

Translate this page into:
Miniscrews as an alternative for orthopedic traction of the maxilla: A case report

*Corresponding author: Ricardo Alves de Souza, Department of Orthodontics, Universidade Estadual do Sudoeste da Bahia, Jequie, Bahia, Brazil. ricardoorto@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Souza RA, Dourado GB, Farias IM, Pithon MM, Neto JR, de Paiva JB. Miniscrews as an alternative for orthopedic traction of the maxilla: A case report. APOS Trends Orthod 2020;10(1):132-8.
Abstract
The aim of this study was to report the case of a Class III prepuberal patient treated by a maxillary protraction using four miniscrews. The screws were installed between maxillary first molars and second premolars and between mandibular canines and first premolars. A 1/4˝ intermaxillary elastics were used in both sides, ligating the upper-lower screws to perform a maxillary protraction and correction of the Class III malocclusion. A bite plate made by resin flow was made on lingual surfaces of the mandibular incisors to eliminate occlusal interference. After 16 months of treatment, it was possible to see a significant improvement of patient’s facial profile, with overcorrection in overjet and preservation of the tissues and integrity of dental roots.
Keywords
Angle Class III malocclusion
Maxillary retrusion
Orthodontic anchorage procedures
Facemask

INTRODUCTION
The treatment of patients who present Class III malocclusion with maxillary deficiency, using skeletal anchorage with miniplates for maxillary protraction has been shown in several studies.[1-5] The results obtained by computed tomography demonstrated that the use of these devices transferred the forces directly to the sites of maxillary sutures, improving the orthopedic effect, due to the force not being dissipated in the periodontal ligament.[6] Therefore, this protocol has advantages in comparison with conventional facemask therapy because it prevents the undesirable effects of tooth movement, such as maxillary molar mesialization and extrusion; maxillary incisor protrusion and mandibular incisor retroinclination;[1-5,7-9] and mandibular rotation in the clockwise direction[10] and eliminates possible limitations imposed by patients’ rejection to use a facemask.[11,12]
De Clerck et al.[2,3] used titanium miniplates, temporary anchorage devices, and intermaxillary elastics so that the maxillary protraction forces would act directly on the bony structures during the orthopedic treatment of Class III patients. Souza et al.[13] used a similar mechanic using miniscrews, avoiding surgical step of miniplates placement, with great results in maxillary protraction and facial pattern Improvement.
Considering these aspects, it was decided to perform a maxillary protraction supported by miniscrews as an alternative to the miniplates therapy.
DIAGNOSIS
The patient, a 10-year-old girl, leukoderm, mesofacial, with concave profile due to maxillary deficiency, greater exposure of the lower incisors when smiling, medium buccal corridor, and no passive lip sealing, reported that her smile and teeth were ugly, and her chin was big. During the intrabuccal examination, she presented a negative overjet, absence of space for maxillary second premolars that caused migration of the first maxillary molars and an Angle’s Class II relationship. Her maxillary first premolars were also rotated and there was a little crowding of the mandibular incisors [Figure 1].

- Initial clinical aspect of the patient.
The panoramic radiograph showed the presence of included maxillary second premolars; carpal examination showed closure to the prepubertal growth spurt. The cephalometric tracings and measurements confirmed the skeletal Class III pattern with maxillary retrusion and good mandible positioning [Figure 2 and Table 1].
