

Translate this page into:
Excellence in lingual orthodontics: Its challenges and solutions — The iLingual three-dimensional low-profile tandem slot
Address for correspondence: Dr. Jignesh Kothari, Private Practioner, Ex. Asst. Professor, Department of Orthodontics, Terna Dental College, Nerul, Navi Mumbai, Maharashtra, India. E-mail: drjigneshkothari@gmail.com
This article was originally published by Wolters Kluwer and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Since its inception in 2007 as a stock bracket design the iLingual braces had evolved over the years to a completely customized lingual orthodontic appliance. The demand for maximum individualization is met by using state-of-the-art computer-aided design/ computer-aided manufacturing technology incorporating the bracket design into a complete digital workflow. Additional advantages of the system include complete three-dimensional control with tandem slot, direct and thus simplified rebonding in the event of bracket loss, more precise finishing, and enhanced patient comfort.
Keywords
Computer-aided design/computer-aided manufacturing appliances
customized lingual
lingual orthodontics

INTRODUCTION
Few aspects of dentistry have undergone as dramatic a boom in recent years as dental esthetics. However in contrast to services provided by general dentists, orthodontic therapy often extends over a long period, so not only is the outcome of esthetic significance to the patient, but also the course taken to achieve that outcome. From the esthetic perspective the best appliance to be totally invisible and give complete three-dimensional (3D) control to correct any kind of malocclusion is a fixed lingual appliance.[1-5]
Despite the demand for “invisible braces,” lingual orthodontics failed to catch on in the United States in the mid-1980s, and it became less significant thereafter. However, further developments at different levels, such as laboratory-based bracket positioning, archwire fabrication, indirect bonding and perseverance of dedicated clinicians has led to a rise in the number of lingually treated patients in Europe and Asia.[5-10] When doctors with experience in this technique are asked why they have ceased to use it, three explanations are commonly given: The bracket loss rate is substantially higher than in labial cases, and the indirect rebonding technique is complex and imprecise; the finishing process is time-consuming, and the average quality falls far short of that of labial cases;[11,12] and patients often have difficulty adapting to the appliance, especially when undergoing lingual treatment in both arches.[13,14]
These basic fears of lingual orthodontics can now be overcome with the help of technological advances in the field. Customized appliances generated by computer-aided design/computer-aided manufacturing CAD/CAM are the future in this fi eld.[15,16] Individualization of the bracket base, a process used in various laboratory processes and always essential in the lingual technique, takes place during fabrication of the single brackets;[17-19] in other words, each tooth has its own customized bracket, made with state-of-the-art computer-aided design/computer-aided manufacturing (CAD/CAM) software coupled with high-end, rapid prototyping techniques. The iLingual 3D system is one such innovation using state of the art CAD/CAM technology. This article outlines the evolution, development and production of an innovative, fully customized lingual bracket system, and demonstrates its effi ciency with brief case reports.
iLingual three-dimensional
The first prototype of iLingual braces were developed by Dr. Jignesh Kothari in the year 2007 and thereafter several prototypes were produced to modify the design and make it more user-friendly at the same time making it more effi cient for treatments. The brackets were made by CAD design manufactured with rapid prototyping and casted in gold alloy. In 2009 iLingual ribbon arch stock bracket (0.025″ × 0.0175″ slot size) was introduced with vertical insertion in anteriors and horizontal insertion in posteriors, the same was used with the modifi ed target set up for individualization. In 2011 the bracket design was integrated with a digital workfl ow to create India’s fi rst CAD/CAM lingual appliance the iLingual 3D. In 2012 the design was modifi ed to make it more rounded from all dimensions to make it more acceptable to the tongue. In 2014 we reworked the design to make it 25% smaller [Figure 1] in dimension yet retaining the functionality of the system. Along with this, we also downsized the slot size form 0.0175 × 0.025″ to 0.016″ × 0.022″ with the fi nal slot-fi lling wire being 0.022″ × 0.016″ TMA [Figure 2]. The only main drawback with the ribbon arch system with vertical insertion in the anteriors is the TIP control which requires reverse over ties and is sometimes diffi cult to achieve and maintain through the treatment [Figure 3].
