

Translate this page into:
Age and gender differences in maxillary canine impaction severity and orthodontic treatment difficulty – A retrospective cross-sectional study


*Corresponding author: Nabeel Almotairy, Department of Orthodontics and Pediatric Dentistry, Qassim University, Buraidah, Saudi Arabia. n.s.almotairy@qu.edu.sa
-
Received: ,
Accepted: ,
How to cite this article: Alsmnan A, Althunayyan A, Alshawy E, Almotairy N. Age and gender differences in maxillary canine impaction severity and orthodontic treatment difficulty – A retrospective cross-sectional study. APOS Trends Orthod 2023;13:168-75.
Abstract
Objectives:
The objectives of this study were to compare the maxillary canine impaction severity and orthodontic treatment difficulty in relation to age and gender.
Material and Methods:
Orthopantomograms of 105 patients with maxillary canine impaction were retrospectively collected and divided into 50 adolescents (11–17 years; 30% females) and 55 young adults (18–25 years; 34% females). Canine impaction severity was determined using one angular and three linear radiographic measurements, while orthodontic treatment difficulty was determined using a modified Pitt et al. index. Age and gender differences were assessed using Chi-square with Bonferroni correction and Mann–Whitney U-tests (P < 0.05), while the association between orthodontic treatment difficulty index score and age was assessed using linear regression analysis (95% confidence interval).
Results:
Compared to young adults, adolescents had mild (<30°) canine long axis to midline angulation (P = 0.008) and distally positioned cusp tip of impacted canine relative to adjacent lateral incisor root (P < 0.001). Meanwhile, males compared to females had distally positioned cusp tip of impacted canine relative to adjacent lateral incisor root (P = 0.008), while females compared to males had the canine cusp tip mesial to lateral incisor root (P = 0.002). The orthodontic treatment difficulty trend increased with age (R2 = 0.077; P < 001) and was higher in young adults than adolescents (P = 0.0218).
Conclusion:
The severity of maxillary canine impaction was higher in young adults and, to a lesser extent, in females. Orthodontic treatment difficulty of impacted maxillary canines also increased with age but not gender.
Keywords
Canine
Panoramic radiographs
Radiographic determinants
Linear and angular measurements
Adult

INTRODUCTION
Playing a pivotal role in both facial esthetics and occlusal function, the maxillary canine is regarded as a cornerstone in the dental arch. The impaction of maxillary canines is second to mandibular third molars, ranging across different populations from 0.92% to 2.2%, with a female predilection at a ratio of 2:1, with most impacted canines located palatally.[1] The etiology of canine impaction remains unknown, with two theories that have been put forward to explain this anomaly.[2] The first is the guidance theory, which emphasizes the role of the maxillary lateral incisor’s root in the eruption or impaction of maxillary canines.[3,4] The second theory suggested a genetic predisposition to maxillary canine impaction.[5,6] However, no single hypothesis can explain canine impaction completely.
In motivated and compliant patients with good dental health and where interceptive measures are deemed inappropriate, surgical exposure combined with orthodontic traction is the preferred approach for managing palatally impacted canines.[1,7,8] The orthodontist’s decision to expose and orthodontically align or remove the impacted maxillary canine is usually based on a radiographic evaluation of its intraosseous position.[9] Researchers have proposed a radiographic grading system to evaluate the severity of maxillary canine impaction.[10-12] Previous studies have reported four radiographic determinants, which positively correlate with the prognosis for exposure and alignment of ectopic canines.[12] These determinants include angulation of the canine long axis to the midline, vertical position of the canine crown from the occlusal plane, anteroposterior position of the canine root apex, and the degree of overlap of the adjacent incisor by the canine cusp tip.
Previous studies have found that canine impaction prediction and successful treatment prognosis were associated with the patient’s age and the canine’s location to adjacent teeth.[9,11,13,14] Where an increase in canine long axis to upper midline angulation, vertical distance to the occlusal plane, and its overlap of the adjacent lateral incisor can result in an increased impaction prediction and reduced prognosis for spontaneous correction.[9,11,13,15] Becker and Chaushu found that the increase in a patient’s age can result in a higher possibility of treatment failure and a longer duration of orthodontic traction,[14] while the study by Fleming et al. found that increasing age does not influence the impacted canine treatment duration.[16] However, there is little evidence linking the influence of the radiographic determinants on the duration of orthodontic traction of impacted canines.
