

Translate this page into:
An evaluation of panoramic radiograph to assess mandibular asymmetry as compared to posteroanterior cephalogram
Address for correspondence: Dr. Astitva Agrawal, Department of Orthodontics and Dentofacial Orthopaedics, School of Dental Sciences, Sharda University, Knowledge Park III, Greater Noida, Uttar Pradesh, India. E-mail: astitva87@gmail.com
This article was originally published by Wolters Kluwer and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Aim and Objectives
To assess the reliability of orthopantomograms (OPGs) in detecting facial asymmetry.
Materials and Methods
The OPGs and posteroanterior cephalograms for 10 patients with facial asymmetry were obtained from the outpatient department of the dental college. These radiographs were traced and analyzed. Six measurements (four linear and two angular measurements) were made on both sides. Asymmetry was defined by subtracting the right and the left side measurements. The differences from OPG were compared to those obtained from posteroanterior cephalograms. The kappa statistics and intra-class correlation coefficient (ICC) were used to calculate the differences.
Results
The ICC was calculated between OPGs and posteroanterior cephalograms difference measurements. The class interval for all measurements was noted between 0.61 and 0.84. The ICC was 0.7861, which shows strong correlation between the values (P < 0.0005) by probability 10−5, within 95%, coefficient correlation lies between 0.61 and 0.84. Kappa test gives a value of 0.64, which shows strong agreement between the measurements.
Conclusion
Individually, the measurements from OPGs may not be reliable but the obtained difference between the values of the OPGs and the posteroanterior cephalograms are comparable in nature and show strong correlation and can be used to detect facial asymmetry.
Keywords
Asymmetry
correlation
orthopantomograms
posteroanterior cephalograms

INTRODUCTION
The primary goal of orthodontic treatment is to create a balanced and harmonious facial appearance. Although perfect craniofacial symmetry does not exist in nature, asymmetry ranges from clinically undetectable to a gross abnormality.
The etiology of mandibular asymmetry is vast and might be a combination of genetic and environmental influences. Common causes include trauma, infections, developmental abnormalities, myogenic problems, and syndromes such as Treacher Collins, occlusal interferences, and joint pathologies like rheumatoid arthritis. Traditionally, mandibular asymmetry has been diagnosed by a combination of tools. These include a thorough clinical examination followed by photographs of various frontal and side views, in addition to radiographs such as lateral and posteroanterior cephalograms, oblique radiographs of the mandible taken at 45°, and panoramic radiographs.[1-3]
The orthopantomogram (OPG) is commonly used in daily clinical routine. This radiograph allows a bilateral view and adequate information on vertical measurements. Studies on panoramic radiography have shown that horizontal measurements tend to be particularly unreliable because of nonlinear variation in magnification at different object depths,[4] whereas vertical and angular measurements are acceptable provided the patient’s head is positioned properly.[5]
The diagnosis of asymmetries is important for treatment.[6] Although most practitioners do not use panoramic images for mandibular asymmetry diagnosis,[7,8] other studies support their use and show that some practitioners depend on conventional panoramic images.[9-11]
Since long the posteroanterior cephalogram has been used in the orthodontic and orthognathic diagnosis and surgery planning for the treatment of asymmetry.[12-14] The posteroanterior cephalogram provides valuable mediolateral information which is useful for facial asymmetric evaluation and essential for transverse evaluation of the craniofacial skeleton and dentoalveolar structures.[14]
Transversal measurements can be performed on both a posteroanterior cephalogram and an oblique mandibular radiograph. Both types of radiographs, however, have limitations in both methods that are affected by a tilt of the head or angulation of the beam.[13,15]
MATERIALS AND METHODS
Ten patients having facial asymmetry were selected from the visiting dental outpatient department. A routine, conventional panoramic radiograph made by a standardized technique was used for the analysis. A posteroanterior cephalogram was taken from the same unit from where the OPG was taken. Both radiographs were manually traced on acetate sheets-economy grade lacquered polyester single matte (Garware Polyester Ltd., Mumbai, India). Thickness was 50 μ with a 0.5 mm thick lead 3H pencil.
Linear and angular measurements were made on both the tracings. Since the measurements made on the posteroanterior cephalograms were considered to be the gold standard for measuring asymmetry, the values obtained from the panoramic image was compared to them to check the reliability and accuracy of the panoramic radiographs.
Landmarks
Orbitale (Or) — Lowest point on bony orbit [Figure 1a and b].
