive distalization mechanics: (a) Low-positioned buccal miniscrews: Purple arrow: line of force from short hook on archwire to low-positioned miniscrews, which is below the CR(T). Bold green circular arrow: clockwise rotational moment relative to CR(T), (b) Class II elastics: Purple arrow: line of force provided by class II elastics, which is below the CR(T) Bold green circular arrow: clockwise rotational moment relative to CR(T). The extrusion of maxillary incisors and mandibular molars worsen the gummy smile and induce mandibular backward rotation. (c) High-pull palatal gear technique: Purple dot line: line of force from lateral incisors to midpalatal screw, which is above and in front of the CR(T). Bold red circular arrow: counterclockwise rotational moment relative to CR(T). CR(T): Center of resistance of total dentition.
The HPPG technique utilizes one-single miniscrew inserted at the anterior portion of T zone.[3] The success rate of screw insertion is notably high for the premium bone quality at the anterior palate. There would be minimal risk of root contact during screw insertion and tooth movement. The simple design of the appliance allows efficient installation at the chairside without extra laboratory work and improves patient comfort.
The clinicians should carefully diagnose the etiology of gummy smile to determine the appropriate treatment modality. Common causative factors for gummy smile include altered passive eruption of the incisors, hyperactivity of the lip elevator muscles, and vertical maxillary excess. This patient had elongated upper anterior dentoalveolus and declined orthognathic surgery; therefore, the whole arch intrusion and distalization with HPPG would be a viable alternative treatment for her. The treatment planning was based on the desired upper incisor position after orthodontic treatment[7] and also considered the overbite, overjet, chin prominence, and facial proportion of each patient to determine the occlusal plane rotation. The screw position and force application point relative to the center of resistance were, then, designed accordingly. In this case, the palatal miniscrew was inserted at the anterior T zone, produced a line of force passed superiorly and anteriorly to the center of resistance of the upper arch,[8] and thus created whole maxillary dentition intrusion and distalization with a counterclockwise rotation [Figure 3]. The upper central incisors were intruded for 3.5 mm, while the upper first molars were intruded for 1 mm. This counterclockwise rotation of the upper occlusal plane facilitated deep bite and gummy smile correction, meanwhile, creating the occlusal clearance for mandibular forward rotation to improve the facial profile.
The intrusive distalization should be performed with light force on a rigid archwire to ensure the teeth are moving in the alveolar bone housing without torque loss. 10° of buccal crown torque could be incorporated into the archwire to control the buccolingual inclination for those cases with straight incisors to begin with.
The whole arch intrusive distalization of the mandibular dentition is also essential to prevent interincisal interference and allow forward rotation of the mandible. The clinicians should thoroughly evaluate the proportion of upper and lower incisors intrusion to preserve proper upper incisal show after the gummy smile is resolved.
The factors associated with external root resorption during orthodontic treatment include root morphology, root proximity to the buccal or lingual cortical bone, the patients’ genetic features, the magnitude of orthodontic force, the treatment duration, and the amount of apical displacement. In this retreatment case, although attempting a large amount of vertical movement of incisors, the whole arch intrusion and distalization were performed with light force and ideal incisal torque to ensure the tooth movement within the cancellous bone. The en-masse tooth movement with a straight-forward force system also facilitates the completion of treatment within reasonable treatment duration. As a result, there was no obvious root resorption noted on the post-treatment radiograph. However, we should still be cautious with the anatomical limits of the palatal cortex and incisive canal while striking for a large amount of intrusive distalization of the dentition.[9]
Kang et al. researched the stability of vertical dimension following total arch intrusion with buccal interdental dual miniscrews.[10] The authors found a 40.69% relapse in the vertical movement of anterior teeth (U1-PP) and 30.00% relapse of the anterior facial height (AFH) after maxillary total arch intrusion. No significant relapse of the distance between maxillary molars and the palatal plane (U6-PP) was noted in the retention period. Although the study revealed some significant relapse of the vertical variables, the amount of relapse was relatively small [mandibular plane angle (MPA) +0.73°, AFH +0.81 mm, upper incisor to palatal plane (U1-PP) +0.83 mm], which implied little clinical impact on the patients’ occlusion and profile.
