

Translate this page into:
Changes in vermilion lip morphology following orthodontic treatment with premolar extraction for Angle Class II maxillary protrusion
*Corresponding author: Jun Nihara, Division of Orthodontics, Faculty of Dentistry and Graduate School of Medical and Dental Sciences, Niigata University, 2-5274 Gakkocho-dori, Chuo-ku, Niigata, 951-8514, Japan. nihara@dent.niigata-u.ac.jp
-
Received: ,
Accepted: ,
How to cite this article: Oomori Y, Nihara J, Takahashi K, Saito I. Changes in vermilion lip morphology following orthodontic treatment with premolar extraction for Angle Class II maxillary protrusion. APOS Trends Orthod 2020;10(2):89-95.
Abstract
Objectives:
The objective of the study was to clarify the changes in vermilion lip morphology following orthodontic treatment in Japanese patients with Class II maxillary protrusion.
Materials and Methods:
The subjects were 15 adult women diagnosed as having Angle Class II maxillary protrusion who had undergone orthodontic treatment with premolar extraction. For analysis, profile photographs taken at the first examination and at completion of active treatment were used for linear and angular measurements. For linear measurements on the lateral facial photographs, an X–Y coordinate system was established using a lateral cephalogram superimposed along the line of the profile. Measurement points relating to the vermilion lip morphology were measured on the facial photographs by digital processing, with the Frankfort horizontal (FH) plane as the X-axis, and the line perpendicular to the X-axis passing through the alar curvature point (Ac) as the Y-axis.
Results:
The results of linear measurements showed significant retraction of approximately 3.0 mm in the upper vermilion lip, and mean retraction of the upper incisors after treatment was approximately 6.0 mm. However, whereas mean retraction of the lower incisors was approximately 1.0 mm, there was significant retraction of the lower vermilion lip of over 3.0 mm. Significant reduction in vermilion height was also found in the upper vermilion lip. With regard to angular measurements, the upper lip and total vermilion showed significant reductions that indicated inversion.
Conclusion:
Adequate retraction of the upper incisors in the maxillary protrusion with excessive overjet may retract not only the upper vermilion lip but also the lower one, suggesting that morphological changes in the lower lip are affected by the positioning of the upper incisors. In addition, the patterns of morphological changes differed between the upper and lower vermilion lips, with a large proportion of rotational change toward the mucous membrane in the upper vermilion lip and with a pattern of change resembling horizontal displacement in the lower vermilion lip. Total vermilion showed a significant reduction in vermilion height due to the reduction in height of the upper vermilion lip.
Keywords
Facial photograph
Lateral cephalogram
Lip morphology
Vermilion lip

INTRODUCTION
Orthodontic tooth movement can bring about considerable changes in the morphology of the perioral soft tissues surrounding the dentition and occlusion. Proffit et al. mentioned a paradigm shift in current orthodontics, referring to the concept of the soft-tissue paradigm and noted that the importance of soft tissues has been recognized not just from the point of view of esthetics but also as a treatment goal.[1] Peck and Peck have indicated that since the lips and teeth are fundamental elements of the facial profile, orthodontists should give consideration to the esthetics of the mouth through trade-offs between dentition and soft tissues.[2] Thus, it is very important for orthodontists to predict post-treatment changes in the soft-tissue profile when deciding the treatment strategy in clinical practice.
However, Spyropoulos has stated that facial esthetics may be affected by elements other than the profile.[3] Lip morphology has been considered one of the most important elements for facial esthetics so that there have been numerous reports on the factors affecting attractive or desirable lip morphology that have focused on areas other than the profile.[4-10] Especially in orthodontic fields, the anteroposterior position of the upper and lower incisors affects lip morphology, and some studies on incisor retraction and changes in lip morphology have been published.[11,12] Ioi et al. studied the effects of the difference in vermilion lip height on lip esthetics with subjective items,[13] and they concluded that vermilion lip morphology may have a large effect on facial harmony. Changes in vermilion lip morphology with aging[4] and the effects of premolar extraction on changes in vermilion lip morphology[14] have been previously reported. These studies, however, investigated changes in vermilion lip morphology from the frontal view. We previously investigated the details of changes in vermilion lip morphology in bimaxillary protrusion cases from the lateral view using lateral cephalograms and facial photographs.[15] That study clarified the difference in the patterns of changes between upper and lower vermilion lips following bimaxillary anterior teeth retraction.