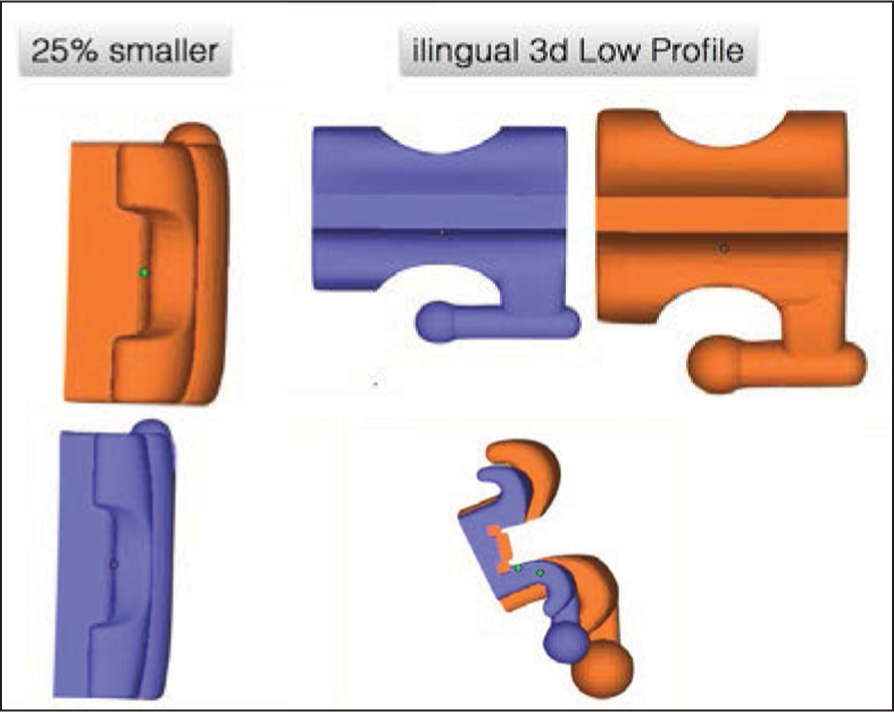
- iLingual 3D low profi le 25% smaller
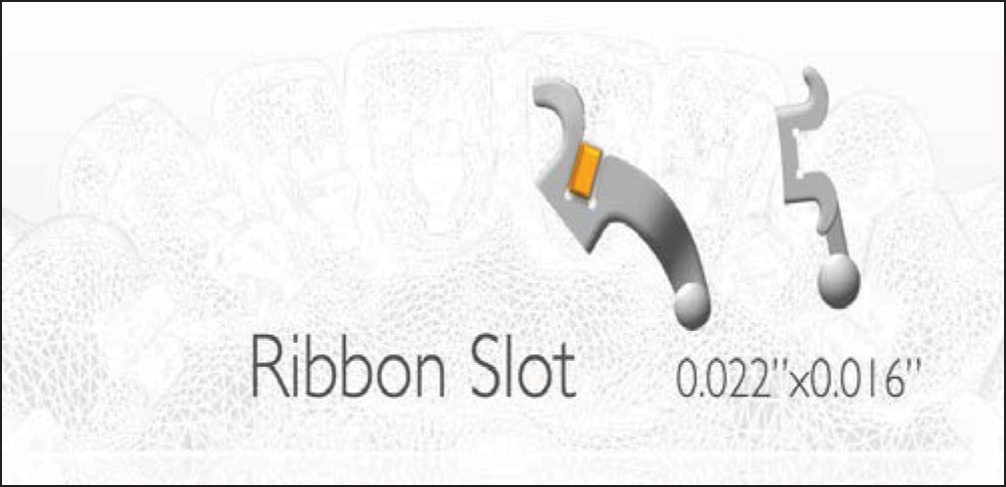
- Ribbon arch slot 0.022” × 0.016” with vertical insertion in anteriors and horizontal insertion in posteriors
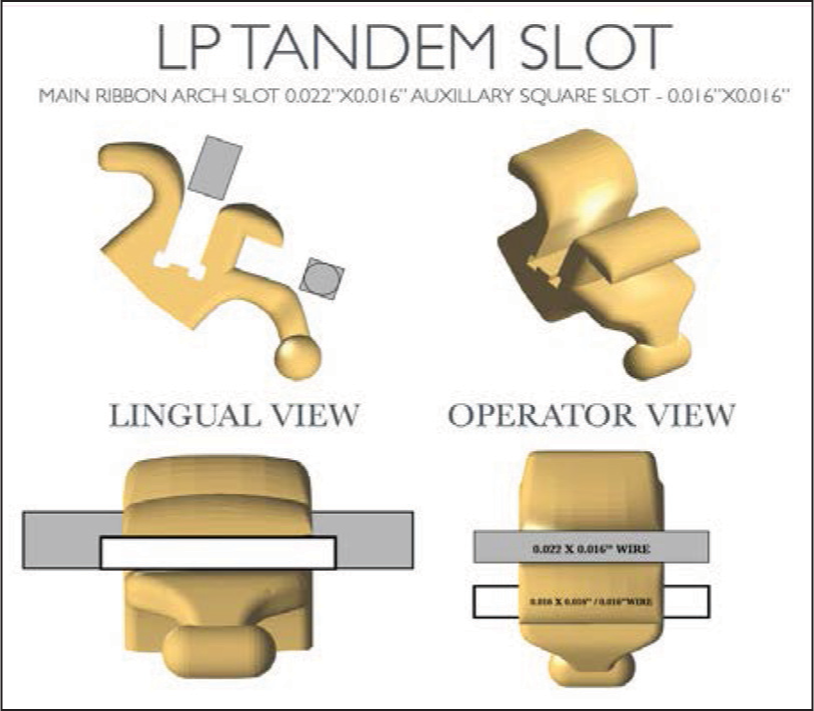
- Low profile tandem slot main ribbon arch slot 0.022” × 0.016” auxillary square slot - 0.016” × 0.016”
To overcome this problem and give the user the fl exibility of dual slot we introduced the ilingual 3D LPT tandem slot in 2015 [Figure 3]. The tandem slot [Figure 3] is basically an addition of a horizontal insertion slot (0.016″ × 0.016″ square slot) in the anterior teeth only to receive a round wire from 0.012″ to 0.016″ for TIP control. The main arch wire still remains the ribbon arch 0.022″ × 0.016″. This eliminates the need for reverse overties and encourages simple ligation mechanics giving complete control in all 3D.