| Norm | T0 | T1 | T2 | T3 | |
|---|---|---|---|---|---|
| SNA (°) | 82° | 78° | 82° | 83° | 83° |
| SNB (°) | 80° | 83° | 82° | 82° | 83° |
| ANB (°) | 2° | ‒5° | 0 | 1 | 0 |
| Wits (mm) | ‒1 mm(♂) 0 (♀) | ‒7 mm | ‒2 mm | ‒1 mm | ‒2 mm |
| SN-PP (°) | 8.5° | 13° | 11° | 11° | 11° |
| FMA (°) | 25° | 18° | 17° | 18° | 17° |
| SN-GoGn (°) | 32° | 27° | 25° | 25° | 25° |
| 1.1 (°) | 131° | 123° | 124° | 127° | 127° |
| 1.NA (°) | 22° | 35° | 37° | 36° | 36° |
| 1-NA (mm) | 4 mm | 9 mm | 9 mm | 8 mm | 8 mm |
| 1.NB (°) | 25° | 27° | 25° | 25° | 25° |
| 1-NB (mm) | 4 mm | 4 mm | 4.5 mm | 4 mm | 4 mm |
| NAP (°) | 0 | 10° | 7° | 7° | 7° |
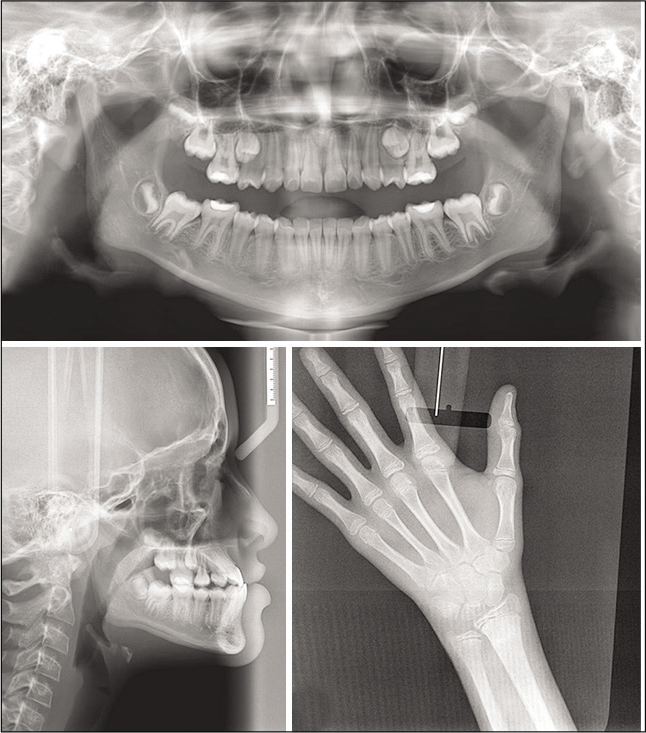
- Initial radiographic images.
The etiological factors of deficiency of the patient’s middle third of the face presented strong hereditary relationships that were possible to perceive when talking to her parents during the initial examinations.
TREATMENT PLAN AND PROGRESS
Considering the possibility of taking advantage of the patient’s growth spurt, an alternative treatment plan was proposed aiming to protrude the maxilla to correct the dentofacial imbalance.
For this purpose, conventional orthodontic miniscrews (Morelli, Sorocaba, Brazil) were placed in the mesial site of the maxillary permanent first molars and in the distal region of the mandibular canines. The threadable part of the miniscrews used was 10 mm long, with a screw thread diameter of 1.5 mm and transmucous section of 2 mm. In the treatment plan, it was decided to remove the included second premolars to increase the amount of space for inserting the maxillary miniscrews.
Just after the miniscrews insertion, 1/4˝ intermaxillary elastics (Morelli, Sorocaba, Brazil) were fitted with a light force next to 100 g. After 30 days, the patient was instructed to use 1/4˝ intermaxillary elastics with medium force of approximately 200 g, and when she opened her mouth, this increased to about 230 g. Resin flow was used on the lingual surfaces of mandibular incisors to eliminate the occlusal interference [Figure 3]. The patient was instructed to replace the elastics once a day, and from this stage onward, monthly follow-up appointments were made.
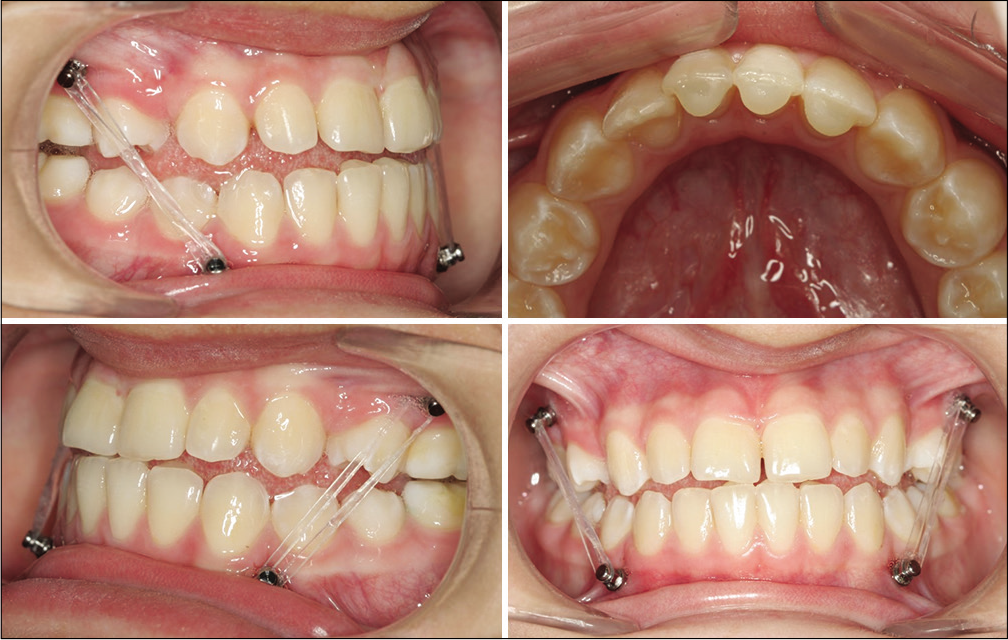
- Mini-implants in position supporting the elastics.
