

Translate this page into:
Comparing posterior airway space changes in Class III patients treated with face mask and reverse chin cup
 , Mahsa Khademi4, Korosh Majidi5, Vincenzo Grassia6, Ludovica Nucci6, Michele Simeone7
, Mahsa Khademi4, Korosh Majidi5, Vincenzo Grassia6, Ludovica Nucci6, Michele Simeone7

*Corresponding author: Abdolreza Jamilian, Full Professor and Consultant of Orthodontics, No 14, Pesiyan St., Vali Asr St. Tehran, Iran. info@jamilian.net
-
Received: ,
Accepted: ,
How to cite this article: Farhadi M, Jamilian A, Khademi M, Majidi K, Grassia V, Nucci L. Comparing posterior airway space changes in Class III patients treated with face mask and reverse chin cup. APOS Trends Orthod. 2025;15:19-25. doi: 10.25259/APOS_107_2024
Abstract
Objectives:
The aim was to compare the posterior airway changes in patients treated with a face mask and reverse chin cup and to assess the stability over a 1.5-year follow-up period.
Material and Methods:
This historical cohort study consisted of two groups containing 20 patients with skeletal Class III malocclusion. The average age of the patients in groups one (Facemask) and two (reverse chin cup) was 7.77 ± 1.30 years and 8.6 ± 1.36 years, respectively. Seventeen cephalometric variables were measured before, after treatment, and after a 1.5-year follow-up. Comparisons were made within each group and between the two groups. Repeated measures, analysis of variance, or Friedman test were used.
Results:
There was no significant difference between the two groups in the posterior airway space. For patients who used face masks, six variables (AD1-posterior nasal spine [PNS], AD2-PNS, anterior nasal spine [ANS]-PNS, ANS-PNS-PPW, AA-PNS, and PNS-P) considerably increased (P < 0.05). In the reverse chin cup group, three variables (AD2-PNS, ANS-PNS-PPW, and PNS-P) considerably changed (P < 0.05). Moreover, no significant changes (P > 0.05) were observed in any variables after the 1.5-year follow-up period.
Conclusion:
In this study, the reverse chin cup and face mask effectively corrected Class III malocclusion and significantly increased the posterior airway space. The face mask showed greater enhancement compared to the reverse chin cup, and these improvements were maintained after a 1.5-year follow-up. However, the two groups had no significant difference regarding the posterior airway space changes.
Keywords
Cephalometry
Malocclusion
Orthodontics
Posterior airway

INTRODUCTION
Skeletal Class III malocclusion occurs due to mandibular prognathism, maxillary deficiency, or a combination of both,[1] and it is usually associated with dentoalveolar problems, including anterior edge-to-edge relation or anterior and posterior cross-bite, which can exist simultaneously.[2] It has been said that this malocclusion can also be associated with morphological characteristics of the oropharyngeal airway. The reported data show that Class III adults might have larger total oropharyngeal volume. Still, constriction areas in the retropalatal and retroglossal compartments of the oropharynx are more significant than in other people.[3] In most cases, the base of the tongue is the most constricted area.[4] Furthermore, Class III people are more likely to be mouth breathers than Class I individuals.[5] In correcting this malocclusion, more attention is paid to increasing the growth of the maxilla.[6] Because almost half of the Class III malocclusions are caused by maxillary deficiency.[1] Various methods have been introduced to correct this condition, such as the reverse chin cup, growth modification with orthopedic appliances,[7] and face masks or appliances that focus on maxillary protraction.[8] Treating this malocclusion is particularly challenging for orthodontists[9] and the difficulty increases as the patient ages.[10] Moreover, growth modification approaches are no longer suitable after growth cessation, and surgery is recommended.[6] One of the critical factors in determining a good prognosis in this malocclusion is maxillary deficiency.[11] Although there is abundant evidence from treating these patients using different devices, including reverse chin cups and face masks, due to the conflicting results reported by researchers, many differences of opinion have arisen among orthodontists.[12] It is stated that orthopedic treatment with maxillary protraction for Class III malocclusion can increase the posterior airway space, which seems to be retained after treatment. However, we have little trust in these data because the existing studies are of poor quality and have a small sample size, leading to low confidence.[13] Thus, this study aimed to compare the posterior airway changes in patients treated with a face mask and reverse chin cup and to assess the stability of their results over a 1.5-year follow-up period. The null hypothesis was that there was no significant difference between posterior airway variables before and after treatment across the groups.