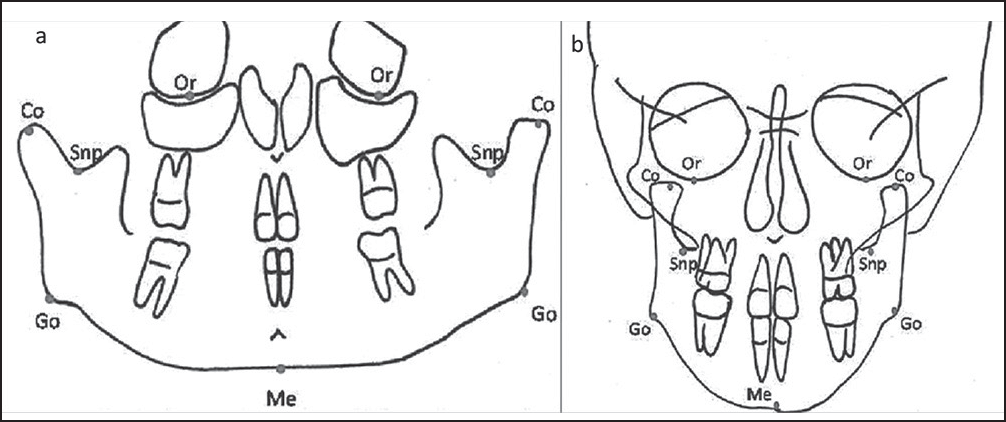 Figure 1
Figure 1- (a) Landmarks made on orthopantomogram. (b) Landmarks made on posteroanterior cephalogram
Condylion (Co) — Most superior point on coronoid process [Figure 1a and b].
Sigmoid notch point (Snp) — Deepest point on sigmoid/mandibular notch [Figure 1a and b].
Gonion (Go) — Most posteroanterior point at the angle of mandible [Figure 1a and b].
Menton (Me) — The most inferior midline point on the mandibular symphysis, the lowest point on the symphyseal shadow of the mandible [Figure 1a and b].
Horizontal plane
Orbital plane — Line connecting point orbitale bilaterally [Figure 2a and b].
 Figure 2
Figure 2- (a) Horizontal planes in orthopantomogram. (1) Orbital plane. (2) Sigmoid notch plane. (3) Mandibular plane. (b) Horizontal planes in posteroanterior cephalogram. (1) Orbital plane. (2) Sigmoid notch plane. (3) Mandibular plane
Sigmoid notch planes — Tangent drawn from the deepest point on sigmoid notch parallel to orbitale plane (drawn on the left and right sides separately) [Figure 2a and b].
Mandibular plane — Line drawn from the lower most point on mandible parallel to the orbitale plane [Figure 2a and b].
Following linear measurements will be made on both tracings
Length of condyle — Measured from the Co to sigmoid notch plane along the long axis of condylar process [Figure 3a and b].
 Figure 3
Figure 3- (a) Linear measurements of both sides on orthopantomogram. (1) Condylar length. (2) Ramus length. (3) Corpus length. (4) Total length. (b) Linear measurements made on posteroanterior cephalogram (1) condylar length. (2) Ramus length. (3) Corpus length. (4) Total length
Length of ramus — Measured from point Co to point Go [Figure 3a and b].
Length of corpus — Measured from point Go to point Me [Figure 3a and b].
Total length — Measured from Co to point Me [Figure 3a and b].
Following angular measurements will be made on both tracings
Gonial angle — Co-Go-Me [Figure 4a and b].
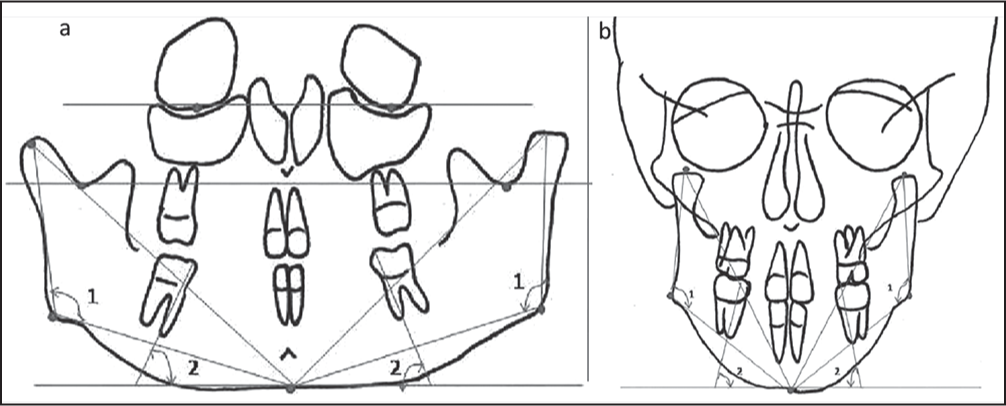 Figure 4
Figure 4- (a) Angular measurements made on orthopantomogram. (1) Gonial angle. (2) Inclination of first molar angulation. (b) Angular measurements made on posteroanterior cephalogram. (1) Gonial angle. (2) Inclination of first molar angulation
Mandibular first molar angulation — Angulation of mandibular molars to the mandibular plane (line passing through mesiobuccal cusp and mesial root to mandibular plane) [Figure 4a and b].
