

Translate this page into:
Mandibular canine development as an indicator of maxillary cleft site canine development

*Corresponding author: Matthew Brian Harper, Department of Dentistry, Boston Children’s Hospital, Boston, Massachusetts, United States. matthew.harper@childrens.harvard.edu
-
Received: ,
Accepted: ,
How to cite this article: Harper MB, Ross E, MacLaine J, Padwa BL, Aldosari M. Mandibular canine development as an indicator of maxillary cleft site canine development. APOS Trends Orthod. 2024;14:109-14. doi: 10.25259/APOS_172_2023
Abstract
Objectives:
The objective of this study was to determine if mandibular canine development is an indicator of maxillary cleft site canine development.
Material and Methods:
A cross-sectional chart review with analysis of cone-beam computed tomography (CBCT) imaging of patients aged 7–12 with a unilateral complete cleft lip and palate who received alveolar bone graft surgery from January 2009 to January 2019. Three-dimensional (3D) measurements of the cleft site canine and ipsilateral mandibular canine were taken. A two-dimensional image was created from the 3D CBCT to simulate a traditional panoramic radiograph. Descriptive statistics and multivariable linear regression analyses were conducted, adjusting for age and gender. Pearson and Spearman correlations were calculated. The main outcome measure was the mandibular canine crown-to-root ratio (C:RR) compared to that of the maxillary cleft site canine C:RR.
Results:
Five hundred and thirteen patients were reviewed, of which 78 met the inclusion criteria. Adjusting for age and gender, every unit change in mandibular canine C:RR corresponds to 0.69 (95% confidence interval [CI] = 0.42–0.95) change in maxillary canine C:RR, up to a mandibular canine C:RR of 3. Beyond a mandibular C:RR of 3, no change in the maxillary canine C:RR was observed (−0.02; 95%CI = −0.27–0.24). Pearson correlation coefficient was r = 0.65, and the Spearman correlation was P = 0.75.
Conclusion:
Mandibular canine C:RR is correlated to maxillary cleft site canine C:RR when the mandibular canine C:RR is ≤3.
Keywords
Cleft lip and palate
Orthodontics
Crown-to-root ratio
Cone-beam computed tomography

INTRODUCTION
There exists some discrepancy as to the ideal timing to perform an alveolar bone graft in patients with cleft lip ± palate (CL±P). While some report successful grafts in the primary or early mixed dentition when patients are 5–6 years old,[1,2] many surgical centers recommend grafting during the late mixed dentition before the eruption of the permanent maxillary canines.[3-5]
Current practice for determining the optimal time for alveolar bone grafting in patients with CL±P involves estimating when the maxillary cleft site canine will erupt based on the degree of root development.[6,7] Typically, patients with CL±P are assessed radiographically using a two dimensional (2D) panoramic radiograph; however, canine position adjacent to the cleft site is often significantly altered as a result of the cleft.[8] In addition, many patients with CL±P have maxillary hypoplasia,[9] and therefore, the maxillary cleft site canine is often displaced outside the focal trough of the panoramic image. As a result of the variations in tooth and arch position, the maxillary cleft site canine can appear distorted,[10] while the mandibular dentition is often more reliably imaged in panoramic radiographs.[11] Due to the limitations of 2D imaging, clinicians often recommend more extensive three-dimensional (3D) imaging[10],which increases patient exposure to ionizing radiation.[12]
If mandibular canines are more reliably measured in traditional 2D imaging, the relationship between the development of the mandibular canine and the maxillary cleft site canine could be informative for practitioners without access to 3D imaging. The primary aim of this study was to determine whether mandibular canine development is an indicator of maxillary cleft site canine development.
MATERIAL AND METHODS
Study design and population
A cross-sectional chart review and analysis of cone-beam computed tomography (CBCT) imaging for patients who underwent alveolar bone grafting from January 2009 to January 2019 at Boston Children’s Hospital was performed. All children with a diagnosis of unilateral complete cleft lip and palate (CLP) who had a pre-operative CBCT taken between the ages of 7 and 12 years were included in the study. Included patients had a CBCT taken of the mandible and maxilla, such that both mandibular and maxillary canines could be reviewed. The included patients had this CBCT taken in preparation for an upcoming alveolar bone graft. Patients with clefts associated with syndromes (e.g., Van der Woude syndrome) were excluded from this study. In addition, patients with any congenitally missing canine teeth were excluded from the study. Demographic information was collected from electronic health records, including age at the time of surgery, age at the time of CBCT imaging, gender, race, and cleft diagnosis.