On the other hand, in the treatment of Angle Class II maxillary protrusion cases, sufficient retraction of the upper anterior teeth is typically required to obtain appropriate overjet, resulting in improvement of lip incompetence and perioral soft-tissue tension. In other words, the amount of retraction of upper anterior teeth is much larger than that of lower anterior teeth. With the conclusion of our previous study, we hypothesized that the different amounts of retraction between the upper and lower anterior teeth could cause different patterns of vermilion lip morphology.
Thus, this study aimed to clarify the morphological changes of the vermilion lips following orthodontic treatment in cases of Angle Class II maxillary protrusion.
MATERIALS AND METHODS
Subjects
The subjects of the study were 15 Japanese women aged in their 20s and 30s who were diagnosed with Angle Class II maxillary protrusion with overjet ≥5 mm and who all underwent orthodontic treatment at Niigata University Medical and Dental Hospital. The patients’ mean age at the first examination was 27 years 4 months (range, 23–37 years), and their mean age at the end of dynamic treatment was 30 years.
The exclusion criteria were as follows: (1) Physical trauma, maxillofacial syndrome, or congenital abnormality; (2) marked asymmetry of the frontal view of the face; and (3) open bite or deep overbite (front teeth vertical overlap of 0–3.0 mm was included).
Treatment was carried out using a standard edgewise device in all cases. Upper and lower premolar extraction was carried out in 12 cases, and upper premolar extraction only was carried out in the remaining 3 cases. Two-stage retraction of the front teeth was carried out, with distal movement of the canines, followed by retraction of the incisors. The spaces were closed using rectangular wire with tear drop-type vertical loops. In all cases, Kloehn headgear was used on the maxillary molars for the purpose of reinforced anchorage. Following completion of dynamic treatment, a removable retainer was fitted to the maxilla, and a fixed retainer was fitted to the mandible in all cases.
This study was carried out with the approval of the Institutional Review Board of Niigata University (No. 26-R36-08-22). Written, informed consent was obtained from all participants before the start of the study, according to the principles the Declaration of Helsinki.
Methods
Photography conditions and photograph importing
Profile photographs taken at the first examination and at completion of dynamic treatment were used for the measurement of lip morphology. Profile photographs were taken using a film camera (FM3A, Nikon, Japan), with the subject seated and the head held with the Frankfort horizontal (FH) plane parallel to the floor by an ear rod. Photographs were taken under the same conditions before and after orthodontic treatment, with the lips closed at the intercuspal position. For digital measurements, all photographs were imported to a computer by a scanner (ES-10000G, Epson, Nagano, Japan) at a resolution of 1200 dpi.
Superimposition of photographs and cephalograms and coordinate system construction lateral cephalograms and profile photographs were superimposed by the same method that we previously reported.[15] The facial photographs taken before and after active orthodontic treatment were adjusted to the lateral cephalograms taken at the same time point following the soft-tissue profile line referencing the chin region, nasal tip, and glabella using image retouching software (Photoshop CS5, Adobe Inc., San Jose, CA, USA). The FH line on the lateral cephalograms at the start of active orthodontic treatment was transferred to facial photographs.
