

Translate this page into:
Republication: Conservative Management of Skeletal Class II Malocclusion with Gummy Smile, Deep Bite, and a Palatally Impacted Maxillary Canine
Address for correspondence: Prof. W. Eugene Roberts, 8260 Skipjack Drive, Indianapolis, IN 46236. E-mail: werobert@iu.edu
This article was originally published by Wolters Kluwer and was migrated to Scientific Scholar after the change of Publisher.
Abstract
A 21-year-old female presented with chief complaints of crooked teeth, canine impaction, deep bite, and “gummy smile” (excessive maxillary gingival exposure when smiling). Increased facial convexity (15.5°), increased lower facial height (56%), and incompetent protrusive lips (E-line to upper left 2 mm, E-line to lower left 2 mm) were associated with a severe Class II malocclusion (nearly a full cusp bilaterally). There was 7.5 mm of overjet, 100% anterior deepbite, and a left posterior buccal crossbite. Cephalometrics revealed a skeletal discrepancy due to a protrusive maxilla and a retrusive mandible (SNA 85°, SNB 78°, and ANB 7°). Cone-beam computed tomography imaging revealed a palatally impacted right maxillary canine (UR3) near to the adjacent lateral incisor (UR2). The retained right primary canine (URc) was extracted. A simplified open-window technique was utilized to surgically expose its impacted successor. A maxillary anterior mini-screw provided anchorage to align the UR3 in its correct anatomical position. Nonextraction treatment with a passive self-ligating fixed appliance was indicated to align and level both arches. Anchorage provided by infrazygomatic crest bone screws, and maxillary anterior miniscrews were used for the correction of Class II malocclusion and gummy smile. To achieve more esthetic crown lengths in the maxillary anterior segment, gingivectomy was performed with a diode laser 2 months after fixed appliances were removed. This challenging skeletal Class II malocclusion with a Discrepancy Index of 38 was treated in 32 months to excellent outcomes: Cast-radiograph evaluation score of 25 and an pink and white dental esthetic score of 2. All facial and dental corrections were stable at the 6 months follow-up evaluation (Int J Orthod Implantol 2017;48:24-46).
Republished with permission from: Ariel Wong, Chang CH, Roberts WE. Conservative Management of Skeletal Class II Malocclusion with Gummy Smile, Deep Bite, and a Palatally Impacted Maxillary Canine. Int J Orthod Implantol 2017;48:24-46.
Keywords
Arch retraction
bite-turbos
bone screws
class II malocclusion
deepbite
extra-alveolar
gummy smile
infrazygomatic crest
laser gingivectomy
palatal canine impaction
self-ligating brackets
temporary anchorage devices

Introduction
Complex malocclusions require careful analysis to determine the optimal treatment plan for correcting the patient’s chief complaints, consistent with long-term stability. Unesthetic debilitating malocclusions that previously required orthognathic surgery can now be managed conservatively with extra-alveolar bone screw anchorage.
History and Etiology
A 21-year-old female patient presented for orthodontic consultation [Figure 1]. Her chief complaints were crooked teeth, canine impaction, deep bite, and gummy smile. Facial evaluation showed a convex profile, protrusive lips, increased lower facial height, hyperactive mentalis muscle (“golf ball chin” on lip closure), and a retrusive mandible [Figure 1]. A full smile revealed an asymmetric, excessive gingival display (“gummy smile”) [Figure 2]. The casts showed a full-cusp Class II malocclusion of the right first molars and almost a full cusp Class II on the left [Figure 3]. Overall, the buccal segments were severe Class II (6 mm) bilaterally. Intraoral examination revealed a retained right maxillary deciduous canine (URc), ∼4 mm of interdental spaces in the maxillary anterior segment, buccal crossbite of the left premolars [Figure 3], deep bite, and 7.5 mm of overjet [Figure 4]. The upper dental midline was coincident with the facial midline; however, the lower dental midline was shifted 1 mm to the right of the other two midlines.

- Pretreatment facial and intraoral photographs

- Gummy smile, asymmetrical gingival display, and occlusal canting are documented in a frontal photograph
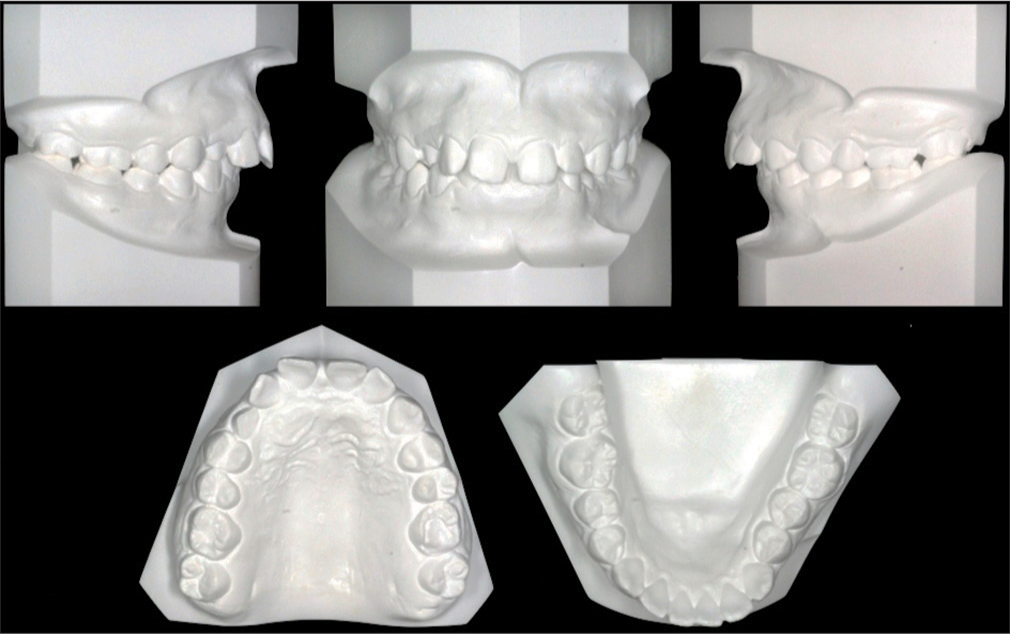
- Pretreatment dental models (casts)

