

Translate this page into:
Evaluation of treatment changes associated with maxillary molar distalization with the distal jet appliance
Address for correspondence: Dr. Ashok Karad, Smile Care, 1C/3-3, 2, Sujata Niwas, S. V. Road, Bandra (West), Mumbai - 400 050, Maharashtra, India. E-mail: drashokkarad@gmail.com
This article was originally published by Wolters Kluwer and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Objectives
Maxillary molar distalization is one of the non-extraction treatment options to gain space in the maxillary arch for the resolution of class II malocclusions. This retrospective clinical study was aimed at evaluating the nature of maxillary first molar movement after distalization with the distal jet and its effects on incisor position and facial soft-tissues.
Materials and Methods
The study sample consisted of 22 subjects (10 boys, 12 girls) having an average age of 13.04 years at the time of obtaining pre-treatment diagnostic records. The distal jet was the only appliance used during the distalization phase of treatment. All patients were treated by a single clinician with strict adherence to a standardized treatment protocol. The average duration of molar distalization was 6.09 months. Pre-treatment and postdistalization lateral cephalograms were obtained to analyze dentoalveolar and soft-tissue changes.
Results
This study revealed that the maxillary first molars were distalized by an average of 4.29 mm into a class I molar relationship. In the process, the molars exhibited distal molar tipping (6.66°) and extrusion (1.45 mm). The maxillary incisors were displaced and tipped labially by 1.89 mm and 2.84° respectively, leading to an increase in overjet by 0.86 mm and decrease in overbite by 0.98 mm. The soft-tissue changes involved upper and lower lip protrusion by 0.84 mm and 1.45 mm respectively, with an increase in lower facial height by 1.36 mm.
Conclusion
This study confirmed the reliable and effective distalization of maxillary first molars with the distal jet, with certain undesirable and reciprocal effects on incisor position and minimal impact on the facial soft-tissues.
Keywords
Class II malocclusion
distal jet
molar distalization
non-extraction approach

INTRODUCTION
Class II malocclusion is one of the most common problems encountered in orthodontic practice today. Advances in mechanotherapy and changes in treatment concepts and philosophies now minimize the need for extractions in mild to moderate discrepancies.[1] Non-extraction treatment of class II malocclusions, which are characterized by the absence of skeletal involvement, frequently requires distal driving of maxillary molars into a class I relationship. Several intraoral distalizing appliances have been introduced to eliminate the need for patient cooperation. The distal jet is a palatally placed, intra-arch maxillary molar distalization appliance.
AIM OF THE STUDY
The primary aim of this retrospective clinical study was to evaluate the nature of maxillary distal molar movement with the distal jet appliance alone and the secondary aim was to analyze its effects on incisor position and facial soft-tissues.
MATERIALS AND METHODS
This retrospective study was designed to evaluate cephalometrically the treatment changes associated with maxillary molar distalization with the distal jet appliance. The sample size for this study was calculated with a power analysis, which indicated that 20 patients were needed to achieve 80% power to detect clinically significant differences during various stages of treatment.
Patients with dental class II malocclusion were included in the study. Sample selection was based on the following inclusion and exclusion criteria.
Inclusion criteria
Bilateral Angle’s class II malocclusion (including division 1 and division 2) on skeletal class I bases.
Mild to moderate discrepancy in the upper arch.
Non-extraction treatment approach.
Normal or low mandibular plane (MP) angle cases.
Only distal jet used for distalization without any fixed appliance.
No breakage of distal jet during treatment.
Exclusion criteria
Previous orthodontic treatment.
Crossbites.
Vertical growth pattern.
Poor oral hygiene.
Missing or history of extraction of teeth.
Poor quality radiographs.
The sample for this retrospective study consisted of 22 patients (10 boys, 12 girls), from the author’s private orthodontic practice. The average age of the patients was 13.04 years (range, 9-20 years) at the beginning of the treatment. Out of all class II cases, eight cases had division 1 malocclusion, four had division 2 and ten exhibited crowding. The status of permanent second molars was variable, with 13 patients exhibiting fully erupted teeth, five with partially erupted teeth and in four cases, they were not erupted. All patients showed the presence of the permanent dentition except two, who were in the late mixed dentition stage with the presence of second deciduous molars.
