

Translate this page into:
Assessment of stress changes in dentoalveolar and skeletal structures of the mandible with the miniplate anchored Forsus: A three-dimensional finite element stress analysis study
Address for Correspondence: Dr. Pawankumar Dnyandeo Tekale, Department of Orthodontics, Dr Rajesh Ramdasji Kambe Dental College and Hospital, Akola, Maharashtra, India. E-mail: pawan0804@gmail.com
This article was originally published by Wolters Kluwer and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Objective
The study conducted to assess the effects of a fixed functional appliance (Forsus Fatigue Resistant Device; 3M Unitek, Monrovia, CA, USA) on the mandible with three-dimensional (3D) finite element stress analysis.
Materials and Methods
A 3D finite element model of mandible with miniplate at mandibular symphysis was prepared using SolidEdge software along with the plate geometry. The changes were deliberated with the finite element method, in the form of highest von Mises stress and maximum principal stress regions.
Results
More areas of stress were seen in the model of the mandible at cortical bone in canine region at bone and miniplate interface.
Conclusions
This fixed functional appliance studied by finite element model analysis caused more von Mises stress and principal stress in both the cortical bone and the condylar region.
Keywords
Anchorage
fixed functional appliances
skeletally anchored Forsus

INTRODUCTION
The orthodontic treatment is aimed toward the correction of underlying dental or skeletal malocclusion achieving the treatment outcome as pleasant facial profile, healthy periodontium, proper position of condyles in fossa of temporomandibular joint and an acceptable occlusion.[1]
Most commonly observed class II malocclusion, affects approximately one-third of the patients pursuing orthodontic treatment.[2,3] The treatment options for the corrections of class II malocclusion in growing age include the early phase of the functional appliance with growth modification and later the fixed orthodontic treatment.[1,3] In an adult patient, the options for class II corrections include the camouflage or the surgical orthodontics.
McNamara[4] stated mandibular retrusion is one of the most common characteristics of class II malocclusion. Skeletal class II malocclusion with retrognathic mandible can be corrected using several types of removable or fixed functional appliances during active growth. The appliance selection varies rendering to the clinicians’ preference, patient compliance, and growth pattern.[5] The removable functional appliance enables clinician to perform treatment in two phases, beginning with phase I which is mainly directed toward skeletal correction followed by fixed orthodontic treatment in the second phase. The fixed functional appliances, on the other hand, have certain advantages over removable functional appliances, such as less patient cooperation required and simultaneously fixed orthodontic treatment can be carried out thereby reducing treatment duration.[6] Fixed functional appliances enhances more horizontal condylar growth compared with removable appliances thereby enhancing the mandibular growth.[6,7]
Fixed functional appliances are considered to be noncompliant class II correctors; these are Herbst, Jusper Jumper, Twin Force Bite Corrector, Forsus, etc. Previous studies proved the efficiency of those fixed functional appliances; however, distal and intrusive movement of maxillary molars, mesial movement of mandibular molars, labial flaring of mandibular incisors have been reported to be some disadvantages of fixed functional appliances.[8-10] Among all class II correctors, the Forsus™ has proven to be most comfortable to a patient, right from installation itself. The Forsus corrector, not being as forceful as Herbst, allows gradual overpowering of the patient’s oral musculature.[11-13]
Although previously performed studies have proved the efficiency of Forsus, the protrusion of the mandibular incisor was the most common problem which further limits the skeletal effect of the functional appliance.[8,10,12] Aslan et al.[14] used a Forsus FRD appliance combined with a miniscrew, it was concluded that the mandibular incisor protruded significantly. The overjet and molar corrections were dentoalveolar, and no skeletal improvement was concluded. Recently, Celikoglu et al.[15] successfully treated a case having skeletal class II malocclusion due to mandibular retrusion using a Forsus FRD appliance with miniplate anchorage inserted on the mandibular symphysis. Remodeling changes in the condylar head and glenoid fossa been reported after functional appliance treatment and the skeletal class II due to mandibular retrognathism was corrected.