Since early diagnosis and intervention are crucial for the management of impacted canines, orthodontists in clinical practice are interested in evaluating their radiographic position, thus gauging the impaction severity and treatment difficulty. Therefore, this study aims to compare the maxillary canine impaction severity and orthodontic treatment difficulty with age and gender.
MATERIAL AND METHODS
This retrospective and cross-sectional study was approved by the Committee of Research Ethics at Qassim University, Saudi Arabia (#21-01-06). The present study retrospectively screened orthopantomograms from approximately 5000 patients who had attended the dental clinics at Qassim University during the past 5 years (2018–2022). Based on a previous study, a power calculation was conducted using G*Power software (version 3.1.9.6; Heinrich Heine University Düsseldorf, Düsseldorf, Germany).[17] For an effect size of 0.6 and 95% significance level (α = 0.05; β = 80%), a sample of 90 participants was needed for this study. The four authors conducted an initial screening to select those orthopantomograms that fulfilled the inclusion/exclusion criteria. High-quality orthopantomograms from healthy patients aged 11–25 years were included, while orthopantomograms with pathological anomalies such as tumors, cysts, and cleft palate or with radiographic artifacts obscuring the maxillary canine region were excluded from the study.
The selected orthopantomograms were then examined further to include patients who have a maxillary canine impaction. The final set of orthopantomograms was classified according to the patient’s age into two age groups: An adolescent group (11–17 years) and a young adult group (18–25 years). Demographic data were collected regarding the patient’s age and gender as well as canine impaction laterality (uni-or bilateral), buccopalatal position, and impaction side (right or left for unilateral impaction only). All collected orthopantomograms were acquired using CRANEX D Digital Panoramic and Cephalometric X-ray Unit (SOREDEX™, Tuusula, Finland).
Radiographic examination
An experienced orthodontist (N.A.) evaluated the severity of canine impaction using four radiographic measurements obtained from the literature.[10-12,18-20] Each measurement contains a set of grades to gauge the degree of impaction severity [Figure 1]. These measurements are detailed below:
Angulation of canine long axis to the midsagittal line [Figure 1a]: Grade 1, <30°; Grade 2, 30–45°; and Grade 3, >45°.
Canine root apex location [Figure 1b]: Grade 1, in the location of canine root apex; Grade 2, in the first premolar root apex area; and Grade 3, in the second premolar root apex area.
Canine cusp tip vertical position [Figure 1c]: Grade 1, at the cementoenamel junction level of adjacent lateral incisor; Grade 2, within the cementoenamel junction and middle of the root of adjacent lateral incisor; Grade 3, within the middle of the root and root apex of adjacent lateral incisor; and Grade 4, apical to the adjacent lateral incisor root apex.
Canine cusp tip horizontal position [Figure 1d]: Grade 1, overlapping less than half of the root of adjacent lateral incisor; Grade 2, overlapping less than half of the root of adjacent lateral incisor but not extending beyond its boundaries; Grade 3, completely overlapping the adjacent lateral incisor root but not extending to central incisor boundaries; and Grade 4, completely overlapping the adjacent lateral incisor root and extending to central incisor boundaries.

- (a-d) A schematic represents the grades of the applied radiographic measurements to evaluate the impacted maxillary canine severity.
A calibration session was performed twice at 3-week intervals using 25 orthopantomograms that were randomly selected by a free-random selection software (Pick me! by Donation Coder forum, 2009).
Assessment of orthodontic treatment difficulty
A modified Pitt et al.[20] index was used to determine the difficulty of orthodontic treatment of impacted maxillary canines based on the following factors: Patient’s age, canine buccopalatal position and angulation, apex location, and vertical and horizontal position. Those factors have a subset of scores, and each score was multiplied by a weighting factor [Table 1]. The cumulative score for each patient ranges between 8.5 and 28.5.