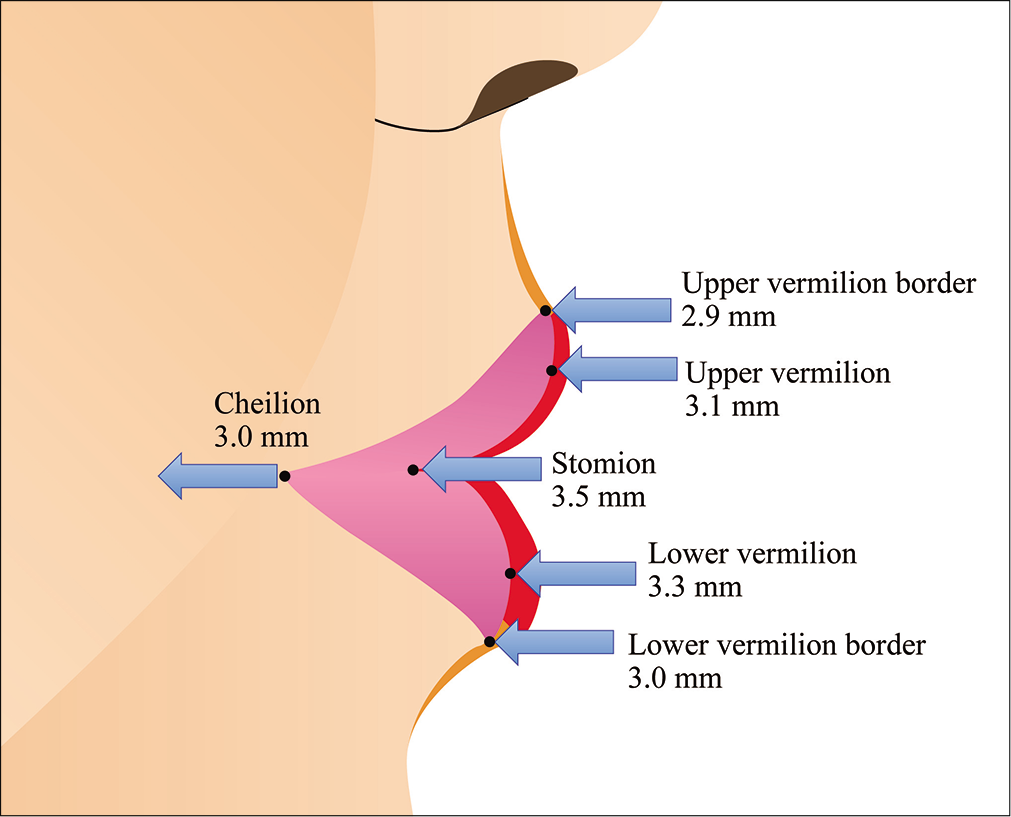
X–Y coordinates were constructed using the FH line for the X-axis and a perpendicular line drawn intersecting the X-line at the alar curvature point (Ac) for the Y-axis [Figure 1].

- The coordinate system on lateral facial photographs and measurements. ① Upper vermilion border depth (mm), ② Upper vermilion depth (mm), ③ Lower vermilion border depth (mm), ④ Lower vermilion depth (mm), ⑤ Stomion depth (mm), ⑥ Cheilion depth (mm), ⑦ U-total vermilion depth (⑥+②) (mm), ⑧ L-total vermilion depth (⑥+④) (mm), ⑨ Upper vermilion angle (degrees), ⑩ Lower vermilion angle (degrees), ⑪ Inter-vermilion angle (degrees), ⑫ Upper vermilion height (mm), ⑬ Lower vermilion height (mm), ⑭ Total vermilion height (mm).
Measurement of vermilion lip areas
Six sites were set as landmarks relating to the vermilion lips on the profile photographs on which the coordinate system was established [Figure 1]. Eleven linear measurements and three angular measurements were made using image processing software (Image J Ver. 1.48, US National Institutes of Health, Bethesda, MD, USA). All measurements were made by the same person (Y.O.). Data calibration was carried out by calculating on the basis of prior studies showing 10 cm to be equivalent to 452 dots on the image processing screen so that 1 dot = 0.22 mm.
Reliability
To calculate measurement error, 10 photographs were randomly selected, and, in each case, the lateral cephalogram and the profile photograph were again superimposed and measured after an interval of at least 2 weeks. Measurement error was calculated using Dahlberg’s formula, and measurement error ranges were 0.04–0.62 mm for linear measurements and 0.57°–1.04° for angular measurements. The reliability coefficient exceeded 98% for all measurement items [Table 1].
