

Translate this page into:
Assessment of the quality, reliability, and readability of the websites about orthognathic surgery

*Corresponding author: Rüveyda Doğrugören, Department of Orthodontics, Gülhane Faculty of Dental Medicine, University of Health Sciences, Ankara, Türkiye. ruveydadogrugoren@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Doğrugören R, Topsakal KG, Öztürk T. Assessment of the quality, reliability, and readability of the websites about orthognathic surgery. APOS Trends Orthod. doi: 10.25259/APOS_81_2024
Abstract
Objectives:
The purpose of this study is to evaluate the accuracy, dependability, and readability of websites providing information about orthognathic surgery.
Material and Methods:
A total of 300 websites encountered through Google, Yahoo, and Bing search engines using the search terms “orthognathic surgery” and “jaw surgery” were utilized. Websites containing duplicate advertisements, original articles, or course content with video links unrelated to the topic were excluded from the study. Ninety-three websites were included in the study. The included websites were assessed for reliability and quality using the DISCERN, Ensuring Quality Information for Patients (EQIP), and Journal of American Medical Association (JAMA) tools. Readability was evaluated by determining the Flesch Reading Ease Score (FRES) and Flesch–Kincaid Grade Level (FKGL) scores. The data that did not show normal distribution were analyzed using the Kruskal–Wallis test. Post hoc comparisons were conducted using the least significant difference and Mann– Whitney U-tests. A significance level of P < 0.05 was accepted.
Results:
The mean DISCERN score was (38.47 ± 10.47), the EQIP score was (57.34 ± 10.73), and the JAMA score was (0.81 ± 0.99). The FRES was determined to be (43.89 ± 11.36), and the FKGL score was (12.06 ± 2.3). In the layperson group, the highest scores were found in the DISCERN (44.62 ± 9.73) and JAMA (1.85 ± 0.8) analyses compared to other groups.
Conclusion:
Website content on orthognathic surgery is generally of poor quality, and moderate reliability, with readability often being challenging for the average reader. There is a need for more user-friendly websites that offer comprehensive and easily digestible information to better serve orthognathic surgery patients.
Keywords
Websites
Orthognathic surgery
Patient information

INTRODUCTION
The internet has become a primary source of information for individuals seeking data on a range of health-related topics, including dental and medical treatments. The increasing trend is driven by the convenience and accessibility of online resources. A growing body of evidence indicates that individuals are more inclined to explore their medical conditions online than to engage in discourse with healthcare professionals. This is attributed to the ease of access and perceived anonymity of these digital platforms.[1] However, the pervasiveness of online information carries the risk of misinformation, which can potentially result in suboptimal patient decisions, heightened anxiety, and even a delay in seeking appropriate treatment options.[2] While websites can facilitate communication between patients and healthcare professionals, such evaluations not only ensure that patients receive accurate and reliable information but also empower clinicians to guide their patients toward trustworthy sources.[3]
Furthermore, websites facilitate communication between patients and field specialists, thereby enhancing their understanding of complex procedures. However, research has shown that a significant proportion of available online content may be biased or inaccurate, which can adversely affect patient perceptions and lead to misinformed treatment decisions. To address this issue, several tools have been developed to evaluate the quality of online health information.[4] Among these tools, the Quality Criteria for Consumer Health Information (DISCERN) instrument assesses the reliability and quality of treatment information, the Ensuring Quality Information for Patients (EQIP) toolkit evaluates the competency and transparency of websites, and the Journal of American Medical Association (JAMA) Benchmark examines the transparency of website authorship and disclosure.[5-7] In addition, the Flesch Reading Ease Score (FRES) and Flesch-Kincaid Grade Level (FKGL) are used to assess the readability of website content, with higher FRES scores indicating easier readability and lower FKGL scores representing content suitable for lower grade levels.[8,9]
Congenital and skeletal disorders in the jaw and face due to genetic, environmental, or iatrogenic factors impact individuals both functionally and esthetically. These disorders should be treated with fixed or removable orthodontic appliances. Still, in severe skeletal Class II and Class III cases, craniofacial anomalies, and the presence of asymmetry, orthognathic surgical planning may be required to achieve ideal facial esthetics. Orthognathic surgery impacts patients’ quality of life both pre- and post-operation and is extensive, often spanning several years.[10] The decision to undergo this treatment is pivotal, especially considering it involves general anesthesia and carries a notable risk of complications.[11]
Individuals often base their treatment decisions on information obtained from platforms such as social media, websites, and YouTubeTM. However, a literature review has found that the reliability and readability of content on YouTube and other websites have generally poor-quality scores.[12-14] The availability of reliable and high-quality information from various online platforms can significantly facilitate clinicians’ tasks. Literature reviews reveal that researchers utilize various criteria for website evaluation. Aldairy et al. evaluated websites about orthognathic surgery using DISCERN analysis and reported that the information obtained from most websites had a low DISCERN score.[15]
Engelmann et al. assessed EQIP analysis and reported a broad range of website scores, with some sites leading patients to form unrealistic expectations.[16] Bavbek and Tuncer found that patients generally obtain low-quality information from the internet when researching medical websites.[17] In light of this, the present study aims to fill this gap by evaluating the quality, reliability, and readability of a diverse set of websites that provide information on orthognathic surgery. By applying a combination of the DISCERN, EQIP, and JAMA tools, this study provides a more holistic evaluation of the current state of online information on this topic and highlights areas that need improvement to better serve potential patients and clinicians alike.