| Factors | Score | Weight |
|---|---|---|
| Age | ||
| <12 years | 1 | 1.5 |
| 12–15 years | 2 | |
| 16–18 years | 3 | |
| >18 years | 4 | |
| Canine angulation | ||
| Grade 1 | 1 | 1 |
| Grade 2 | 2 | |
| Grade 3 | 3 | |
| Apex location | ||
| Grade 1 | 1 | 1.5 |
| Grade 2 | 2 | |
| Grade 3 | 3 | |
| Vertical position | ||
| Grade 1 | 1 | 1.5 |
| Grade 2 | 2 | |
| Grade 3 | 3 | |
| Grade 4 | 4 | |
| Horizontal position | ||
| Grade 1 | 1 | 2 |
| Grade 2 | 2 | |
| Grade 3 | 3 | |
| Grade 4 | 4 | |
| Buccopalatal position | ||
| Buccal | 1 | 1 |
| Palatal | 1 |
Statistics
Statistical analysis was conducted using the Statistical Package for the Social Sciences (SPSS) program (version 23; SPSS Inc, Chicago, IL). Test-retest reliability of the radiographic measurements was performed using Cohen’s Kappa (k) with a 95% confidence interval. Descriptive statistics were calculated, and the Chi-square test was used to examine the relationship between independent variables (patient’s age and gender) and dependent variables (canine impaction laterality, canine buccopalatal position, canine impaction side, and the radiographic measurements of canine impaction severity). The association between age and orthodontic treatment difficulty index score (excluding age factor) was analyzed by linear regression (95% confidence interval). While the difference in orthodontic treatment difficulty between age groups (excluding age factor) and gender were evaluated using the Mann–Whitney U-test. The P-value threshold for all the tests was set to 0.05. For significant Chi-square main effects, adjusted standardized residuals (z-scores) were converted to P-values for post hoc comparison with Bonferroni correction for multiple comparisons.
RESULTS
Sample characteristics
Out of the orthopantomograms screened, 105 patients with maxillary canine impaction were identified (an overall prevalence of 2.1%) with an average age of 17.5 ± 4.57 years. The adolescent group comprised 50 patients with an average age of 13.28 ± 1.81 years, while the young adult group comprised 55 patients with an average age of 21.34 ± 2.38 years. No differences were identified in gender distribution among the age groups [Table 2].
| Variable | 11-17 years | 18-25 years | Total | P-value* |
|---|---|---|---|---|
| n (%) | n (%) | n (%) | ||
| Sex | ||||
| Male | 35 (70) | 36 (65.5) | 71 (67.6) | 0.679 |
| Female | 15 (30) | 19 (34.5) | 34 (32.4) | |
| Impaction laterality | ||||
| Unilateral | 29 (58) | 42 (76.4) | 71 (67.6) | 0.060 |
| Bilateral | 21 (42) | 13 (23.6) | 34 (32.4) | |
| Buccopalatal position | ||||
| Buccal | 25 (35.2) | 15 (22.1) | 40 (28.8) | 0.095 |
| Palatal | 46 (64.8) | 53 (77.9) | 99 (71.2) | |
| Impaction side | ||||
| Right | 14 (48.3) | 21 (50) | 35 (49.3) | 1 |
| Left | 15 (51.7) | 21 (50) | 36 (50.7) | |
| Variable | Male | Female | Total | P-value* |
| n (%) | n (%) | n (%) | ||
| Impaction laterality | ||||
| Unilateral | 46 (64.8) | 25 (73.5) | 71 (67.6) | 0.504 |
| Bilateral | 25 (35.2) | 9 (26.5) | 34 (32.4) | |
| Buccopalatal position | ||||
| Buccal | 30 (31.3) | 10 (23.3) | 40 (28.8) | 0.419 |
| Palatal | 66 (68.8) | 33 (76.8) | 99 (71.2) | |
| Impaction side | ||||
| Right | 22 (47.8) | 13 (52) | 35 (49.3) | 0.806 |
| Left | 24 (52.2) | 12 (48) | 36 (50.7) |
The total number of impacted canines was 139. Most patients have a unilateral maxillary canine impaction (58% and 76.4% for Groups 1 and 2, respectively), where they occur on the left and right sides almost equally. The majority of the impacted canines were palatal (71.22%), while the remaining 28.78% were buccal. Further, no age-or gender-related differences were found on maxillary canine impaction laterality, buccopalatal position or impaction side [Table 2].
Test-retest reliability
The results showed good intra-rater agreement for the four radiographic measurements. The results were as follows: Canine angulation, k = 0.892, 95% CI (0.747–1.037), P < 0.0001; apex location, k = 0.746, 95% CI (0.547–0.946), P < 0.0001; vertical position, k = 0.884, 95% CI (0.729–1.039), P < 0.0001; and horizontal position, k = 0.821, 95% CI (0.642–0.999), P < 0.0001.