All patients were started with the distal jet therapy by a single clinician following similar protocol in every patient. The appliance was cemented in the upper arch without any fixed appliance. Mean duration for distalization was 6.09 months, with a range of 4-10 months. Lateral cephalograms were obtained at the pre-treatment (T1) and postdistalization (T2) stages.
All cephalometric radiographs were traced and analyzed manually by a single examiner on acetate tracing paper of 50 micron thickness using 0.5 mm lead pencil under similar conditions of illumination. The important hard and soft-tissue landmarks were marked on the headfilm. The Horizontal plane (HP) was constructed at 7° to Sella-Nasion plane, at Nasion. For vertical reference, a vertical plane (VP) was drawn from Sella, perpendicular to HP. Dentoalveolar and soft-tissue changes were evaluated using 13 parameters (9 linear and 4 angular), as shown in Figure 1, at T1 and T2.
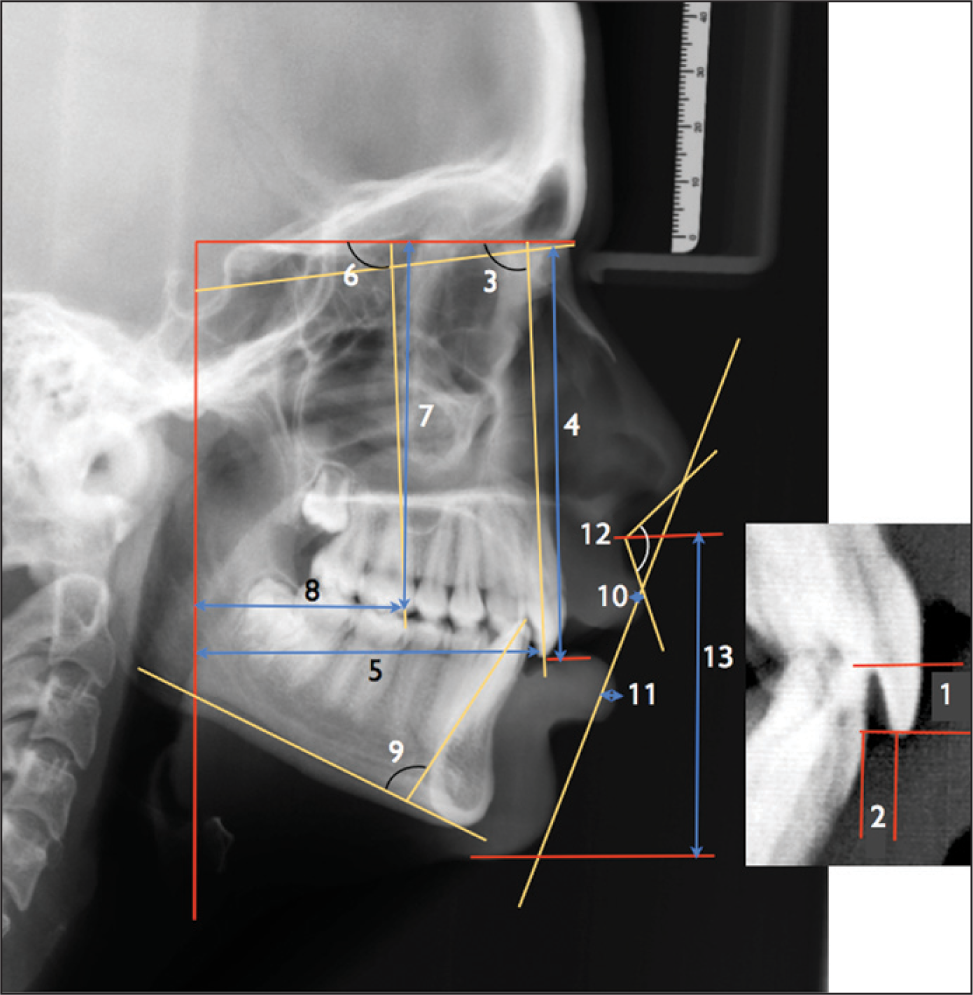
- Linear and angular cephalometric measurements 1. Overbite (mm); 2. Overjet (mm); 3. U1-Horizontal plane (HP) (°); 4. U1-HP (mm); 5. U1-Vertical plane (VP) (mm); 6. U6-HP (°) 7. U6-HP (mm); 8. U6-VP (mm); 9. L1-Mandibular plane (°); 10. Upper lip-E plane (mm); 11. Lower lip-E plane (mm); 12. Nasolabial angle (°); 13. Lower face height (mm)
Following parameters were used:
Overbite (OB) (mm).