TREATMENT RESULTS
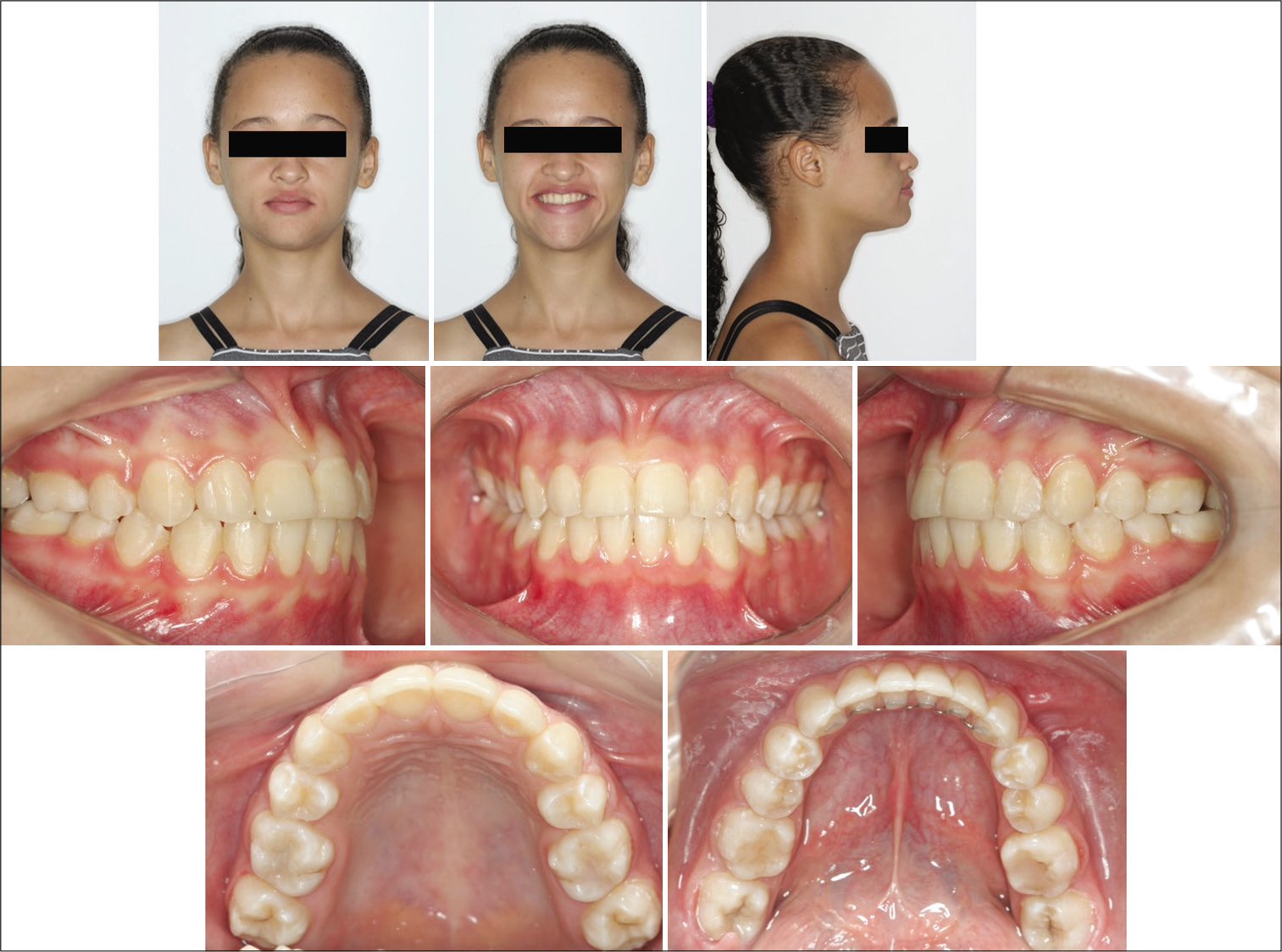
After 16 months, the orthopedic phase and retention have ended. It was possible to verify a significant improvement in the patient’s facial profile, which became smoothly convex, the tissues, integrity of the dental roots, and that the patient had already surpassed the growth spurt [Figures 4 and 5].