Canine impaction severity
The canine long axis to midline angulation for the total sample was Grade 1 (48.2%; <30°) and showed a statistical difference among age groups (χ2 [2, n = 139] = 7.155, P = 0.028; [Table 3]). Post hoc comparison showed that adolescents were more likely to have Grade 1 canine angulation than young adults (59.2% and 36.8% for groups 1 and 2, respectively; P = 0.008). Regarding gender differences, both males and females mostly have grade 1 canine angulation (51% and 41.9% for males and females, respectively) with no differences in the distribution of Grades 1, 2, and 3 canine angulations (χ2 [2, n = 139] = 1.348, P = 0.510).
| Variable | 11–17 years | 18–25 years | Total | P-value | Male | Female | Total | P-value |
|---|---|---|---|---|---|---|---|---|
| n(%) | n(%) | n(%) | n(%) | n(%) | n(%) | |||
| Canine angulation | ||||||||
| Grade 1 | 42 (59.2)‡ | 25 (36.8)‡ | 67 (48.2) | 0.028* | 49 (51) | 18 (41.9) | 67 (48.2) | 0.510 |
| Grade 2 | 14 (19.7) | 23 (33.8) | 37 (26.6) | 23 (24) | 14 (32.6) | 37 (26.6) | ||
| Grade 3 | 15 (21.1) | 20 (29.4) | 35 (25.2) | 24 (25) | 11 (25.6) | 35 (25.2) | ||
| Apex location | ||||||||
| Grade 1 | 25 (35.2) | 17 (25) | 42 (30.2) | 0.074 | 29 (30.2) | 13 (30.2) | 42 (30.2) | 1 |
| Grade 2 | 23 (32.4) | 35 (51.5) | 58 (41.7) | 40 (41.7) | 18 (41.9) | 58 (41.7) | ||
| Grade 3 | 23 (32.4) | 16 (23.5) | 39 (28.1) | 27 (28.1) | 12 (27.9) | 39 (28.1) | ||
| Vertical position | ||||||||
| Grade 1 | 19 (26.8) | 18 (26.5) | 37 (26.6) | 0.348 | 26 (27.1) | 11 (25.6) | 37 (26.6) | 0.165 |
| Grade 2 | 35 (49.3) | 40 (58.8) | 75 (54) | 47 (49) | 28 (65.1) | 75 (54) | ||
| Grade 3 | 16 (22.5) | 8 (11.8) | 24 (17.3) | 20 (20.8) | 4 (9.3) | 24 (17.3) | ||
| Grade 4 | 1 (1.4) | 2 (2.9) | 3 (2.2) | 3 (3.1) | 0 (0) | 3 (2.2) | ||
| Horizontal position | ||||||||
| Grade 1 | 51 (71.8)§ | 27 (39.7)§ | 78 (56.1) | 0.002* | 61 (63.5)‡ | 17 (39.5)‡ | 78 (56.1) | 0.015* |
| Grade 2 | 5 (7) | 8 (11.8) | 13 (9.4) | 9 (9.4) | 4 (9.3) | 13 (9.4) | ||
| Grade 3 | 4 (5.6) | 12 (17.6) | 16 (11.5) | 11 (11.5) | 5 (11.6) | 16 (11.5) | ||
| Grade 4 | 11 (15.5) | 21 (30.9) | 32 (23) | 15 (15.6)‡ | 17 (39.5)‡ | 32 (23) |
The canine root apex location for the total sample was mainly at the first premolar location (41.7%; Grade 2) but showed no age-or gender-related differences (χ2 [2, n = 139] = 5.201, P = 0.074 and χ2 [2, n = 139] = 0.001, P = 1, respectively). Similarly, the canine vertical position was mainly within the cementoenamel junction and root midway of the adjacent lateral incisor (54%; Grade 2) and showed no age-or gender-related differences (χ2 [2, n = 139] = 3.297, P = 0.348 and χ2 [2, n = 139] = 5.093, P = 0.165, respectively).
The canine horizontal position for the total sample mainly overlapped less than half the width of the lateral incisor (56.1%; Grade 1) and showed both age- and gender-related differences (χ2 [2, n = 139] = 15.144, P = 0.002 and χ2 [2, n = 139] = 10.426, P = 0.015, respectively). Post hoc comparison showed that adolescents compared to young adults were more likely to have Grade 1 canine horizontal position (71.8% and 39.7%, respectively; P < 0.001). Meanwhile, males were more likely than females to have impacted canines overlapping less than half the width of the lateral incisor (63.5% and 39.5%, respectively; P = 0.008), while females were more likely than males to have Grade 4 canine horizontal position (39.5% and 15.6%, respectively; P = 0.002).