MATERIAL AND METHODS
The study was carried out under the provisions established by the Declaration of Helsinki. Ethical approval was obtained from the IAU Local Research Ethics Committee (1395.032). Informed consent was obtained from all patients and their parents before treatment.
This historical cohort study consisted of two groups containing 20 patients with skeletal Class III malocclusion. Group one was assigned to face mask (eight males, 12 females), and Group two was related to reverse chin cup (11 males, nine females). The sample size was calculated using G*Power (Faul, Erdfelder, Buchner, and Lang, 2020, version 3.1.9) with an effect size of 0.48, an alpha (α) error probability of 0.05, a number of measurements of 3, and a power (1-β error probability) of 0.95.
The patients were all collected from an orthodontic clinic and were treated by the same specialist. Names and types of treatment were removed from each patient’s document before the measurements to minimize bias. Therefore, researchers who traced and measured the variables and the ones who collected the data were unaware of each patient’s treatment protocol. The mean age of the face mask group was 7.77 ± 1.30 years, and the average age of the reverse chin cup group was 8.6 ± 1.36 years. All subjects gave informed written consent. The eligibility criteria for participants were as follows:
Initial negative overjet
Initial anterior cross-bite
Initial Class III molar relationship
Treated with a facemask or reverse chin cup.
The exclusion criteria were as follows:
Mandibular shift and congenital disease or endocrine disorders, previous orthodontic treatment or surgical intervention, previous history of trauma, syndromes, history of tonsillectomy/adenoidectomy, history of treatment with continuous positive airway pressure, history of medication intake, history of upper airway obstruction, history of frequent colds (more than 6 times in the past 1 year), and having a cold or upper airway inflammatory disease at the time of taking the lateral cephalograms.
None of the patients or their parents wanted to choose orthognathic surgery treatment. Lateral cephalograms, orthopantograms, and photos were taken before, after treatment, and after a 1.5-year follow-up. The following cephalometric variables were measured:
SNA: The angle at the intersection of the SN line and NA line
SNB: The angle at the junction of the SN line and NB line 3. ANB: The angle at the intersection of the NA line and NB line
Wits appraisal: The distance between the AO line and the BO line
Facial angle: The angle at the intersection of the Frankfurt plane and the N-Pog line
Y-axis: The angle at the intersection of the SN line and the N-Gn line
Gogn-sn: The angle at the intersection of Go-Gn and SN line
Inclination angle: The angle at the intersection of the N’ line perpendicular to the palatal plane
AD1-posterior nasal spine (PNS): The distance of ad 1 to the PNS. AD1 is the intersection point of the posterior pharyngeal wall and the line from PNS to the basion
AD2-PNS: The distance of AD2 to PNS; AD2 is the intersection point of the posterior pharyngeal
Wall and the line from the midpoint of the line from Sella (S) to Ba to PNS
Anterior nasal spine (ANS) PNS-PPW: Nasopharyngeal space, PNS to the posterior pharyngeal wall along the palatal plane line
AA-PNS: The distance of the most anterior point of the atlas vertebra (AA) to PNS
P-pp: The distance between the tip of the soft palate (p) and the horizontal counterpoint on the posterior pharyngeal wall
Ph-pph: the distance of horizontal counterpoints on the anterior and posterior pharyngeal wall in the oropharynx at its narrowest area[14]
ANS-PNS-P (°): The angle, ANS to PNS to tip of the soft palate (p)
PNS-P: The distance of PNS to point p
Sp1–Sp2: The thickest cross-section of the soft palate.
Distances are expressed in millimeters, while angles are specified in degrees.
The characteristics of groups are outlined as follows:
Group 1: Patients in this group received a multi-adjustable face mask (Ortho Technology Inc., Tampa, FL, USA), and in the upper jaw, a full anchorage removable appliance was given to them. The upper removable appliance contained two Adams clasps on the permanent first molars, two C clasps on the primary canines, and two C clasps on the permanent central incisors. For the increase of anchorage reinforcement, if needed, the number of C and Adams clasps could be added.to deliver approximately 500 g of force, two orthodontic latex elastics (5/160, medium size) connected the upper removable appliance’s hooks to the face mask’s horizontal crossbar. The patients were informed to wear the appliance full-time and were only allowed not to wear it while eating, engaging in contact sports, or brushing their teeth.