- Inferior (left) and lateral (right) intraoral views show Impinging (100%) anterior deep bite and large overjet (7.5 mm)
Radiographic documentation is lateral cephalometric [Figure 5] and panoramic radiographs [Figure 6]. Both panoramic [Figure 6] and cone-beam computed tomography (CBCT) imaging [Figure 7] revealed a palatally impacted right permanent canine (UR3) and three developing third molars (UL8, LL8 and LR8); the UR8 was missing. There was no additional contributing medical or dental history. Cephalometric measurements are presented in Table 1, and diagnostic details are outlined below.
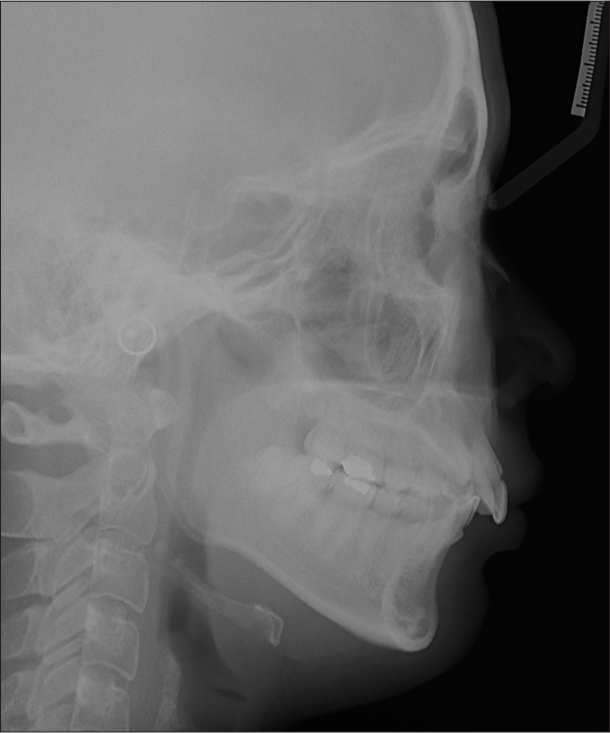
- Pretreatment lateral cephalometric radiograph
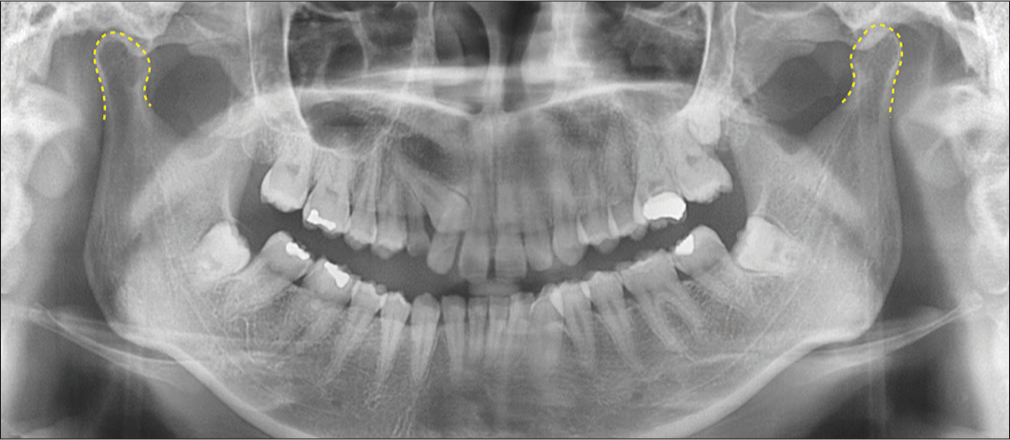
- Pretreatment panoramic radiograph shows both condylar heads outlined in yellow
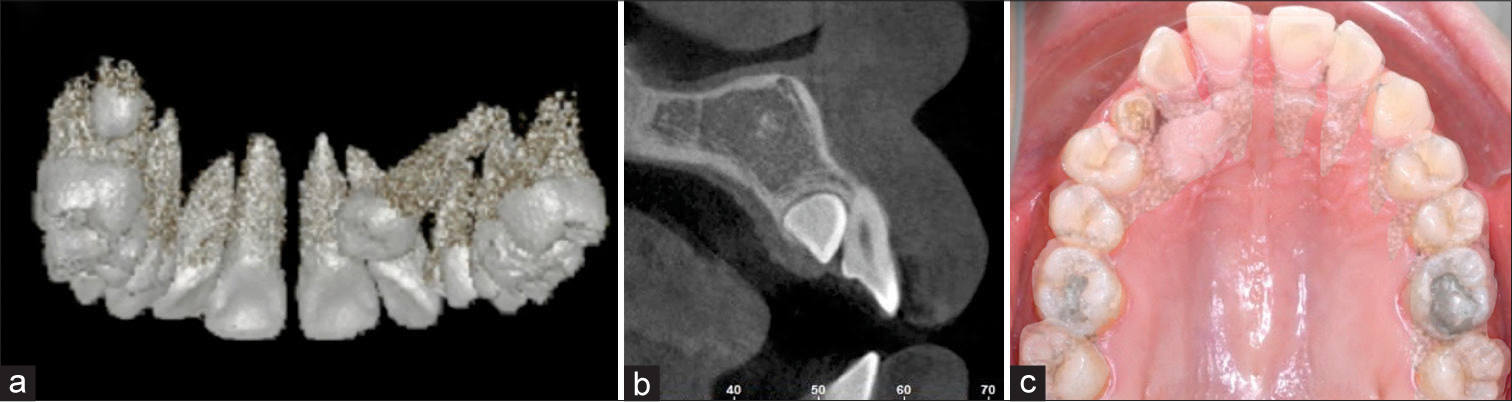
- (a) Three-dimensional image of the maxillary dentition documents the relative position of the impacted canine. (b) A sagittal cut through the UR2 region of a cone-beam computed tomography image shows a cross-section through the cervical region of the impacted UR3. (c) A cone-beam computed tomography image of the maxillary arch is superimposed on an occlusal intraoral photograph to reveal the position of the impacted canine
| Pre-TX | Post-TX | Difference | |
|---|---|---|---|
| Skeletal analysis | |||
| SNA° (82°) | 85° | 84° | 1° |
| SNB° (80°) | 78° | 77° | 1° |
| ANB° (2°) | 7° | 7° | 0° |
| SN-MP° (32°) | 39° | 41° | 2° |
| FMA° (25°) | 32° | 34° | 2° |
| Dental analysis | |||
| U1 to NA mm (4 mm) | 1 mm | 4 mm | 3 mm |
| U1 to SN° (104°) | 96° | 90° | 6° |
| L1 to NB mm (4 mm) | 6 mm | 6 mm | 0 mm |
| L1 to MP° (90°) | 102° | 97° | 5° |
| Facial analysis | |||
| E-line UL (−1 mm) | 2 mm | 2 mm | 0 mm |
| E-line LL (0 mm) | 2 mm | 1 mm | 1 mm |
| %FH N-ANS-Me (53%±3%) | 56% | 57% | 1% |
| Convexity G-Sn-Pg’ (13°) | 15.5° | 15.5° | 0° |
Diagnosis
Skeletal
Class II relationship due to the maxillary protrusion and relative mandibular retrusion (SNA 85°, SNB 78°, ANB 7°)
High mandibular plane angle (SN-MP 39°, FMA 32°).
Dental
Class II molar relationships: near full cusp bilaterally (6 mm)
Overjet of 7.5 mm
100% impinging deepbite
Retrusive upper incisors (U1 to NA 1 mm) with decreased axial inclination (U1 to SN 96°)
Increased axial inclination the lower incisors (L1 to MP 102°).
Facial
Convex profile (15.5°)
Protrusive lips (2 mm/2 mm to the E-line)
Hyperactive mentalis with the lips closed.
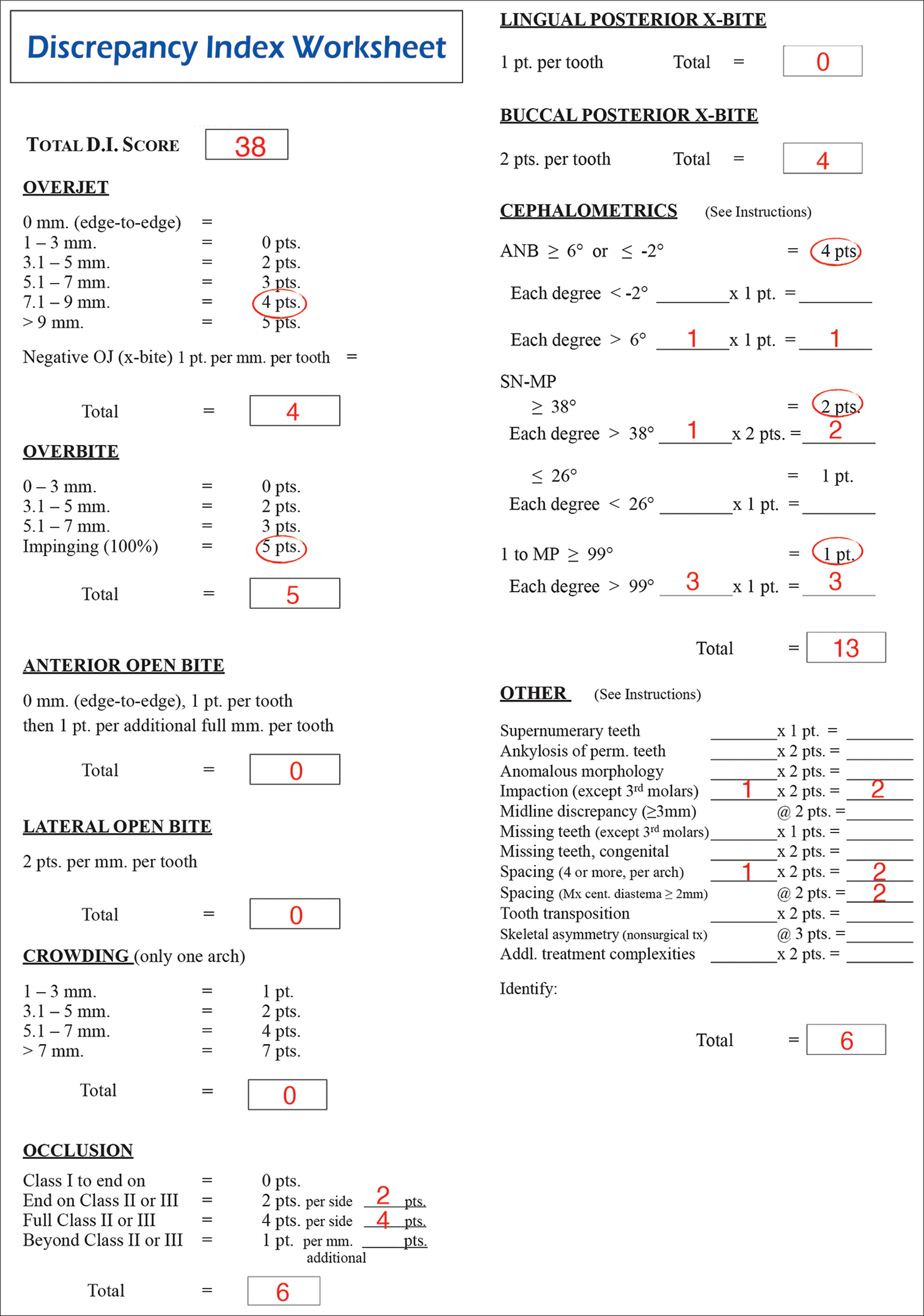
The American Board of Orthodontics (ABO) Discrepancy Index (DI)[1] was 38 points as shown in the subsequent worksheet in worksheet 1 (p12) at the end of this report.
Treatment Objectives
Maxilla (all three planes):
A-P: Retract
Vertical: Maintain