Radiographic assessment of outcomes
Measurements of the cleft site canine and ipsilateral mandibular canine were taken in both 2D and 3D. The 3D measurements were made directly from CBCT imaging. Measurements were taken from a sagittal view of the canine corresponding to the mid-facial section of the tooth, along the long axis [Figure 1a]. Measurements of crown length and canine length were recorded separately. Canine length was measured from the incisal edge to the most apically appearing calcified tooth structure. Crown length was measured along the long axis of the tooth, from incisal edge to the intersection of a line drawn perpendicular from the cementoenamel junction (CEJ) on the facial surface. Root length was then calculated as the difference between canine length and crown length. In this study, crown-to-root ratio (C:RR) was reported as an absolute number as opposed to a ratio. It was calculated by dividing the crown length by the root length. For example, a C:RR of 2:1 was represented as a value of 2.

- Measurements taken of maxillary cleft site canine and ipsilateral mandibular canine. Images taken from “dolphin imaging software”. (a) Green arrow specifies measurement of canine length taken in three-dimensional imaging. (b) White lines specify measurement of canine length taken in two-dimensional imaging.
The 2D measurements were made from a panoramic radiograph that was fabricated from the same CBCT [Figure 1b]. The process for building the panoramic images was based on replicating the typical positioning settings that would be used to obtain a standard panoramic image from a conventional in-office panoramic radiograph system. The patient’s head was carefully positioned using Frankfort horizontal landmarks of orbitale and porion.[13] Measurements of canine length were taken from this 2D image using the same landmarks as those in 3D, this time measured along the long axis of the tooth at the mid-facial surface. All measurements were made using a single computer program by a single clinician Matthew B. Harper (MBH) who is experienced with the software (dolphin imaging and management solutions, Patterson dental; Chatsworth, CA, USA). As an innate component of the CBCT and imaging software, all measurements taken from the 3D image were recorded in millimeters without a magnification factor. To account for variation in magnification of the 2D imaging, each panoramic radiograph was created with a millimeter ruler bar. To assess the intra-examiner reliability, 10 patients were selected at random for repeat measurements three months after the initial data collection.
Statistical analysis
Descriptive statistics, reporting the distribution of the demographic characteristics and the average age of the patients included in our sample, were performed. Paired t-tests were used to evaluate the difference between 2D and 3D measurements for the mandibular and maxillary canines separately. To estimate the change in maxillary canine C:RR (dependent variable) with each unit change in mandibular canine C:RR (independent variable), a multivariable linear regression was performed, adjusting for age and gender. After plotting the maxillary and mandibular canine C:RR ratio in a scatter plot, a spline term was added to the linear regression at a mandibular canine C:RR of 3, after which the relationship changes. In addition, Pearson and Spearman correlations were calculated to assess the strength of the linear relationship.
A power calculation determined that 46 patients were needed to detect a difference of 0.685 or larger between the maxillary and mandibular canine C:RR, with 80% power and alpha (α) of 0.05. All statistical analyses were performed using Stata/SE Version 15.1 (StataCorp, College Station, TX).
RESULTS
Five hundred and thirteen patients were reviewed, of which 78 met the inclusion criteria. The most common reason for exclusion was a cleft diagnosis other than unilateral complete CLP (213 patients or 42%). Many patients were also excluded due to inadequate imaging for the study criteria (117 patients or 23%). The mean age at the time of imaging of included patients was 9.4 years (standard deviation ± 1.0 years), 55% of patients were male, and 63% had a left-sided cleft [Table 1].
| n(%) | |
|---|---|
| Gender | |
| Male | 43 (55) |
| Female | 35 (45) |
| Laterality | |
| Left | 49 (63) |
| Right | 29 (37) |
| Race/ethnicity | |
| Caucasian | 28 (36) |
| Asian | 24 (31) |
| Hispanic | 8 (10) |
| African American | 3 (4) |
| Other | 5 (6) |
| Declined | 10 (13) |
| Age* | |
| Minimum | 7.2 years |
| Maximum | 12.0 years |
| Average | 9.3 Years |
| Standard deviation | ±1.02 years |
Canine 2D panoramic measurements were compared to 3D CBCT measurements. The mandibular canine length measured from the panoramic radiograph closely matched that of the 3D CBCT, with an average difference of only 0.19 mm (P > 0.05). In contrast, 2D maxillary canine measurements differed significantly from the 3D imaging measurements by 0.42 mm (P < 0.05) [Figure 2]. The intra-examiner average absolute agreement of interclass correlation for all measurements ranged between 0.92 and 0.99, indicating excellent examiner reliability.