- Final clinical aspect after orthopedic treatment.
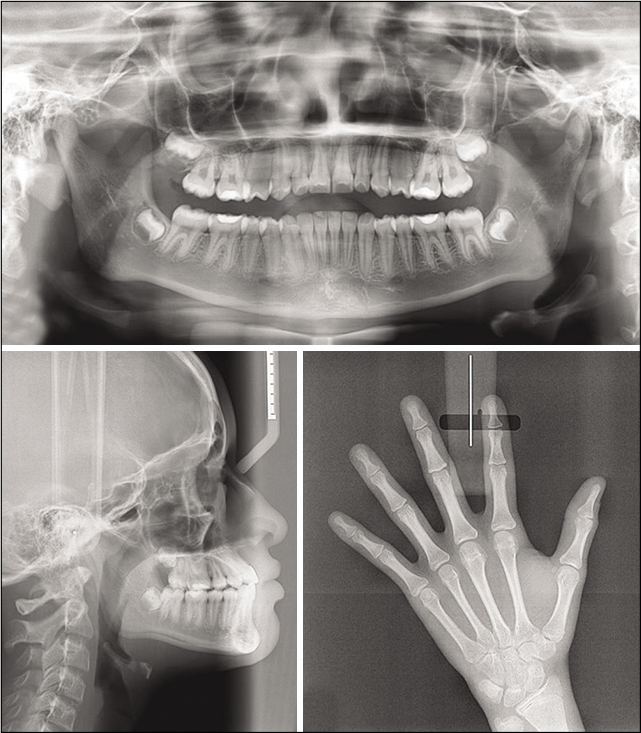
- Final radiographic images after orthopedic treatment.
The superimposition [Figure 6] and T1 cephalometric measurements [Table 1] showed an improvement in the profile and a greater protraction of the maxilla, as well as of the maxillary molars and incisors when compared with those of the mandible. There was also a slight counterclockwise rotation of the maxilla.
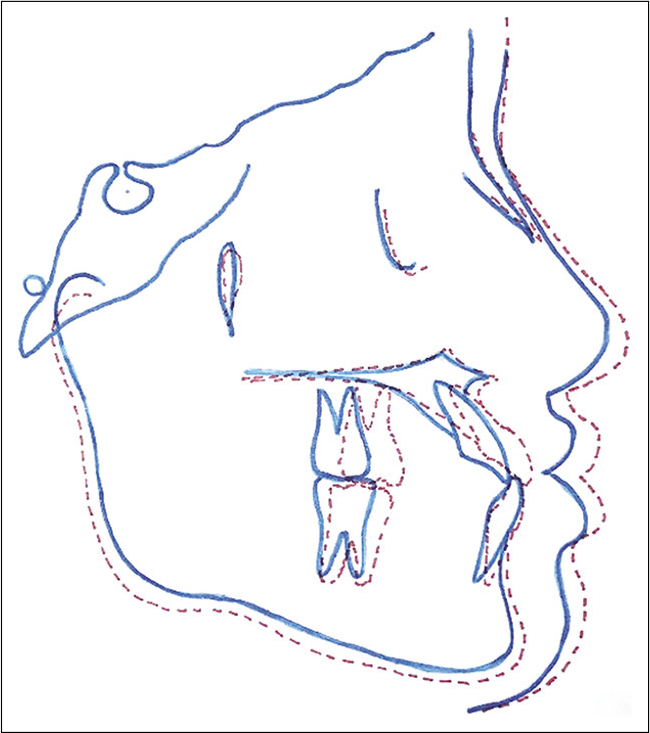
- Superimposition before and after maxillary protraction treatment showing the point A has moved further forward than point B, and a discrete anti-clockwise rotation that occurred in the palatine plane.
