

Translate this page into:
An archwire for non-invasive improvement of occlusal cant and soft tissue chin deviation

*Corresponding author: Dr. Eric Jein-Wein Liou, Department of Craniofacial Orthodontics, Chang Gung Memorial Hospital. 6F 199 Tung-Hwa North Road, Taipei, 105, Taiwan. lioueric@ms19.hinet.net
-
Received: ,
Accepted: ,
Abstract
Nonsurgical improvement of an occlusal cant, lip cant, and soft tissue chin deviation has been considered not possible merely through orthodontic treatment without surgical intervention. The purpose of this report was to illustrate a possible new field in orthodontics for a non-invasive improvement of the occlusal cant and soft tissue chin deviation through orthodontic approach by an innovative orthodontic archwire (Yin-Yang wire) and the others.
Keywords
Orthodontic archwire
Occusal cant
Asymmetry

INTRODUCTION
An occlusal cant could be due to an asymmetric pattern of skeletal and/or dentoalveolar development.[1-5] It also could be iatrogenic due to inappropriate orthodontic treatments.[6] During the clinical assessment, we could place a tongue blade across canines or first molars for evaluating the anterior or posterior occlusal cant, respectively.[7] Either the anterior or posterior occlusal plane should coincide with the interpupillary plane.[8]
Orthognathic surgery combined with surgical orthodontics has been a treatment of choices for the correction of an occlusal cant.[1,9,10] In recent years, temporary anchorage devices (TADs) have been applying extensively for the treatment of an anterior or posterior occlusal cant using a range of different biomechanics without orthognathic surgery.[11-14] On the other hand, various nonsurgical treatment options including high-pull headgear, posterior bite blocks, and active magnetic vertical correctors were reported.[15-17] However, these appliances are bulky and all require patient compliance. Noncompliant appliances such as auxiliary intrusion arches or cantilever-typed springs have also been reported.[2,18]
Improvement of an occlusal cant with a continuous archwire without auxiliary wires, TADs, or orthognathic surgery has never been reported yet. The purpose of this report was to present an innovative archwire called Yin-Yang archwire (MEM, Taiwan) for a simple and easy correction of an occlusal cant.
The Yin-Yang archwire
Configuration of archwire
This archwire is pre-fabricated with titanium-molybdenum alloy (TMA) for a good range of springback.[19-21] It is a continuous archwire with a wavy configuration resembling a symbol of yin and yang at the front view, or a combination of curve of Spee and reverse curve of Spee at the side view [Figure 1].
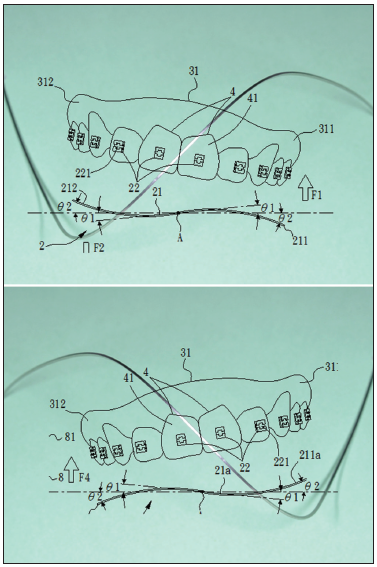
- The configuration and orientation of an Yin-Yang archwire. An orientation of left side up Yin-Yang archwire at the frontal view is for the correction of a left side down occlusal cant. An orientation of right side up Yin-Yang archwire at the frontal view is for the correction of a right side down occlusal cant.
The Yin-Yang archwire has 0.017 × 0.025 and 0.018 × 0.025 wire size series. The 0.017 × 0.025 wire size is for the 18-slot size brackets, and 0.018 × 0.025 is for the 22-slot size brackets. It should be placed from molar to molar in each tooth bracket just like a conventional plain archwire.
It has 60º and 100° up-and-down configurations. The 100° is for the correction of a cant in the beginning, and the 60° is to maintain the correction [Figure 1].
Mechanics of archwire
The mechanics of a Yin-Yang archwire is reciprocal extrusion and intrusion between right and left. The wavy down wire configuration is to extrude teeth, and the wavy up wire configuration is to intrude teeth. The magnitude of extrusion and intrusion is equal and reciprocal. The extrusion is an anchorage for the intrusion, and the intrusion is an anchorage for the extrusion.
To complete the reciprocal mechanics between extrusion and intrusion at the posterior, a transpalatal arch (TPA) or lingual holding arch (LHA) together with a Yin-Yang archwire are necessary for the correction of a posterior and anterior occlusal cant. TPA and LHA may be not necessary for a correction of anterior occlusal cant only.
Selection of archwire
It has two orientations. To select a proper orientation for the occlusal cant correction, orient the archwire so that both ends of the archwire are at the same level and then check the up-and-down orientation at the anterior. A right side up occlusal cant should be corrected by an Yin-Yang archwire with a right side down and left side up orientation at the anterior. A left side up occlusal cant should be corrected by an Yin-Yang archwire with a left side down and right side up orientation at the anterior [Figure 1].
CASE REPORT
Clinical assessments
A 21-year-old female patient seeking for no jaw bone surgery reported to the orthodontic department with a chief complaint of “sticking out and crooked front teeth and a skewed face.” Clinical evaluation disclosed the presence of a 2.5 mm chin deviation to the left at soft tissue Pog in reference to the facial midline, a 5.8° left side up lip-line cant, 7.5° left side up uneven maxillary gingival line and occlusal cant in reference to the interpupillary line, and a left side up roll rotation excessive gummy smile. Intraoral findings included an Angle Class I molar relationship, 3.0 mm OB, 3.0 mm OJ, lower dental midline deviating to the right 1.5 mm in reference to the facial midline, upper, and lower moderate anterior crowding, and proclined upper and lower anterior teeth [Figure 2].