The cephalometric analysis is routinely used to study remodeling changes in the dentofacial complex. The current use of magnetic resonance imaging, cone beam computed tomography (CBCT) in creating the three-dimensional (3D) model of the dentofacial skeleton has improved the accuracy and empathetic of the remodeling changes in the condylar head, glenoid fossa, and dentofacial complex.[16-19] The finite element method (FEM) is applicable to the biomechanical study of strains and stresses produced in internal structures of the craniofacial complex. Chaudhry et al.[20] evaluated the properties of a fixed functional appliance (Forsus Fatigue Resistant Device [FRD]) on the mandible with 3D finite element stress analysis. The study concluded that with the Forsus, a tooth-supported appliance, both the von Mises and principal stresses augmented more in the teeth than in the mandible at the resting stage. Till date, none of the FEM studies was conducted evaluating the von Mises and principal stresses on the mandible with skeletally anchored Forsus.
The purpose of this study was to assess the stress pattern distribution in different parts of the mandible and associated structures with a miniplate (inserted in mandibular symphysis) anchored fixed functional appliance (Forsus FRD) using the FEM with a CT-generated 3D image.
MATERIALS AND METHODS
Bone and tooth morphology were obtained through CT scan and later through reverse engineering. Model was generated in the step file format. The geometries for cortical of 2 mm thickness and inner cancellous bone was separated. Teeth geometry was built after root portions were extracted. Periodontal ligament with 0.2 mm thickness was modeled. The overall geometry was assembled and meshed using HyperMesh (version 11; Altair Engineering, Huntsville, Ala). Different components were created for attaching properties to cortical, cancellous, periodontal ligament, and teeth structure. The geometry was meshed with solid elements. Due to complexity, free mesh was used with solid-45 element properties. The material properties assigned were Young’s modulus (or modulus of elasticity) and the Poisson ratio [Table 1].[18,19]
| Elastic modulus (GPa) | Poison’s ratio | |
|---|---|---|
| Cortical bone | 13.7 | 0.3 |
| Cancellous bone | 1.37 | 0.3 |
| Periodontal ligament | 0.00069 | 0.45 |
| Teeth | 18,600 | 0.3 |
| Implant and plate | 110 | 0.33 |
Model of mandible with miniplate at mandibular symphysis was prepared using SolidEdge software (Siemens, Plano, Tex) along with the plate geometry. The members were imported to HyperMesh for placement and meshing [Figure 1]. The forces generated by fixed functional appliances vary from 150 to 200 g (1.47–1.98 N). Hence, in the present study, forces of 2 N were applied to simulate the application of a fixed functional appliance between the maxillary molars and the mandibular anterior segment.[21] The meshed finite element model was imported and analyzed using Ansys14.5 (version 12.1; Canonsburg, PA) after application of loads. The results for von Mises and principal stresses are represented to know the stress condition.
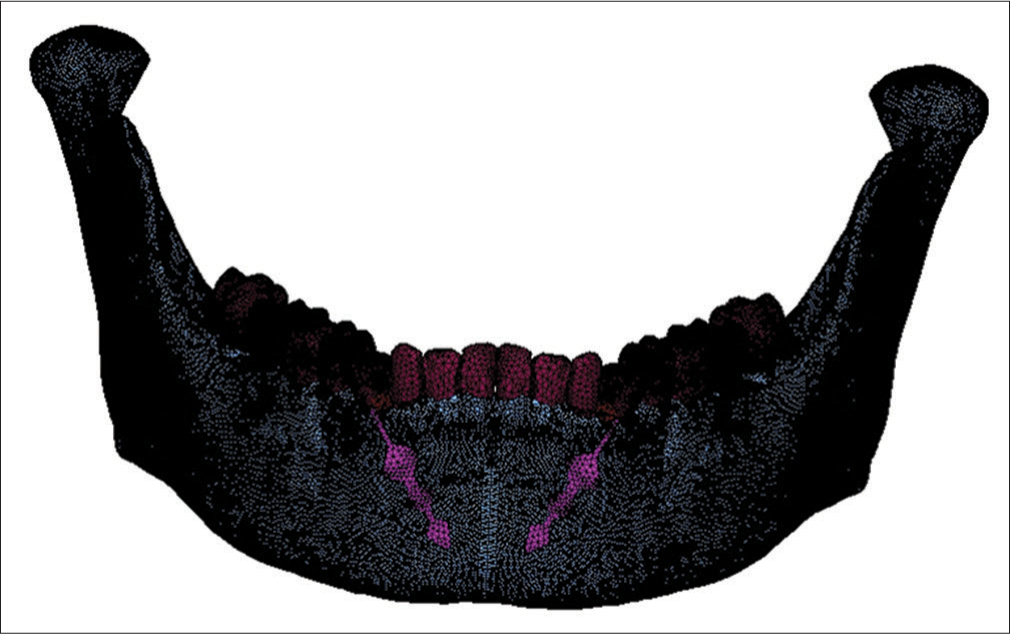
- Mesh model of mandible with miniplate attached to symphysis of mandible
Software used
CT scan, Reverse Engineering Software, SolidEdge, HyperMesh, Ansys Computer: 8GB Ram with 500 GB Hard disc, P5 configuration.