| Dahlberg’s formula | |
|---|---|
| ① Upper vermilion border depth (mm) | 0.07 |
| ② Upper vermilion depth (mm) | 0.04 |
| ③ Lower vermilion border depth (mm) | 0.13 |
| ④ Lower vermilion depth (mm) | 0.04 |
| ⑤ Stomion depth (mm) | 0.05 |
| ⑥ Cheilion depth (mm) | 0.38 |
| ⑦ U-total vermilion depth (mm) | 0.39 |
| ⑧ L-total vermilion depth (mm) | 0.41 |
| ⑨ Upper vermilion angle (degrees) | 0.62 |
| ⑩ Lower vermilion angle (degrees) | 0.57 |
| ⑪ Inter-vermilion angle (degrees) | 1.04 |
| ⑫ Upper vermilion height (mm) | 0.24 |
| ⑬ Lower vermilion height (mm) | 0.13 |
| ⑭ Total vermilion height (mm) | 0.23 |
Statistical significance
Changes following orthodontic treatment were analyzed statistically using the Wilcoxon signed-rank test. Analysis was carried out using JMP statistics software (ver. 5.0, SAS Institute Japan, Tokyo, Japan). The level of significance was set at 5%.
RESULTS
Subjects
The mean age of the subjects at the completion of dynamic treatment was 30 years, 4 months (23–37 years). The mean measurement values at the start of dynamic treatment were ANB 6.0º, U1-FH 121.7º, IMPA 97.3º, maxillary arch length discrepancy −3.2 ± 2.2 mm, and mandibular arch length discrepancy −3.2 ± 1.8 mm. The mean amounts of retraction of the incisors as a result of the treatment were 6.1 mm in the maxilla and 1.3 mm in the mandible.
Changes in vermilion lip morphology as a result of treatment
Changes following treatment for maxillary protrusion are shown in [Table 2]. The amounts of change were as follows: (1) Upper vermilion border depth −2.9 mm and (2) upper vermilion depth −3.1 mm. (3) Lower vermilion border depth decreased by 3.0 mm and (4) lower vermilion depth decreased by 3.3 mm, indicating significant retraction in both upper and lower lips. (5) Stomion decreased by 3.5 mm and (6) cheilion by 3.0 mm, both values showing significant retraction. There was no significant difference in (7) U-total vermilion depth or (8) L-total vermilion depth, which shows the anteroposterior depth of the upper and lower vermilion lips, respectively. (9) The upper vermilion angle decreased significantly by 5.0º, and the (10) lower vermilion angle decreased by 0.6º, but the difference was not significant. (11) The inter-vermilion angle decreased significantly by 5.6º. (12) Upper vermilion height decreased by 1.7 mm, (13) lower vermilion height increased by 0.2 mm, and (14) total vermilion height decreased by 1.5 mm. Of these, only the (13) lower vermilion height increase was not significant [Table 2].
| Pre-treatment | Post-treatment | Changes | |||||
|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | ||
| ① Upper vermilion border depth (mm) | 11.5 | 1.9 | 8.6 | 1.8 | −2.9 | 1.6 | *** |
| ② Upper vermilion depth (mm) | 12.0 | 1.9 | 8.9 | 1.8 | −3.1 | 1.5 | *** |
| ③ Lower vermilion border depth (mm) | 7.2 | 2.3 | 4.2 | 2.2 | −3.0 | 2.1 | *** |
| ④ Lower vermilion depth (mm) | 8.2 | 2.3 | 4.9 | 2.1 | −3.3 | 2.1 | *** |
| ⑤ Stomion depth (mm) | −3.5 | 1.7 | 1.5 | 1.8 | −3.5 | 1.7 | *** |
| ⑥ Cheilion depth (mm) | −4.1 | 1.7 | −7.0 | 1.5 | −3.0 | 1.9 | *** |
| ⑦ U-total vermilion depth (mm) | 16.1 | 2.0 | 14.9 | 2.3 | −0.2 | 1.3 | N.S |
| ⑧ L-total vermilion depth (mm) | 12.2 | 1.9 | 12.0 | 2.1 | −0.3 | 1.4 | N.S |
| ⑨ Upper vermilion angle (degrees) | 54.1 | 7.4 | 49.0 | 7.2 | −5.0 | 6.6 | ** |
| ⑩ Lower vermilion angle (degrees) | 74.2 | 11.2 | 73.7 | 7.4 | −0.6 | 10.0 | N.S |
| ⑪ Inter-vermilion angle (degrees) | 128.3 | 15.8 | 148.0 | 13.6 | −5.6 | 14.0 | * |
| ⑫ Upper vermilion height (mm) | 10.3 | 2.3 | 8.7 | 1.9 | −1.7 | 1.1 | *** |
| ⑬ Lower vermilion height (mm) | 8.0 | 1.9 | 8.2 | 1.2 | 0.2 | 1.2 | N.S |
| ⑭ Total vermilion height (mm) | 18.3 | 2.6 | 16.8 | 1.8 | −1.5 | 1.4 | ** |
DISCUSSION
Subjects
There have been several previous reports of soft-tissue changes in the maxillofacial region due to anatomical morphology or orthodontic treatment. Differences in the morphological characteristics of the vermilion lips due to age and sex have been reported,[16] and the present study, therefore, minimized the effects of age and sex by only having subjects who were women in their 20s or 30s.