- The pre-treatment extraoral and intraoral photographs of a case of Class I bimaxillary protrusion with facial asymmetry, chin deviation, lip cant, gummy smile, and maxillary occlusal cant.
Three-dimensional cone-beam computed tomography analysis
Three-dimensional cone-beam computed tomography (3D CBCT) analysis revealed a Class I skeletal jaw bone relationship with bimaxillary dentoalveolar protrusion, a 3.0 mm mandibular deviation to the left at Pog in reference to the mid-sagittal plane perpendicular to the floor, and a 7.5° left side up maxillary anterior occlusal cant (canine to canine) and 2.5° left side up posterior occlusal cant (1st molar to 1st molar) in reference to the FH plane [Figure 3].

- The pre-treatment 3D CBCT of the case revealed bimaxillary protrusion with mandibular asymmetry and a left side up maxillary occlusal cant.
Treatment goals and treatment plan
Since the patient asked for non-surgical treatment, the treatment goals were non-surgical approaches to improve the anterior crowding, bimaxillary dentoalveolar protrusion, gummy smile, uneven maxillary gingival line, and occlusal cant, but ignore the soft tissue lip-line cant and chin deviation.
Orthodontic treatment plan with extraction of the maxillary 2nd premolars (had resin restorations) and mandibular 1st premolars for the relief of anterior crowding and improvement of bimaxillary dentoalveolar protrusion, intrusion of maxillary anterior teeth using intruding cantilever arms for the gummy smile, and the Yin-Yang archwires for the maxillary and mandibular occlusal cant was the treatment of choice after the patient had been well-informed consent.
Sequence of orthodontic treatment
The sequence of orthodontic treatment was first extraction of the upper and lower premolars, and alignment and leveling for relieving upper and lower anterior crowding. The maxillary and mandibular anterior teeth were then retracted and intruded for space closure and improving the bimaxillary protrusion and excerssive gummy smile. After the space closure, the occlusal cant was corrected by using the Yin-Yang archwires. The final step was the lower dental midline correction and detailings.
Treatment appliances and mechanics
The upper and lower dentitions were bonded with 0.022 slot ceramic self-ligating brackets and aligned and leveled with 0.014 and 0.016 × 0.022 NiTi archwires first for 2.5 months after the extraction.
The maxillary and mandibular en masse retraction-and-intrusion was completed rapidly in 6.5 months by the submucosal injection of platelet-rich plasma in the upper and lower anterior teeth,[22] upper and lower 0.016 × 0.022 SS as the main archwires, NiTi coil springs for the anterior retraction, and 0.017 × 0.025 TMA intrusive lever arms for the anterior intrusion [Figure 4].