- Average maxillary and mandibular canine length measurements from two-dimensional and three-dimensional images; *indicates statistical significance (P < 0.05).
Average C:RR of the mandibular canines was 1.94 and 2.05 for maxillary canines [Figure 3]. The relationship between these two measurements for each patient is displayed in a scatter plot [Figure 4]. When the mandibular C:RR was ≤ 3, there was a direct relationship between mandibular C:RR and maxillary CC: R. After adjusting for age and gender, each unit change in the mandibular C:RR was associated with a 0.69 change in the maxillary C:RR. For mandibular C:RR above 3, no relationship was observed [Table 2]. Pearson correlation coefficient was r = 0.65, and the Spearman correlation was P = 0.75.
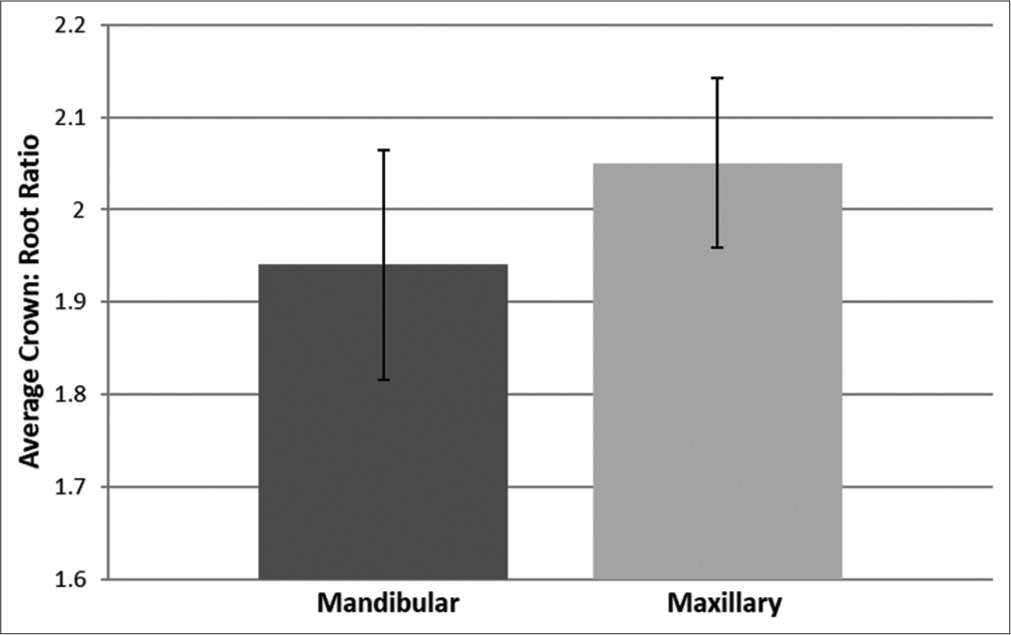
- Average maxillary and mandibular crown-to-root ratio values from three-dimensional images.

- Scatter plot comparing mandibular and maxillary crown-to-root ratio values.
| 2.45 | β0 | |
| Mandibular C:RR | 0.685* | β1 |
| Spline | −0.015 | β2 |
| Gender | −0.332* | β3 |
| Age | −0.156* | β4 |
E (Maxillary C:RR)=β0+β1(Mandibular C:RR <3)+β2 (Mandibular C:RR ≥3)+β3(gender)+β4(age); “E” refers to “Expected Outcome” for Maxillary canine crown-to-root ratio, *indicates statistical significance (P<0.05)
DISCUSSION
It is known that CBCT imaging improves the accuracy of assessing tooth morphology in three dimensions,[14,15] while there is anticipated distortion of teeth when assessed with 2D panoramic imaging due to variation in X-ray beam angulation and overlap of adjacent anatomic structures.[11]
It has been demonstrated in the past that CBCT is sensitive enough to identify the CEJ of a tooth.[16]
The results of this study suggest that 2D panoramic imaging fabricated from CBCT provides an accurate estimate of the mandibular canine’s true length in 3D, and a less reliable measurement of maxillary cleft site canines. Although there was a statistically significant result in the maxillary data set with an average difference of 0.42 mm between 2D and 3D measurements, this is unlikely to be clinically significant. While the results validate a higher degree of accuracy in measuring mandibular canines comparatively, it appears that the accuracy of measuring maxillary cleft site canines from a 2D image may be higher than previously thought.