The process
Impressions — Accurate PVS impressions taken with two-step technique are mandatory. Intraoral scanned fi les in standard triangulation language (STL) format are also acceptable.
Impression requirements
All margins must be evident.
All cusps and incisal edges shown clearly.
No tray exposure; suffi cient depth of material to avoid exposing the tray.
No presence of folds.
No presence of pull away.
All tooth anatomy present.
No voids.
Full capture of molars (up to second molars).
Scanning
Noncontact scanning of the therapeutic setup is performed with a high-resolution optical 3D scanner (R 700-3 shape). As with human perception, the 3D scanner must examine the model from various perspectives to create a complete 3D representation. The outcome is a compound surface consisting of many thousands of minute triangles (STL surfaces) that can be turned, observed, and processed on a computer with appropriate design software.
Virtual treatment planning
The STL fi les are then loaded in the virtual treatment planning software (ortho analyzer from 3 shape), each tooth is sectioned virtually and after selection of appropriate arch from and occlusal plane determination the teeth are virtually moved in all 3Das per the instructions of the treating orthodontist in the lab order form.
Communication with the orthodontist
The setup fi les and the comparison fi les are shared with the orthodontist by email for approval.
Virtual appliance designing
The setup files are then imported into the designing software for the designing of the iLingual bracket system taking due care to keep a very good balance between the patient comfort, operatory handling of the appliance and the biomechanical effi ciency of the system. Each brace is numbered with the patient initial and tooth number. Designing is done.
Rapid prototyping [Figure 3a]
- Resin out puts after rapid prototyping with tooth number engraved for identifi cation
The bracket design fi les are then sent to a rapid prototyping machine (3D systems) to print the brackets with an accuracy of 15-20 microns in resin.
Casting [Figure 4]
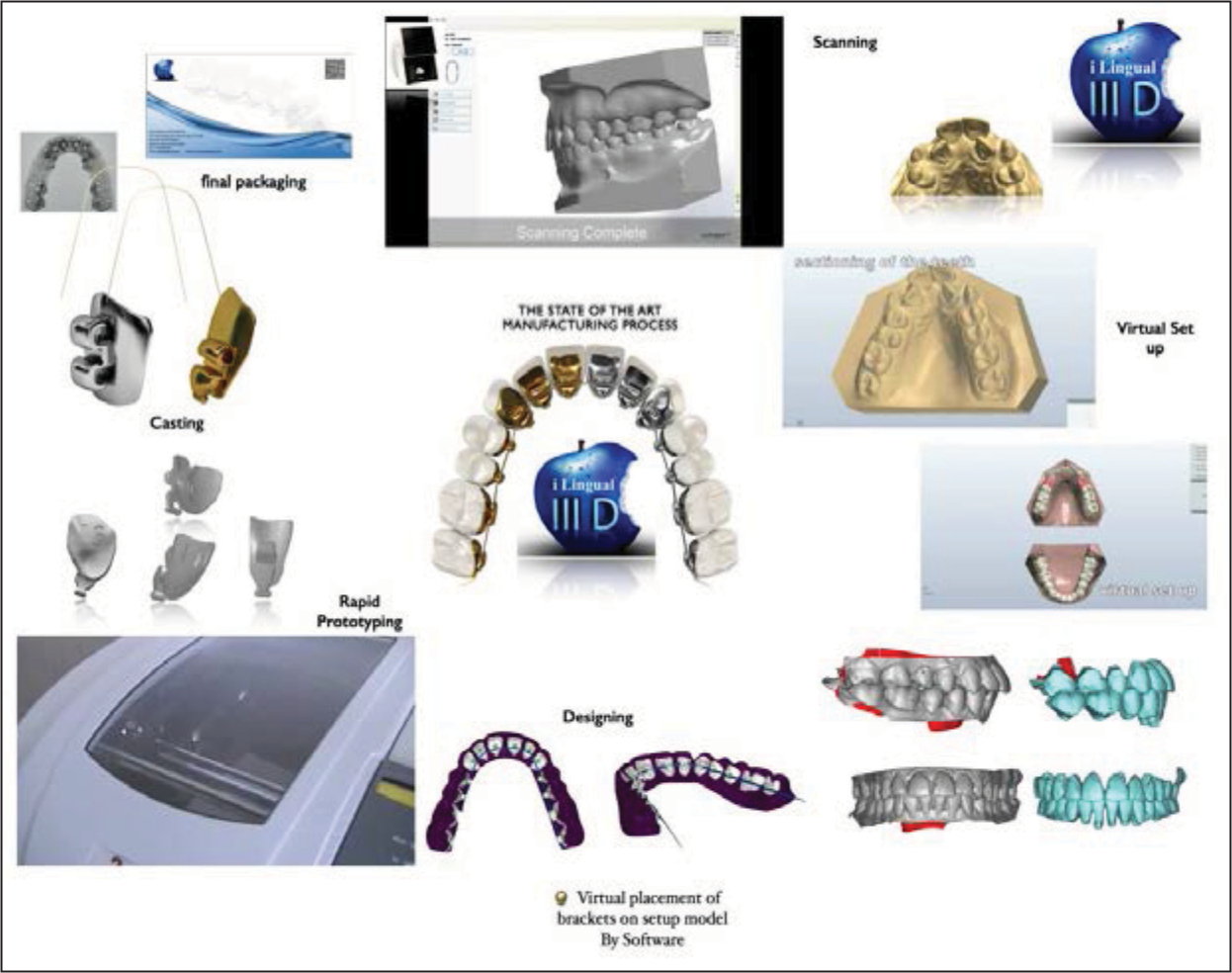
- The complete manufacturing process from start to fi nish
The printed resin brackets are then casted in hard dental gold alloy or in the new “Tilite” titanium alloy. The Tilte titanium alloy is an excellent economical viable alternative to gold, developed in Talladium’s Biomedicine Research Laboratory, a division of Talladium Inc., and the Southern California Aerospace Industry. The secret is the formation of an intermetallic compound that does not have any elemental property and differs from the elements that the alloy is composed of. The nickel content in all the alloys of the formula patented by Talladium is composed of chrome and molybdenum, so the nickel is no nickel anymore, but an inoffensive inter-metallic compound. Tilite is the only nongold alloy that has been approved by the Food and Drug Administration and for ISO certifi cation and is extensively tested by the Universities of Boston, Minnesota and Iowa. Tilite dental alloys outperform all other ceramic alloys in castability, fi nishing and compressive strength, greater esthetics — due to lighter color and thermally resistant.