Overjet (OJ) (mm).
U1 - Horizontal plane (HP) — Angle between maxillary central incisor and HP (degrees).
U1 - HP — Linear distance between maxillary central incisor tip and HP (mm).
U1 - VP — Linear distance between maxillary central incisor tip and VP (mm).
U6 - HP — Angle between maxillary first molar and HP (degrees).
U6 - HP — Linear distance between maxillary first molar and HP (mm).
U6 - VP — Linear distance between maxillary first molar and VP (mm).
L1 - MP — Angle between lower central incisor and MP (degrees).
Upper lip (UL) - E plane — Linear distance between UL and Rickett’s esthetic plane (mm).
Lower lip (LL) - E plane — Linear distance between LL and Rickett’s esthetic plane (mm).
Nasolabial angle (degrees).
Lower face height (LFH) - Soft-tissue lower anterior face height (mm).
Maxillary molar distalization protocol
All subjects in this study had undergone distal driving of maxillary molars using the distal jet appliance to gain space as a part of non-extraction treatment modality. The distal jet appliance is a palatally positioned, non-compliance appliance that uses a flexible molar distalization force system. Its use in these cases was based on several advantages like improved esthetics and comfort, simple activation, better molars control and easy conversion into a Nance holding arch to stabilize molars in their new positions after distalization.
The distal jet appliances used in this study were constructed in the laboratory and were carefully checked prior to their cementation, to make sure that they were fabricated as per the recommendations of the inventors of this appliance.[2,3]
It was constructed on an accurate and detailed working model with correctly placed and sized molar bands for precision fit and performance of the finished appliance. The lingual sheaths were positioned as cervically as possible on first molar bands. The bayonet assembly consisting of bayonets and bayonet directors was made parallel, as closely as possible, to the posterior part of the archform at the level of the centers of resistance of the posterior teeth [Figure 2a]. Vertically, it was parallel to the occlusal plane of the posterior teeth [Figure 2b].

- Standardized orientation of various components of the distal jet
A large Nance palatal button, antero-posteriorly extending from the distal of incisive papilla to the distal aspect of second bicuspid, and laterally extending parallel to the bayonets and directors was made. It was anchored by bondable connectors to the first bicuspids. A bayonet wire was inserted into the lingual sheath of each first molar band and the free end was inserted into the directors, much like a piston. A distal stop, nickel-titanium open coil springs on the bayonets, and the activation lock on the bayonet directors were placed as shown in Figure 2.
All cut ends of the bayonets were smoothened with carborundum disc for free sliding movement without friction. Before cementation, it was made sure that, all components of the appliance followed natural anatomical contours, were connected together passively and did not impinge soft tissues.
After cementation, the appliance was left passive in the patient’s mouth for 2 weeks. It was then activated by sliding the activation lock distally to compress the coil spring by 5-6 mm and generate a distally directed force of approximately 190 g. This was followed by reactivation at 4 week intervals.