MATERIAL AND METHODS
Ethical consideration and assessment tools
Ethical Committee approval was unnecessary for the study as it did not involve human material or data. Data sourced from Google Trends (Google Trends, 2020, Alphabet, USA, https://trends.google.com) indicate a worldwide preference for “orthognathic surgery” and “jaw surgery” as top search terms [Figure 1]. The internet search was conducted in July 2023 using the search terms found with Google Trends “orthognathic surgery” and “jaw surgery” with VPN turned off, utilizing “GoogleTM (Google, 2023, Alphabet, USA, https://www.google.com),” “Yahoo® (Yahoo Inc., 1995, USA, https://www.yahoo.com),” and “BingTM (Microsoft, 2009, USA, https://www.bing.com)” search engines. In 2023, Google was the most preferred search engine, with a 92.62% preference rate. It is followed by Bing search engine (2.9%) and Yahoo search engine (1.15%), respectively.[18]
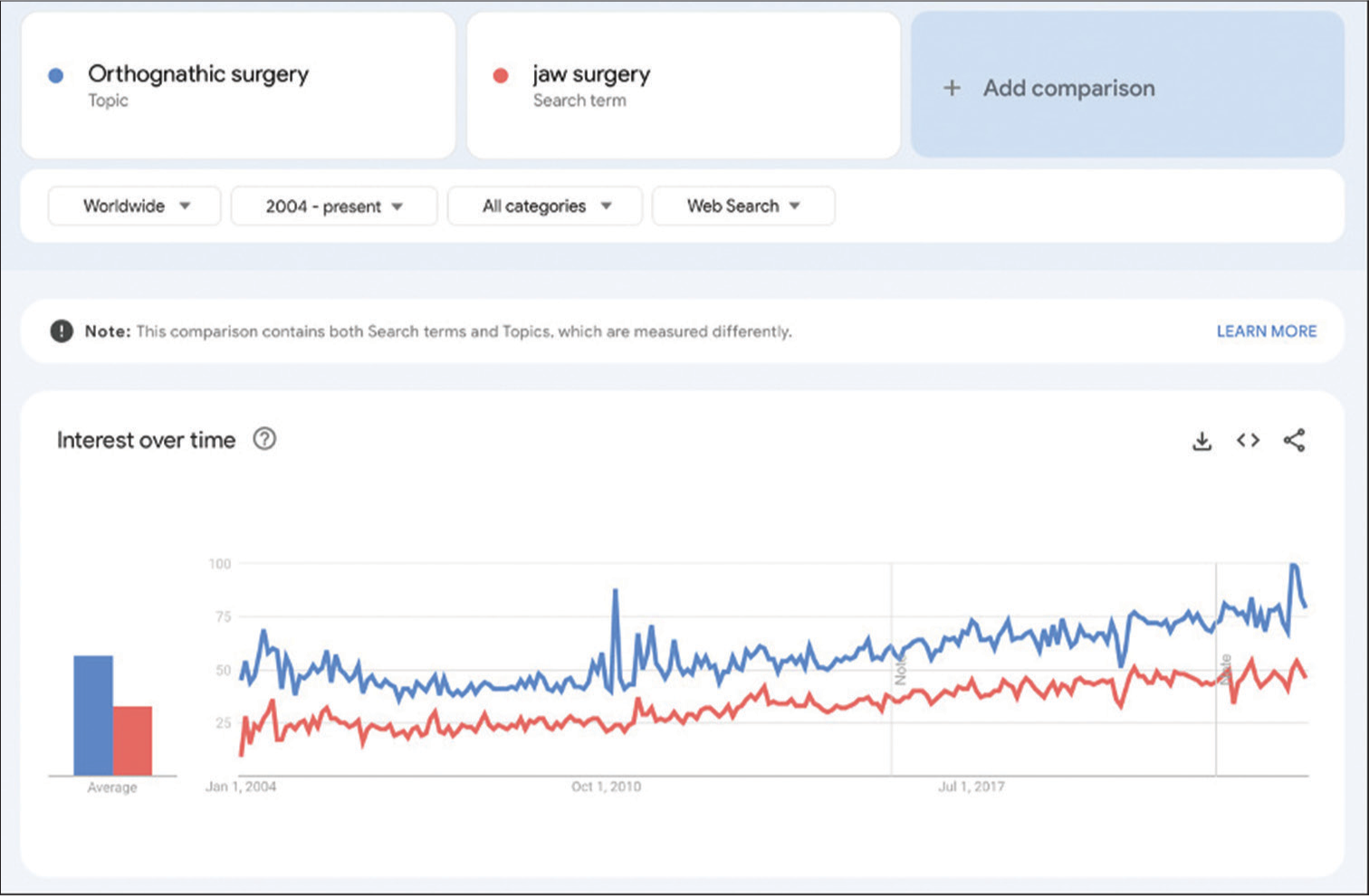
- The appearance of the search terms, orthognathic surgery, and jaw surgery, in Google Trends.