Transverse: Maintain.
Mandible (all three planes):
A-P: Maintain
Vertical: Maintain
Transverse: Maintain.
Maxillary dentition
A-P: Retract the maxillary anterior segment
Vertical: Intrude the maxillary anterior segment
Inter-molar/Inter-canine Width: Expand to properly occlude with the lower dentition.
Mandibular dentition
A-P: Maintain
Vertical: Maintain
Intermolar/Intercanine Width: Upright molars to increase intermolar width
Facial Esthetics: Retract protrusive upper and lower lips.
Treatment Alternatives
First option
Extract three teeth (retained URc, impacted UR3, and UL4). Move the UR4 into the UR3 position. Disadvantages for this treatment option include compromised dental esthetics and ipsilateral loss of canine guidance.
Second option
Extract two teeth (retained URc and impacted UR3), followed by prosthetic restoration with a fixed partial denture or an implant-supported prosthesis. The disadvantages for this approach include cost, loss of tooth structure for conventional prosthesis, implant failure if bone fixtures are used, and a potential compromise in both esthetics and function with either prosthetic option.
Third option
Extract the retained URc and align the dentition with a fixed passive self-ligating (PSL) appliance. Expose the impacted UR3 with an open window technique. Allow the impaction to erupt spontaneously,[2] and then align the entire arch with full fixed orthodontics. Place maxillary anterior miniscrews to intrude the upper incisors for correction of the deep bite. Install maxillary posterior bone screws bilaterally in the infrazygomatic crests (IZC) to provide anchorage for retraction of the entire maxillary dentition. The perceived disadvantages for this option include increased treatment time and potential root resorption of UR2. After weighing the pros and cons, the patient preferred the least invasive, most conservative approach (Option 3) despite the treatment risks. On completion of active treatment, a gingivectomy is indicated on the labial surface of the maxillary anterior segment. Assuming there is adequate biologic width of the gingival attachment, as defined later in this report, a gingivectomy with a diode laser is indicated to increase the crown length of the dentition in the maxillary anterior segment (the esthetic zone).
Treatment Progress
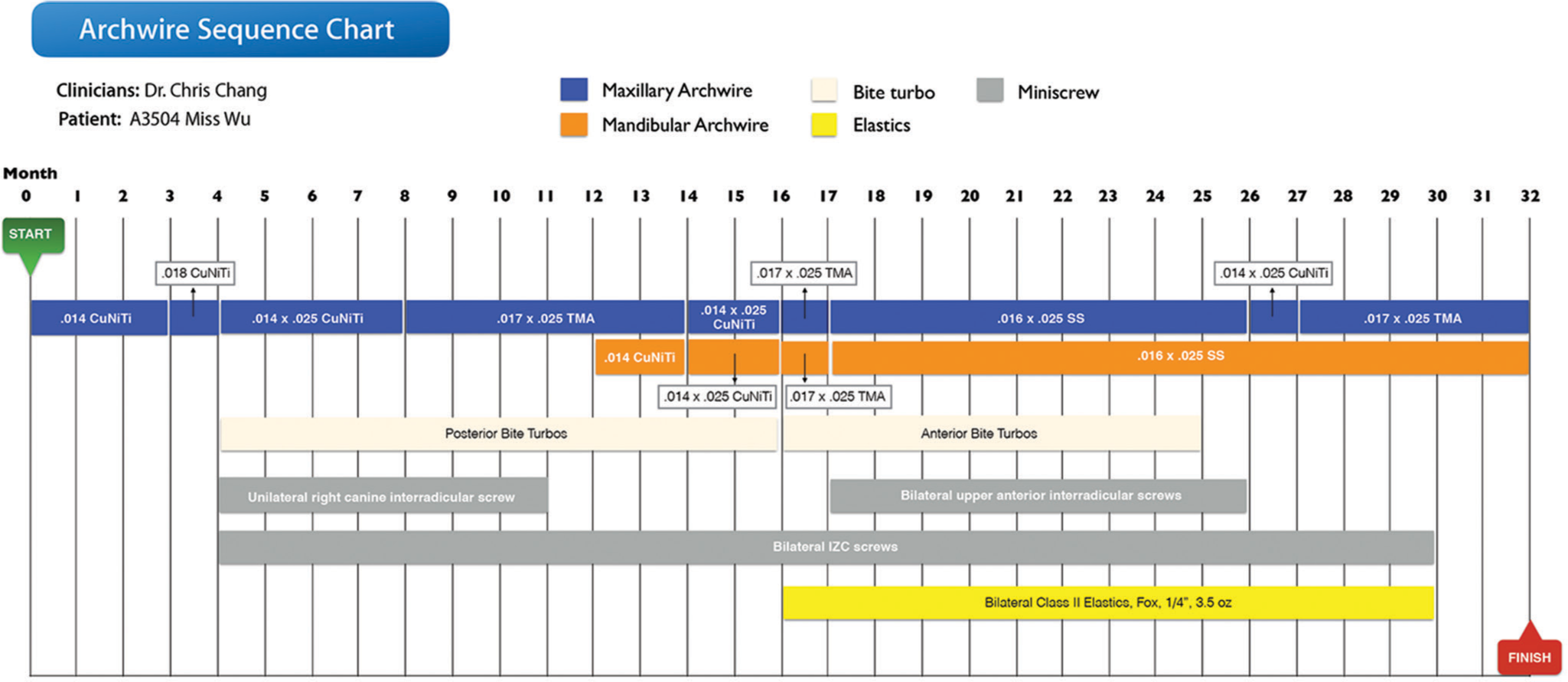
Following extraction of the UR3, a full fixed appliance with 0.022-in slot Damon Q® PSL brackets (Ormco, Glendora, CA) was installed on the maxillary arch. The upper archwire sequence was: 0.014-in CuNiTi, 0.018-in CuNiTi, 0.014 × 0.025-in CuNiTi, 0.017 × 0.025-in TMA, and 0.016 × 0.025-in SS.