Once the molars were distalized into a class I relationship, the distal jet appliance was converted into a modified Nance holding the arch by sealing the lock-spring assembly with flowable composite. Lateral cephalometric radiographs were then obtained for all subjects at this stage. Figures 3 and 4 demonstrate a case, where the maxillary molars were distalized from class II to class I relationship with the standardized protocol used in this study.

- Pre-treatment intraoral photographs

- Postdistalization intraoral photographs
Statistical analysis
Data was coded and entered into excel sheet which was later analyzed by using SPSS Inc. (Statistical Package for the Social Sciences) version 17.0. Descriptive statistics, i.e., mean and standard deviation were calculated for all variables before and after distalization. Wilcoxon sign rank test was used to compare the cephalometric changes after molar distalization. P < 0.05 was considered as statistical significant at 95% of confidence interval.
All radiographs were traced a second time after an interval of 2 weeks and the values were rechecked for error analysis. Systematic bias was examined using a paired t-test and estimation of random error was done with the index of reliability by correlating repeat measurements. Error analysis showed no significant differences when systematic bias was tested (P < 0.05) and correlations were found to be greater than 0.95, indicating no random error.
RESULTS
This comparative study, using lateral cephalograms of 22 subjects, evaluated the treatment changes associated with maxillary molar distalization with the distal jet appliance. It showed a significant amount of change in the position of molars, incisors and soft-tissues after distalization when compared to the initial values as shown in Table 1.
| Variables | Before (T1) | After (T2) | T1-T2 | P value |
|---|---|---|---|---|
| Mean ± SD | Mean ± SD | Mean ± SD | ||
| Overjet (mm) | 4.09±2.09 | 4.95±2.37 | −0.86±1.51 | 0.013* |
| Overbite (mm) | 3.70±1.88 | 2.73±2.24 | 0.98±1.017 | 0.000** |
| Upper incisor — HP (°) | 115.61±9.06 | 118.45±10.35 | −2.84±4.50 | 0.011* |
| Upper incisor — HP (mm) | 78.36±5.24 | 79.59±5.47 | −1.23±2.6 | 0.066 |
| Upper incisor — VP (mm) | 71.57±6.02 | 73.45±6.07 | −1.89±2.42 | 0.002* |
| Upper molar — HP (°) | 83.11±7.62 | 76.45±6.82 | 6.66±5.12 | 0.000** |
| Upper molar — HP (mm) | 73.55±4.81 | 75.00±4.54 | −1.45±1.61 | 0.001* |
| Upper molar — VP (mm) | 38.75±5.14 | 34.41±4.83 | 4.295±0.66 | 0.000** |
| Lower incisor — MP (°) | 101.11±7.67 | 99.77±7.6 | 1.34±2.97 | 0.053 |
| UL-E plane (mm) | −3.00±2.63 | −2.16±2.3 | 0.84±1.87 | 0.027* |
| LL-E plane (mm) | −1.63±3.54 | −0.227±3.32 | 1.45±2.22 | 0.006* |
| NLA (°) | 99.14±10.67 | 99.39±10.06 | −0.25±7.64 | 0.638 |
| LFH (mm) | 65.84±4.124 | 67.57±4.8 | −1.36±3.4 | 0.029* |
*Significant (P < 0.05); **Highly significant (P < 0.001); HP – Horizontal plane; VP – Vertical plane; NLA – Nasolabial angle; LFH – Lower facial height; SD – Standard deviation
Molar changes
Maxillary molars showed significant changes in both HP and VPs after distalization. The maxillary first molars were distalized by an average of 4.29 ± 0.66 mm, tipped distally by 6.66° ± 5.12, with a significant amount of extrusion, i.e., 1.45 ± 1.61 mm.
Incisor changes
Significant changes were observed in the position of upper incisors. There was a significant increase in the angulation of incisors (2.84 ± 4.5°) with respect to HP resulting in increased OJ (0.86 ± 1.51 mm) and decreased overbite (0.98 ± 1.01 mm). They also showed significant labial movement (1.89 ± 2.42 mm), with mild extrusion which was insignificant.