Metallic braces (Dental Morelli, Sorocaba, São Paulo), Roth prescription, slot 0.022”, were bonded, starting orthodontic phase that lasted 12 months [Figure 7]. Some small corrections were performed to grant the correct occlusion fittings. After orthopedic and orthodontic phase was performed, the occlusion showed stability after 2 years follow-up [Figure 8]. [Table 1] shows the cephalometric measures before and after all treatments.
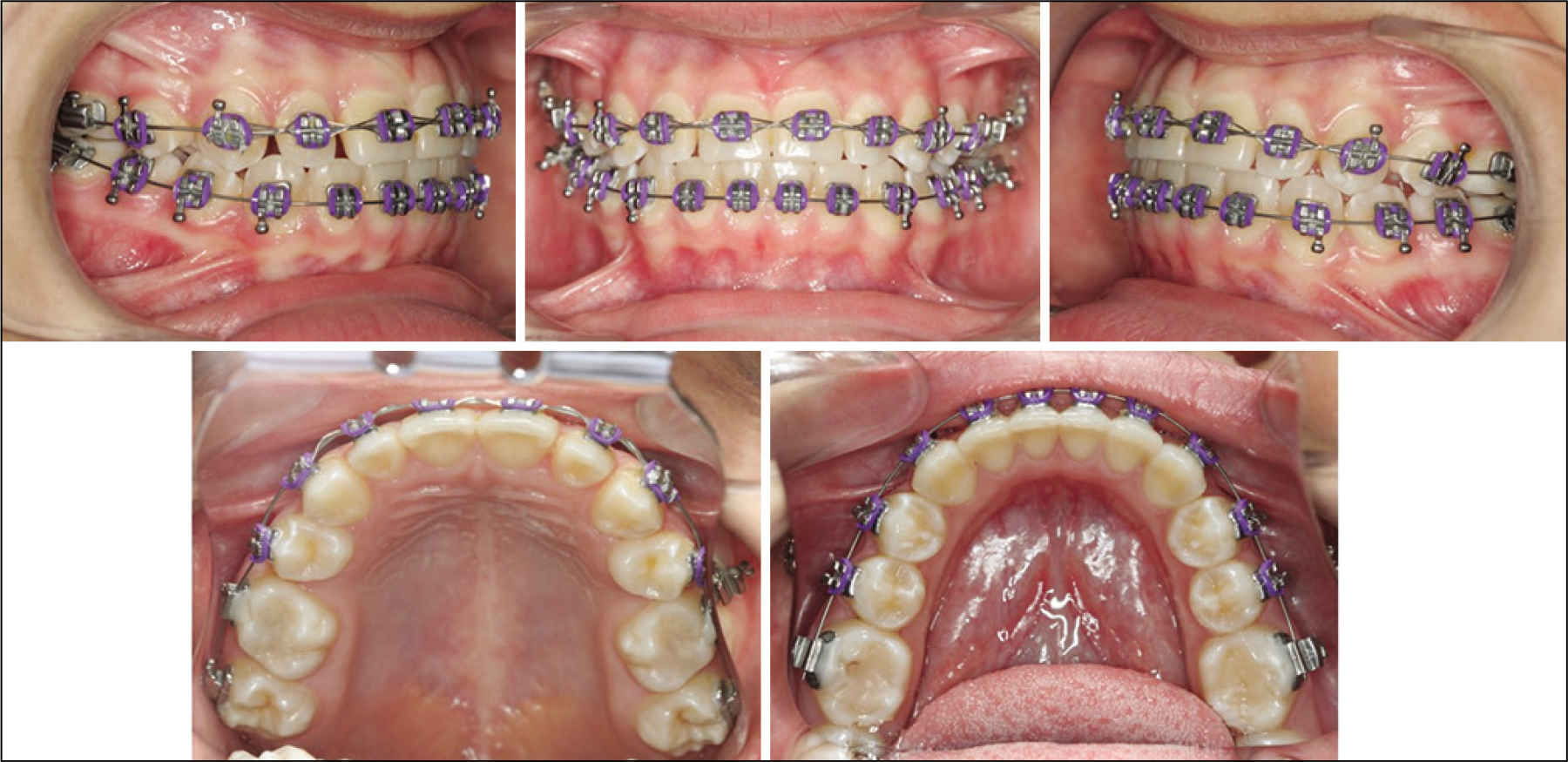
- Orthodontic treatment on course.