An evaluation was conducted on the top 50 websites for every search engine and keyword.[19] In the present study, the first 50 results that people are likely to view have been evaluated.[15,16]
English websites related to the topic were preferred as inclusion criteria for the study. The study excluded repeated websites on different search engines, advertisement websites, YouTube videos, research articles, and informed consent documents. Websites were evaluated using DISCERN, EQIP, and JAMA assessment tools and were categorized according to the author or website owner. Furthermore, the readability of the websites was assessed using the FRES and FKGL tools.
The DISCERN instrument
The DISCERN tool, comprising 16 questions, each scored between 1 and 5, is divided into three sections. The initial eight questions are designed to gauge the websites’ reliability, while questions nine through 15 focus on assessing the content quality concerning treatment options. The 16th question yields an aggregate score for the websites.[20] In the scoring, one point indicates that the insufficient or absent information (definitely no); five points indicate that the best information presented on the website. According to the total average scores, websites are classified into five groups: 16–26 points = very poor; 27–38 points = poor; 39–50 points = average; 51–62 points = good; and >63 points = excellent.[21] The scoring of the DISCERN tool is based on the average score determined in three categories: Reliability, treatment option, and overall score.[5]
EQIP toolkit
The EQIP toolkit, a 20-question evaluation tool, assesses the reliability and validity of websites. Scores range from 0% to 100%, with higher percentages indicating greater website competency regarding the topic.[6] The formulation of the EQIP evaluation tool is provided below: [22]
Score = (“Yes” × 1 + “Partially yes” × 0.5)/(20−“NA”×1).
JAMA benchmark (Silberg standard)
The JAMA benchmark facilitates the evaluation of websites in terms of transparency and reliability. It employs four simple questions, with content, respectively, consisting of authorship, attribution, disclosure, and currency. Unlike other tools, the JAMA benchmark does not assign scores to individual criteria; instead, it simply notes the presence or absence. The final evaluation yields a score ranging from 0 to 4, with 4 indicating that a website meets all criteria.[7]
FRES and FKGL scoring
The FRES and FKGL are tools used to evaluate text readability. These scores are influenced by the number of words per sentence and the syllable count, with higher counts making a text more complex. A FRES score in the 90–100 range suggests that a 10–11-year-old child can easily comprehend the text. Conversely, a score of 0–29 indicates that the text is suitable for readers with a university-level education.[8,23] Furthermore, the FKGL value determines the reader’s grade level based on the text’s readability.[9] The formulations for FRES and FKGL scoring are provided below. FRES Score = 206.835 – (1.015 × average sentence length) – (84.6 × average number of syllables per word)
FKGL = (0.39 × average number of words per sentence) + (11.8 × average number of syllables per word) −15.59.
Statistical analysis
Data collection was executed using Microsoft Office Excel software, and IBM’s Statistical Package for the Social Sciences software (Version 24, Armonk, NY, USA) facilitated the statistical analyses. The Shapiro–Wilk test assessed the normality of data distributions, while the Levene test scrutinized homogeneity. For analyzing data that conformed to normal distribution and homogeneity, the one-way analysis of variance (ANOVA) was employed for group comparisons. Conversely, the Kruskal–Wallis test was utilized for analyzing data that deviated from normal distribution. Subsequent post hoc analyses for the one-way ANOVA utilized the least significant difference test, and the Mann–Whitney U test was applied following the Kruskal–Wallis test. Superscript letters were used in tables to denote pairwise comparison results. The Spearman correlation coefficient was deployed to explore the relationship among quality criteria, with a statistical significance threshold set at P < 0.05.