Lower incisor position did not change much with respect to the MP during distalization.
Soft tissue changes
Both UL and LL showed statistically significant forward positioning after distalization (0.84 ± 1.87 mm and 1.45 ± 2.2 mm respectively), with LL moving more forward than the UL. Even the lower facial height was increased significantly (1.36 ± 3.4 mm), but no changes were observed in the nasolabial angle.
Some of these significant dentoalveolar changes are shown in the Figures 5 and 6.

- Molar and incisor changes after distalization

- Mean values of six key parameters before and after distalization
DISCUSSION
Patient cooperation is one of the most important elements in orthodontic treatment success.[4] However, it has been reported that patient cooperation with prescribed intraoral and extraoral appliances like removable functional appliances, intermaxillary elastics, headgears, etc. is unpredictable.[5,6] Considering this, several fixed intra-arch distalizing appliances have been introduced to eliminate the need for patient compliance, and to achieve more predictable results. Some of the intra-arch maxillary molar distalizing modules that reduce the need for patient cooperation are pendulum appliance,[7] Karad’s Integrated Distalization System,[8] repelling magnets,[9] Jones jig[10] and distal jet appliance.[2] Though these appliances require minimal patient cooperation, several studies have reported adverse treatment effects like maxillary first molar tipping and anchor loss while molars are being distalized into a Class I relationship.[11,12]
Among these appliances, the distal jet — a palatal, non-compliance, intra-arch, maxillary molar distalization appliance, is considered to have several distinct advantages.[3] The maxillary molars are driven distally with less tipping and palatal displacement of molars, and there is no need to construct a separate holding appliance as the same appliance can be easily converted into a holding appliance to stabilize the molars into their new positions after distalization. Few studies have analyzed the dentoalveolar and skeletal changes after distalization of molars with the distal jet.[13-15]
This retrospective clinical study was carried out using a sample of 22 Class II patients, to evaluate treatment changes associated with maxillary molar distalization with the distal jet. The dentoalveolar and soft-tissue changes were carefully analyzed using pre-treatment and postdistalization lateral cephalograms.
The results of this study revealed that the distal jet effectively drives maxillary molars distally; however, this is associated with some undesirable effects like distal molar tipping and extrusion, maxillary incisor proclination leading to increased OJ, protrusion of lips and increased lower facial height. The main goal of molar distalization therapy with any distalizing appliance is to produce a translation type of distal molar movement with minimal untoward effects. In this study, at T2, a class I molar relationship was achieved, on an average, in 6.09 months.
This study demonstrated significant distal displacement of maxillary first molars, i.e., an average of 4.29 mm. Other studies on the distal jet, reported the distalization of molars as 2.1 mm,[13] 3.2 mm[14] and 2.8 mm.[15]
The amount of distal tipping of the molars relative to the horizontal reference plane was 6.660. Whereas, according to others, it was 3.3°,[13] 3.1°,[14] and 5°.[15] At first glance, the distal tipping of the molar, produced by the distal jet in this study seemed to be relatively greater than other studies. However, when greater amount of distal molar translation (4.29 mm) is compared with the amount of molar tipping, the result indicated that the first molars were, in fact, tipped distally by 1.55°/mm of distal tooth movement. This was less than that reported by Bussick and McNamara[16] for the pendulum (1.9°/mm) and Ngantung et al.[13] for the distal jet with full fixed appliances (1.6°/mm). However, it is greater than that reported by Bolla et al.[14] for the distal jet without full fixed appliances (1°/mm).