Orthodontic treatment difficulty
A statistically significant difference in orthodontic treatment difficulty (excluding age factor) was identified between adolescents and young adults (U = 1871, z = −2.284, P = 0.0218; [Figure 2]). The results showed that young adults had an increased orthodontic treatment difficulty score (median = 14, IQR [9.75-17], n = 68) compared to adolescents (median = 11, IQR [8.5-15], n = 71). Meanwhile, the orthodontic treatment difficulty index score was higher in females than males by 3.5 points (males, median = 14.5, IQR [10.5-19.5]; females, median = 18, IQR [12-22]) but showed no statistical differences (U = 1669, z = −1.797, P = 0.072; [Figure 2]). By excluding the age factor, the regression model found that the patient’s age explains 7.7% of the variation in orthodontic treatment difficulty (R2 = 0.077, F [1,137] = 11.491, P < 001). The model predicts that with the incremental increase in age by 1 year, the orthodontic treatment difficulty index score increases by 0.27 [Figure 3].
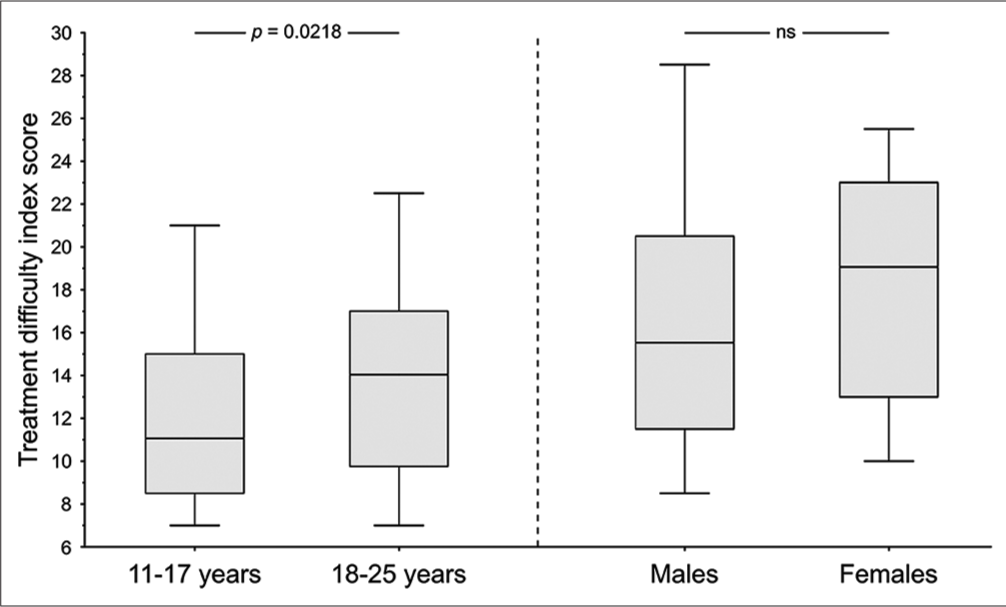
- Box plot of the patient’s gender and orthodontic treatment difficulty-weighted score. ns: Non-significant result.
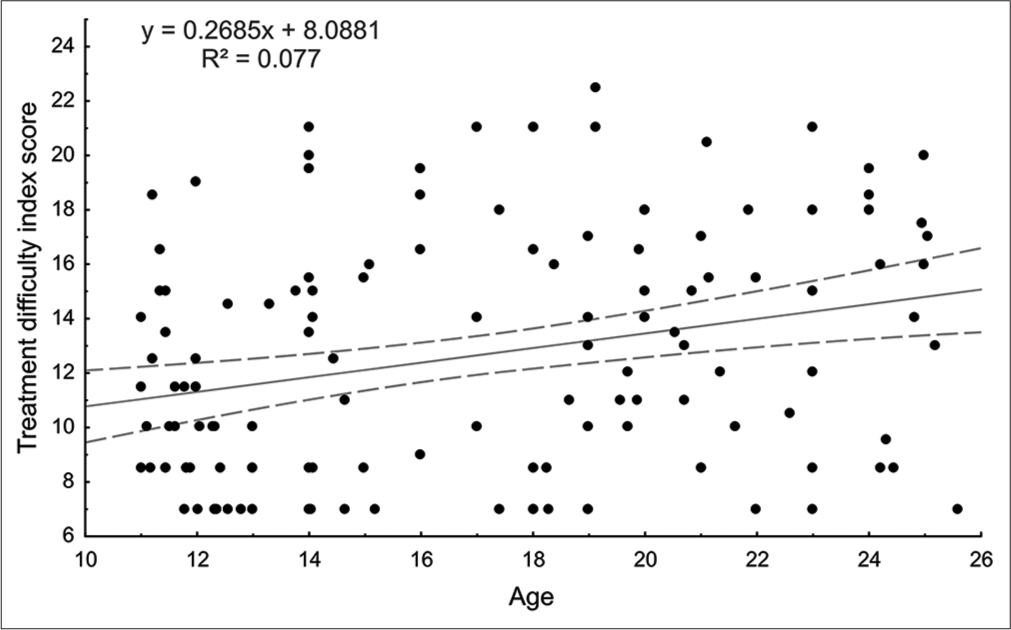
- Linear regression analysis with a 95% confidence interval of the patient’s age and orthodontic treatment difficulty weighted score (excluding age factor).