The current literature shows there is less distortion of mandibular dentition than that of the maxillary dentition in a traditional 2D panoramic radiograph.[17] It is likely that the maxillary canines in our study were imaged more clearly than expected due to a limitation in the study design. When building the panoramic radiograph from CBCT imaging, the software requires a custom-drawn focal trough to be traced. The focal trough, however, is not customizable in a traditional panoramic radiograph system, which likely results in a higher inaccuracy in measuring the maxillary cleft site canine on 2D panoramic radiographs.
Overall, the canine teeth measurements from this study seem to be fairly consistent with existing literature. The average mandibular canine crown length in this study was 10.3 mm, which is similar to the reported values in the literature of 10.3 mm[18] and 11 mm.[19] The average maxillary canine crown length in this study was 10.4 mm, which is in between the reported values of 9.5 mm[18] and 10.8.[20] Slight variation in measurements may be due to the fact that the study population consisted of patients with CLP. There is no reported difference in canine C:RR between patients with and without CLP.[21] However, the majority of the reported literature on tooth measurements uses study populations that are healthy and Caucasian. The incidence of CLP is known to vary with different racial and ethnic groups.[22] Our study population was consistent with the literature for the prevalence of CLP among the American population,[22-24] with a higher proportion of Asian and Hispanic patients and a lower proportion of African American patients [Table 1].
The regression analysis suggests that a relationship exists between the C:RRs of the mandibular canines and the maxillary cleft site canines. It is important to note that this linear relationship is only observed when the mandibular canine C:RR has a value of 3 or less. The average age of patients with a mandibular canine C:RR of 3 or less was calculated. Based on the data collected in this study, the mandibular canine C:RR is 3 or less at an age of 8.7 years in females, and 9.2 years in males. Younger patients who have a mandibular canine C:RR >3 showed no relationship between the mandibular and maxillary canine ratios. This may be due to the fact that measuring the canine at this immature state is unreliable, as there is only minimal root formation completed at this point in development.
This is the first study showing the potential use of mandibular canines as an assessment tool in relation to the developmental stage of the maxillary cleft site canine. The clinical relevance of this data allows clinicians who may not have access to 3D imaging technology to better predict cleft canine development. Alternatively, this data could help determine the best time to expose a patient to 3D imaging to maximize the benefit of this diagnostic tool. A panoramic radiograph taken at an age of approximately nine years or older should provide a clear image of the mandibular canine. The mandibular canine length and crown length can be measured to calculate the C:RR. With this value, using the equation listed in [Table 2], the maxillary cleft site canine C:RR can be estimated. This provides the clinician with a reliable estimate of the maxillary canine tooth development, which may not be clearly imaged in the panoramic radiograph. This information is helpful in estimating the most appropriate timeframe for alveolar bone grafting.
It is understood that the development of the maxillary cleft site canine is only one factor involved in planning for the alveolar bone graft procedure. Decision-making involves other important factors, including but not limited to the presence or absence of a maxillary cleft site lateral incisor, the inclination of the maxillary cleft site canine and its height with respect to the occlusal plane, and the bony and periodontal support in the area of the cleft.[8,25] The purpose of this study was to focus solely on the C:RR of the maxillary cleft site canine thus these other factors were not explored. This study does not negate the value of 3D imaging as it is beneficial to gain insight about factors other than the development of the maxillary cleft site canine.
CONCLUSION
Measurements of the mandibular canine in a 2D panoramic image can be used to estimate maxillary cleft site canine development. This information is useful in determining the best time for alveolar bone grafting. Based on these results, clinicians can appropriately time the following 3D imaging to best prepare for a bone graft procedure.
Acknowledgments
The authors would like to thank Dr. Richard Bruun, DDS for early contributions in the conception of the study. The authors are also grateful to Dr. R. Frederick Lambert, DMD, MPH for helpful discussions and contributions to the writing of the manuscript.
Ethical approval
The study was approved by the Institutional Review Board at Boston Children’s Hospital – protocol J#IRB-P00031536, dated December 2019.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- Evaluation of success of alveolar cleft bone graft performed at 5 years versus 10 years of age. J Craniomaxillofac Surg. 2016;44:21-6.
- [CrossRef] [PubMed] [Google Scholar]
- A new reliable method for alveolar bone grafting at about 6 years of age. J Oral Maxillofac Surg. 2009;67:2045-53.