- The mechanics and appliances for the maxillary and mandibular en masse retraction.
After the extraction space closure and en masse maxillary and mandibular en masse retraction-and-intrusion, the left side up lip cant and occlusal cant were improved slightly, but the chin deviation remained unchanged [Table 1]. An upper Yin-Yang archwire followed by a lower Yin-Yang archwire was placed for 6 months to further improve the maxillary and mandibular occlusal cant [Figure 5].

- An orientation of left side down and right side up maxillary Yin-Yang archwire was applied for correcting the left side up and right side down lip cant and maxillary occlusal cant after the extraction space had been closed of the case.
| Measurements | T0 | T1 | T2 | T3 |
|---|---|---|---|---|
| Clinical LC | 5.8° | 4.1° | 2.0° | 1.3° |
| Clinical OC | 7.5° | 4.7° | 0.5° | 1.0° |
| CBCT OC | 7.5° | NA | 0.5° | NA |
| Clinical CD | 2.5 mm | 2.5 mm | 0.0 mm | 0.0 mm |
| CBCT CD | 3.0 mm | NA | 3.0 mm | NA |
LC: Lip cant, OC: Occlusal cant, CD: Chin deviation, CBCT: Cone-beam computed tomography
Finally, Class II elastics were used on the right side for the midline correction and the treatment was completed 1 year after placement of the upper Yin-Yang wire. Patient was given lingual bonded and Essix retainers for maintenance [Figure 6].

- The post-treatment extraoral and intraoral photographs revealed the bimaxillary protrusion, chin deviation, lip cant, gummy smile, and the left side up maxillary occlusal cant were improved of the case.
Post-treatment clinical assessments
Clinical assessments of the treatment result revealed that the 2.5 mm chin deviation to the left at soft tissue Pog was almost corrected in reference to the facial midline, the 5.8° left side up lip cant was improved to 2.0°, the 7.5° left side up uneven maxillary gingival line and occlusal cant was improved to 0.5° in reference to the interpupillary line, and a left side up roll rotation excessive gummy smile was improved to an even and balancing smile. The smile arc also coordinated with the lower lip during smile [Figure 6].
Intraorally, the Angle Class I molar relationship was maintained, the 3.0 mm OB and 3.0 mm OJ were improved, lower dental midline deviating to the right 1.5 mm was corrected in reference to the facial midline, upper and lower moderate anterior crowding was relieved, and the proclaimed upper and lower anterior teeth were improved and uprighted [Figure 6].
Pre-treatment and Post-treatment 3D CBCT assessments and superimpositions
3D CBCT analysis revealed a Class I skeletal jaw bone relationship was maintained, bimaxillary dentoalveolar protrusion was improved, a 3.0 mm mandibular deviation to the left at Pog remained uncorrected before and after the treatment in reference to the mid-sagittal plane perpendicular to the floor, the 7.5° left side up maxillary anterior occlusal cant was improved to 0.5°, and the 2.5° left side up posterior occlusal cant was improved to 1.3° in reference to the FH plane [Figure 7] [Table 1].