RESULTS
The results presented changes in relations of von Mises stresses and principal stresses. A total of 558,426 elements with 376,242 nodes were used for this study. The schematic color changes represent the areas of maximum and minimum stress when material properties were evaluated. Red displays the maximum principal stress region, which is mainly tensile stress, and blue displays the minimum principal stress region, which was compressive stress.
The results were designed in terms of von Mises and principal stresses in the following regions: cortical bone, cancellous bone, periodontal ligament, teeth, and condyle [Table 2]. The maximum value of von Mises stresses was recorded in mandible when fixed functional appliance loaded 0.713 MPa in the cortical bone [Figure 2], 0.177 MPa in the cancellous bone [Figure 3], 0.009 MPa in the periodontal ligament [Figure 4], 0.552 MPa in the teeth [Figure 5], and 0.397 MPa in the condyle [Figure 6].
| Von Mises stress (MPa) | Principal stress (MPa) | |
|---|---|---|
| Overall | 0.796 | 0.619 |
| Cortical bone | 0.713 | 0.619 |
| Cancellous bone | 0.177 | 0.139 |
| Periodontal ligament | 0.009 | 0.007 |
| Teeth | 0.552 | 0.537 |
| Condoyle | 0.397 | 0.436 |

- Von Mises stress contours in cortical bone
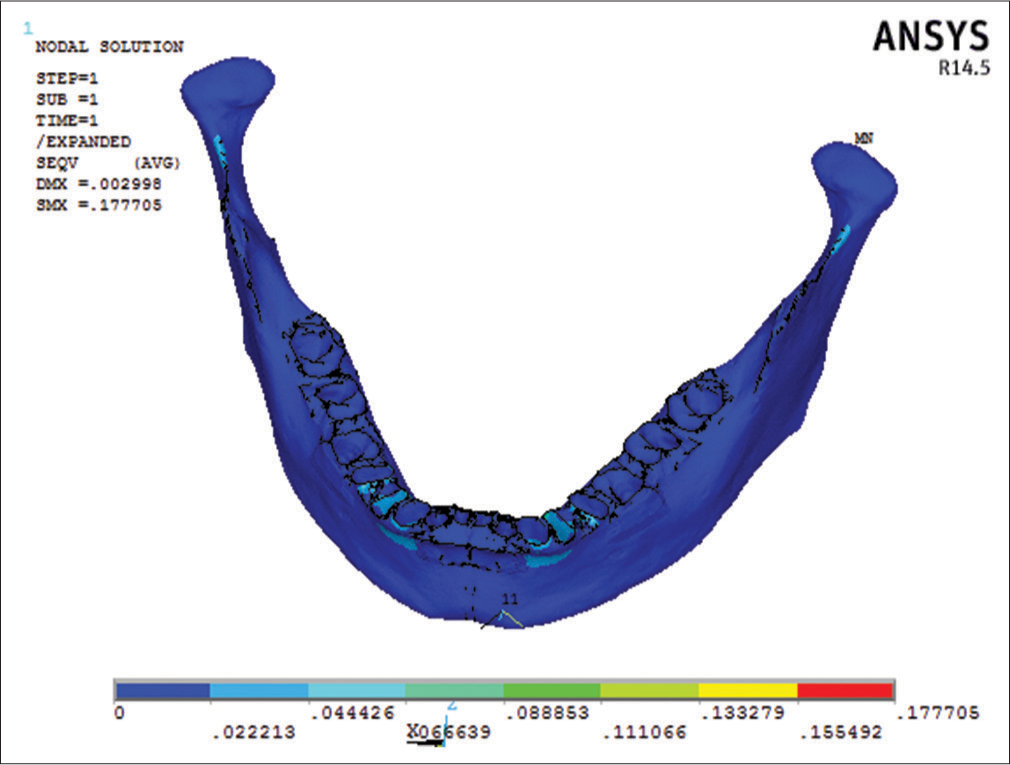
- Von Mises stress contours in cancellous bone
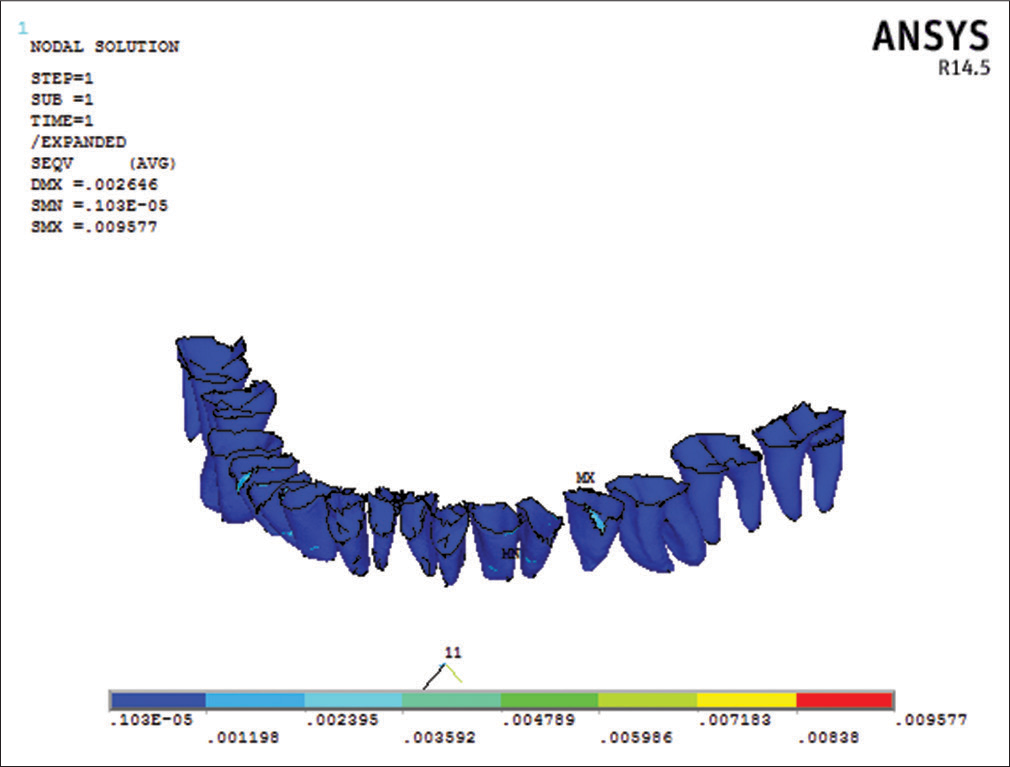