Exclusion criteria
Samples were excluded on the bases of unerupted or missing incisors, unerupted or missing molars, unerupted teeth overlying the incisors, and molar apices, as well as rotated head.
The six measurements (four linear and two angular) were made separately for OPG tracings and posteroanterior cephalogram. The differences were calculated for the left and right sides, and asymmetry was defined.
Correlation was calculated with a variance components analysis using the intra-class correlation coefficient (ICC). The ICC has a value between 0 and 1 and measures the strength of agreement among observer. The ICC is similar to the kappa coefficient. Analogous to kappa, an ICC of 0.61 to 0.80 is interpreted as substantial agreement and an ICC of 0.81-1.00 as an almost perfect agreement.
RESULTS
Comparison between orthopantomogram and posteroanterior cephalogram – statistical analysis
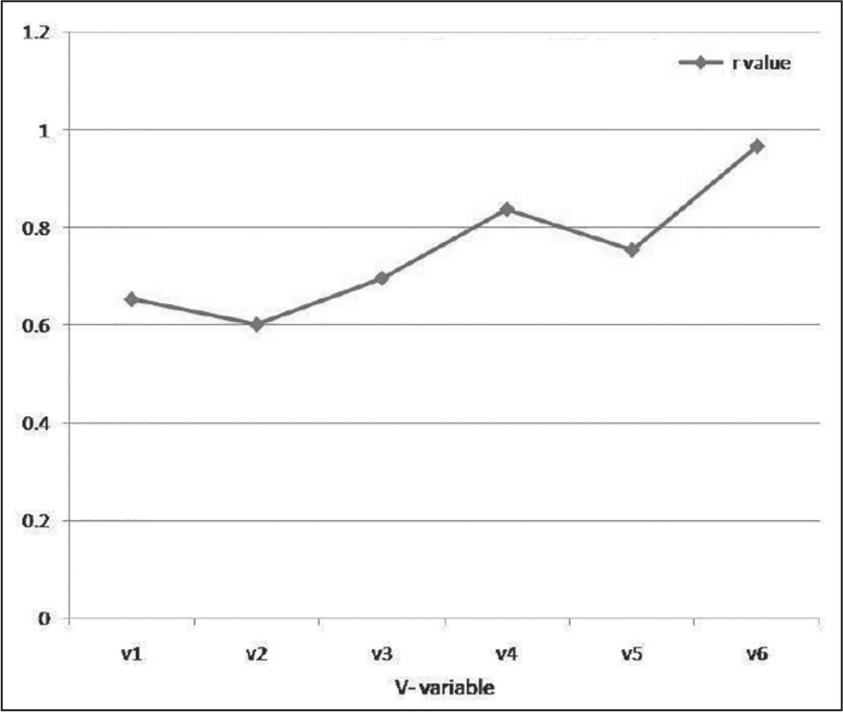
The asymmetries as measured by the OPG and by the cephalograms for the different variables of the ten patients are shown by calculating the mean and standard deviation [Table 1]. The correlation coefficient between the two columns is 0.75. The probability of obtaining such a high correlation coefficient from random uncorrelated data is 5.5 × 10−12. The 95% confidence interval for the correlation coefficient is (0.61, 0.84). Thus, the probability for the correlation coefficient to lie between 0.61 and 0.84 is 95%. It can be concluded that there is very strong correlation between the asymmetries as measured by the two methods [Table 2 and Figure 5].