Group 2: Patients were given a reverse chin cup and a removable palatal appliance. The upper removable appliance included the following components: Two Adams clasps on the permanent first molar, two C-clasps on the permanent central incisors, two C-clasps on the permanent lateral incisors, and two C-clasps on the primary canines. A porous acrylic chin cup with two arms was bent to form a hook, and two hooks were embedded in the palatal canine area of the upper removable appliance. Hooks on the porous acrylic chin cup were connected to the hooks on the removable palatal appliance with heavy-size, 5/16” orthodontic latex elastics [Figure 1].
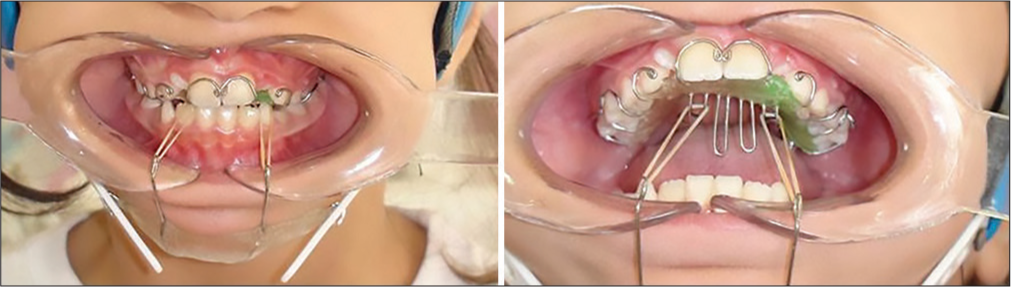
- The reverse chin cup used in this study.
Before, after the treatment, and after a 1.5-year follow-up, lateral cephalograms of all patients were traced. Tracing was done manually with a ruler and protractor. The measurement accuracy was checked by tracing each lateral cephalogram twice by the same researcher. Intraclass correlation coefficients (ICCs) calculated for each variable showed the measurements to be consistent at 95%, indicating no random error. Variables were compared within each group and between two groups.
All the statistical analyses were performed using the Statistical Package for the Social Sciences software version 25.0 (IBM, Chicago, Illinois, USA). Data are shown as mean (standard deviation). The normality of the data distribution was assessed using the Kolmogorov–Smirnov test. The repeated measures analysis of variance followed by a Tukey post hoc or Friedman test (for non-normal variables) was also utilized to compare the mean outcome quantities in each group. In this study, P < 0.05 was considered statistically significant. Twenty patients were randomly selected to evaluate the data for 4 weeks. There were no statistically significant differences in the test-retest reliability (ICC and limits of agreement statistics) for the 2-time intervals.
In the design and reporting of our study, we adhered to the STROBE checklist, confirming our compliance with its recommended protocol.
RESULTS
The average duration of treatments in group 1 was 29 ± 9 months, and in group 2, it was 25 ± 8 months. There was no significant difference in variables between the two groups before treatment. In the skeletal variables, there was a significantly increased in SNA in both groups. In the patients treated with face masks (group 1), the other three variables in this dimension had significant changes. SNB decreased, and ANB and Wits saw significant increases. In group 2, a significant increase has been seen in ANB and Wits (P < 0.05). The difference in the results after treatment in the ANB and Wits was significant between the two groups. While there was a slight increase in Y-Axis and Gogn-sn in the face mask groups, there was a slight decrease in Gogn-sn in the reverse chin cup group. In addition, the inclination angle slightly decreased in the face mask group but slightly increased in the reverse chin cup group. However, these changes were not significant [Table 1]. Regarding the changes in the patients’ posterior airway space, there was no significant difference between the two groups in this area. In the reverse chin cup group (group 2), ANS-PNS-PPW and PNS-P (P < 0.05) had a significant change. PP-P and PH-PPH were the only variables that decreased after treatment, although this change was insignificant. Contrary to the fact that other variables increased after treatment, their increases were insignificant in this group. However, results in the patients who used face masks show a considerable rise in six variables (P < 0.05), namely, AD1-PNS, AD2-PNS, ANS-PNS, ANS-PNS-PPW, and AA-PNS, PNS-P [Table 2]. Although small rises in the other variables were detected, they were insignificant. Furthermore, no significant differences were found between all variables after a 1.5-year follow-up (P > 0.05) [Table 3].