RESULTS
The measurements were conducted by an orthodontist with at least 5 years of experience, and for intra-researcher consistency, 10% of the websites were measured again after 2 weeks. The intraobserver reliability, calculated using the intraclass correlation coefficient with a 95% confidence interval, indicated a high level of agreement, demonstrating the consistency and reproducibility of the measurements.
Three hundred websites were initially recorded for the study, and only 93 met the inclusion criteria [Figure 2]. The websites that met the criteria were categorized based on the field of the website owner or author. Fifty-four of the websites were managed by oral and maxillofacial surgeons, 11 by orthodontists, eight by plastic surgeons, seven by multidisciplinary clinics, and 13 by unidentified individuals or non-health professionals. A comparison of groups based on each question of the DISCERN instrument is shown in [Table 1]. Significant differences among groups were found in the answers to the third (P = 0.037), fifth (P < 0.001), sixth (P < 0.001), and 16th (P = 0.043) questions. The third question had the lowest values on websites belonging to maxillofacial surgeons (4.02 ± 0.57), statistically significantly lower than those of orthodontists (4.45 ± 0.52). In the evaluation of the fifth and sixth questions, the Layperson group demonstrated significantly higher scores compared to all other groups. In addition, in the assessment of the 16th question, the Layperson group’s scores were significantly higher than those of the maxillofacial surgery group, as detailed in [Table 1].
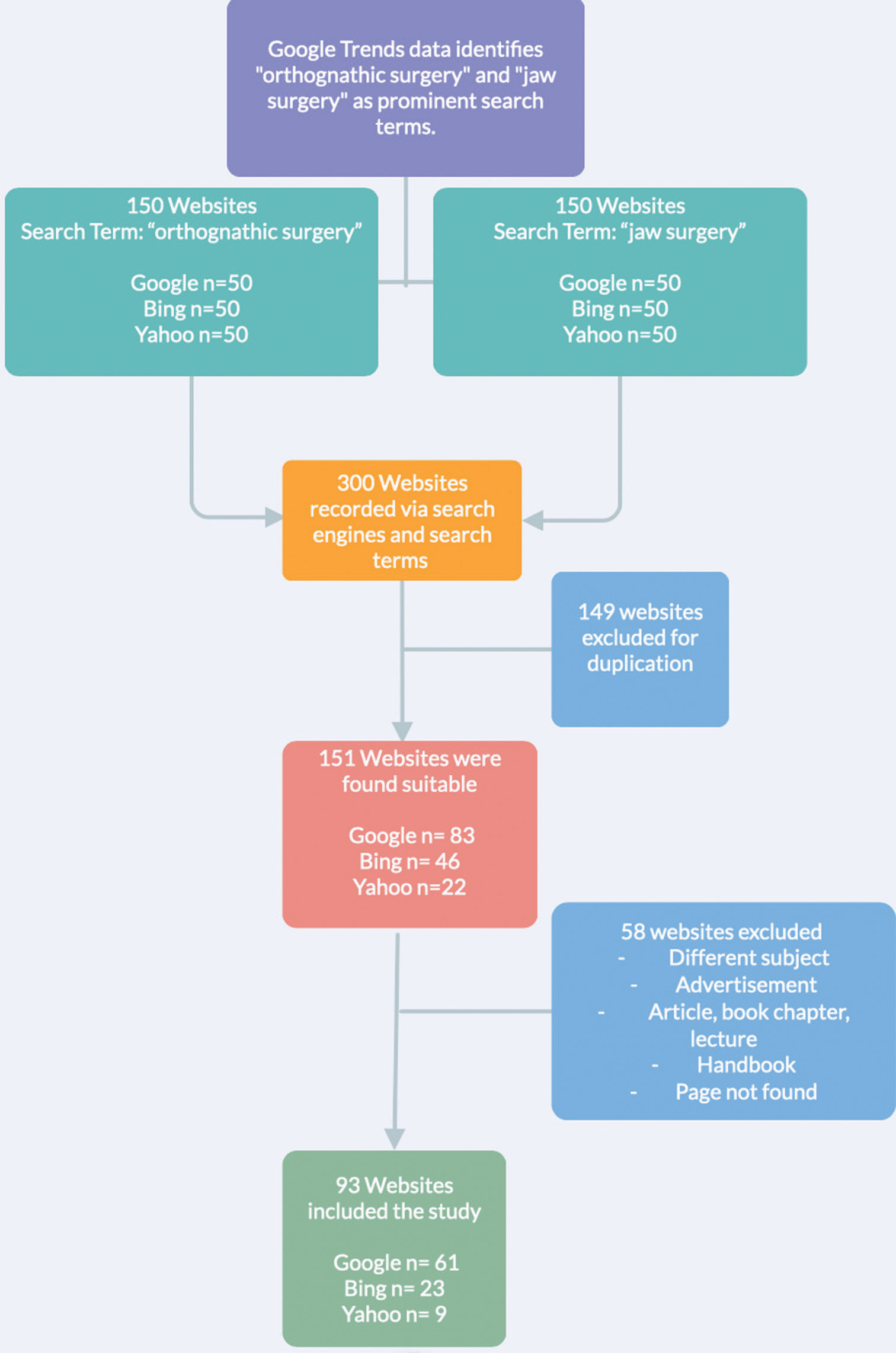
- Flowchart for this study.