In the 2nd month of treatment, surgical exposure of the impacted UR3 was completed using a simplified open window technique [Figure 8]. CBCT imaging was required for precise localization of the impaction relative to adjacent teeth [Figure 7]. Local anesthesia was administered at the surgical site, and the location of the crown was marked with a sharp surgical explorer [Figure 8]. A dental electrosurgical unit was used to remove the soft tissue covering the crown of the UR3, while carefully avoiding the greater palatine artery. Uncovering a palatally impacted UR3 in the maxillary anterior area has the potential for severe bleeding if the adjacent artery is severed. The use of an electrosurgical unit for the uncovering procedure provides the surgeon with the means to rapidly coagulate the bleeding artery if it is accidentally severed.
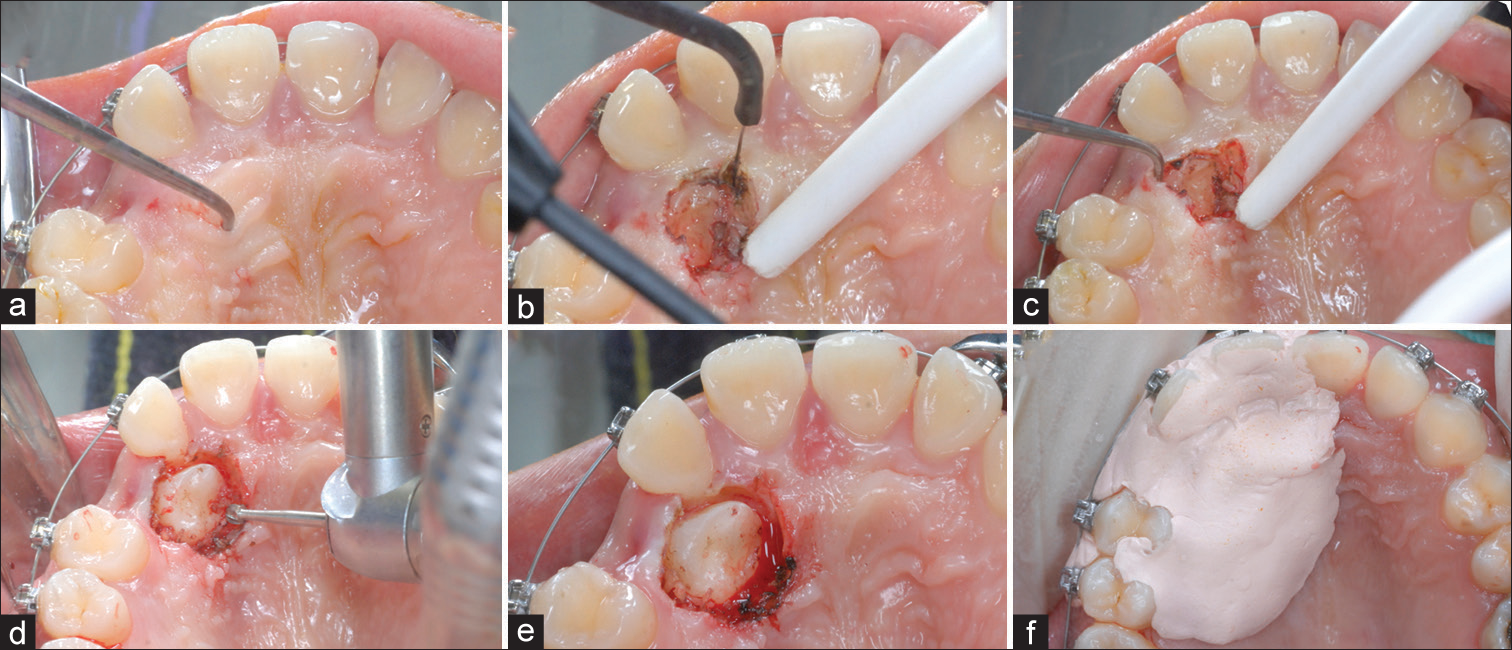
- (a) The simplified open window technique begins with precise location of the crown of the impaction by sounding through the soft tissue to detect enamel. (b) The palatal soft tissue covering the crown is removed with electrosurgery. (c) An explorer is used to penetrate the overlying cervical bone to estimate the location of the cementoenamel junction. (d) Bone covering the crown is carefully removed with a round bur in a high-speed handpiece down to the level of the cementoenamel junction. (e) Canine crown is exposed without severing the greater palatine artery or damaging the tooth. (f) COE-PAK® periodontal dressing is placed for patient comfort and to prevent soft tissue from recovering the exposed crown
An explorer was used to determine the position of the UR3 crown. Since spontaneous tooth eruption is facilitated by removing bone apical to the height of contour of the crown,[2] a high-speed handpiece with a carbide round bur, and irrigation was used to remove the overlying bone down to the level of the cementoenamel junction (CEJ). To insure patient comfort and control hyperplastic soft tissue, COE-PAK® periodontal dressing was placed over the wound.
In the 3rd month, an open coil spring was installed to create space for the impacted canine [Figure 9]. Approximately 2 months after the surgical procedure, a button was bonded on the UR3. At the same appointment, a 2 mm × 12 mm bone screw (OrthoBoneScrew®, Newton’s A Ltd, Hsinchu City, Taiwan) was inserted on the labial aspect of the alveolar ridge position. The latter anchored an elastic power chain that was attached to the button bonded on the UR3 to apply traction for guiding the canine laterally [Figure 10]. Additional 2 mm × 12 mm bone screws were placed in each IZC for bilateral extra-alveolar (E-A) anchorage [Figure 10]. Furthermore, glass ionomer bite turbos (BTs) were bonded on the lower first molars to open the bite for correction of the left posterior crossbite tendency [Figure 11].