Transfer trays
Brackets are indirectly transferred by the means of double layer transfer tray with a inner soft core of 1.5 mm bioplast and outer hardcore for the stability of 0.5 mm Duran.
Wires
All wires necessary for the case are provided customized manually as per the requirement of the case from the arch wire design generated from the software.
Advantages of the iLingual three-dimensional system
Quality.
Predictability.
Patient comfort.
Max 3D control and better fi nishing.
Better effi ciency due to vertical insertion.
Better rotation control.
Better torque control.
Better TIP control with (tandem slot).
Simple and easy to learn.
Easy rebondings.
DISCUSSION
The introduction of tandem slot increases the effi ciency of the appliance overcoming the only slight drawback with vertical insertion brackets of inadequate TIP control [Figure 5]. The tandem slot with it’s the auxiliary square slot helps in leveling anteriors and achieving desired tip control with simple ligation mechanics. This does away with the reverse over ties. It is especially help full in cases where TIP control in anteriors is critical like missing laterals and replacements with implants, lower incisor extractions, unilateral extraction cases, bilateral extraction cases with fi rst premolar extractions where cuspid tip is important. Since the main arch wire still remains the ribbon arch it provides great torque control. The auxiliary slot gives the operator the fl exibility to use either slot up to the 0.016″ S.S. round wires in tandem or in single as the case may demand. Downsizing the slot to a 0.022 × 0.016″ from the conventional 0.025 × 0.018″ is done based on clinical experience after using the appliance for 6 years and on more than 1000 patients. The advantage is that it allows the operator to fi nish the case with lesser and lighter wires which are easy to manipulate if case may demand so, at the same time maintaining the required rigidity on the lingual side due to the reduced inter-bracket distance. Hence, the fi nal fi nishing wire is 0.022 × 0.016″ TMA to fi ll the slot and due to the CAD/CAM process and the quality check of torque play complete expression of prescription is possible even with 0.022 × 0.016″ slot size.
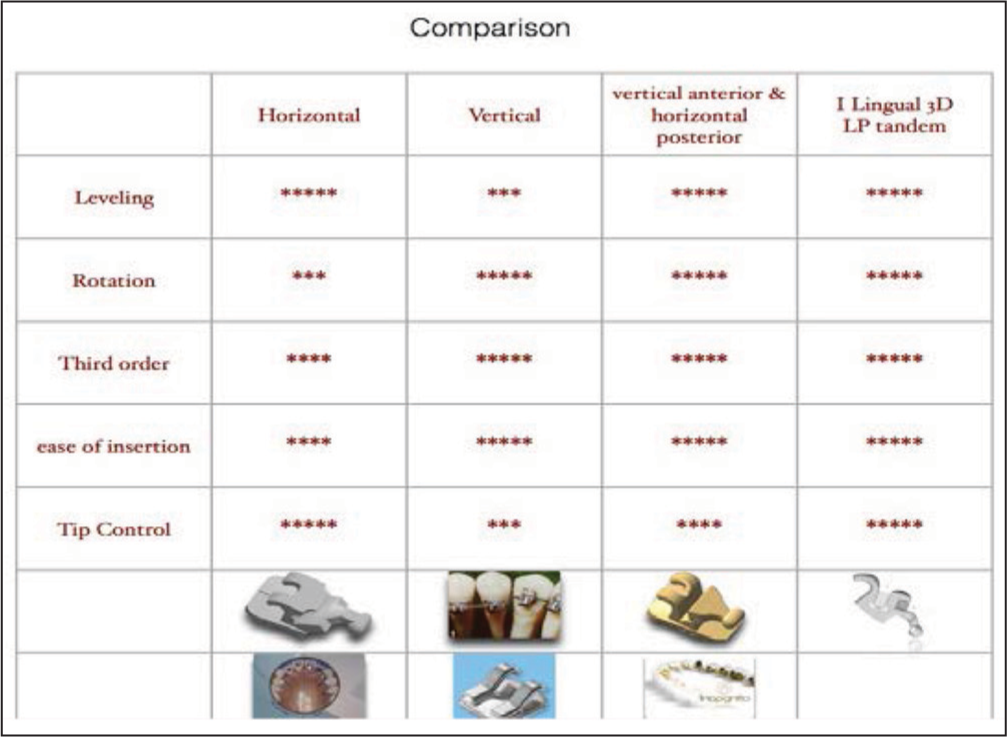
- Comparison between different lingualbracket designs
This customized system also addresses four problems traditionally associated with lingual brackets: The brackets are more diffi cult to bond and tend to debond more often, fi nishing is more diffi cult, the brackets cause speech problems or irritate the tongue in some patients and the increased chair side time to manage every case with a lingual appliance.