| Question descriptions | Multidisciplinary clinic (n=7) | Plastic surgeon (n=8) | No author disclosed (n=13) | Orthodontist (n=11) | Maxillofacial surgeon (n=54) | Totally | P-values* | |
|---|---|---|---|---|---|---|---|---|
| Section 1 (questions 1-9): The reliabiliy of the publication | ||||||||
| Q1 | Are the aims clear? | 4.1440.69 | 4.1340.64 | 4.2340.44 | 4.0940.54 | 3.9340.72 | 4.0240.66 | 0.629 |
| Q2 | Does it achieve its aims? | 3.7140.49 | 3.540.93 | 4.0840.64 | 440.77 | 3.6340.85 | 3.7340.81 | 0.224 |
| Q3 | Is it relevant? | 4.5740.53a,b | 4.38±0.52a,b’c | 4.23±0.73a,b’c | 4.45±0.52b | 4.0240.57c | 4.1740.6 | 0.037 |
| Q4 | Is it clear what sources of information were used to compile the publication (other than author/producer)? | 2.1441.95 | 1.0040.00 | 1.6241.5 | 1.3641.21 | 1.1940.8 | 1.3241.08 | 0.212 |
| Q5 | Is it clear when the information used or reported in the publication was produced? | 2.4341.9a | 1.00±0.00b | 4.0841.75e | 2.09±0.87a,b | 1.72±1.53a,b | 2.0941.77 | 0.000 |
| Q6 | Is it balanced or unbiased? | 3.4341.81a | 3.8841.13a | 4.77±0.44b | 3.73±1.01a | 3.33±0.97a | 3.6341.11 | 0.000 |
| Q7 | Does it provide details of additional sources of support and information? | 2.1441.95 | 1.0040.00 | 1.6941.49 | 1.8241.6 | 1.1940.78 | 1.3941.13 | 0.107 |
| Q8 | Does it refer to areas of uncertainty? | 1.02±0.01 | 1.1340.35 | 1.0040.00 | 1.0040.00 | 1.2640.85 | 1.1640.66 | 0.519 |
| Section 2 (questions 9-15): The quality of the information on treatment choices | ||||||||
| Q9 | Does it describe how each treatment works? | 3.1441.57 | 2.5041.69 | 2.6941.44 | 2.7341.68 | 2.6341.38 | 2.6841.44 | 0.917 |
| Q10 | Does it describe the benefits of each treatment? | 3.5741.13 | 2.8840.99 | 2.9241.26 | 3.3641.43 | 2.6541.36 | 2.8641.32 | 0.293 |
| Q11 | Does it describe the risks of each treatment? | 2.1441.95 | 2.7541.58 | 2.5441.81 | 2.1841.66 | 1.6741.29 | 1.9841.51 | 0.096 |
| Q12 | Does it describe what would happen if no treatment is used? | 1.2940.76 | 1.1340.35 | 1.3141.11 | 1.2740.47 | 1.1540.68 | 1.1940.71 | 0.333 |
| Q13 | Does it describe how treatment choices affect the overall quality of life? | 3.1441.35 | 3.8840.83 | 3.6941.18 | 3.0941.51 | 2.8041.61 | 3.0841.5 | 0.211 |
| Q14 | Is it clear that there may be more than one possible choice of treatment? | 1.0040.00 | 1.541.41 | 1.6941.25 | 1.9141.22 | 1.6141.14 | 1.641.14 | 0.309 |
| Q15 | Does it provide support for shared decision-making? | 1.2940.76 | 241.41 | 1.3140.48 | 1.6441.03 | 1.2440.55 | 1.3740.75 | 0.377 |
| Section 3 (question 16): Overall quality rating of the publication | ||||||||
| Q16 | This question is rated accordingly to Note | 2.57±1.13a,b | 2.2541.04lb | 2.77±0.73a | 2.36±0.92a,b | 1.9840.86b | 2.2040.92 | 0.043 |
| Note: 1 (Low: Serious, or extensive shortcomings). 2. 3 (Moderate: Potentially important but no serious shortcomings). 4. 5 (High: Minimal shortcomings) | ||||||||
DISCERN: Quality criteria for consumer health information. Data was given MeantSD. Statistically significant values are indicated in bold. * Results of Kruskall-Wallis test. The Mann-Whitney U-test was used for pairwise comparisons between groups. Letters in superscript indicate inline group comparison. The same letters indicate the similarity between the groups
The comparison of the DISCERN instrument among all website groups is presented in [Table 2].