| Variable | OPG mean±SD | PA cephalogram mean±SD | OPG Vs PA cephalogram mean difference and SD | Paired t test | p value |
|---|---|---|---|---|---|
| Length of condyle (Co-Snp) | 1.2±0.918937 | 2±1.66667 | 1±1.1055 | 0.10018 | 0.2004 |
| Length of ramus (Co-Go) | 1.8±0.918937 | 2.35±0.944281 | 0.65±0.7472 | 0.10168 | 0.2034 |
| Length of corpus (Go-Me) | 2.15±1.780293 | 2.65±1.616753 | 1.1±0.8432 | 0.25959 | 0.5195 |
| Total length (Co-Me) | 2.55±1.442413 | 2.1±1.629588 | 0.75±0.6346 | 0.26072 | 0.5215 |
| Gonial angle (Co-Go-Me) | 2.4±1.149879 | 2.3±1.512907 | 0.8±0.5374 | 0.43484 | 0.8697 |
| Mandibular 1st molar angulation | 2.45±1.921371 | 3.25±1.512907 | 0.8±0.5374 | 0.18957 | 0.3791 |
SD – Standard deviation; OPG – Orthopantomogram
| Variable no | Variable | r value |
|---|---|---|
| V1 | Length of condyle(Co-Snp) | 0.652929 |
| V2 | Length of ramus(Co-Go) | 0.601823 |
| V3 | Length of corpus(Go-Me) | 0.695821 |
| V4 | Total length(Co-Me) | 0.836688 |
| V5 | Gonian angle(Co-Go-Me) | 0.753659 |
| V6 | Mandibular 1st molar angulation | 0.965166 |
*P value is set at <0.0005; **Values < 0 as – no agreement; 0–0.20 – slight; 0.21–0.40 – fair; 0.41–0.60 – moderate; 0.61–0.80 – substantial; 0.81–1 – almost perfect agreement
- Correlation discrepancy between the left and right sides of individual variables showing asymmetry detected orthopantomogram and posteroanterior cephalogram values for each variable
These values [Table 1] give the probability that the two columns are drawn from the same normal distribution. Differences are regarded as significant if the P < 0.05. As each of the P values for all the six variables is more than 0.05, the difference is not significant for any of the variables.
Kappa test gives a value of 0.64, which shows strong agreement between the measurements. 0-0.20 as slight, 0.21-0.40 as fair, 0.41-0.60 as moderate, 0.61-0.80 as substantial, and 0.81-1 as almost perfect agreement as suggested by Landis and Koch.
The ICC between posteroanterior cephalogram and OPG was investigated together. No significant differences were found between the OPG and posteroanterior cephalogram.
In accordance with the P value selected for the purpose of our study, it is observed that no significant difference is present between the variables (P < 0.0005). Therefore, the results are in line with our initial hypothesis which stated that asymmetry noted from OPG can be compared to the asymmetry obtained from posteroanterior cephalogram
DISCUSSION
Traditionally, the values of OPG have been studied in isolation, which arguably may not provide the most reliable results. Hence, the main focus of this study was aimed at trying to establish a better mechanism to derive greater reliability in calculating asymmetry.
The goal of this study was to gain some clarity regarding the diagnosis of mandibular asymmetry with panoramic radiographs. A criterion for this study was the use of a gold standard to evaluate the accuracy of the panoramic image in the detection of mandibular asymmetry.
Diagnosing of mandibular asymmetry is a complex problem. Mandibular asymmetry may be caused by a number of factors such as condylar hyperplasia, hemimandibular hypertrophy, hemimandibular elongation, coronoid hyperplasia, and temporomandibular joint disorders, etc. Though the precise differentiation of these conditions may be confusing, clinical environment requires radiographic impressions at first hand before any other data are available.
Tronje et al.[4] mathematically calculated the accuracy of panoramic measurements. Within certain limits, the panoramic film can be used for vertical measurements in clinical practice if the patient is properly positioned. They also concluded that horizontal dimension is unreliable.
Habets et al.[11] altered the central position of a synthetic mandible up to 10 mm in the horizontal plane of a Siemens orthopantomograph 5 and took nine pantomographic radiographs. The authors suggested that the 6% observed difference between left and right condylar height measured on the panoramic film might be a result of technical errors, and differences greater than 6% can be considered true vertical asymmetry.
Kjellberg et al.[16] imaged two dry skulls in six positions with three panoramic units. They found out that manufacturer’s listed magnification for the panoramic unit might not correct for all areas of the panoramic radiograph. Therefore, different panoramic machines provide different measurements. Condylar ratio can be used to look for condylar height asymmetries, unaffected by positioning error, distortion, or magnification errors.
Laster et al.[17] compared horizontal and vertical measurements of anatomic points on 30 skulls imaged with ideal, 7 mm laterally shifted, and 10° rotation around a vertical axis positioning in a Sirona Orthophos Plus Panoramic Unit with measurements obtained by software on digital images. The purpose of this study was to assess the changes in both linear measurements and symmetry ratios on panoramic radiographs. They found that horizontal measurements provided the greatest differences between the panoramic image and actual skull. Magnification reported by the manufacturer was consistently less than the calculated magnification. Accuracies for detecting asymmetry on the panoramic image were 67% for ideal, 70% for rotated, and 47% for shifted. They said that caution should be used when making absolute measurements or relative comparisons.