- In the 3rd month of treatment, an open-coil spring was placed between the right maxillary lateral incisor and first premolar to create space to align the impacted canine

- (a) In the 4th month, a miniscrew is placed between the 1st premolar and canine position and loaded with 150 g-force (cN) of traction to move the impacted canine into its correct anatomical position. (b) A right lateral intraoral radiograph shows the mechanism for retraction of the right buccal segment as the palatally displaced canine is moved into the arch. (c) A left lateral view reveals symmetric mechanics to retract the left buccal segments with 280 g-force (cN) per side

- In the 12th month of treatment brackets are bonded to the maxillary right canine (left) and also on the entire lower arch (center). BTs are noted on the occlusal surfaces of the mandibular first molars (right)
Eleven months into treatment, the miniscrew providing anchorage for labial movement of the UR3 was removed, and 1 month later, (12 months into treatment) brackets were bonded to the UR3 and the entire lower dentition [Figure 11]. The lower archwire sequence for was 0.014-in CuNiTi, 0.014 × 0.025-in CuNiTi, 0.017 × 0.025-in TMA, and 0.016 × 0.025-in SS.
In the 16th month, two anterior BTs were bonded on the maxillary central incisors to aid in correction of the 100% deepbite. Class II elastics (Fox 1/4-in, 3.5-oz) were applied bilaterally to correct the Class II molar and canine relationships.
In the 17th month, two 1.5 mm × 8 mm miniscrews (Newton’s A Ltd, Hsinchu City, Taiwan) were placed between the roots of the upper central and lateral incisors for anchorage to prevent extrusion of the maxillary anterior segment when Class II elastics were applied [Figure 12]. In the 26th month, the anterior miniscrews were removed. In the 30th month, interproximal reduction was performed to address the black triangles noted between the maxillary anterior teeth.
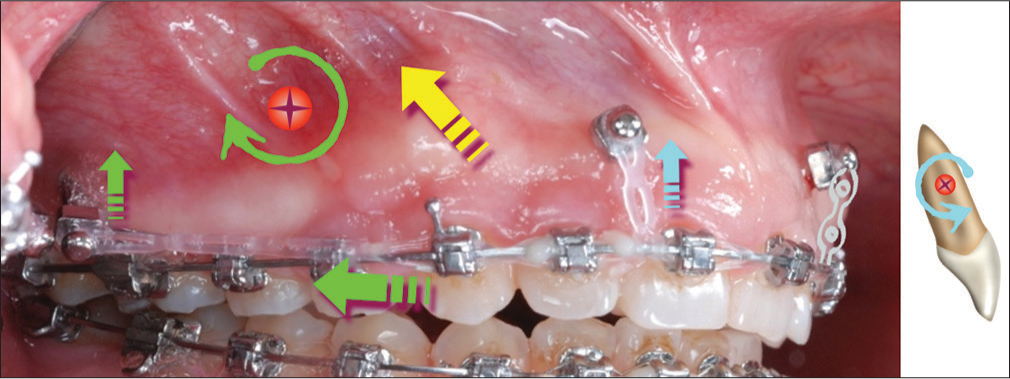
- Based on a presumed CR for the maxillary arch (red circle with a cross), the chain of elastics from the infrazygomatic crest bone screw to the cuspid bracket has distal and vertical components (straight green arrows) that produce a clockwise moment around the CR. The maxillary anterior miniscrew anchors an intrusive force (blue arrow) that creates a counterclockwise moment (blue curved arrow) tending to flare the maxillary incisors. The presumed resultant for all the applied loads is the yellow arrow. CR – Center of resistance
After 32 months of active treatment, all fixed appliances were removed. Upper 2–2 fixed retainers and upper and lower clear removable retainers were delivered. The patient was instructed to wear the retainers full time for the first 6 months and nights only thereafter. Home care and retainer maintenance instructions were provided. Two months into retention, a diode laser was used for a maxillary midline labial frenectomy, as well as for esthetic crown lengthening of the teeth in the maxillary anterior segment [Figure 13].
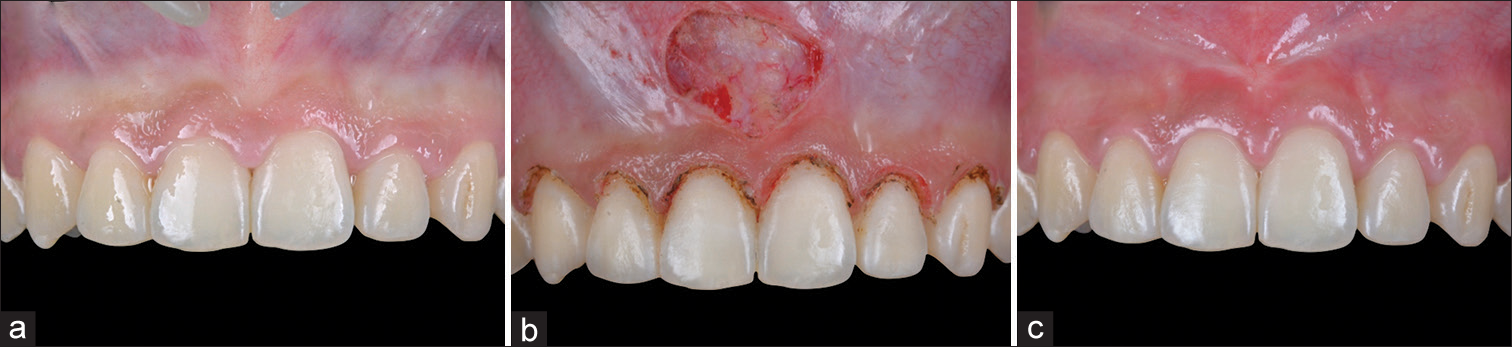
- (a) Preoperative photograph shows the irregular gingival margins and clinical crown lengths in the maxillary anterior esthetic zone. There is also a low attachment of the maxillary midline frenum. (b) Image taken immediately after diode laser gingivectomy and frenectomy which was performed 2 months into active treatment. (c) Follow-up 1 month later shows esthetically pleasing tooth proportions and gingival contours, as well as an apical migration of the revised frenum attachment
Treatment Results
Optimal results were obtained through interdisciplinary treatment with surgical exposure of the UR3 and the use of a passive self-ligating bracket system for alignment [Figure 14]. The ABO Cast-Radiograph Evaluation (CRE)[3] score was 25, which was 25 (Worksheet 2, p13), documents an excellent result for a severe malocclusion with a DI of 38 points. The major residual discrepancies scored for the CRE included marginal ridges (4 points), buccolingual inclinations (7 points), and occlusal relationships (10 points). Comparison of the before [Figures 1-7] and after [Figures 14-18] treatment records revealed a dramatic improvement in facial form and dental alignment. Posttreatment radiographic results are documented in the cephalometric and panoramic radiographs [Figures 16 and 17]. Dentoalveolar changes are shown in the superimposition of cephalometric tracings before and after treatment [Figure 18]. Posttreatment TMJ radiographs in the opened and closed positions show symmetrical and well-positioned condylar heads of the mandible [Figure 19]. Lip strain was improved dramatically; however, the soft-tissue profile of the upper lip did not follow the hard tissue in a 1:1 manner as the maxilla was retracted, so the patient’s protrusive lip profile was not completely corrected. Overall, the posttreatment photographs show optimal correction of the palatally impacted canine, deep bite, posterior buccal crossbite, gummy smile, and lip strain. The dental esthetic result was excellent, with a score of 2 points (Worksheet 3, p14). The patient was well satisfied with the result.

- Posttreatment facial and intraoral photographs

- Posttreatment dental models (casts)

- Posttreatment panoramic radiograph

- Posttreatment lateral cephalometric radiograph
![Superimposed cephalometric tracings showing dentofacial changes resulting from 32 months of active treatment (red) compared to the pretreatment (black). Note that the maxilla and particularly the maxillary incisors did not move as expected in the presumed loading diagram [Figure 12]](/content/9/2018/8/3/img/APOS-8-146-g020.png)
- Superimposed cephalometric tracings showing dentofacial changes resulting from 32 months of active treatment (red) compared to the pretreatment (black). Note that the maxilla and particularly the maxillary incisors did not move as expected in the presumed loading diagram [Figure 12]