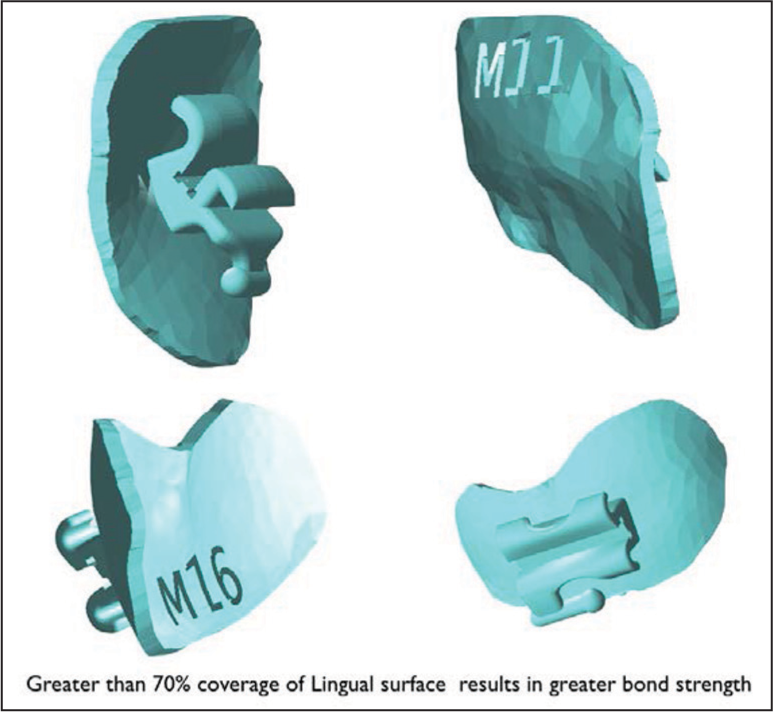
Several steps have been taken to address the problem of diffi cult bonding and frequent debonding. First, the bracket bases have been extended covering more than 70% of the lingual surface of the tooth [Figure 3a]; this results in greater bond strength. Overall, the brackets have a lower-profi le, which induces less leverage when biting on appliance components [Figure 1]. However, this alone is no guarantee of a reduced bracket loss rate. The quality of the impressions for the bonding model and of the indirect bonding is still crucial.[21,22] If a bracket does need to be rebonded, the form-fi t properties between the bracket base and the tooth provide a positive lock making repositioning a simple task. On completion of treatment, the brackets should be removed with special debonding pliers (Ormco, Glendora, Calif or American Orthodontics).
The major factor contributing to problems in the finishing process is the inaccurate fit between brackets and arch wires (torque play). The virtual production of the brackets on the computer almost completely eliminates errors in the actual production of the bracket bases. An important step in simplifying the finishing process is reducing the torque play with nominally slot-filling arch wires, because the arch wires tend to be smaller and the slots notably larger than the given values. The resulting torque play might lead in some cases to substantial finishing problems.[11,16] If the appliance is positioned farther away from the labial surface of the tooth in terms of an increased positioning thickness, this problem is intensified in almost direct proportion.[11] In particular, incorrect torque can impact the second order in clinical terms. Stamm et al.,[11] for instance, reported that a 10° inaccuracy in torque results in an average vertical deviation of 1.2 mm. This correlation is even more pronounced in the buccal region due to the greater positioning thickness. The German Institute of Standards and Norms (DIN 13971-2) specifies tolerances for bracket slots at between 0.0181 and 0.0197 in. The slot tolerance guaranteed by the manufacturer for the iLingual 3D bracket presented here is between 0.0160 and 0.0164 in. Each bracket slot is measured on completion of the production process with precise measuring instruments. If a slot is too small, it undergoes precision enlargement with a broach tool; if it is too large, the bracket is refabricated.