| Cephalometric parameters | Face mask | Reverse chin cup | Between two groups (post-treatment) | ||||
|---|---|---|---|---|---|---|---|
| Pre-treatment mean (SD) | Post-treatment mean (SD) | P-value | Pre-treatment mean (SD) | Post-treatment mean (SD) | P-value | P-value | |
| SNA | 79.75 (2.22) | 81.65 (2.16) | 0.001 | 78.65 (3.07) | 80.55 (2.04) | 0.009 | 0.106 |
| SNB | 81.00 (1.95) | 80.55 (1.88) | 0.03 | 81.80 (2.46) | 81.65 (2.25) | 0.857 | 0.102 |
| ANB | −1.25 (1.55) | 1.30 (1.59) | 0.001 | −3.10 (2.36) | −1.10 (2.13) | <0.001 | 0.001 |
| Wits | −4.05 (1.39) | −0.35 (1.24) | 0.001 | −5.70 (3.66) | −2.10 (2.0) | <0.001 | 0.003 |
| Facial angle | 87.85 (4.07) | 87.35 (3.17) | 0.520 | 88.75 (4.87) | 88.55 (3.59) | 0.841 | 0.269 |
| Y-axis | 57.55 (3.85) | 58.75 (3.80) | 0.088 | 58.60 (3.33) | 58.85 (2.98) | 0.666 | 0.927 |
| Gogn-sn | 33.00 (5.27) | 34.15 (5.69) | 0.012 | 33.05 (5.87) | 32.95 (5.45) | 0.883 | 0.500 |
| Inclination angle | 92.30 (7.29) | 90.75 (5.81) | 0.592 | 88.20 (6.44) | 91.00 (5.59) | 0.015 | 0.899 |
SD: Standard deviation, SNA: The angle at the intersection of the SN line and NA line, SNB: The angle at the junction of the SN line and NB line, ANB: The angle at the intersection of the NA line and NB line.
| Cephalometric parameters | Face mask | Reverse chin cup | Between two groups (post-treatment) | ||||
|---|---|---|---|---|---|---|---|
| Pre-treatment mean (SD) | Post-treatment mean (SD) | P-value | Pre-treatment mean (SD) | Post-treatment mean (SD) | P-value | P-value | |
| AD1-PNS | 13.35 (4.48) | 16.10 (4.91) | 0.001 | 15.85 (5.35) | 16.00 (5.14) | 0.8 | 0.9 |
| AD2-PNS | 11.25 (3.39) | 13.15 (4.13) | 0.003 | 12.85 (4.18) | 14.15 (4.04) | 0.05 | 0.4 |
| ANS-PNS | 43.40 (2.74) | 45.30 (3.25) | 0.001 | 48.20 (12.58) | 49.15 (12.18) | 0.08 | 0.1 |
| ANS-PNS-PPW | 21.20 (2.89) | 23.30 (2.83) | 0.001 | 21.80 (3.85) | 22.90 (3.78) | 0.02 | 0.7 |
| AA-PNS | 28.75 (2.92) | 30.50 (2.96) | 0.001 | 30.60 (8.27) | 31.40 (7.71) | 0.4 | 0.7 |
| PH-PPH | 10.80 (3.38) | 11.60 (3.23) | 0.3 | 12.60 (6.83) | 11.90 (4.61) | 0.8 | 0.8 |
| ANS-PNS-P | 125.15 (8.73) | 125.40 (9.26) | 0.8 | 122.45 (10.84) | 123.85 (7.46) | 0.3 | 0.5 |
| PNS-P | 27.00 (2.77) | 29.10 (2.99) | 0.009 | 30.90 (6.82) | 32.10 (7.06) | 0.0 | 0.1 |
| SP1-SP2 | 7.35 (1.14) | 8.35 (4.82) | 0.5 | 8.35 (2.23) | 8.35 (1.73) | 0.8 | 0.1 |
| p-pp | 10.10 (4.32) | 10.60 (2.68) | 0.4 | 11.25 (5.63) | 10.75 (3.57) | 0.4 | 0.6 |
SD: Standard deviation, PNS: Posterior nasal spine, ANS: Anterior nasal spine, AD1-PNS: the distance of ad1 to the posterior nasal spine (PNS). ad1 is the intersection point of the posterior pharyngeal wall and the line from PNS to the basion. AD2-PNS: the distance of ad2 to PNS; ad2 is the intersection point of the posterior pharyngeal wall and the line from the midpoint of the line from Sella (S) to Ba to PNS. ANSPNS-PPW: nasopharyngeal space, PNS to the posterior pharyngeal wall along the palatal plane line. AA-PNS: the distance of the most anterior point of the atlas vertebra (AA) to PNS. p-pp: the distance between the tip of the soft palate (p) and the horizontal counterpoint on the posterior pharyngeal wall. PH-PPH: the distance of horizontal counterpoints on the anterior and posterior pharyngeal wall in the oropharynx at its narrowest area.[14]ANS-PNS-p (°): the angle, anterior nasal spine (ANS) to PNS to tip of the soft palate (p). PNS-P: the distance of PNS to point p. SP1–SP2: the thickest cross-section of the soft palate.