- Von Mises stress contours in periodontal ligament

- Von Mises stress contours in teeth

- Von Mises stress contours in condyle
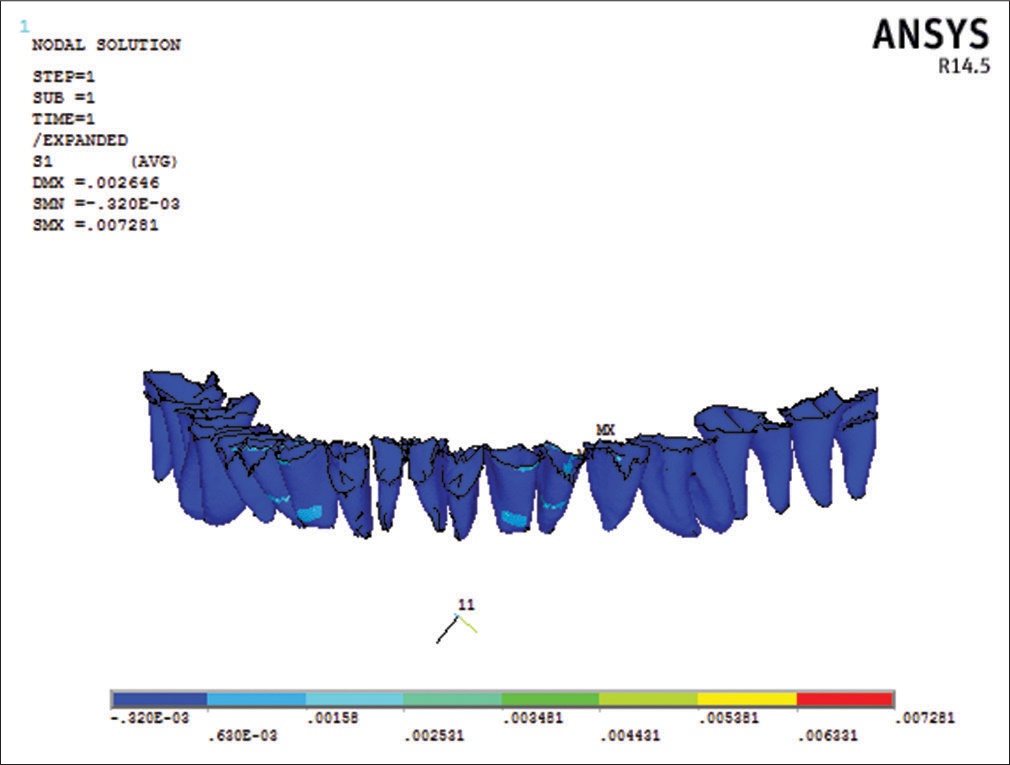
The maximum value of principle stresses was recorded in mandible when fixed functional appliance was loaded 0.619 MPa in the cortical bone [Figure 7], 0.139 MPa in the cancellous bone [Figure 8], 0.007 MPa in the periodontal ligament [Figure 9], 0.537 MPa in the teeth [Figure 10], and 0.436 MPa in the condyle [Figure 11]. Overall Von Mises stress with maximum stress value was 0.796548 MPa and the principle stress with the maximum value was 0.61956 Mpa. The maximum stress was taking place in the cortical section at canine region.