In the present study, pre-treatment overjet ≥5 mm was defined as maxillary protrusion. This is the same standard used in prior studies by Islam and Bravo that evaluated soft-tissue profiles.[17,18] Furthermore, to exclude the effect on vermilion lip morphology of the vertical position of the incisors or overbite correction, overbite in the range of 2.0–4.0 mm was selected. The present subjects showed average retraction of 6.2 mm in the maxillary incisors and 1.3 mm in the mandibular incisors as a result of orthodontic treatment. The amount of retraction in the maxillary incisors in particular was clearly greater than in the previous studies,[19] indicating appropriate selection of maxillary protrusion cases for treatment to be carried out with adequate retraction of maxillary incisors.
Measurement method
Color photographs were needed for the analysis of changes in vermilion lip morphology because the vermilion lip region cannot be distinguished on cephalograms. Therefore, a previously reported method of evaluation by means of a coordinate system based on the FH plane using superimposed lateral cephalograms and profile photographs was used to allow easy comparison with the results of our previous study.[15]
The coordinate system in the present study used the Ac. According to reports by Kim et al. and Lim et al.,[20,21] the Ac point is minimally affected by three-dimensional changes in perioral soft tissue during treatment. The Ac point is highly reproducible when plotting graphically and may thus be considered a suitable reference point for the coordinate system.
Several studies have reported evaluations of changes in perioral soft tissues when the lips are relaxed.[21-24] Hillesund et al. stated that the “relaxed” position is preferable to the “closed” position for evaluation since labial tension may offset post-procedural changes.[22] However, all previous studies focusing on vermilion lip morphology and its esthetics carried out evaluations with the lips closed.[9,25-27] This is thought to be because of the possibility that the interlabial gap when the lips are relaxed may affect vertical measurements of lip morphology. The present study similarly aimed to clarify changes in vermilion lip morphology as a factor affecting esthetics, and since vertical height of the vermilion was evaluated, it was impossible to ignore the interlabial gap when the lips are relaxed. Consequently, profile photographs with the lips closed taken before and after treatment were used to evaluate vermilion lip morphology.
Changes in vermilion lip morphology after orthodontic treatment
Evaluations of vermilion lip morphology before and after treatment showed clear retraction of the upper and lower lips as a result of retraction of the anterior teeth by orthodontic treatment [Table 2 and Figure 2]. The results may be compared to the results of a study by Roos that used lateral cephalograms to investigate changes in the soft-tissue profile following orthodontic treatment in maxillary protrusion cases.[28] Roos found that the ratio of upper incisor retraction to posterior movement of the upper vermilion lip was 2.5:1, which was a similar trend to the results obtained in the present study. Furthermore, in the lower lip region,[28] Roos found that the ratio of lower incisor retraction to posterior movement of the lower vermilion lip was 1.3:1. However, that of the present study was 1:2.3, the amount of posterior movement of the lower vermilion lip was greater than the retraction of the lower incisors. This may be due to the difference between the two study conditions, with the lips relaxed in the study by Roos studied and with the lips closed in the present study.
- Changes in the upper and lower vermilion lips before and after orthodontic treatment (anteroposterior changes).