- Final clinical aspect 2 years after orthodontic treatment.
DISCUSSION
The use of skeletal anchorage for facial orthopedic treatment[1-5] has been shown a promising option compared with traditional protocols, in patients with Class III due to maxillary deficiency. However, some situations may be difficult to control by the professional, like convincing the parents and patients of the surgical stages required for installing and removing the miniplates, especially in children. Aware of this situation, the authors decided to use orthodontic miniscrews instead of miniplates in the case reported, showing satisfactory results.
In this case, the main doubt was about the capability of the miniscrews to support the higher forces during orthopedic treatment. Some authors[1,2] highlighted that miniplates are not completely stable during orthodontic treatment, with a failure rate around 7%. These failures arise from tissue irritation and infection, generating with the cusp tip of the maxillary canine tooth tending to the mesial in relationship with the mandibular canine. There was a slight overcorrection in the patient’s overjet at the end of the treatment. The final radiograph showed preservation of inflammation and peri-implant bone loss, causing destabilization of the miniplates.[14,15] Souza et al.[13] related that 16.7% miniscrews were lost in the treatment, a lower tax, considering the facility of placing the miniscrews and the no surgical step to install them. In the case presented, no miniscrews have failed. Light and continuous forces were used throughout the treatment, and the miniscrews chosen were thicker and larger in size, with the intention of increasing the area of contact with the bone, and possibly increase the stability during the use of intermaxillary elastics. Other difficulties related were the presence of the included maxillary second premolars at the beginning of treatment. However, it was decided to remove them because the spaces were almost completely closed, and the patient would have ended the treatment with molar relationship in Class II.
Rapid maxillary expansion (RME), a procedure widely accepted for Class III treatment, provides destabilization of the maxillary sutures, which optimizes maxillary protraction.[16-18] Some recent studies related the correction of Class III malocclusion with and without RME, pointing out that this step was not mandatory before maxillary protraction.[19] The answer to this question was well justified in the study of Cha and Ngan,[19] in which miniplates were used as support for the facemask, and the results demonstrated that there were far fewer effects on teeth and vertical alterations in the group without RME. The patient related had no significant transverse alterations, so was chosen to not perform REM. In this case, after extractions of the included maxillary second premolars, it was possible to insert the maxillary miniscrews and to begin with protrusion of the maxilla using intermaxillary elastics.
According to some authors,[20-22] maxillary protraction with anchorage supported on teeth is usually accompanied by rotation of palatine plane, and downward and backward rotation of the mandible, resulting in an attempt to improve the skeletal relationship. Another side effect was loss of arch length as a result of mesial movement of the posterior teeth – especially in mixed dentition – and dental extrusion, inclination, and increase in vertical dimension.[21]
As shown in [Table 1], cephalometric values of the patient presented a significant improvement in many measures. SNA increased from 78° to 82° and ANB from –5° to 0. Wits reduced from ‒7 mm to ‒2 mm, and the patient’s facial pattern remained stable with a slight variation of FMA and SN-GoGn. Cephalometric measures remained stable even after 2 years of orthopedic treatment. In the cephalometric superimposition, the effect of maxillary protraction was much greater than the downward displacement – very common in the facemask protocol – which could increase the patient’s facial height. Counterclockwise rotation of the palatine and mandibular plane was moderate, similar to the study of De Clerck et al.[1]
It is possible to state that patient’s cooperation with this protocol was greater than it would be with the use of the facemask, with a positive reflection on the psychosocial aspect. The force used for maxillary traction with miniscrews, using intermaxillary elastics, may be better tolerated by patients for 24 h/day. Whereas, use of the facemask requires greater cooperation from patients because it involves prejudice in children’s social lives.[12] Another important point was the greater facility and lower level of discomfort in the procedure of miniscrews placement, when compared with miniplates. However, further studies such as clinical trials with significant samples will be necessary to confirm the use of miniscrews as an anchorage option for maxillary protraction in Class III patients.
CONCLUSION
It was possible to observe maxillary advancement in the patient, indicating that maxillary protraction with mini- implants can be possible.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Orthopedic traction of the maxilla with miniplates: A new perspective for treatment of midface deficiency. J Oral Maxillofac Surg. 2009;67:2123-9.