| Cephalometric parameters | Face mask mean (SD) | P-value (comparison of face mask results between post-treatment and 1.5-year follow-up) | Reverse chin cup mean (SD) | P-value (comparison of Reverse Chin Cup results between post-treatment and 1.5-year follow-up) |
|---|---|---|---|---|
| SNA | 81.35 (2.05) | 0.66 | 80.30 (1.96) | 0.69 |
| SNB | 80.80 (1.90) | 0.68 | 82.05 (2.56) | 0.58 |
| ANB | 1.15 (1.69) | 0.77 | −1.20 (1.94) | 0.88 |
| Wits | −0.55 (1.11) | 0.59 | −2.25 (2.02) | 0.81 |
| Facial angle | 87.55 (3.36) | 0.85 | 89.10 (3.50) | 0.63 |
| Y-axis | 58.55 (3.80) | 0.87 | 58.55 (3.38) | 0.76 |
| Gogn-sn | 34.65 (5.75) | 0.78 | 33.40 (5.85) | 0.79 |
| Inclination angle | 91.35 (5.55) | 0.74 | 90.50 (6.67) | 0.80 |
| AD1-PNS | 15.85 (4.78) | 0.87 | 15.80 (5.13) | 0.90 |
| AD2-PNS | 12.95 (4.22) | 0.88 | 13.80 (4.14) | 0.78 |
| ANS-PNS | 45.10 (3.14) | 0.84 | 48.45 (14.14) | 0.86 |
| ANS-PNS-PPW | 22.85 (2.85) | 0.62 | 22.45 (4.29) | 0.71 |
| AA-PNS | 30.10 (2.94) | 0.67 | 30.75 (8.98) | 0.79 |
| PH-PPH | 11.25 (2.86) | 0.72 | 12.15 (5.12) | 0.87 |
| ANS-PNS-P | 124.90 (8.77) | 0.86 | 123.20 (7.82) | 0.77 |
| PNS-P | 28.60 (2.94) | 0.60 | 32.20 (7.33) | 0.68 |
| SP1-SP2 | 6.95 (0.82) | 0.21 | 8.45 (2.39) | 0.89 |
| p-pp | 10.25 (2.49) | 0.67 | 10.50 (4.09) | 0.82 |
SD: Standard deviation, PNS: Posterior nasal spine, ANS: Anterior nasal spine, AD1-PNS: the distance of ad1 to the posterior nasal spine (PNS). ad1 is the intersection point of the posterior pharyngeal wall and the line from PNS to the basion. AD2-PNS: the distance of ad2 to PNS; ad2 is the intersection point of the posterior pharyngeal wall and the line from the midpoint of the line from Sella (S) to Ba to PNS. ANSPNS-PPW: nasopharyngeal space, PNS to the posterior pharyngeal wall along the palatal plane line. AA-PNS: the distance of the most anterior point of the atlas vertebra (AA) to PNS. p-pp: the distance between the tip of the soft palate (p) and the horizontal counterpoint on the posterior pharyngeal wall. PH-PPH: the distance of horizontal counterpoints on the anterior and posterior pharyngeal wall in the oropharynx at its narrowest area. ANS-PNS-p (°): the angle, anterior nasal spine (ANS) to PNS to tip of the soft palate (p). PNS-P: the distance of PNS to point p. SP1–SP2: the thickest cross-section of the soft palate, SNA: The angle at the intersection of the SN line and NA line; SNB: The angle at the junction of the SN line and NB line; ANB: The angle at the intersection of the NA line and NB line.