Furthermore, the present results showed posterior movement of not only the foremost part of the vermilion lip but also the cheilion, which is the part of the vermilion lip furthest to the posterior, indicating posterior movement of the whole vermilion lip. The amount of posterior movement of the cheilion was less than that reported by Eidson et al.[24] They evaluated lip morphology using a non-contact 3-D laser scanner, but they found relatively low measurement accuracy in the undercut and areas of shadow, particularly in the region of the cheilion, and this is probably a factor that gave rise to results different from those of the present study.
In the angular measurements of the vermilion lips, a tendency toward inversion accompanying the posterior movement of the vermilion lip was found only in the upper vermilion lip, and no significant changes were found in the lower vermilion lip [Table 2 and Figure 3]. It may be conjectured that this is the effect of different patterns of changes between the upper and lower lips.
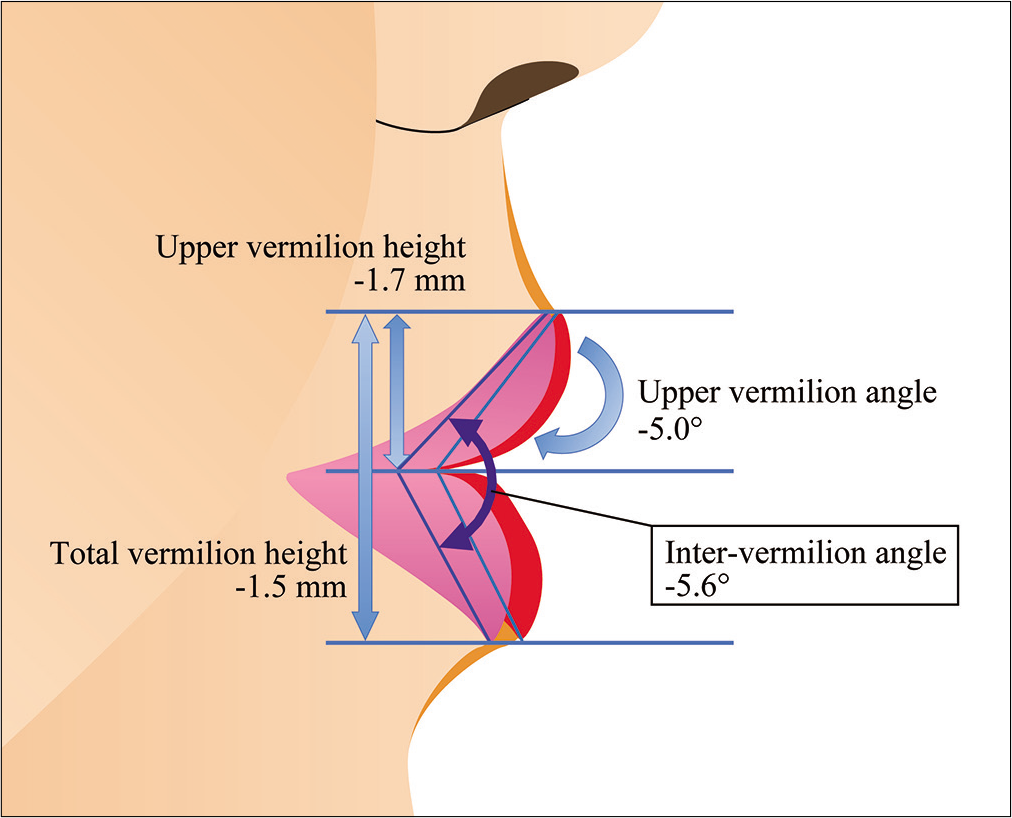
- Changes in the upper and lower vermilion lips before and after orthodontic treatment (vertical changes, rotation changes).