- Posttreatment temporomandibular joint radiographs show that mandibular contours and articular relationships are within normal limits for both on the right and left sides. The open and closed positions for the right temporomandibular joint are shown in the two images on the left side, and the same relationships for the left temporomandibular joint are shown on the right side of the illustration
Discussion
Palatally impacted maxillary canines
After third molars, maxillary canines are the second most commonly impacted teeth, affecting approximately 2% of the population.[4] Two-thirds of maxillary canine impactions are palatal, and the remaining third are transalveolar or labial to the roots of the adjacent teeth.[5,6] The etiology for the location of palatally impacted maxillary canines is unknown;[7] however, both guidance and genetic theories have been proposed.[8,9] The guidance theory holds that the lateral incisor root serves as a guide for canine eruption, so a missing lateral incisor or deformed root interferes with the normal path of eruption. The genetic theory proposes an inherent predisposition to palatally impacted maxillary canines.[10] There are multiple sequelae associated with canine impactions including: (1) migration of adjacent teeth, (2) internal or external root resorption of the impaction and/or adjacent teeth, (3) cyst formation, (4) infection, and (5) referred pain.[11]
The maxillary canines are important keystones for optimal dental esthetics and function,[12] so their proper eruption and alignment are a high priority. Proper diagnosis is critical for efficient surgical and orthodontic management of eruption anomalies. CBCT is a precise method for three-dimensional (3D) localization of an unerupted canine.[13] Without 3D imaging, it is difficult to plan an efficient and relatively atraumatic uncovering of an impaction. CBCT imaging is also useful for planning the orthodontic mechanics to recover the canine and align it in the arch.
There are two methods for managing palatal impactions – preventative and surgical.[5,14] Prevention with interceptive treatment is preferable if the problem is diagnosed at an early age. This approach for an unerupted maxillary canine involves extracting the deciduous canine, and then, orthodontically opening the space between the maxillary permanent lateral incisor and the primary first molar or permanent first premolar. Ericson and Kurol[5] reported that removing the maxillary deciduous canine before 11 years of age has a differential effect on the normal eruption of the succedaneous canine. If the radiographic image of the canine crown is located distal to the midline of the lateral incisor root, 91% of the potentially impacted canines erupt normally [Figure 20]. However, the success rate decreases to 64% if the canine crown is located mesial to the midline of the lateral incisor root. Timely extraction of the deciduous canine is very effective for enhancing the eruptive potential of a canine, with a deviated path of eruption; however, the space opening must be carefully managed to avoid root resorption if the unerupted canine is near the roots of the adjacent lateral incisors and/or premolars.[15]
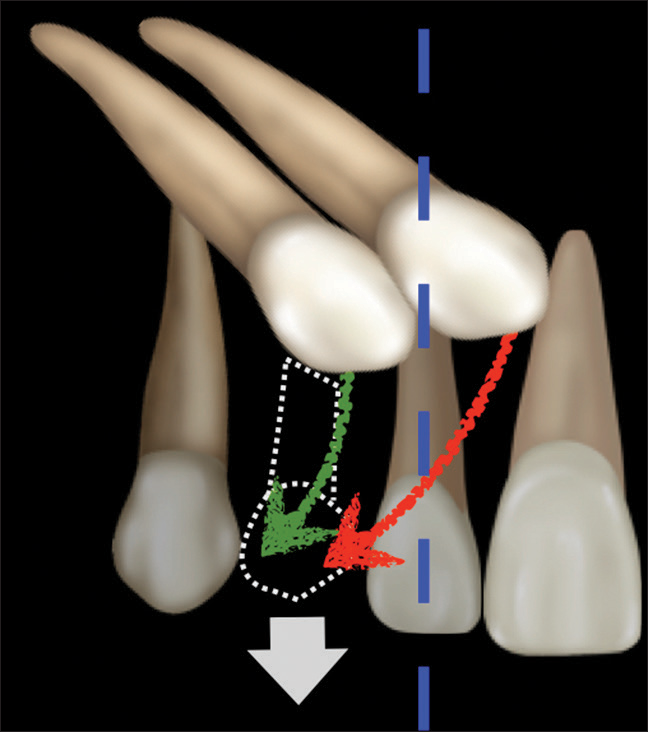
- Illustration of the concept proposed by Ericsson and Kurol (1988) for prevention of maxillary permanent canine impaction by the timely extraction of the retained deciduous canine (outline dotted in white) and space opening if needed to accommodate the erupting canine. The probable success of the procedure depends on the sagittal position of the unerupted canine relative to the midline of the maxillary canine in a two-dimensional radiograph
If prevention is not feasible, or the procedure fails to prevent the impaction, the most desirable approach is surgical exposure of the canine in combination with orthodontic treatment.[14] This type of interdisciplinary treatment requires careful communication between the orthodontist, surgeon, and patient. Kokich[2] described several advantages of preorthodontic uncovering and spontaneous eruption of the palatally impacted canine, when compared to the closed eruption technique. Removing the relatively thick palatal mucosa and bone covering the impacted canine allows for more predictable spontaneous eruption. However, in young adult patients, the passive pre-orthodontic eruption process requires almost a year, and the procedure is less predictable in adolescent patients.[14]
For the present patient, miniscrew-guided eruption of the impacted canine was performed in conjunction with surgical uncovering and orthodontic treatment [Figure 21]. After exposing the impacted canine using a simplified open-window technique, the previously impacted tooth extruded 2-3 mm in 2 months. A miniscrew was placed on the labial surface for anchorage to guide the movement of the canine into the arch-form. As palatal impactions are moved facially, gingival accumulation on the labial surface is common and may result in an unesthetic short clinical crown. The excess gingival tissue is easily removed with a diode laser before bracket placement.[16]
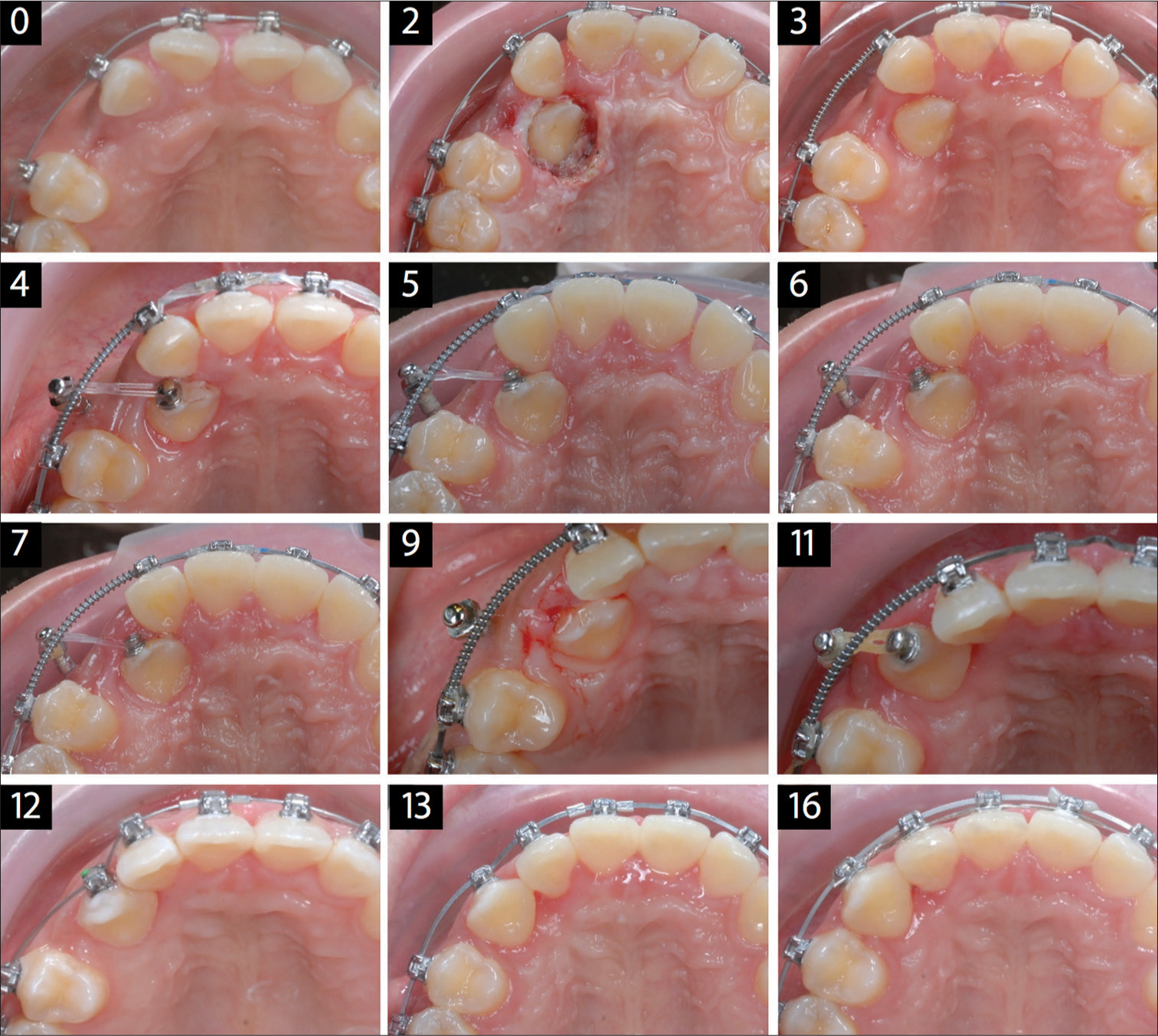
- The progression for the recovery and alignment of the palatally impacted right maxillary canine is shown in a series of occlusal photographs taken at monthly intervals from the start of treatment at zero months to completion of the initial alignment at 16 months