DISCUSSION
The present study suggests that using a face mask or reverse chin cup appliance may result in the following outcomes: (i) Anterior displacement of the maxilla and (ii) anterior movement of the maxillary dentition along with lingual movement of the mandibular incisors. All posterior airway space variables were increased except P-PP and PH-PPH in the reverse chin cup group. At the same time, all variables in the face mask group have been increased. However, this change was significant in six variables, namely, AD1-PNS, ANS-PNS, AA-PNS, AD2-PNS, ANS-PNS-PPW, and PNS-P (The null hypothesis has been rejected). We can infer that the face mask raised the total posterior airway space more than the reverse chin cup, but it is essential to consider that the results did not show a significant difference between the two groups. After a 1.5-year follow-up, there was no significant difference between all variables, and the number of them remained approximately the same, indicating that these changes were maintained. In the study of Akin et al.[15] the face mask results were better than the reverse chin cup. However, in our study, unlike them, the reverse chin cup, despite not being as good as the face mask, had acceptable results, which may be due to the difference in the treatment protocol and the device. However, many other factors that cannot be controlled cannot be ignored. It is stated that bone-anchored maxillary protraction devices could improve airway dimensions. However, the change in airway dimension is not necessarily correlated with the physical function. This means that even significant increases in airway dimensions do not necessarily imply a clinical improvement in airway problems.[16,17] Considering that mandibular, maxillary, cranial base, hyoid, and head position characteristics are related to sleep apnea,[18] although it may not have a direct and proven cause, it is not ineffective either. Although there is a lot of evidence that they are effective,[19] Chen et al. reported that after protraction headgear and rapid maxillary expansion (PE) treatment of Class III malocclusion with maxillary skeletal hypoplasia leads to a significant increase in the volume of the nasopharynx and velopharynx. However, the volume of the glossopharynx and hypopharynx remains unchanged in the short term.[20] In our study, both velopharynx and glossopharynx spaces were changed, which could be why the treatment of all patients was completed. Moreover, Kale and Buyukcavus conducted a study. They concluded that the most effective protraction method in terms of pharyngeal airway dimensions, especially in the nasopharynx, is the application of the face mask with skeletal anchorage.[21] In our research, the face mask has been an effective device in this space due to the statistically significant difference in the two mentioned variables. Tuncer et al. reported that the chin cup increased the nasopharyngeal area compared to the control group in their study, and there was no significant difference between the samples with different vertical characteristics,[22] but Akin et al.[15] stated that the face mask increased those areas more than the chin cup in their research. However, there were no differences between the groups treated with face mask removable maxillary appliances and modified tandem traction bow appliances according to the mean pharyngeal airway shapes due to the Kaygisiz et al. study.[23] Available data and evidence suggest that treating Class III malocclusion increases the posterior airway space, which seems to be retained after treatment.[13] Our results and achievements in this research are consistent with the previous studies and confirm that treating patients with reverse chin cups and face masks leads to an increase in the mentioned area. It should also be considered that soft tissue can also be a risk factor for apnea[24] and it was not possible to measure the soft tissue of the air space in this research. In this study, a reverse chin cup (Chin support with cranial straps [Hickham]) and multi-adjustable face mask were used and, also, to provide a better air vent and reduce skin irritation, we used a porous acrylic chin pad for the patients who were given reverse chin cup.[7] As mentioned, there is still limited information available in this field. Further studies with larger sample sizes and three-dimensional and functional assessments are recommended to validate these findings.
Limitation
It is well known and accepted that airway space measurement cannot be determined using a 2D lateral cephalometric radiograph as this is a 3D air space. This is a drawback to this study that does not consider this important fact. The lateral cephalogram and airway space measurement method can have major confounding factors, such as patient head posture during radiograph and tongue position. I recommend that future studies be done using cone-beam computed tomography. However, this study is a basic one for future studies.
CONCLUSION
In this study, the reverse chin cup and face mask effectively corrected Class III malocclusion and notably contributed to a significant increase in the posterior airway space. Notably, the face mask exhibited a greater enhancement in the posterior airway space than the reverse chin cup. However, the two groups had no significant difference regarding the posterior airway space changes. Importantly, these positive changes persisted even after a 1.5-year follow-up period. However, to solidify these findings, it is imperative to corroborate them clinically through comprehensive analyses of breathing function and ability.
Acknowledgments
The authors thank all the subjects for their participation in this study.
Authors’ contributions
MF: Data acquisition and drafting; AJ: Conception, drafting, revision, and final approval of the version and corresponding authors; MK and KM: Design of the work and revision of important intellectual content; VG and LN: Literature review, analysis, and interpretation of the data. All authors read and approved the final version of the manuscript.