- Principle stress contours in cortical bone
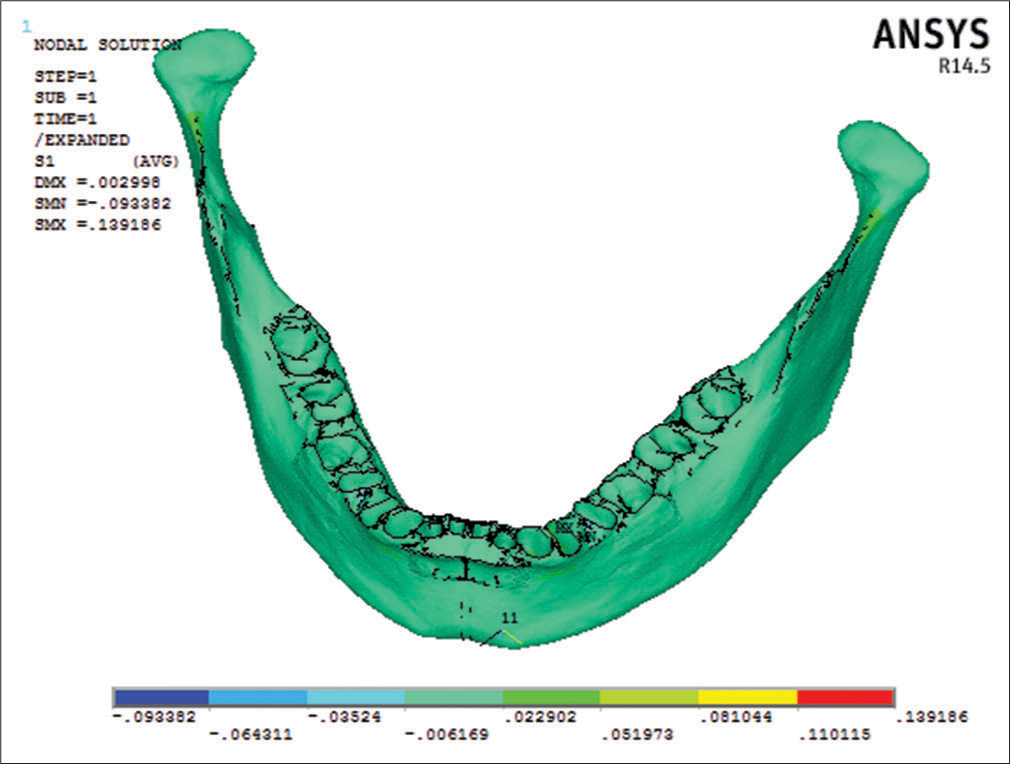
- Principle stress contours in cancellous bone
- Principle stress contours in periodontal Ligament

- Principle stress contours in teeth

- Principle stress contours in condyle
DISCUSSION
Class II malocclusions resulting from orthognathic maxilla and retruded mandible are generally treated with functional orthodontic appliances that create orthopedic forces directed at the mandibular structures. These appliances affect the jaws with the remodeling of the mandibular condyle, remodeling of the glenoid fossa, repositioning the mandibular condyle in the glenoid fossa, and autorotation of the mandibular bone. Among the fixed functional appliances available, Forsus-FRD has long been proved to be one of the best treatment modality for mild to moderate class II malocclusion in spite of its limitation like labial flaring of mandibular incisors.
Giuntini et al.[22] compare the dentoskeletal changes produced by the Twin-block appliance (TB) followed by fixed appliances versus the Forsus FRD in combination with fixed appliances in growing patients having class II division 1 malocclusion. It was concluded that TB appliance produced greater skeletal effects in terms of mandibular advancement and growth stimulation while the Forsus caused significant proclination of the mandibular incisors. Aslan et al.[14] used a Forsus FRD appliance combined with a miniscrew, the overjet and molar corrections were dentoalveolar, mandibular incisors protruded significantly, and no skeletal improvement was concluded. To overcome the protrusion of mandibular incisor and to achieve the skeletal effect, Unal et al.[23,24] evaluate the skeletal, dentoalveolar, and soft tissue effects of the Forsus FRD appliance with miniplate anchorage for the treatment of skeletal class II malocclusion. The result showed that this new approach was an effective method for treating skeletal class II malocclusion due to the mandibular retrusion through a combination of skeletal and dentoalveolar changes.
This combination of fixed functional appliance with miniplate anchorage eliminated the limitations of the tooth and tissue born Forsus. Hence, there was need of evaluation of the skeletal effects of the fixed functional appliance anchored with miniplate. Biomechanical studies have shown that the compressive and tensile stresses from functional orthopedic forces are the key determinants to remodeling of the bones.[25,26]
The present study was conducted to assess the stress pattern distribution in different parts of the mandible and associated structures with a miniplate anchored fixed functional appliance (Forsus FRD) using the FEM with a CT-generated 3D image. The von Mises stress and the principal stress were maximum in the cortical bone at the canine region, and the values were 0.713329 MPa, 0.61956 MPa, respectively. In the cancellous bone, the maximum von Mises stress was recorded at the canine and miniplate interface with value 0.177705 MPa, while the principal stress was 0.139186 MPa. Stress in the periodontal ligament with Maximum von Mises was 0.009577 MPa while principal stress was 0.007 MPa. Von Mises stress in the Teeth Structure with Maximum stress value was 0.552 MPa and principal stress in the teeth structure with Maximum stress value was 0.537227 MPa. von Mises stress in the Condyle region was 0.397 MPa whereas principal stress in the condoyle Region with maximum stress value was 0.436787 MPa.