DISCUSSION
The severity of maxillary canine impaction varies according to its intraosseous position. The present study used orthopantomograms to compare the maxillary canine impaction severity and orthodontic treatment difficulty with age and gender. This study found a 2.1% overall prevalence of maxillary canine impaction among the study population, which supports the findings of extant studies for other populations.[1] Although earlier studies indicated that females have more maxillary canine impactions than males,[9,21] this study identified more males than females with canine impaction in both age groups. However, this may be explained by the location of the dental clinics at Qassim University from which the present study derived its retrospectively acquired orthopantomograms since these are located in the city outskirts, they may be less likely to be attended by female patients.
The present study also found bilateral canine impaction in 32.4% of the sample, slightly higher than some studies[9,12,22-24] but lower than other studies.[25,26] Meanwhile, the canine impaction in this study was almost one-third buccally while the remaining two-thirds were palatal, which is in agreement with the previous studies.[9,23,27] Further, the impaction side distribution was almost equal between the left and right sides, aligning with other studies.[28,29] However, no gender or age-group differences were identified concerning canine impaction laterality, buccopalatal position or side.
The prognosis for the successful management of impacted canines depends on the position of the tooth vertically and horizontally, its relationship to the roots of the adjacent teeth, and the operator’s skill during surgical exposure and orthodontic traction.[7,10] The previous literature reported contradicting results concerning the influence of patient’s age on the canine long axis to midline angulation. While others found that the long axis to midline angulation of impacted canines increases as the patient’s age increases,[17,30] another study did not.[16] However, in partial agreement with the previous studies, the present study’s findings showed that adolescents have milder angulation than young adults. Similar to earlier studies,[16,19,21] the current study also found that the impacted canine root apex was mainly at the first premolar location. Earlier studies also indicated that the vertical position of impacted canines compared to antimere canines does not change as the patient’s age increases,[17,30] suggesting a genetic predisposition for canine impaction.[5] Corroborating earlier studies,[17,30] the present study also found no age differences in the vertical position of the impacted canine.
The horizontal position of the unerupted maxillary canine cusp tip concerning the adjacent lateral incisor root can be used to predict canine impaction and treatment duration.[9,11,13,16,31] The previous studies indicated that compared to antimere canines, canines that were predicted to be impacted have their cusp tip overlapping or mesial (Grades 3 or 4) to the lateral incisor root.[11,31] The previous studies also suggested that as the patient’s age increases, this increases the severity of canine impaction,[14,20] and the duration of orthodontic treatment.[14] In relation to this, the present study found that the horizontal position of the maxillary impacted canine cusp tip mainly was Grade 1 in adolescents compared to young adults. Although the literature has yet to highlight the severity of canine impaction in females than males, this study showed that males were more likely than females to have a Grade 1 canine horizontal position, while females were more likely than males to have a Grade 4 position. These results align with Nieri et al.,[9] and we proposed that since females are genetically more likely to have canine impaction than males,[5] canine impaction severity can be explained by the gender-linked predisposition of females than males. However, factors other than gender should play a factor in determining the treatment difficulty of impacted canines, such as the patient’s age at the start of treatment, number of failed appointments, underlying malocclusion, and the patient’s poor oral hygiene compliance and maintenance.[9,14,32,33]