| Multidisciplinary Clinic (n=7) | Plastic Surgeon (n=8) | Layperson (n=13) | Orthodontist (n=11) | Maxillofacial Surgeon (n=54) | Totally | P-values | |
|---|---|---|---|---|---|---|---|
| DISCERN Section 1 | 23.57±7.44a, b | 20.00±2.62a | 25.69±4.79b | 22.55±5.07a | 20.26±4.46a | 21.52±5.04 | 0.001* |
| DISCERN Section 2 | 15.57±4.43 | 16.63±6.44 | 16.15±5.71 | 16.18±7.00 | 13.74±5.46 | 14.75±5.72 | 0.329* |
| DISCERN Section 3 | 2.57±1.13a, b | 2.25±1.04a, b | 2.77±0.73a | 2.36±0.92a, b | 1.98±0.86b | 2.2±0.92 | 0.043* |
| DISCERN Total Score | 41.71±12.3a, b | 38.88±9.73a, b | 44.62±9.73a | 41.09±11.78a, b | 35.98±9.74b | 38.47±10.47 | 0.023* |
| EQIP | 61.79±14.84 | 58.13±10.59 | 60.38±10.2 | 61.59±12.41 | 55.05±9.66 | 57.34±10.73 | 0.164** |
| JAMA | 1.14±1.35a | 0.5±0.76a | 1.85±0.8b | 0.91±1.04a | 0.54±0.84a | 0.81±0.99 | 0.001* |
| FRES | 44.21±11.34 | 42.33±6.12 | 49.68±10.68 | 39.62±14.19 | 43.55±11.33 | 43.89±11.36 | 0.276** |
| FKGL | 12.39±2.76 | 12.35±1.65 | 11.11±2.05 | 12.45±2.45 | 12.12±2.36 | 12.06±2.3 | 0.622* |
DISCERN: Quality criteria for consumer health information, EQIP: Ensuring quality information for patients, JAMA: Journal of American medical association, FRES: Flesch reading ease score, FKGL: Flesch-Kincaid grade level, ANOVA: Analysis of variance. Data were given Mean±SD. Statistically significant values are indicated in bold. *Results of Kruskall–Wallis test. **Results of One-way ANOVA test. The Mann–Whitney U-test was used for pairwise comparisons between groups. Letters in superscript indicate inline group comparison. The same letters indicate the similarity between the groups
Significant differences were found in DISCERN Section 1, DISCERN Section 3, DISCERN Total Score, and JAMA values. The highest values for answers to DISCERN Section 1 questions were found in the Layperson group. The lowest values for the answer to the DISCERN Section 3 question were in the maxillofacial surgeon group. The DISCERN total score values were lowest in the maxillofacial surgeon group and highest in the Layperson group. The highest JAMA scores were also found in the Layperson group. No significant differences were found in other quality criteria among groups.
The examination of the relationship between scores obtained from websites for quality criteria is shown in [Table 3]. DISCERN, EQIP, JAMA, and FRES values showed a positive correlation with each other, while FKGL values showed a negative correlation with all others.
| DISCERN | EQIP | JAMA | FRES | FKGL | |
|---|---|---|---|---|---|
| DISCERN | 1 | 0.606** | 0.465** | 0.247* | −0.255* |
| EQIP | 0.606** | 1 | 0.401** | 0.278** | −0.221* |
| JAMA | 0.465** | 0.010** | 1 | 0.088 | −0.081 |
| FRES | 0.247* | 0.278** | 0.088 | 1 | −0.937** |
| FKGL | −0.255* | −0.221* | −0.081 | −0.937** | 1 |
DISCERN: Quality criteria for consumer health information, EQIP: Ensuring quality information for patients, JAMA: Journal of American medical association, FRES: Flesch reading ease score, FKGL: Flesch-Kincaid grade level. Data was given Spearman Correlation Coefficients. *Correlation is significant at the 0.05 level (two-tailed), **Correlation is significant at the 0.01 level (two-tailed)
DISCUSSION
This study aims to assess the reliability, quality, and readability of online content related to orthognathic surgery. Websites sourced through three distinct search engines were analyzed and classified according to the expertise area of the author or site owner. Utilizing the first section of the DISCERN Instrument to evaluate reliability, it was found that the reliability across all groups was moderate. Readability was generally categorized at very difficult levels, while the quality of the websites, as determined by EQIP, was rated as poor.