As the clinical examples show, the finishing of a lingual case can thus be performed with minimal or no additional bends.
CASE REPORTS
Case 1
Case of Cl I crowding with mild skeletal Cl III tendency, anterior crossbite and posterior crossbite in relation to 15 and 25 with C/O of unesthetic smile, case was treated with non-extraction mechanics with iLingual 3D appliance in both upper and lower arches [Figures 6-8].

- Case Report 1: Cl I malocclusion with crowding and anterior & posterior cross bite. Non extraction treated with Ilingual 3D appliance

- Case Report 1: Treatment progress

- Case Report 1: Intra oral pre-treatment-virtual set up-intra oral post-treatment
Case 2
Cl III Skeletal malocclusion with prognathic mandible and asymmetry crowding and anterior and posterior cross bite. Case was treated with nonextraction mechanics with iLingual 3D appliance and Orthognathic Surgery (B.S.S.O.) [Figures 9-11].

- Case Report 2: Cl III Skeletal malocclusion with prognathic mandible and asymmetry crowding and anterior & posterior cross bite non extraction treated with iLingual 3D appliance & orthognathic surgery ( B.S.S.O.)

- Case Report 2: Intra oral pre-treatment-virtual set uppres surgical orthodontic decompensation, surgical phase & post surgical orthodontics

- Intra oral pre-treatment-virtual set up-intra oral post-treatment
Case 3
Cl III malocclusion with severe crowding and anterior cross bite. Case refused surgical option was treated with camouflage treatment with retromolar TAD’s with iLingual 3D appliance and en-mass distillation of the mandibular dentition [Figures 12-14].
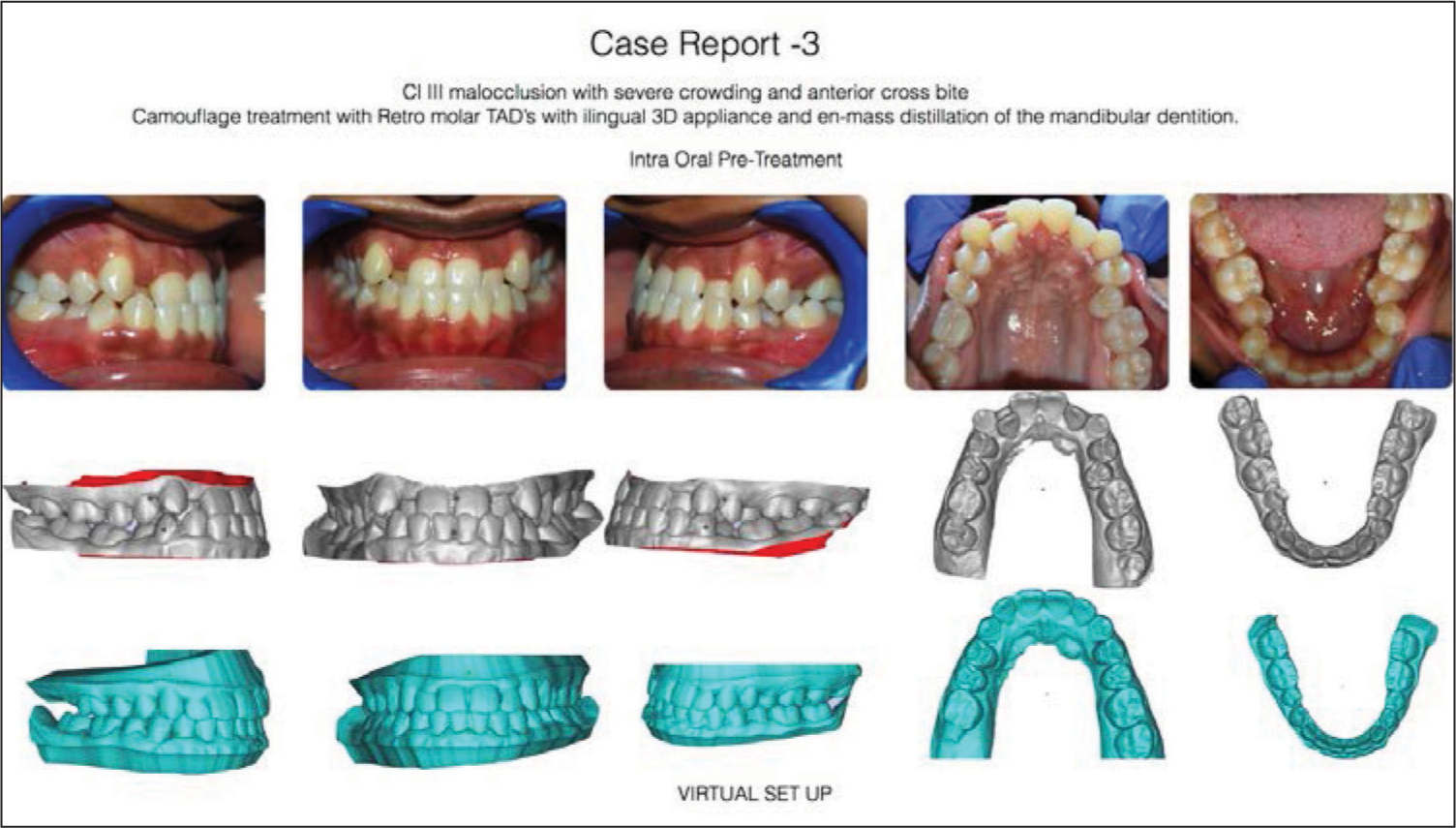
- Case Report 3: Cl III malocclusion with severe crowding and anterior cross bite Camoufl age treatment with Retro molar TAD’s with ilingual 3D appliance and en-mass distillation of the mandibular dentition
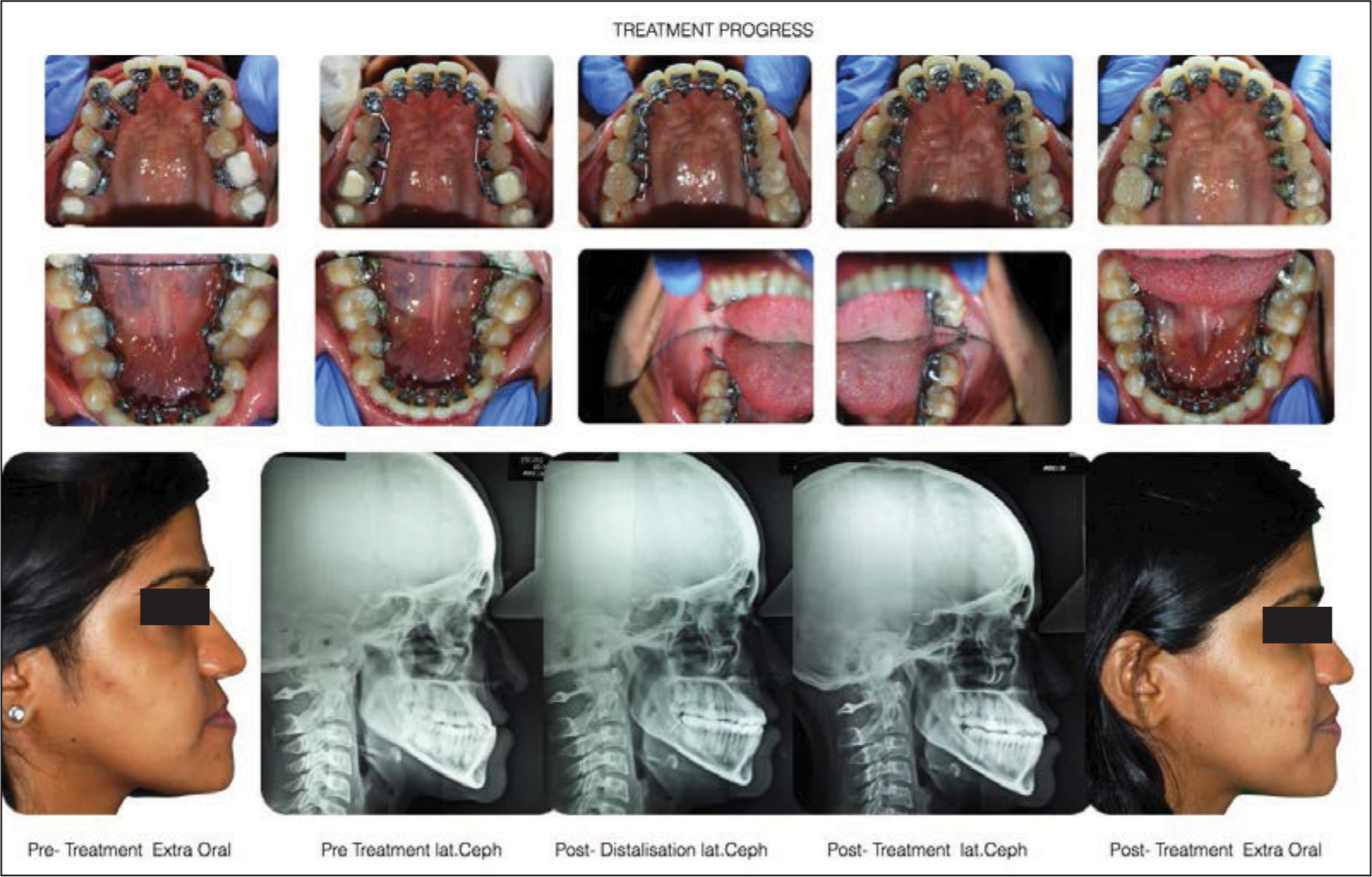
- Case Report 3: Treatment progress

- Case Report 3: Intra oral pre-treatment-virtual set up-intra oral post-treatment
Case 4
Cl I malocclusion with narrow arches, exaggerated buccal corridor with anesthetic smile treated with iLingual 3D appliance with improvement in arch forms by incorporating buccal root torque in premolars region for stability [Figure 15].