The results of linear and angular measurements showed that the upper vermilion lip tended to rotate toward the internal side while retracting, at the same time maintaining its anteroposterior dimensions. The lower vermilion lip retracted with hardly any rotation at all, or, in other words, it tended to retract with only a very slight decrease in anteroposterior depth. This fact can be explained by the difference in the patterns of changes between upper and lower vermilion lips from an anatomical perspective, as we reported previously; the orbicularis oris muscle runs through the layer under both the upper and lower vermilion lips, but the anatomical attachment site differs.[29] Rotational change of the upper vermilion lip, which at the center is attached in its upper region to the nasal septum (nasolabialis) was observed, while the lower vermilion lip, which has no vertical muscle bundle in the central region, showed a pattern of movement similar to parallel displacement. The vertical dimensions showed significant decreases in upper vermilion height and total vermilion height, while there was no significant change in lower vermilion height. These differences in height changes between the upper and lower vermilion lips are likely due to the effects of the anatomical differences discussed above. In addition, these patterns of changes should be taken into consideration, particularly when predicting changes in labial morphology with treatment for maxillary protrusion.
This study examined the details of vermilion lip morphological changes in relation to esthetic harmony in Angle Class II maxillary protrusion patients. Lip incompetence improved, and appropriate profiles were obtained by orthodontic treatment combined with premolar extraction. Retraction of the vermilion lips as a result of upper and lower incisor retraction was found, and reduction in vermilion height was found mainly in the upper vermilion lip. Compared with the results of vermilion lip morphology in patients with Angle Class I bimaxillary protrusion, the patterns of change were similar to those of Angle Class II maxillary protrusion. However, the amounts of changes were different from each other; in particular, the amount of lower vermilion lip retraction was more than that of the lower incisors. This indicated that the changes of vermilion lip morphology depend on the type of malocclusion. Orthodontists should pay attention to these kinds of factors to achieve suitable facial esthetics with appropriate occlusion. The vermilion lip morphological changes after orthodontic treatment have yet to be studied in cases of malocclusion showing mandibular protrusion, open bite, or deep bite, and further research is needed to be able to predict morphological changes following treatment in such cases.
CONCLUSION
This study clarified the morphological changes in the vermilion lips of Japanese patients with Angle Class II maxillary protrusion following orthodontic treatment. The incisors were retracted by the orthodontic intervention, and as a result, the upper vermilion lip moved back while rotating inside, whereas the lower vermilion moved in parallel. In particular, the amount of retraction was 2 times greater than that of the lower incisors on the lower vermilion lip region on lip closure. The results suggest that, in Angle Class II maxillary protrusion, changes in the anteroposterior position of the upper incisors due to orthodontic treatment affect not only the upper vermilion lip but also the lower vermilion lip. Furthermore, in the diagnosis of Angle Class II maxillary protrusion, the positional relationships of the upper incisors and the upper and lower lips need to be taken into account to predict the changes in the facial profile as a result of treatment.
ACKNOWLEDGMENTS
The authors would like to express their gratitude to Dr. Shuichi Morita for kind and valuable assistance in planning, pursuing, and reviewing this study.
Authors’ contributions
Concepts: Yuko Oomori and Jun Nihara
Design: Jun Nihara
Definition of intellectual content: Jun Nihara, Kojiro Takahashi, and Isao Saito
Literature search: Yuko Oomori
Clinical studies: Yuko Oomori
Experimental studies: Yuko Oomori
Data acquisition: Yuko Oomori
Data analysis: Yuko Oomori and Jun Nihara
Statistical analysis: Jun Nihara
Manuscript preparation: Yuko Oomori, Jun Nihara, Kojiro Takahashi, and Isao Saito
Manuscript editing and review: Yuko Oomori, Jun Nihara, Kojiro Takahashi, and Isao Saito
Guarantor: Yuko Oomori
Declaration of patient consent
Institutional Review Board (IRB) permission obtained for the study.
Financial support and sponsorship
This work was supported by JSPS KAKENHI Grant Number JP17k17319.
Conflicts of interest
There are no conflicts of interest.
References
- Selected aspects of the art and science of facial esthetics. Semin Orthod. 1995;1:105-26.
- [CrossRef] [Google Scholar]
- Significance of the soft tissue profile on facial esthetics. Am J Orthod Dentofacial Orthop. 2001;119:464-71.
- [CrossRef] [PubMed] [Google Scholar]
- Why some women look young for their age. PLoS One. 2009;4:e8021.
- [CrossRef] [PubMed] [Google Scholar]
- The esthetic properties of lips: A comparison of models and nonmodels. Angle Orthod. 2004;74:162-6.