- [CrossRef] [PubMed] [Google Scholar]
- Dentofacial effects of bone-anchored maxillary protraction: A controlled study of consecutively treated Class III patients. Am J Orthod Dentofacial Orthop. 2010;138:577-81.
- [CrossRef] [PubMed] [Google Scholar]
- Comparison of two protocols for maxillary protraction: Bone anchors versus face mask with rapid maxillary expansion. Angle Orthod. 2010;80:799-806.
- [CrossRef] [PubMed] [Google Scholar]
- Three-dimensional assessment of maxillary changes associated with bone anchored maxillary protraction. Am J Orthod Dentofacial Orthop. 2011;140:790-8.
- [CrossRef] [PubMed] [Google Scholar]
- Three-dimensional analysis of maxillary changes associated with facemask and rapid maxillary expansion compared with bone anchored maxillary protraction. Am J Orthod Dentofacial Orthop. 2013;144:705-14.
- [CrossRef] [PubMed] [Google Scholar]
- Midfacial protraction with skeletally anchored face mask therapy: A novel approach and preliminary results. Am J Orthod Dentofacial Orthop. 2008;133:440-9.
- [CrossRef] [PubMed] [Google Scholar]
- Treatment response and long-term dentofacial adaptations to maxillary expansion and protraction. Semin Orthod. 1997;3:255-64.
- [CrossRef] [Google Scholar]
- Sagittal changes after maxillary protraction with expansion in Class III patients in the primary, mixed, and late mixed dentitions: A longitudinal retrospective study. Am J Orthod Dentofacial Orthop. 2000;117:669-80.
- [CrossRef] [PubMed] [Google Scholar]
- Postpubertal assessment of treatment timing for maxillary expansion and protraction therapy followed by fixed appliances. Am J Orthod Dentofacial Orthop. 2004;126:555-68.
- [CrossRef] [PubMed] [Google Scholar]
- Cephalometric effects of face mask/expansion therapy in Class III children: A comparison of three age groups. Am J Orthod Dentofacial Orthop. 1998;113:204-12.
- [CrossRef] [Google Scholar]
- Correction of Class III malocclusion using modified tandem appliance-two case reports. J Indian Soc Pedod Prev Dent. 2013;31:286-91.
- [CrossRef] [PubMed] [Google Scholar]
- Mechanical evaluation of orthodontic mini-implants of different lengths. J Oral Maxillofac Surg. 2013;71:479-86.
- [CrossRef] [PubMed] [Google Scholar]
- Maxillary protraction with rapid maxillary expansion and facemask versus skeletal anchorage with mini-implants in Class III patients: A non-randomized clinical trial. Prog Orthod. 2019;20:35.
- [CrossRef] [PubMed] [Google Scholar]
- Factors associated with the stability of titanium screws placed in the posterior region for orthodontic anchorage. Am J Orthod Dentofacial Orthop. 2003;124:373-8.
- [CrossRef] [Google Scholar]
- A clinical evaluation of titanium miniplates as anchors for orthodontic treatment. Am J Orthod Dentofacial Orthop. 2005;128:382-4.
- [CrossRef] [PubMed] [Google Scholar]
- An orthopedic approach to the treatment of Class III malocclusion in young patients. J Clin Orthod. 1987;21:598-608.
- [Google Scholar]
- Skeletal response to maxillary protraction with and without maxillary expansion: A finite element study. Am J Orthod Dentofacial Orthop. 2009;135:723-8.
- [CrossRef] [PubMed] [Google Scholar]
- Skeletal changes of maxillary protraction in patients exhibiting skeletal class III malocclusion: A comparison of three skeletal maturation groups. Angle Orthod. 2003;73:26-35.
- [Google Scholar]
- The effects of maxillary protraction therapy with or without rapid palatal expansion: A prospective, randomized clinical trial. Am J Orthod Dentofacial Orthop. 2005;128:299-309.
- [CrossRef] [PubMed] [Google Scholar]
- Skeletal anchorage for orthopedic correction of growing Class III patients. Semin Orthod. 2011;17:124-37.
- [CrossRef] [Google Scholar]
- Effects of facemask treatment anchored with miniplates after alternate rapid maxillary expansions and constrictions; a pilot study. Angle Orthod. 2011;81:639-46.
- [CrossRef] [PubMed] [Google Scholar]
- A novel method for treatment of Class III malocclusion in growing patients. Prog Orthod. 2017;18:40.
- [CrossRef] [PubMed] [Google Scholar]