Despite the optimal mechanical design, we should still respect the limitations of biological boundaries regarding distalization.[11] The patient was fully informed about the pros and cons of the nonsurgical treatment plan and understood the limitations of this treatment alternative. Cosmetic chin enhancement procedures such as injectable fillers or chin implants could be considered to finalize the facial balance.[12] In this case, the patient was already satisfied with the orthodontic treatment results; therefore, no further cosmetic procedure was done.
Both dental protrusion and hyperdivergent facial pattern cause the imbalance between the hard-tissue and soft-tissue envelope. If we ignore the vertical disharmony and attempt to solve the mentalis strain solely by retraction of the dentition, it would be difficult due to the limited retraction capacity left in this non-extraction treatment. Even if we succeed, the incisors could be over-retracted with compromised palatal alveolar bone support[13] and insufficient tooth show. In this case, the majority of profile improvement comes from the forward rotation of the mandible. The combined intrusion and distalization movement and the counterclockwise rotation of the occlusal plane led to the best balance between the facial profile and upper incisal display.
CONCLUSION
Bimaxillary whole arch intrusion and distalization with HPPG technique and mandibular TSADs could be a valid treatment alternative for retreating hyper-divergent patients.
Ethical approval
This is a pure clinical case report, the Institutional Review Board approval is not required.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- Adult orthodontic retreatment: A survey of patient profiles and original treatment failings. Am J Orthod Dentofacial Orthop. 2020;158:371-82.
- [CrossRef] [PubMed] [Google Scholar]
- Orthodontic retreatment: Positive effects on the patient's self-esteem and quality of life. Dental Press J Orthod. 2021;26:e21bbo5.
- [CrossRef] [PubMed] [Google Scholar]
- The T-zone: Median vs. paramedian insertion of palatal mini-implants. J Clin Orthod. 2016;50:543-51.
- [Google Scholar]
- Orthodontic retreatment for vertical control in a patient with skeletal Class II long face. Am J Orthod Dentofacial Orthop Clin. 2023;3:30-42.
- [CrossRef] [Google Scholar]
- Simulation of miniscrew-root distance available for molar distalization depending on the miniscrew insertion angle and vertical facial type. PLoS One. 2020;15:e0239759.
- [CrossRef] [PubMed] [Google Scholar]
- Total arch maxillary distalization using infrazygomatic crest miniscrews in the treatment of Class II malocclusion: A prospective study. Angle Orthod. 2023;93:41-8.
- [CrossRef] [PubMed] [Google Scholar]
- Maxillary incisor position-based orthodontic treatment with miniscrews. Semin Orthod. 2022;28:123-35.
- [CrossRef] [Google Scholar]
- Finite-element investigation of the center of resistance of the maxillary dentition. Korean J Orthod. 2009;39:83-94.
- [CrossRef] [Google Scholar]
- Approximation and contact of the maxillary central incisor roots with the incisive canal after maximum retraction with temporary anchorage devices: Report of 2 patients. Am J Orthod Dentofacial Orthop. 2015;148:493-502.
- [CrossRef] [PubMed] [Google Scholar]
- Stability of vertical dimension following total arch intrusion. BMC Oral Health. 2023;23:164.
- [CrossRef] [PubMed] [Google Scholar]
- Mandibular posterior anatomic limit for molar distalization. Am J Orthod Dentofacial Orthop. 2014;146:190-7.
- [CrossRef] [PubMed] [Google Scholar]
- Chin augmentation techniques: A systematic review. Plast Reconstr Surg. 2023;151:758-71.
- [CrossRef] [PubMed] [Google Scholar]
- The anterior alveolus: Its importance in limiting orthodontic treatment and its influence on the occurrence of iatrogenic sequelae. Angle Orthod. 1996;66:95-109.
- [Google Scholar]