Kambylafkas et al.[18] evaluated the ability of panoramic radiographs to assess side-to-side differences in condyle and ramus height. By using a phantom marked with radiopaque steel balls representing either right or left side of mandible, two sets of panoramic films were created with an OPG OP 100. They found that 2.1% average variation in the total height of the mandible laminograph is recommended as the gold standard for measuring posterior vertical mandibular asymmetry. Correlation between the laminograph and panoramic measurements is 0.92 for total height and 0.39 for condylar height. Using the 6% cut off reported by Habets et al.,[11] the sensitivity and the specificity for diagnosing mandibular asymmetries with panoramic images are 0.62 (total height) and 1.0, respectively. The panoramic radiograph can be used to evaluate vertical posterior mandibular asymmetry.
In another study, the ICC between lateral cephalogram and OPG was investigated for the orthodontists and maxillofacial surgeons together for linear measurements. No significant differences were found between the OPGs and lateral cephalogram.[19-20]
Horizontal measurements have been shown to be particularly unreliable because of the nonlinear variation in the magnification at different object depths; whereas, vertical measurements are relatively reliable.[4]
CONCLUSION
Following results have been concluded:
A strong correlation exists between the posteroanterior cephalogram and OPG.
All the variables taken in this study, that are four linear measurements-length of condyle (Co-Snp), length of ramus (Co-Go), length of corpus (Go-Me), total length (Co-Me) and two angular measurements-gonial angle (Co-Go-Me), and mandibular first molar angulation, are found to be comparable in both posteroanterior cephalogram and OPG.
Clinically, the panoramic view is unique and may be used as a primary diagnostic tool in detecting asymmetry along with posteroanterior cephalogram.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- A computer-based assessment of structural and displacement asymmetries of the mandible. Am J Orthod Dentofacial Orthop. 1991;100:19-34.
- [Google Scholar]
- Facial asymmetry. The diagnostic challenge. Atlas Oral Maxillofac Surg Clin North Am. 1996;4:1-18.
- [Google Scholar]
- Image distortion in rotational panoramic radiography. IV. Object morphology; outer contours. Acta Radiol Diagn (Stockh). 1981;22:689-96.
- [Google Scholar]
- Panoramic radiographs: A tool for investigating skeletal pattern. Am J Orthod Dentofacial Orthop. 2003;123:175-81.
- [Google Scholar]
- Visualizing the mandibular ramus in panoramic radiography. Oral Surg Oral Med Oral Pathol. 1971;31:422-9.
- [Google Scholar]
- The condylar asymmetry measurements in different skeletal patterns. J Oral Rehabil. 2003;30:738-42.
- [Google Scholar]
- The Orthopantomogram, an aid in diagnosis of temporomandibular joint problems. II. The vertical symmetry. J Oral Rehabil. 1988;15:465-71.
- [Google Scholar]
- Posteroanterior (frontal) cephalometry In: Athanasiou AE, ed. Orthodontic Cephalometry. London: Mosby-Wolfe; 1995. p. :125-40.
- [Google Scholar]
- Posteroanterior cephalometry: Craniofacial frontal analysis In: Jacobson A, Jacobson RL, eds. Radiographic Cepahalometry: From Basics to 3D Imaging. Hanoover Park: Quintessence Publishing Co. Inc.; 2006. p. :267-92.
- [Google Scholar]
- Oblique lateral cephalometric radiographs of the mandible in implantology: Usefulness and reproducibility of the technique in quantitative densitometric measurements of the mandible in vivo. Clin Oral Implants Res. 2000;11:476-86.
- [Google Scholar]
- Condylar height on panoramic radiographs. A methodological study with a clinical application. Acta Odontol Scand. 1994;52:43-50.
- [Google Scholar]
- Accuracy of measurements of mandibular anatomy and prediction of asymmetry in panoramic radiographic images. Dentomaxillofac Radiol. 2005;34:343-9.
- [Google Scholar]
- Validity of panoramic radiographs for measuring mandibular asymmetry. Angle Orthod. 2006;76:388-93.
- [Google Scholar]
- Linear mandibular measurements: Comparison between orthopantomograms and lateral cephalograms. Cleft Palate Craniofac J. 2009;46:147-53.
- [Google Scholar]
- Reproducibility of rotational panoramic radiography: Mandibular linear dimensions and angles. Am J Orthod Dentofacial Orthop. 1986;90:45-51.
- [Google Scholar]