The distalized maxillary first molars in this study demonstrated statistically significant extrusion (1.45 mm). Other studies reported this finding in the range of 0.2-1 mm.[14,15,17]
Anchorage preservation is critical during maxillary molar distalizaion. The anchorage support in all subjects in this study comprised of the first premolar support and use of a large acrylic Nance palatal button to distribute reactive anterior forces generated from the activation of the coil springs, over a large area of the palate. The results of this study also revealed significant changes in the incisor position. The maxillary incisors were labially displaced and proclined, suggestive of anchorage loss. They were moved anteriorly by 1.89 mm and were tipped anteriorly by 2.84°. These findings were similar to that reported by Bolla et al.[14], i.e., 1.3 mm and 3.1° respectively. However, other studies reported greater anchorage loss; 12.2° by Ngantung et al.,[13] and 3.7 mm and 13.7° by Chiu et al.[15] A greater degree of labial incisor tipping in these studies may be attributed to the simultaneous use of full bracketed appliances. The incisor changes observed in this study resulted in increase in OJ by 0.86 mm and reduction in overbite by 0.98 mm. In other studies,[13,15] OJ increase was 1.7 and 2.4 mm respectively while Bolla et al.[14] noticed no change in the OJ and overbite. These changes in the maxillary incisor position clearly indicate that this anchorage system cannot completely resist the reactive anterior force generated as a result of activation of the distal jet. In spite of reducing the force levels used for distalization, anchorage control was not effective with the mechanotherapy employed.
With the dentoalveolar change, soft tissues also moved considerably. Both lips showed protrusion, with LL moving more than the upper. The lower anterior face height (soft tissue) also increased significantly. These soft tissue changes were in accordance with other studies.[13,15]
Distal jet was compared with other appliances in various studies. As reported by Ghosh and Nanda,[12] distalization of molars with pendulum was less (3.37 mm), with more of tipping (8.36°) when compared to our results, whereas anchor loss was similar (2.55 mm, 1.29°). No change was observed in the VP of molars while premolars showed little extrusion (1.7 mm). Soft-tissues showed similar response as with the distal jet in this study, with anterior movement of both lips and increased lower anterior face height.
In other study with pendulum,[15] molars showed greater distal movement (6.1 mm) and distal tipping (10.7°) with lesser extrusion (0.5-1 mm), whereas anteriors showed lesser anchor loss (1.1 mm mesial movement and 3.1° labial flaring) than this study. However, LL and LFH showed a similar pattern of change.
Though a study by Fuziy et al.[18] observed very significant molar distalization (4.6 mm) with the pendulum appliance, the amount of distal tipping was too much (18.5°). There was comparable amount of anchor loss seen in incisors in the form of 1.11 mm of mesial movement and 2.84° of labial tipping as well as significant incisor extrusion (1.14 mm).
The results of this study with the distal jet are quite similar to the results of First class appliance by Papadopoulos et al.,[19] with a similar amount of distalization (4 mm), anchor loss (1.86 mm), increased OJ (0.68 mm) and no change in the vertical dimension of incisors. However, greater amount of distal tipping of molars (8.56°) was observed with First class appliance.
The use of skeletal anchorage systems has become a new orthodontic treatment strategy over the past decade. In a study by Yamada et al.,[20] upper molars were moved to the distal using miniscrews placed in between the second premolar and the first molar. Though the molars were moved distally just by 2.8 mm with distal tipping of 4.8°, incisors were actually moved distally and showed palatal tipping contrary to our study. Another study,[21] miniscrews used along with distal jet for additional anchorage were effective in carrying out bodily movement of molars (3.92 mm).
When compared to our study, very high distalization amounts (5.9 mm) were seen with predominant bodily movement, when mini implants were used with dual-force distalizer.[22] The premolars and anterior teeth followed the distal movement of the molars with no loss of anchorage. Similar results were observed with lever arm and mini implant system, which control the point of force application and produce the desirable three-dimensional control of molars during distal molar movement.[23]
In a recent study,[24] molar distalization was carried out with zygoma-gear appliance, which consisted of a zygomatic anchorage miniplate. The molar showed distalization in amounts similar to our study (4.37 mm), however, the amount of tipping was quite less (3.3°) and the molars showed intrusion. Another finding which was significant was that there was palatal tipping and a decrease in OJ, indicating that there was no anchorage loss. Similar results were observed by Kilkis et al.,[25] where the zygoma-gear appliance was used for unilateral distalization.