- [Google Scholar]
- Soft-tissue facial characteristics of attractive and normal adolescent boys and girls. Angle Orthod. 2008;78:799-807.
- [CrossRef] [PubMed] [Google Scholar]
- Anteroposterior lip positions of the most-favored Japanese facial profiles. Am J Orthod Dentofacial Orthop. 2005;128:206-11.
- [CrossRef] [PubMed] [Google Scholar]
- Esthetic evaluation of Asian-Chinese profiles from a white perspective. Am J Orthod Dentofacial Orthop. 2008;133:532-8.
- [CrossRef] [PubMed] [Google Scholar]
- Evaluation of the facial dimensions of young adult women with a preferred facial appearance. Korean J Orthod. 2015;45:253-60.
- [CrossRef] [PubMed] [Google Scholar]
- Predicting soft tissue profile changes concurrent with orthodontic treatment. Angle Orthod. 1990;60:199-206.
- [Google Scholar]
- Soft tissue changes associated with first premolar extractions in adult females. Aust Orthod J. 2009;25:24-9.
- [Google Scholar]
- Effects of vermillion height on lip esthetics in Japanese and Korean orthodontists and orthodontic patients. Angle Orthod. 2014;84:239-45.
- [CrossRef] [PubMed] [Google Scholar]
- Effects of extraction of four premolars on vermilion height and lip area in patients with bimaxillary protrusion. Eur J Orthod. 2013;35:521-8.
- [CrossRef] [PubMed] [Google Scholar]
- Changes in vermilion lip morphology after premolars extraction treatment in Japanese patients with bimaxillary protrusion. Orthod Waves Jpn Ed. 2016;75:97-105.
- [Google Scholar]
- Changes in frontal soft tissue dimensions of the lower face by age and gender. World J Orthod. 2002;3:313-20.
- [Google Scholar]
- Lip morphological changes in orthodontic treatment. Angle Orthod. 2009;79:256-64.
- [CrossRef] [PubMed] [Google Scholar]
- Comparison of the changes in facial profile after orthodontic treatment, with and without extractions. Br J Orthod. 1997;24:25-34.
- [CrossRef] [PubMed] [Google Scholar]
- Soft tissue changes after upper premolar extraction in Class II camouflage therapy. Angle Orthod. 2006;76:59-65.
- [Google Scholar]
- Three-dimensional assessment of upper lip positional changes according to simulated maxillary anterior tooth movements by white light scanning. Korean J Orthod. 2014;44:281-93.
- [CrossRef] [PubMed] [Google Scholar]
- Three-dimensional evaluation of soft tissue change gradients after mandibular setback surgery in skeletal Class III malocclusion. Angle Orthod. 2010;80:896-903.
- [CrossRef] [PubMed] [Google Scholar]
- Reliability of soft-tissue profile in cephalometrics. Am J Orthod. 1978;74:537-50.
- [CrossRef] [Google Scholar]
- Three-dimensional soft-tissue and hard-tissue changes in the treatment of bimaxillary protrusion. Am J Orthod Dentofacial Orthop. 2013;144:218-28.
- [CrossRef] [PubMed] [Google Scholar]
- Three-dimensional evaluation of changes in lip position from before to after orthodontic appliance removal. Am J Orthod Dentofacial Orthop. 2012;142:410-8.
- [CrossRef] [PubMed] [Google Scholar]
- The attractive lip: A photomorphometric analysis. J Plast Reconstr Aesthet Surg. 2015;68:902-29.
- [CrossRef] [PubMed] [Google Scholar]
- Aesthetic perception of the height of the lip vermilion border by black and white laypeople. J Res Dent Tubarao. 2014;2:5.
- [CrossRef] [Google Scholar]
- The role of orthodontics as an auxiliary tool to lip augmentation. An Bras Dermatol. 2011;86:773-7.
- [CrossRef] [PubMed] [Google Scholar]
- Soft-tissue profile changes in Class II treatment. Am J Orthod. 1977;72:165-75.
- [CrossRef] [Google Scholar]
- Anatomy of the Human Body. (20th ed). Philadelphia, PA: Lea & Febiger; 1918. p. :383-5.
- [CrossRef] [Google Scholar]