- [CrossRef] [PubMed] [Google Scholar]
- Increase in age is associated with worse outcomes in alveolar bone grafting in patients with bilateral complete cleft palate. J Craniofac Surg. 2014;25:380-2.
- [CrossRef] [PubMed] [Google Scholar]
- Long-term outcome of secondary alveolar bone grafting in cleft lip and palate patients: A 10-year follow-up cohort study. J Plast Surg Hand Surg. 2013;47:503-8.
- [Google Scholar]
- Elimination of the residual alveolar cleft by secondary bone grafting and subsequent orthodontic treatment. Cleft Palate J. 1986;23:175-205.
- [Google Scholar]
- Prediction of outcome of secondary alveolar bone grafting in children born with unilateral cleft lip and palate. Eur J Orthod. 2003;25:205-11.
- [CrossRef] [PubMed] [Google Scholar]
- Timing of alveolar bone grafting determines different outcomes in patients with unilateral cleft palate. J Craniofac Surg. 2012;23:1283-6.
- [CrossRef] [PubMed] [Google Scholar]
- Canine eruption in patients with complete cleft lip and palate. Cleft Palate Craniofac J. 2008;45:73-80.
- [CrossRef] [PubMed] [Google Scholar]
- Orthognathic surgery for patients with cleft lip and palate. Clin Plast Surg. 2009;46:157-71.
- [CrossRef] [PubMed] [Google Scholar]
- An optimized imaging protocol for orofacial cleft patients. Clin Exp Dent Res. 2018;4:152-7.
- [CrossRef] [PubMed] [Google Scholar]
- Accuracy of the orthopantomogram in assessment of tooth length in orthodontic patients. Singapore Dent J. 2000;23:68-71.
- [Google Scholar]
- Radiation protection in dental radiology-recent advances and future directions. Phys Med. 2017;44:222-6.
- [CrossRef] [PubMed] [Google Scholar]
- Orientation-sella-nasion or Frankfort horizontal. Am J Orthod. 1976;69:648-54.
- [CrossRef] [PubMed] [Google Scholar]
- Crown and root lengths of incisors, canines, and premolars measured by cone-beam computed tomography in patients with malocclusions. Korean J Orthod. 2013;43:271-8.
- [CrossRef] [PubMed] [Google Scholar]
- Reproducibility and accuracy of measuring unerupted teeth using limited cone beam X-ray CT. Dentomaxillofac Radiol. 2007;36:2-6.
- [CrossRef] [PubMed] [Google Scholar]
- Accuracy and reliability of cone-beam computed tomography for measuring alveolar bone height and detecting bony dehiscences and fenestrations. Am J Orthod Dentofac Orthop. 2010;137:109-19.
- [CrossRef] [PubMed] [Google Scholar]
- Measurements of tooth length in panoramic radiographs. 1. The use of indicators. Dentomaxillofac Radiol. 1992;21:26-30.
- [CrossRef] [PubMed] [Google Scholar]
- Wheeler's dental anatomy, physiology, and occlusion (9th ed). St. Louis: Saunders Elsevier; 2010. p. :138.
- [Google Scholar]
- Anatomic crown width/length ratios of unworn and worn maxillary teeth in white subjects. J Prosthet Dent. 2003;89:453-61.
- [CrossRef] [PubMed] [Google Scholar]
- Evaluation of teeth development in unilateral cleft lip and palate patients in mixed dentition by using medical image control systems. Niger J Clin Pract. 2018;21:156-62.
- [Google Scholar]
- Cleft lip and palate: Understanding genetic and environmental influences. Nat Rev Genet. 2011;12:167-78.
- [CrossRef] [PubMed] [Google Scholar]
- Birth defects data from population-based birth defects surveillance programs in the United States, 2007 to 2011: Highlighting orofacial clefts. Birth Defects Res A Clin Mol Teratol. 2014;100:895-904.
- [CrossRef] [PubMed] [Google Scholar]
- National Birth Defects Prevention Network: Updated national birth prevalence estimates for selected birth defects in the United States, 2004-2006. Birth Defects Res A Clin Mol Teratol. 2010;88:1008-16.
- [CrossRef] [PubMed] [Google Scholar]
- The presurgical status of the alveolar cleft and success of secondary bone grafting. Cleft Palate Craniofac J. 2000;37:179-84.
- [CrossRef] [PubMed] [Google Scholar]