- The post-treatment three-dimensional (3D) cone-beam computered tomograph, and the pre- and post-treatment 3D image superimposition of the case revealed the maxillary occlusal cant was corrected through the intrusion of the right side maxillary anterior teeth and extrusion of the left side maxillary anterior teeth. The silver color is pre-treatment, and the red color is post-treatment.
Clinical assessment of 12 months post-treatment follow-up
Clinical assessments of the 12 months post-treatment revealed that the soft tissue Pog correction in reference to the facial midline was maintained, the lip cant was 1.3° left side up, and the anterior occlusal cant was 1.0° left side up. The smile arc coordinated with the lower lip during a smile. Intraorally, the Angle Class I molar relationship, OB, OJ, and dental midline were maintained. Although the anterior occlusal cant relapsed slightly, the treatment results remained balancing and stable [Figure 8] [Table 1].

- The 1-year post-treatment follow-up revealed the treatment results are stable.
DISCUSSION
The left side up anterior occlusal cant improved 7.0° in this report. This was due to both the auxiliary intrusive arms and Yin-Yang archwire. The auxiliary intrusive lever arms firstly contributed for 40% (2.8/7.0) of the improvement in 6.5 months of en masse anterior retraction, and the Yin-Yang archwire secondarily contributed for 60% (4.2/7.0) of the improvement in 6 months. In comparison to the auxiliary intrusive lever arms, the Yin-Yang archwire was more effective for the improvement of anterior occlusal cant.
The mechanics of auxiliary intrusive lever arms is similar to the auxiliary intrusion arches or cantilever-typed springs reported before.[2,18] The auxiliary intrusive lever arms might improve the anterior occlusal cant through the uneven intrusion of the maxillary anterior teeth between the right and left. However, this uneven intrusion of anterior teeth also oppositely extruded the right and left posterior teeth unevenly and worsened the posterior occlusal cant. Instead of worsening, the posterior occlusal cant of this report was improved from 2.5° to 1.2° (1.3° improved), and this would be due to the Yin-Yang archwire.
For a left side up posterior occlusal cant, a TPA/LHA with buccal crown torque on the right side and palatal/lingual crown torque on the left side could reinforce the posterior cant improvement biomechanically. On the opposite, a TPA/LHA with palatal/lingual crown torque on the right and buccal crown torque on the left could reinforce the improvement of a right side up posterior occlusal cant.
The most controversial point of this report is the lip cant which was improved both after the improvement of the bimaxillary dentoalveolar protrusion and occlusal cant, and furthermore the soft tissue chin deviation improved after the improvement of occlusal cant by the Yin-Yang archwire, although the skeletal mandibular asymmetry remained the same after treatment. This is contradicted to the conventional orthodontic concept that the soft tissue asymmetry could not be improved without correction of the underlying skeletal asymmetry through orthognathic surgery.
It has been revealed that the lip thickness and shape are different during relaxation or contraction of circumoral musculature,[23] and the lip-line canting at rest is related to the right-left difference of muscular activity of the zygomaticus major.[7] One of the assumptions to explain for the reasons why the lip cant was improved without orthognathic surgery in this report is the changes of muscle tone of the circumoral musculature, such as the mentalis, depressor anguli oris, depressor labial inferioris, zygomaticus major, levator labii superioris, or orbicularis oris muscular were uneven before the tretment, and became relaxed and evenly balancing and changed the soft tissue asymmetry after correction of the bimaxillary protrusion and occlusal cant. However, this assumption needs further clinical studies to be proven.