- Case Report 4: Cl I malocclusion with narrow arches, exaggerated buccal corridor with anaesthetic smile treated with iLingual 3D appliance with improvement in arch forms by incorporating buccal root torque in premolars region for stability
Some lingual orthodontic patients, especially those being treated in both arches, have speech problems and irritation of the tongue.[13,14,23-25] However, the reduced thickness of these brackets compared with traditional lingual brackets has made this much less of a problem [Figure 10]. Prospectively designed studies evaluating both subjective and objective perceptions are aimed at shedding further light on this matter.[26,27] The clinical track record to date underlines the positive infl uence of a lower-profi le lingual appliance both on articulation and on the extent of soft tissue irritation.
The chair side time is also reduced with ease of use of these customized appliances. The convenience of vertical insertion in anteriors, open second molar brackets instead of tubes, ease of rebondings, customized archwires provided for the full case from initial to final all help improve chair side efficiency and reduce appointment times. The preprogrammed appliances also help in reducing the frequency of appointments.
CONCLUSIONS
Custom bracket manufacturing provides new opportunities, especially in lingual orthodontics, by solving three of the most frequently cited drawbacks of lingual appliances: Difficult bonding and rebonding procedures and more frequent accidental debonding, difficult finishing processes, and patient discomfort.
The essential advantage of custom design and manufacturing is the unlimited individuality of the appliance. With the incorporation of tandem slot the vertical insertion ribbon arch appliance has become even more versatile overcoming the only drawback of inadequate tip control. iLingual 3D tandem slot appliance gives the operator the versatility of both vertical insertion and horizontal insertion in the anteriors and is one of the first custom appliances to offer this option. This seems to be the logical next step on the path to a lingual treatment concept adapted to both the patient and the orthodontist.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Fixed and removable appliances In: Proffit WR, ed. Contemporary Orthodontics (2nd ed). St. Louis: Mosby; 1993. p. :18-75.
- [Google Scholar]
- Lingual orthodontics: A status report. Part 6. Patient and practice management. J Clin Orthod. 1983;17:240-6.
- [Google Scholar]
- Lingual orthodontics — Its renaissance. Am J Orthod Dentofacial Orthop. 1989;96:120-37.
- [Google Scholar]
- Lingual orthodontics: Clinical reflections. Rev Orthop Dento Faciale. 1990;24:475-98.
- [Google Scholar]
- New orthodontic treatment with lingual bracket mushroom arch wire appliance. Am J Orthod. 1979;76:657-75.
- [Google Scholar]
- Resin core indirect bonding system — Improvement of lingual orthodontic treatment. J Jpn Orthod Soc. 1998;57:83-91.
- [Google Scholar]
- The use of lingual appliances for correction of bimaxillary protrusion (four premolars extraction) Am J Orthod Dentofacial Orthop. 1997;112:357-63.
- [Google Scholar]
- A simple lingual bracket (2D-control) for minor crowding and periodontal problems. J Ling Orthod. 2000;1:1-4.
- [Google Scholar]
- Relation between second and third order problems in lingual orthodontic treatment. J Ling Orthod. 2000;3:5-11.
- [Google Scholar]
- Discomfort caused by bonded lingual orthodontic appliances in adult patients as examined by retrospective questionnaire. Am J Orthod Dentofacial Orthop. 1999;115:83-8.
- [Google Scholar]
- Speech performance in lingual orthodontic patients measured by sonagraphy and auditive analysis. Am J Orthod Dentofacial Orthop. 2003;123:146-52.
- [Google Scholar]
- Lingual orthodontics (part 2): Archwire fabrication. J Orofac Orthop. 1999;60:416-26.
- [Google Scholar]
- Lingual orthodontics: A system for positioning the appliances in the laboratory. Orthod Fr. 1989;60(Pt 2):695-704.
- [Google Scholar]
- The customised lingual appliance set-up service (CLASS) system In: Romano R, ed. Lingual Orthodontics. Hamilton-London: B.C. Decker; 1998. p. :163-73.
- [Google Scholar]
- Lingual orthodontics (part 1): Laboratory procedure. J Orofac Orthop. 1999;60:371-9.
- [Google Scholar]
- Calibration Certificate No. K010549.3 Decom Prü Flabor. D-24376 Kappeln, Germany: GmbH & Co. KG;
- Lingual orthodontics (Part 3): Intraoral sandblasting and indirect bonding. J Orofac Orthop. 2000;61:280-91.
- [Google Scholar]
- Lingual technique — Patients’ characteristics, motivation and acceptance. Interpretation of a retrospective survey. J Orofac Orthop. 2002;63:227-33.
- [Google Scholar]
- Parametric and nonparametric assessment of speech changes in labial and lingual orthodontics: A prospective study. APOS Trends Orthod. 2013;3:99-109.
- [Google Scholar]
- Evaluation of the parameters underlying the decision by adult patients to opt for lingual therapy: An international comparison. J Orofac Orthop. 2003;64:135-44.
- [Google Scholar]
- Comparison of 3 bonded lingual appliances by auditive analysis and subjective assessment. Am J Orthod Dentofacial Orthop. 2003;124:737-45.
- [Google Scholar]
- Comparison of the effect on oral discomfort of two positioning techniques with lingual brackets. Angle Orthod. 2004;74:226-33.
- [Google Scholar]