Efficient management of impacted maxillary canines requires a proper diagnosis and thorough understanding of anchorage demands for proper alignment. Becker et al.[17] analyzed a sample of 37 impacted maxillary canines and found that the most common reasons for failure to recover an impaction were related to two diagnostic deficiencies: (1) inaccurate assessment of the location and orientation of the impaction, and (2) failure to understand the anchorage demands for proper alignment.[17] For the present patient, the CBCT image was used to plan the surgical uncovering and miniscrew anchorage. This approach resulted in ideal functional and esthetic alignment without periodontal or esthetic compromise.
Gummy smile
The ideal amount of gingival display when smiling is around 1–2 mm.[18] Excessive maxillary gingival exposure is commonly referred to as “gummy smile.” The problem may be generalized or localized and has multiple etiologies.[19,20] Extraoral factors include as follows: (1) short and/or hypermobile upper lip, (2) maxillary anterior dentoalveolar extrusion, and (3) vertical maxillary excess. Intraoral manifestations include gingival hypertrophy and altered passive eruption (APE).
APE occurs when the gums do not physiologically recede following active tooth eruption. Coslet’s[21] classification of APE is based on the width of attached keratinized gingiva and the location of the osseous crest in relation to the CEJ. There are four classifications of APE: Type I Subgroup A, Type I Subgroup B, Type II Subgroup A, and Type II Subgroup B. In all four groups, the free gingival margin is located occlusal to the CEJ. Classification of APE is helpful in determining subsequent treatment,[22] and a summary can be shown in Table 2.
 |
 |
 |
 |
|
|---|---|---|---|---|
| Type I-A | Type I-B | Type II-A | Type II-B | |
| Zone of attached keratinized gingiva | Adequate | Adequate | Inadequate | Inadequate |
| Osseous crest in relation to the CEJ | Osseous crest is 2-3 mm apical to the CEJ | Osseous crest is at the CEJ | Osseous crest is 2-3 mm apical to the CEJ | Osseous crest is at the CEJ |
| Treatment | Gingivectomy | Gingivectomy + osseous surgery | Apically positioned flap | Apically positioned flap + osseous surgery |
CEJ – Cementoenamel junction
APE-related, short clinical crowns were diagnosed as the etiology of the current patient’s gummy smile. Measuring gingival sulcus depth and bone sounding under local anesthesia to determine the level of crestal bone are important diagnostic tools for determining if a gingivectomy is indicated to correct gummy smile.[23] The present patient exhibited an adequate zone of attached gingiva, and the bone sounding depth was found to be 5 mm. Based on Coslet’s[21] classification [Table 2] of APE, the patient was classified as Type I-A (excessive gingival width), and a diode laser gingivectomy was deemed an appropriate treatment to enhance dental esthetics by increasing crown lengths in the anterior segment.
Diode laser
Gingivectomy and labial frenectomy
It is important to have a good understanding of biologic width before a gingivectomy procedure.[24,25] Some symptoms of biologic width violation include persistent gingival inflammation, recurrent pocket depths, and tissue recession.[24] Biologic width is a term that was coined by Cohen[23] and is defined as the combined heights of the connective tissue attachment and epithelial attachment. In 1961, Gargiulo et al.[26] reported the average connective tissue height was 1.07 mm, and the average epithelial attachment was 0.97 mm, leading to an average biologic width of 2.04 mm. The average depth of the facial gingival sulcus was 0.69 mm, thus the average total gingival height above the bone was found to be approximately 2.73 mm [Figure 22]. Kois[27] rounded this value up to 3 mm and called it the biologic zone [Figure 22]. Maintaining a biologic zone of 3 mm is an important factor in maintaining a healthy dentogingival complex.
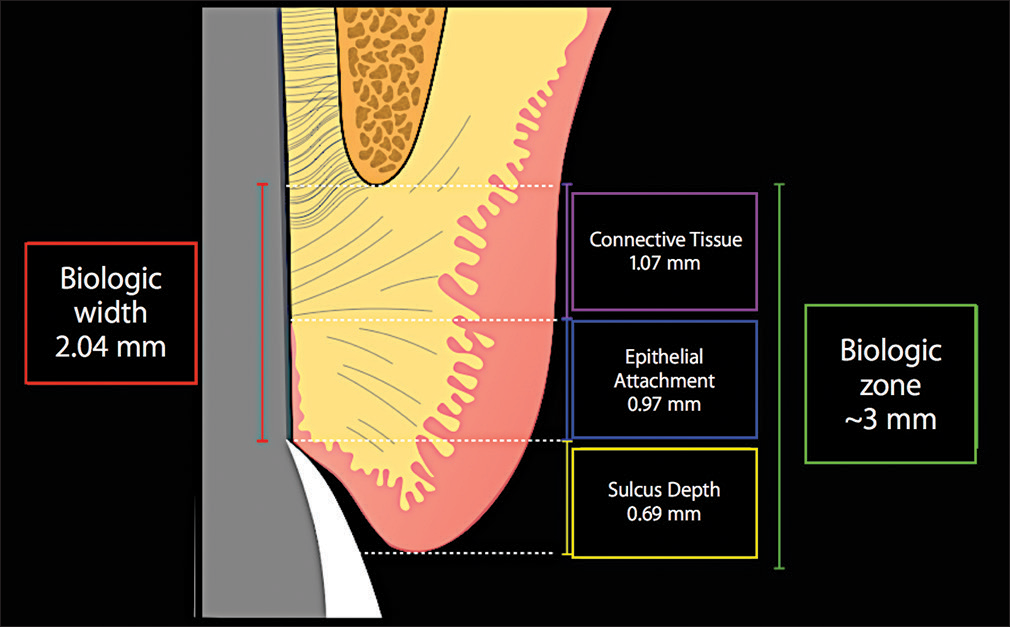
- A diagram of the periodontal attachment to a tooth illustrates the concept of biologic width: sulcus depth + width of the epithelial attachment + connective tissue attachment of collagen fibers directly into cementum occlusal to the alveolar bone crest. The total width of the biologic zone is ∼3 mm
For the present patient, the 3 mm reserved for maintaining the biologic zone was subtracted from the 5 mm bone sounding depth, revealing 2 mm of gingival width could be safely removed with laser gingivectomy.[28] As an additional procedure, the area of attachment for an impinging maxillary midline frenum was also removed with the diode laser, and the wound healed by secondary intention.
The word “LASER” is an acronym which stands for Light Amplification by Stimulated Emission of Radiation. Dental devices are generally classified as superficial and deep penetrating lasers.[29] Diode lasers deeply penetrate the tissue and are well absorbed by hemoglobin, thereby producing a layer of coagulation within the soft tissues (hemostasis) that controls bleeding. Diode lasers are usually preferred for dental soft-tissue revision because of their precise cutting and coagulation ability. For orthodontic gingival hypertrophy, diode laser gingivectomy is reported to provide earlier healing and greater improvement in gingival health compared to scalpel surgery.[30,31] Pre- and post-treatment comparison of gingival exposure when smiling is documented in Figure 23.