Ethical approval
The research/study was approved by the Institutional Review Board at IAU Local Research Ethics Committees, number IR.IAU.Dental.REC.1395.032, dated 11th April 2016.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship: Nil.
References
- Components of adult class III malocclusion. J Oral Maxillofac Surg. 1984;42:295-305.
- [CrossRef] [Google Scholar]
- The evaluation of maximum bite force in the occlusal rehabilitation of patient with Angle Class III malocclusion: A case report. J Adv Prosthodont. 2013;5:364-8.
- [CrossRef] [Google Scholar]
- The oropharyngeal airway in young adults with skeletal class II and class III deformities: A 3-D morphometric analysis. PLos One. 2016;11:e0148086.
- [CrossRef] [Google Scholar]
- Airway volume for different dentofacial skeletal patterns. Am J Orthod Dentofacial Orthop. 2011;139:e511-21.
- [CrossRef] [Google Scholar]
- Craniofacial changes and symptoms of sleep-disordered breathing in healthy children. Dental Press J Orthod. 2015;20:80-7.
- [CrossRef] [Google Scholar]
- Orthodontic treatment planning: Limitations, controversies and special problems In: Proffit WR, ed. Contemporary orthodontics (4th ed). St.Louis: Elsevier; 2007.
- [Google Scholar]
- A novel approach in treatment of maxillary deficiency by reverse chin cup. Int J Orthod Milwaukee. 2010;21:27-31.
- [Google Scholar]
- Orthopedic treatment outcomes in class III malocclusion: A systematic review. Angle Orthod. 2008;78:561-73.
- [CrossRef] [Google Scholar]
- Components of class III malocclusion in juveniles and adolescents. Angle Orthod. 1986;56:7-30.
- [Google Scholar]
- Cephalometric effects of face mask/expansion therapy in Class III children: A comparison of three age groups. Am J Orthod Dentofacial Orthop. 1998;113:204-12.
- [CrossRef] [Google Scholar]
- The effect of chin-cup therapy in class III malocclusion: A systematic review. Open Dent J. 2016;10:664-79.
- [CrossRef] [Google Scholar]
- Effect of orthopedic treatment for class III malocclusion on upper airways: A systematic review and meta-analysis. J Clin Med. 2020;9:3015.
- [CrossRef] [Google Scholar]
- Upper airway dimensions in class II malocclusion: Effects of headgear treatment. Angle Orthod. 2007;77:1046-53.
- [CrossRef] [Google Scholar]
- Effects of chincup or facemask therapies on the orofacial airway and hyoid position in class III subjects. J Orofac Orthop. 2015;76:520-30.
- [CrossRef] [Google Scholar]
- Airway dimensional changes following bone anchored maxillary protraction: A systematic review. BMC Oral Health. 2023;23:260.
- [CrossRef] [Google Scholar]
- Effect of class III bone anchor treatment on airway. Angle Orthod. 2015;85:591-6.
- [CrossRef] [Google Scholar]
- Craniofacial morphology in obstructive sleep apnea: A review. Clin Pulm Med. 2010;17:189-95.
- [CrossRef] [Google Scholar]
- Effects of class iii orthopaedics on pharyngeal airway: A systematic review and meta-analysis. J Pharm Negat Results. 2022;13(Suppl 10):4400-12.
- [Google Scholar]
- Three-dimensional evaluation of the upper airway morphological changes in growing patients with skeletal Class III malocclusion treated by protraction headgear and rapid palatal expansion: A comparative research. PLoS One. 2015;10:e0135273.
- [CrossRef] [Google Scholar]
- Determining the short-term effects of different maxillary protraction methods on pharyngeal airway dimensions. Orthod Craniofac Res. 2021;24:543-52.
- [CrossRef] [Google Scholar]
- Pharyngeal airway dimensions after chin cup treatment in Class III malocclusion subjects. J Oral Rehabil. 2009;36:110-7.
- [CrossRef] [Google Scholar]
- Geometric morphometric analysis of the pharyngeal airway during treatment of class III malocclusion. Am J Orthod Dentofacial Orthop. 2022;162:374-85.
- [CrossRef] [Google Scholar]
- Obesity and craniofacial structure as risk factors for obstructive sleep apnoea: Impact of ethnicity. Respirology. 2012;17:213-22.
- [CrossRef] [Google Scholar]