The improvement of soft tissue chin deviation without surgical improvement of the underlining mandibular asymmetry has never been reported before, and it is not possible to answer the reasons merely from this report. Although the improvement of soft tissue chin deviation of this report was after the application of Yin-Yang archwire, the role of improvement of bimaxillary dentoalveolar protrusion and changes of circumoral musculature on the improvement of soft tissue chin deviation could not be ignored. The improvement of soft tissue chin deviation through orthodontic management without surgical intervention in this report might have opened a completely new window toward a different side in orthodontics that has not been explored before. A clinical study has been undertaken for exploring the possible explanations.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/ their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Facial asymmetry: Etiology, evaluation, and management. Chang Gung Med J. 2011;34:341-51.
- [PubMed] [Google Scholar]
- Biomechanics of orthodontic correction of dental asymmetries. Am J Orthod Dentofacial Orthop. 1995;107:618-24.
- [CrossRef] [Google Scholar]
- An appraisal of growth and reaction to extraoral anchorage. Simulation of orthodontic-orthopedic results. Am J Orthod. 1986;89:113-21.
- [CrossRef] [Google Scholar]
- A concept and classification of centers of rotation and extraoral force systems. Angle Orthod. 1973;43:384-401.
- [PubMed] [Google Scholar]
- Orthodontic considerations for orthognathic surgery In: , ed. Principles of Oral and Maxillofacial Surgery. Philadelphia, PA: J.B. Lippincott Co.; 1992. p. :1237.
- [Google Scholar]
- Undesirable canting of the occlusal plane during orthodontic treatment. J Clin Orthod. 2007;41:757-61.
- [PubMed] [Google Scholar]
- Correlations of frontal lip-line canting with craniofacial morphology and muscular activity. Am J Orthod Dentofacial Orthop. 2007;132(278):e7-14.
- [CrossRef] [PubMed] [Google Scholar]
- Dental smile esthetics: The assessment and creation of the ideal smile. Semin Orthod. 2012;18:193-210.
- [CrossRef] [Google Scholar]
- Severe class II malocclusion with facial asymmetry treated with intraoral vertico-sagittal ramus osteotomy and leFort I osteotomy. Am J Orthod Dentofacial Orthop. 2009;135:809-19.
- [CrossRef] [PubMed] [Google Scholar]
- Orthodontic-orthognathic surgical treatment in a patient with class II subdivision malocclusion: Occlusal plane alteration. Am J Orthod Dentofacial Orthop. 2011;140:703-12.
- [CrossRef] [PubMed] [Google Scholar]
- Correction of a canted occlusal plane with miniscrews in a patient with facial asymmetry. Am J Orthod Dentofacial Orthop. 2006;130:244-52.
- [CrossRef] [PubMed] [Google Scholar]
- Titanium screw anchorage for correction of canted occlusal plane in patients with facial asymmetry. Am J Orthod Dentofacial Orthop. 2007;132:237-42.
- [CrossRef] [PubMed] [Google Scholar]
- Management of occlusal canting with miniscrews. Angle Orthod. 2014;84:737-47.
- [CrossRef] [PubMed] [Google Scholar]
- Use of rhythmic wire system with miniscrews to correct occlusal-plane canting. Am J Orthod Dentofacial Orthop. 2010;137:540-7.
- [CrossRef] [PubMed] [Google Scholar]
- Intrusion of overerupted molars by corticotomy and magnets. Am J Orthod Dentofacial Orthop. 2001;120:209-16.
- [CrossRef] [PubMed] [Google Scholar]
- Contemporary Orthodontics (2). St. Louis: Mosby Year Book; 1993. p. :226-7.
- The performance of bonded magnets used in the treatment of anterior open bite. Am J Orthod Dentofacial Orthop. 1996;109:549-56.
- [CrossRef] [Google Scholar]
- Optimal welding of beta titanium orthodontic wires. Am J Orthod Dentofacial Orthop. 1987;92:213-9.
- [CrossRef] [Google Scholar]
- Thermal and mechanical characteristics of stainless steel, titanium-molybdenum, and nickel-titanium archwires. Am J Orthod Dentofacial Orthop. 2007;131:229-37.
- [CrossRef] [PubMed] [Google Scholar]
- A review of contemporary archwires: Their properties and characteristics. Angle Orthod. 1997;67:197-207.
- [PubMed] [Google Scholar]
- The development of submucosal injection of platelet rich plasma for accelerating orthodontic tooth movement and preserving pressure side alveolar bone. APOS Trends Orthod. 2016;6:5-11.
- [CrossRef] [Google Scholar]
- Ultrasonic investigation of the circumoral musculature. J Anat. 1989;166:121-33.
- [PubMed] [Google Scholar]