The present study used a modified Pitt et al.[20] index to assess the orthodontic treatment difficulty of impacted canines, finding no change in the overall treatment difficulty score according to gender but identifying that this increased in young adults over adolescents. The regression model indicated that the treatment difficulty of impacted canines increases incrementally with age (by 0.27 index score/year). These results corroborate the findings of earlier studies, which showed that the severity of canine impaction increases as the age of the patient increases;[14,20] thus increasing treatment difficulty, which can lead to longer treatment duration.[14,32] It should be noted that the used index does not consider the differences in treatment difficulty between unilateral and bilateral impaction.[9,23] As was shown by Grisar et al., the duration of orthodontic traction of bilateral canine can take 25 months on average compared to 21 months for unilateral impaction.[23] Another limitation of the used index is that it gives equal weight to buccal and lingual canine impaction, while the previous studies showed that palatal canines have a more prolonged orthodontic traction duration than buccal ones.[9,23]
The present study used selected radiographic measurements from orthopantomograms to evaluate canine impaction severity. Orthopantomograms are commonly used in dental practice for diagnostic purposes and planning interceptive therapy. It has also been documented that orthopantomograms can be a reliable and efficient tool for accurate and consistent linear and angular measurements.[34] However, orthopantomograms have certain limitations in assessing canine impaction since they are a two-dimensional representation of a three-dimensional alveolar structure and sometimes distort the frontal dentoalveolar region,[12,13] which can impose limitations when assessing canine impaction. Such limitations are the difficulty in assessing the exact buccopalatal location of the impacted canine and the extent of root resorption of adjacent teeth. In contrast, cone-beam computed tomography (CBCT) is far superior to orthopantomograms in investigating impacted teeth.[35] Therefore, future studies are recommended to implement CBCT to assess canine impaction severity and treatment difficulty and compare it with that of orthopantomograms.
CONCLUSION
Compared to young adults, maxillary impacted canines in adolescents had mild angulation and were distally located in relation to the adjacent lateral incisors.
Females had a severe horizontal position of impacted canines compared to males and a tendency for an increased orthodontic treatment difficulty score.
Orthodontic treatment difficulty of impacted maxillary canines increased with age, which was higher in young adults than adolescents.
Declaration of patient consent
The Institutional Review Board (IRB) permission obtained for the study.
Conflicts of interest
There are no conflicts of interest.
Data availability
All data generated or analyzed during this study are included in this published article and its supplementary information files.
Financial support and sponsorship
Nil.
References
- Canine impaction-a review of the prevalence, etiology, diagnosis and treatment. Semin Orthod. 2019;25:117-23.
- [CrossRef] [Google Scholar]
- Extraction of the deciduous canine as an interceptive treatment in children with palatally displaced canines-Part II: Possible predictors of success and cut-off points for a spontaneous eruption. Eur J Orthod. 2015;37:219-29.
- [CrossRef] [Google Scholar]
- In defense of the guidance theory of palatal canine displacement. Angle Orthod. 1995;65:95-8.
- [Google Scholar]
- Maxillary tooth size variation in dentitions with palatal canine displacement. Eur J Orthod. 2002;24:313-8.
- [CrossRef] [PubMed] [Google Scholar]
- The palatally displaced canine as a dental anomaly of genetic origin. Angle Orthod. 1994;64:249-56.
- [Google Scholar]
- Impacted maxillary canines: A review. Am J Orthod Dentofac Orthop. 1992;101:159-71.
- [CrossRef] [PubMed] [Google Scholar]
- A review of the diagnosis and management of impacted maxillary canines. J Am Dent Assoc. 2009;140:1485-93.
- [CrossRef] [PubMed] [Google Scholar]
- Factors affecting the clinical approach to impacted maxillary canines: A Bayesian network analysis. Am J Orthod Dentofac Orthop. 2010;137:755-62.
- [CrossRef] [PubMed] [Google Scholar]
- An investigation into the response of palatally displaced canines to the removal of deciduous canines and an assessment of factors contributing to favourable eruption. Br J Orthod. 1993;20:215-23.
- [CrossRef] [PubMed] [Google Scholar]
- Canine impaction identified early with panoramic radiographs. J Am Dent Assoc. 1992;123:91-7.
- [CrossRef] [PubMed] [Google Scholar]
- Radiographic examination of ectopically erupting maxillary canines. Am J Orthod Dentofac Orthop. 1987;91:483-92.
- [CrossRef] [PubMed] [Google Scholar]
- Early treatment of palatally erupting maxillary canines by extraction of the primary canines. Eur J Orthod. 1988;10:283-95.