CONCLUSION
The results of this study, based on the analysis of pretreatment and postdistalization lateral cephalograms of 22 patients with class II malocclusion treated with the distal jet appliance, suggest that the maxillary first molars were distalized by a significant amount into a class I relationship. However, in the process of distalization, the distal jet did produce certain undesirable and reciprocal effects on incisor position with minimal impact on the facial soft-tissues.
ACKNOWLEDGMENT
We would like to sincerely thank Dr. Sonal Kothari for the statistical help and assessment.
Source of Support:
Nil.
Conflict of Interest:
None declared.
References
- Sagittal discrepancies In: Karad A, ed. Clinical Orthodontics: Current Concepts, Goals and Mechanics. New Delhi: Elsevier; 2010. p. :67-109.
- [Google Scholar]
- Iatrogenic problems associated with the clinical practice orthodontics In: McNamara JA Jr, Trotman C, eds. Orthodontic Treatment: The Management of Unfavourable Sequelae, Craniofacial Growth Series. Vol 31. Ann Arbor, Michigan: Center for Human Growth and Development, The University of Michigan; 1996. p. :1-28.
- [Google Scholar]
- Prediction of cooperation in orthodontic treatment. Am J Orthod Dentofacial Orthop. 1992;102:15-21.
- [Google Scholar]
- The pendulum appliance for Class II non-compliance therapy. J Clin Orthod. 1992;26:706-14.
- [Google Scholar]
- Rapid Class II molar correction with an open-coil jig. J Clin Orthod. 1992;26:661-4.
- [Google Scholar]
- Evaluation of an intraoral maxillary molar distalization technique. Am J Orthod Dentofacial Orthop. 1996;110:639-46.
- [Google Scholar]
- Posttreatment evaluation of the distal jet appliance. Am J Orthod Dentofacial Orthop. 2001;120:178-85.
- [Google Scholar]
- Evaluation of maxillary molar distalization with the distal jet: A comparison with other contemporary methods. Angle Orthod. 2002;72:481-94.
- [Google Scholar]
- A comparison of two intraoral molar distalization appliances: Distal jet versus pendulum. Am J Orthod Dentofacial Orthop. 2005;128:353-65.
- [Google Scholar]
- Dentoalveolar and skeletal changes associated with the pendulum appliance. Am J Orthod Dentofacial Orthop. 2000;117:333-43.
- [Google Scholar]
- Maxillary molar distalization with noncompliance intramaxillary appliances in Class II malocclusion. A systematic review. Angle Orthod. 2008;78:1133-40.
- [Google Scholar]
- Sagittal, vertical, and transverse changes consequent to maxillary molar distalization with the pendulum appliance. Am J Orthod Dentofacial Orthop. 2006;130:502-10.
- [Google Scholar]
- Noncompliance maxillary molar distalization with the first class appliance: A randomized controlled trial. Am J Orthod Dentofacial Orthop. 2010;137:586.e1-58613.
- [Google Scholar]
- Distal movement of maxillary molars using miniscrew anchorage in the buccal interradicular region. Angle Orthod. 2009;79:78-84.
- [Google Scholar]
- Efficiency of a skeletonized distal jet appliance supported by miniscrew anchorage for noncompliance maxillary molar distalization. Am J Orthod Dentofacial Orthop. 2009;136:578-86.
- [Google Scholar]
- Maxillary molar distalization with the dual-force distalizer supported by mini-implants: A clinical study. Am J Orthod Dentofacial Orthop. 2009;135:282.e1-5.
- [Google Scholar]
- Distal movement of maxillary molars using a lever-arm and mini-implant system. Angle Orthod. 2008;78:167-75.
- [Google Scholar]
- Effects of maxillary molar distalization with Zygoma-Gear Appliance. Angle Orthod. 2012;82:596-602.
- [Google Scholar]
- Unilateral maxillary molar distalization with zygoma-gear appliance. Am J Orthod Dentofacial Orthop. 2012;142:e1-7.
- [Google Scholar]