Based on the findings from the DISCERN analysis, it has been observed that the websites “refer to areas of uncertainty” and provide information about the conditions “what would happen if no treatment” is used at a lower level. In addition, it was noted that the websites provide information in a neutral manner and generally include information about individuals’ quality of life after surgery. According to our study’s results, websites owned or authored by maxillofacial and plastic surgeons were of poor quality. In contrast, those related to orthodontics, multidisciplinary clinics, or those created by unspecified authors or those not in the health field were of medium quality. Furthermore, on evaluating the overall scoring of the websites, they were found to have poor content. Aldairy et al. evaluated websites providing information about orthognathic surgery; the highest DISCERN score was 64, and the lowest was 21.[15] In a study by Bavbek and Tuncer evaluating websites about orthognathic surgery in Türkiye, according to DISCERN analysis results, websites belonging to maxillofacial surgeons had an average score of 43.67, orthodontists’ websites averaged 28.72, and plastic surgeons’ websites scored 33.34.[17] In our study, the highest score was 72, and the lowest was 23. Websites are designed to provide brief information about orthognathic surgery and direct patients to schedule a consultation with a specialist for detailed information. Hence, the outcomes of the research suggest that the websites’ quality ranges from moderate to poor.
In the EQIP analysis, the content quality of the websites was generally rated between 50% and 75%. Notably, websites owned by maxillofacial and plastic surgeons scored lower in the EQIP evaluation. The inclusion of alternative treatment options was found to be limited; while information on orthognathic surgery was prevalent, content on camouflage treatments or alternative surgical options was scarce. In addition, few websites referenced content from other sources. Although some websites featured patient experiences with orthognathic surgery, the majority lacked patient testimonials and data. Engelmann et al. reported an average EQIP score of 68.256 in their evaluation of orthognathic surgery websites.[16] The reason for the value obtained in our study being lower may be the inclusion of more websites in our study.
In the JAMA analysis, it was reported that the general scoring of the websites was average, providing a general idea. This situation generally indicates that the citation and explanation rate on the websites is low. Furthermore, generally, the creation date of the websites is indicated. Individuals can get an idea about the content’s recency thanks to this data. The restricted number of websites disclosing their funding sources in the JAMA benchmark could be attributed to the nature of their creation. Websites on orthognathic surgery are typically informational platforms established by doctors, with minimal financial backing from commercial brands selling medical products. In addition, the general absence of references on these websites might be due to doctors relying on their expertise when disseminating information or perhaps overlooking potential plagiarism issues.
The readability evaluations using FRES and FKGL analyses reveal that the websites’ content is geared toward a college-level audience. The highest FRES score and easy readability were observed in the layperson group. When evaluating the FKGL results, it was seen that the websites have high-school readability levels, and the lowest FKGL score was seen in the Layperson group. When all websites are evaluated, the website contents are generally created suitable for high school and college levels. Pithon and Dos Santos, in their research evaluating websites on post-orthognathic surgery pain, reported that the readability level of the content was suitable for university graduates or undergraduate students.[24] The findings are similar to the findings obtained in our study.
Considering the data obtained in the study, it was detected that some websites do not share their information sources and do not include current treatment options on their websites. In this context, including this data can increase the reliability and quality of the websites. Patients can be allowed to reach different perspectives by also including content found on different websites. At the same time, websites can enlighten uncertain topics and the risks of treatment. Given the varied educational backgrounds of individuals seeking information on orthognathic surgery, adopting simpler language can make the content accessible to a wider audience.
Limitations
The study has several limitations that need to be considered when interpreting the findings. Formerly, the search was limited to English-language websites, which may not represent the information accessible to non-English speaking patients. This restriction could affect the generalizability of our results to a broader population. Furthermore, the search was conducted from a specified location in the USA with the VPN turned off, which may have influenced the search results due to location-based variations in search engine algorithms. In addition, the dynamic nature of the internet means that website content can be frequently updated, potentially altering the accuracy and quality of the information over time. Therefore, the results are only valid for the specific time frame when the data were collected (July 2023). Future studies should aim to include a more diverse range of languages and regions and consider repeated evaluations over different time points to capture the evolving nature of online health information.
CONCLUSION
The findings of this study indicate that the quality of English-language websites on orthognathic surgery is generally low to moderate, and the readability is difficult for the average reader. Patients seeking information should not rely solely on these websites, as incomplete or misleading data may lead to misunderstandings. Therefore, patients need to consult healthcare professionals for accurate and comprehensive guidance. Clinicians, on the other hand, should proactively guide their patients by providing recommendations for reliable online resources and helping them critically evaluate the content they find online. This approach will not only mitigate the risk of misinformation but also empower patients to make more informed treatment decisions.
Ethical approval
The Institutional Review Board approval is not required.