- [CrossRef] [PubMed] [Google Scholar]
- Success rate and duration of orthodontic treatment for adult patients with palatally impacted maxillary canines. Am J Orthod Dentofac Orthop. 2003;124:509-14.
- [CrossRef] [PubMed] [Google Scholar]
- Radiographic predictors of maxillary canine impaction in mixed and early permanent dentition-a systematic review and meta-analysis. Int Orthod. 2021;19:548-65.
- [CrossRef] [PubMed] [Google Scholar]
- Influence of radiographic position of ectopic canines on the duration of orthodontic treatment. Angle Orthod. 2009;79:442-6.
- [CrossRef] [PubMed] [Google Scholar]
- The sequential hypothesis of impaction of maxillary canine-a hypothesis based on clinical and radiographic findings. J Craniomaxillofac Surg. 2012;40:e375-85.
- [CrossRef] [PubMed] [Google Scholar]
- Early prediction of maxillary canine impaction. Dentomaxillofac Radiol. 2016;45:20150232.
- [CrossRef] [Google Scholar]
- Assessment of the root apex position of impacted maxillary canines on panoramic films. Am J Orthod Dentofac Orthop. 2017;152:489-93.
- [CrossRef] [PubMed] [Google Scholar]
- A treatment difficulty index for unerupted maxillary canines. Eur J Orthod. 2006;28:141-4.
- [CrossRef] [PubMed] [Google Scholar]
- Investigation of impacted permanent teeth except the third molar in Chinese patients through an X-Ray study. J Oral Maxillofac Surg. 2010;68:762-7.
- [CrossRef] [PubMed] [Google Scholar]
- Prevalence and characteristics of impacted maxillary canines in southern Chinese children and adolescents. J Investig Clin Dent. 2014;5:38-44.
- [CrossRef] [PubMed] [Google Scholar]
- Surgically assisted orthodontic alignment of impacted maxillary canines: A retrospective analysis of functional and esthetic outcomes and risk factors for failure. Am J Orthod Dentofac Orthop. 2021;159:e461-71.
- [CrossRef] [PubMed] [Google Scholar]
- Pre-treatment radiographic features for the periodontal prognosis of treated impacted canines. J Clin Periodontol. 2007;34:581-7.
- [CrossRef] [PubMed] [Google Scholar]
- Dentoskeletal features associated with unilateral or bilateral palatal displacement of maxillary canines. Angle Orthod. 2004;74:725-32.
- [Google Scholar]
- Retrospective evaluation of treatment time and efficiency of a predictable cantilever system for orthodontic extrusion of impacted maxillary canines. Am J Orthod Dentofacial Orthop. 2018;154:55-64.
- [CrossRef] [PubMed] [Google Scholar]
- Orthodontic considerations in the treatment of maxillary impacted canines. Am J Orthod. 1982;81:236-9.
- [CrossRef] [PubMed] [Google Scholar]
- Evaluation of impacted maxillary canine position using panoramic radiography and cone beam computed tomography. Saudi Dent J. 2021;33:738-44.
- [CrossRef] [PubMed] [Google Scholar]
- Dental anomalies and clinical features in patients with maxillary canine impaction. Angle Orthod. 2013;83:22-8.
- [CrossRef] [PubMed] [Google Scholar]
- Early prediction of maxillary canine impaction from panoramic radiographs. Am J Orthod Dentofac Orthop. 2012;142:45-51.
- [CrossRef] [PubMed] [Google Scholar]
- Prediction of maxillary canine impaction using sectors and angular measurement. Am J Orthod Dentofacial Orthop. 2003;124:651-5.
- [CrossRef] [PubMed] [Google Scholar]
- Factors associated with the duration of forced eruption of impacted maxillary canines: A retrospective study. Am J Orthod Dentofac Orthop. 2006;130:349-56.
- [CrossRef] [PubMed] [Google Scholar]
- An evaluation of factors affecting duration of orthodontic treatment. Am J Orthod Dentofac Orthop. 1999;115:439-47.
- [CrossRef] [PubMed] [Google Scholar]
- The reliability of crown-root ratio, linear and angular measurements on panoramic radiographs. Clin Orthod Res. 2000;3:182-91.
- [CrossRef] [PubMed] [Google Scholar]
- Cone-beam computed tomography and the orthosurgical management of impacted teeth. J Am Dent Assoc. 2010;141:14S-8.
- [CrossRef] [PubMed] [Google Scholar]