The previous FEM studies have evaluated the stress in the region of craniofacial complex with functional appliances. Ulusoy and Darendeliler[27] studied the stress region with the FEM in a dry human mandible with the class II activator and the class II activator and high-pull headgear combination. They found that the regions near the muscle attachment areas were affected the most. The inner part of the coronoid process and the gonial area had the maximum stress values. The study concluded that both functional appliances can cause morphologic changes on the mandible by activating the masticatory muscles to change the growth direction. In the present study, the maximum value of von Mises and principal stress were seen in the cortical bone at canine region at bone and miniplate interface. The von Mises and principal stress were found least in the periodontal ligament. Hence from the present study, it is concluded that the miniplate anchored Forsus causes maximum stress in the cortical and cancellous bone at bone and mini-implant interface, thus the stresses were more pronounced in skeletal structures as compared to the dentoalveolar structures.
Panigrahi and Vineeth[21] evaluate displacement and stress distribution on craniofacial structures associated with fixed functional therapy. The study concluded that the fixed functional therapy causes a posterosuperior displacement of the maxillary dentition and pterygoid plate and thus can contribute to the correction of class II malocclusion. The displacement was more pronounced in the dentoalveolar region as compared to the skeletal displacement. All dentoalveolar structures experienced tensile stress, except for anterior nasal spine and the maxillary posterior teeth. In the another study conducted with CBCT scans of the patient to assess the effects of a fixed functional appliance (Forsus FRD; 3M Unitek, Monrovia, CA, USA) on the mandible with 3D FEM analysis. In this study, a 3D finite element model of the mandible was built from the images produced by CBCT of a patient enduring fixed orthodontic treatment. The changes were studied with the finite element method. The study stated that this fixed functional appliance caused an increase in the principal stress and the von Mises stress in both the cortical bone and the condylar region of the mandible by more than 2 times.
In the present study, Von Mises and principal Stress were maximum at cortical bone and condyle. The maximum stress is taking place in the cortical bone section in the canine region at bone and miniplate interface, and minimum stress was found in periodontal ligament. Thus the stresses were more pronounced in skeletal structures as compared to the dentoalveolar structures.
The further finite element analysis study is needed to evaluate the stresses on muscles and retrodiscal tissue that are associated with mandibular opening and forward positioning.
CONCLUSIONS
In this study, we evaluated the stress distribution on the mandible (miniplate anchored Forsus) with finite element analysis. Our conclusions are as follows:
The maximum Von Mises and principal stress values were obtained at the cortical bone in canine region at bone and mini-implant interface
The mandibular cortical bone was subjected to higher stresses than the condylar region.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Prevalence of malocclusion and orthodontic treatment need in the United States: Estimates from the NHANES III survey. Int J Adult Orthodon Orthognath Surg. 1998;13:97-106.
- [Google Scholar]
- Prevalence of malocclusion among adolescents in central Anatolia. Eur J Dent. 2007;1:125-31.
- [Google Scholar]
- Components of class II malocclusion in children 8-10 years of age. Angle Orthod. 1981;51:177-202.
- [Google Scholar]
- Milestones in the development and practical application of functional appliances. Am J Orthod. 1983;84:48-53.
- [CrossRef] [Google Scholar]
- Soft tissue changes with fixed functional appliances in class II division 1. Angle Orthod. 2006;76:712-20.
- [Google Scholar]
- Skeletal effects of bite jumping therapy on the mandible-removable vs. fixed functional appliances. Orthod Craniofac Res. 2005;8:2-10.