Declaration of patient consent
Patient’s consent was not required as there are no patients in this study.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
Throughout the crafting of this manuscript, the author(s) employed ChatGPT to enhance the readability and assess the grammatical integrity of the original article’s language. Following the utilization of this tool/service, the author(s) meticulously reviewed and refined the content as necessary. The author(s) hereby assume full responsibility for the manuscript’s content
Financial support and sponsorship
Nil.
References
- Health information seeking in the digital age: An analysis of health information seeking behavior among US adults. Cogent Soc Sci. 2017;3:1302785.
- [CrossRef] [Google Scholar]
- Public Health and online misinformation: Challenges and recommendations. Annu Rev Public Health. 2020;41:433451.
- [CrossRef] [PubMed] [Google Scholar]
- Assessing internet access and use in a medically underserved population: Implications for providing enhanced health information services. Health Info Libr J. 2012;29:61-71.
- [CrossRef] [PubMed] [Google Scholar]
- A narrative review on the impact of online health misinformation on patients' behavior and communication. Am J Health Behav. 2024;48:276-84.
- [CrossRef] [Google Scholar]
- The DISCERN instrument. n.d. Available from: https://www.discern.org.uk/discern_instrument.php [Last accessed on 2023 Oct 06]
- [Google Scholar]
- Ensuring quality information for patients: Development and preliminary validation of a new instrument to improve the quality of written health care information. Health Expect. 2004;7:165-75.
- [CrossRef] [PubMed] [Google Scholar]
- Assessing, controlling, and assuring the quality of medical information on the internet: Caveant lector et viewor--let the reader and viewer beware. JAMA. 1997;277:1244-5.
- [CrossRef] [PubMed] [Google Scholar]
- Derivation of New Readability Formulas (Automated Readability Index, Fog Count And Flesch Reading Ease Formula) For Navy Enlisted Personnel United States: University of Central Florida; n.d
- [Google Scholar]
- Quality of life in orthognathic surgery patients: Post-surgical improvements in aesthetics and self-confidence. J Cranio Maxillofac Surg. 2012;40:400-4.
- [CrossRef] [PubMed] [Google Scholar]
- Evaluation of life quality of patients submitted to orthognathic surgery. Dental Press J Orthod. 2013;18:107-14.
- [CrossRef] [PubMed] [Google Scholar]
- Cosmetic facial surgery: Are online resources reliable and do patients understand them? Br J Oral Maxillofac Surg. 2018;56:124-8.
- [CrossRef] [PubMed] [Google Scholar]
- YouTubeTM as an information resource for orthognathic surgery. J Orthod. 2017;44:90-6.
- [CrossRef] [PubMed] [Google Scholar]
- Online patient education materials for orthognathic surgery fail to meet readability and quality standards. J Oral Maxillofac Surg. 2019;77:180.e1-8.
- [CrossRef] [PubMed] [Google Scholar]
- Orthognathic surgery: Is patient information on the Internet valid? Eur J Orthod. 2012;34:466-9.
- [CrossRef] [PubMed] [Google Scholar]
- Quality assessment of patient information on orthognathic surgery on the internet. J Craniomaxillofac Surg. 2020;48:661-5.
- [CrossRef] [PubMed] [Google Scholar]
- Information on the internet regarding orthognathic surgery in Turkey: Is it an adequate guide for potential patients? Turk J Orthod. 2017;30:78-83.
- [CrossRef] [PubMed] [Google Scholar]
- Statcounter global stats. n.d, Available from: https://gs.statcounter.com/search-engine-market-share#yearly-2020-2023 [Last accessed 2023 Oct 06]
- [Google Scholar]
- Information on the internet about clear aligner treatment-an assessment of content, quality, and readability. J Orofac Orthop. 2022;83:1-12.
- [CrossRef] [PubMed] [Google Scholar]
- DISCERN: An instrument for judging the quality of written consumer health information on treatment choices. J Epidemiol Community Health. 1999;53:105-11.
- [CrossRef] [PubMed] [Google Scholar]
- The quality of Internet information on lingual orthodontics in the English language, with DISCERN and JAMA. J Orthod. 2019;46:20-6.
- [CrossRef] [PubMed] [Google Scholar]
- Measuring quality of patient information documents with an expanded EQIP scale. Patient Educ Couns. 2008;70:407-11.
- [CrossRef] [PubMed] [Google Scholar]
- An assessment of the treatment information contained within the websites of direct-to-consumer orthodontic aligner providers. Aust Dent J. 2021;66:77-84.
- [CrossRef] [PubMed] [Google Scholar]
- Information available on the internet about pain after orthognathic surgery: A careful review. Dental Press J Orthod. 2014;19:86-92.
- [CrossRef] [PubMed] [Google Scholar]