- Pretreatment (left) and posttreatment (right) lower facial photographs. The upper two views are a comparison of full smile before and after treatment. The lower two photos area similar comparison with the lips closed
Posterior and anterior bite turbos
For the present patient, the use of posterior BTs opened the bite to permit the correction of buccal crossbite for the upper left premolars. The subsequent anterior BTs were installed on the lingual surfaces on the maxillary central incisors for correction of her deep bite. Because of the large overjet, anterior BTs were bonded more gingivally. BTs should not be used on endodontically treated teeth because the latter are more susceptible to fracture. Upright or lingually tipped maxillary incisors may require a correction in the axial inclination before installing BTs. Anterior BTs serve as vertical stops in occlusion at the desired vertical dimension of occlusion (VDO). Spontaneous eruption of the posterior dentition to the desired occlusal plane, consistent with the treatment VDO, was the primary mechanism for overbite correction. However, the vertical load associated with anterior BTs may result in intrusion of the upper and lower incisors.[32-34]
Class II elastics
Class II elastics tend to retract the maxillary arch and extrude the maxillary anterior segment while rotating the plane of occlusion posteriorly (clockwise). The lower dentition compensates by posterior rotation of the mandible, opening of the VDO, extrusion of the posterior teeth, and increased axial inclination of the incisors. With respect to anterior dental segments, Class II elastics produce two predictable side effects: uprighting of the maxillary incisors and flaring of the mandibular incisors.[35] To resist the incisal tipping effects of Class II elastics, higher torque brackets are indicated in the maxillary anterior and lower torque brackets are prescribed for the mandibular anterior.[36,37] However, for the present patient, standard torque brackets were placed in both arches. This approach worked well for the lower arch because L1 to SN° improved from 102° to 97°. Unfortunately, the expected flaring effect of the intrusive force, anchored by the maxillary anterior miniscrews [Figure 12], was inadequate to counteract the side effects of the Class II elastics, so the axial inclination the upper incisors decreased (U1 to SN° from 96° to 90°). In retrospect, this problem was preventable as follows: (1) use higher torque brackets on the maxillary incisors, (2) progress to larger rectangular archwires to more completely express torque [Table 3], and/or (3) place palatal root torque in the anterior segment of the maxillary rectangular archwire.
Inadequate torque control of the maxillary incisors prevented the complete correction of the Class II posterior segments [Figure 15]. This problem resulted in the deduction of 10 additional points on the CRE score. The patient was adequately treated to ABO standards as evidenced by an overall CRE score of 25; however, if there was adequate overjet for a complete Class II correction, the score would have been a truly outstanding 15.
Conclusions
When treating complex malocclusions, bone screws provide effective anchorage in the maxillary anterior as well as the posterior regions of both arches. Recovery and alignment of an impacted maxillary canine are best accomplished with a simplified open window technique, in combination with miniscrew anchorage, to successfully guide the impacted canine into its correct anatomical position. A Class II malocclusion with gummy smile was efficiently corrected with bilateral IZC bone screws and maxillary anterior miniscrews, but decreased axial inclination of the maxillary incisors prevented complete correction of the Class II buccal segments.
Acknowledgment
The authors would like to thank Dr. Rungsi Thavarungkul for the beautiful illustrations. Thanks to Doctors Chris Chang, Angle Lee, Charlene Chang, Ashley Huang, and Lomia Lee for their mentorship and assistance with data collection.
This article was originally published in an online journal with a limited audience. APOS provides a wider dissemination of the helpful clinical techniques described.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- The ABO discrepancy index: A measure of case complexity. Am J Orthod Dentofacial Orthop. 2004;125:270-8.
- [Google Scholar]
- Preorthodontic uncovering and autonomous eruption of palatally impacted maxillary canines. Semin Orthod. 2010;16:205-11.
- [Google Scholar]
- Objective grading system for dental casts and panoramic radiographs. American board of orthodontics. Am J Orthod Dentofacial Orthop. 1998;114:589-99.
- [Google Scholar]
- A review of early displaced maxillary canines: Etiology, diagnosis and interceptive treatment. Open Dent J. 2011;5:39-47.
- [Google Scholar]
- Early treatment of palatally erupting maxillary canines by extraction of the primary canines. Eur J Orthod. 1988;10:283-95.
- [CrossRef] [Google Scholar]
- Mitchell L, ed. An Introduction to Orthodontics (3rd ed). New York: Oxford University Press; 2007. p. :147-56.
- The etiology of maxillary canine impactions. Am J Orthod. 1983;84:125-32.
- [CrossRef] [Google Scholar]
- A review of impacted permanent maxillary cuspids – Diagnosis and prevention. J Can Dent Assoc. 2000;66:497-501.
- [Google Scholar]
- The Orthodontic Treatment of Impacted Teeth (2nd ed). Abingdon, Oxon, England: Informa Healthcare; 2007. p. :1-228.
- The palatally displaced canine as a dental anomaly of genetic origin. Angle Orthod. 1994;64:249-56.
- [Google Scholar]
- A Textbook of Oral Pathology (2nd ed). Philadelphia: WB Saunders; 1963. p. :2-75.
- A review of the diagnosis and management of impacted maxillary canines. J Am Dent Assoc. 2009;140:1485-93.
- [Google Scholar]
- Comparison of two cone beam computed tomographic systems versus panoramic imaging for localization of impacted maxillary canines and detection of root resorption. Eur J Orthod. 2011;33:93-102.
- [CrossRef] [PubMed] [Google Scholar]
- Radiographic assessment of maxillary canine eruption in children with clinical signs of eruption disturbance. Eur J Orthod. 1986;8:133-40.
- [Google Scholar]
- Canine-lateral incisor transposition: Controlling root resorption with a bone-anchored T-loop retraction. Am J Orthod Dentofacial Orthop. 2016;150:1039-50.
- [Google Scholar]
- Soft tissue considerations for the management of impactions. Int J Orthod Implantol. 2011;24:50-9.
- [CrossRef] [Google Scholar]
- Analysis of failure in the treatment of impacted maxillary canines. Am J Orthod Dentofacial Orthop. 2010;137:743-54.
- [CrossRef] [PubMed] [Google Scholar]
- An esthetic evaluation of lip-teeth relationships present in the smile. Am J Orthod. 1970;57:132-44.
- [CrossRef] [Google Scholar]
- Implant-orthodontic combined treatment for gummy smile with multiple missing teeth. Int J Orthod Implantol. 2013;32:16-32.
- [CrossRef] [Google Scholar]
- Classification and craniofacial features of gummy smile in adolescents. J Craniofac Surg. 2010;21:1474-9.
- [Google Scholar]
- Diagnosis and classification of delayed passive eruption of the dentogingival junction in the adult. Alpha Omegan. 1977;70:24-8.
- [Google Scholar]
- Atlas of Cosmetic and Reconstructive Periodontal Surgery (3rd ed). Hamilton, Ontario, Canada: Decker BC; 2007. p. :259.
- Periodontal and prosthetic aspect of biological width part I: Violation of biologic width. Acta Stomatol Croat. 2000;34:195-7.
- [Google Scholar]
- The “biologic width” – A concept in periodontics and restorative dentistry. Alpha Omegan. 1977;70:62-5.
- [Google Scholar]
- Dimensions and relations of the dentogingival junction in humans. J Periodontol. 1961;32:261-7.
- [CrossRef] [Google Scholar]
- New paradigms for anterior tooth preparation. Rationale and technique. Oral Health. 1998;88:19-22. 25-7, 29-30
- [CrossRef] [PubMed] [Google Scholar]
- Principles of cosmetic dentistry in orthodontics: Part 2. Soft tissue laser technology and cosmetic gingival contouring. Am J Orthod Dentofacial Orthop. 2005;127:85-90.
- [Google Scholar]
- Laser in dentistry: An innovative tool in modern dental practice. Natl J Maxillofac Surg. 2012;3:124-32.
- [CrossRef] [PubMed] [Google Scholar]
- The adjunct effectiveness of diode laser gingivectomy in maintaining periodontal health during orthodontic treatment. Angle Orthod. 2013;83:43-7.
- [Google Scholar]
- Comparing the 810 nm diode laser with conventional surgery in orthodontic soft tissue procedures. Ghana Med J. 2013;47:107-11.
- [Google Scholar]
- Correcting deep-bite with fixed bite ramps. News Trends Orthod. 2009;16:68-71.
- [CrossRef] [Google Scholar]
- Mutilated class II division 2 malocclusion: Implant-orthodontic treatment utilizing flapless implant surgery and platelet-rich fibrin. Int J Orthod Implantol. 2014;33:22-45.
- [Google Scholar]
- Class II deep bite malocclusion with posteriorly-inclined incisors. Int J Orthod Implantol. 2012;25:32-42.
- [CrossRef] [Google Scholar]
- Correction of class II malocclusion with class II elastics: A systematic review. Am J Orthod Dentofacial Orthop. 2013;143:383-92.
- [Google Scholar]
- Honing Damon system mechanics for the ultimate in efficiency and excellence. Clin Impressions. 2008;16:23-8.
- [Google Scholar]
- Begin with the end in mind: Bracket placement and early elastics protocols for smile arc protection. Clin Impressions. 2009;17:4-13.
- [Google Scholar]
- Discrepancy Index worksheet

- Case-radiograph evaluation

- IBOI pink and white esthetic score