- [Google Scholar]
- Class II non-extraction patients treated with the Forsus Fatigue Resistant Device versus intermaxillary elastics. Angle Orthod. 2008;78:332-8.
- [CrossRef] [PubMed] [Google Scholar]
- Forsus Nitinol Flat Spring and jasper jumper corrections of class II division 1 malocclusions. Angle Orthod. 2006;76:666-72.
- [Google Scholar]
- A cephalometric comparative study of class II correction with Sabbagh Universal Spring (SUS (2)) and Forsus FRD appliances. Eur J Dent. 2012;6:302-10.
- [Google Scholar]
- Treatment efficiency in skeletal class II patients treated with the jasper jumper. Angle Orthod. 2007;77:449-56.
- [CrossRef] [Google Scholar]
- Effectiveness of comprehensive fixed appliance treatment used with the Forsus Fatigue Resistant Device in class II patients. Angle Orthod. 2011;81:678-83.
- [Google Scholar]
- Treatment of skeletal class II malocclusion in growing young patient using Forsus appliance. Eur J Clin Orthod. 2016;4:C00261.
- [Google Scholar]
- Treatment effects of the Forsus Fatigue Resistant Device used with miniscrew anchorage. Angle Orthod. 2014;84:76-87.
- [CrossRef] [PubMed] [Google Scholar]
- Treatment of a skeletal class II malocclusion using fixed functional appliance with miniplate anchorage. Eur J Dent. 2014;8:276-80.
- [CrossRef] [PubMed] [Google Scholar]
- Temporomandibular joint growth adaptation in Herbst treatment: A prospective magnetic resonance imaging and cephalometric roentgenographic study. Eur J Orthod. 1998;20:375-88.
- [CrossRef] [PubMed] [Google Scholar]
- Evaluation of the effects of functional orthopaedic treatment on temporomandibular joints with single-photon emission computerized tomography. Eur J Orthod. 2003;25:9-12.
- [Google Scholar]
- Stress distribution in the temporomandibular joint after mandibular protraction: A 3-dimensional finite element method study. Part 1. Am J Orthod Dentofacial Orthop. 2009;135:737-48.
- [Google Scholar]
- Stress distribution in the temporomandibular joint after mandibular protraction: A 3-dimensional finite element study. Part 2. Am J Orthod Dentofacial Orthop. 2009;135:749-56.
- [Google Scholar]
- Evaluation of stress changes in the mandible with a fixed functional appliance: A finite element study. Am J Orthod Dentofacial Orthop. 2015;147:226-34.
- [Google Scholar]
- Biomechanical effects of fixed functional appliance on craniofacial structures. Angle Orthod. 2009;79:668-75.
- [CrossRef] [PubMed] [Google Scholar]
- Treatment effects produced by the Twin-block appliance vs. the Forsus Fatigue Resistant Device in growing class II patients. Angle Orthod. 2015;85:784-9.
- [CrossRef] [PubMed] [Google Scholar]
- Evaluation of the effects of skeletal anchoraged Forsus FRD using miniplates inserted on mandibular symphysis: A new approach for the treatment of class II malocclusion. Angle Orthod. 2015;85:413-9.
- [Google Scholar]
- Effects of miniplate anchored and conventional Forsus Fatigue Resistant Devices in the treatment of class II malocclusion. Angle Orthod. 2016;86:1026-32.
- [Google Scholar]
- Static vs. dynamic loads as an influence on bone remodelling. J Biomech. 1984;17:897-905.
- [CrossRef] [Google Scholar]
- Biomechanical and clinical changes of the craniofacial complex from orthopedic maxillary protraction. Angle Orthod. 1991;61:145-52.
- [CrossRef] [Google Scholar]
- Effects of class II activator and class II activator high-pull headgear combination on the mandible: A 3-dimensional finite element stress analysis study. Am J Orthod Dentofacial Orthop. 2008;133:490.e9-15.
- [CrossRef] [PubMed] [Google Scholar]




