

Translate this page into:
Content analysis and reliability of YouTube™ videos on clear aligner


*Corresponding author: Sanaz Sadry, Department of Orthodontics, Istanbul Aydin University, Istanbul, Turkey. sanazsadry@hotmail.com
-
Received: ,
Accepted: ,
How to cite this article: Sadry S, Buyukbasaran E. Content analysis and reliability of YouTube™ videos on clear aligner. APOS Trends Orthod 2021;11:209-17.
Abstract
Objectives:
The aim of the present study is to evaluate the accuracy and reliability of the information provided in the videos about the clear aligner on the Youtube video platform, an internet information source.
Materials and Methods:
A video search was performed on the Youtube video platform using three keywords determined with the Google Trends application. After the videos were ranked based on their view counts, a total of 75 videos were analyzed, 47 being the first for each term. After applying the exclusion criteria (repetitive content, no audio content or title information, irrelevant to the topic, only promotional content, duration over 15 min, and addressing other orthodontic treatments), the remaining 47 videos were evaluated. Regarding the videos, the following parameters were recorded: View count, number of likes, number of dislikes, number of comments, video duration, and days since the uploaded date. A scoring system consisting of seven parameters was used to classify the video content quality as low and high. The video information and quality index were utilized to evaluate the quality of the videos universally. Statistical analyses were performed with Stata/IC computer program using Shapiro–Wilks, Kruskall–Wallis, Mann–Whitney U, and linear regression (Backward method) tests. Statistical significance value was set at P < 0.05.
Results:
Evaluation of the videos based on their upload source revealed that 27 videos were downloaded from individuals, ten videos from doctors and ten videos from commercial sources, and the number of subscribers to these sources varied significantly (P < 0.05). Evaluation of the videos based on the information provided, revealed that 32 videos had poor quality, ten videos had moderate quality and five videos had good quality information content, and the video durations varied significantly (P < 0.05). It was seen that of the 75 videos viewed, only 10 (13.3%) provided information of moderate-good quality. The number of likes was found to be the parameter that significantly affects the view count (P < 0.05).
Conclusion:
YouTube videos prove insufficient as a source of information on orthodontic treatment with clear aligner. Health-care professionals should be aware of online platforms to ensure that patients can access accurate information.
Keywords
YouTube
Social media
Orthodontic treatment
Clear aligner

INTRODUCTION
In today’s world, the concept of globalization keeps growing further, and internet access plays the biggest part in this.[1] People try to meet their information needs, especially for health problems, through the internet.[2] Patients follow blogs and social media accounts that share medical information and videos, and conduct research on the internet without any restriction of access.[3] The internet is considered a valuable resource that individuals can easily gain access from almost any place without any restrictions, and that can also affect their relationships with health-care professionals.[4] The internet is among the foremost sources for information on the fields of dentistry and healthcare, as well as for face-to-face patient-clinician and patient-patient interaction.[5,6] While only 4.5% of internet users searched for health-related information on the internet in the 2000s, today, this rate has gone up to 80%.[7]
The internet is used by both non-professionals and professionals in any field to share their knowledge and experiences.[8] The sharing platform called social media offers people many advantages including independence, quickness, convenience, and universal access to information.[9] With no access restrictions and pre-check, YouTube™ interactive video platform, the second most used website in the world, can prove useful for individuals, but also contains a lot of misleading information.[10] YouTube™ is also preferred more often by patients for its ability to provide visual and audio information compared to other social media platforms.[11] Today, patients can easily obtain and share information on topics they are curious about on social media before or after treatment. However, the quality of this easily accessible information may affect patients and -indirectly- the treatment process prescribed by physicians.[12,13] Developments in the field of orthodontics particularly focus on the need for aesthetic treatment. The demand for orthodontic treatment by all age groups has created a need for esthetic and comfortable treatment. The production of more esthetic orthodontic appliances has led individuals to not only seek to have healthy teeth; it also generated a demand for orthodontic treatment to improve their appearance.[14] Individuals with aesthetic concerns refuse to wear braces on their teeth during orthodontic treatment due to their appearance, so they incline against the use of conventional fixed appliances.[15] The concern for esthetic and comfortable treatment has led patients to pursue orthodontic treatment with lower visibility, and to that end, ceramic, vinyl, polycarbonate, plastic, zirconia brackets, and teflon-coated archwires have been produced as an alternative to metal brackets.[16] Patients whose esthetic needs could not be satisfied with these tooth-colored materials have prompted physicians to adopt aesthetic orthodontic mechanics such as lingual brackets fixed to the back of the teeth or clear aligner plaques that are less visible and removable. For patients treated with these treatment types, the lack of image anxiety has also boosted self-confidence.[17] Orthodontic treatment with clear aligners has remained a good treatment alternative for patients who demand a beautiful smile without any fixed mechanics on their teeth. Clear aligner treatment, which was introduced with the appliance Invisalign (Align Technology, San Jose, Calif), debuted in 1997 and started to be used by orthodontists in 1999, is now being produced by various companies in many countries today.[18] According to 2003 data, this system is used by 40,000 patients and 6000 orthodontists in the USA and Canada. Today, there are numerous companies that manufacture it under different names. In this regard, various studies evaluated the quality of information available on YouTube™ videos on certain topics related to the fields of medicine and dentistry.[19] However, to the best of the authors’ knowledge, there is no study that analyzes the information quality of YouTube™ video contents related to clear aligner, which prove difficult for patients to understand and physicians to explain and necessitate availability of visual information. The aim of the present study is to examine the quality of the information provided by YouTube™ for patients who seek to learn about orthodontic clear aligner, to evaluate the quality and accuracy of the information provided, and to analyze the effectiveness and usefulness of the videos for patients.
The null hypothesis of this study was that there is no consistency between the view count and number of likes of the videos and the quality of the content. The authors’ alternative hypothesis is that there is a difference in content quality between videos uploaded by a dentist or specialist and videos uploaded by the public.
MATERIALS AND METHODS
Google Trends App is an online search engine used to determine how often a given keyword is searched over a certain period of time.[20] In the present study, the terms “Aligner,” “Aligners,” “Clear aligner,” “Plastic trays,” and “Transparent plate,” which are frequently searched using this application (Google Trends, 2020, Alphabet, USA), were set as the keywords [Figure 1]. The uniform source locators (URLs) of the videos were then backed up and recorded. The videos were further categorized into three main groups based on their uploaders: (1) Dentist/specialist, (2) dental clinic/ university, and (3) other. A video scan was performed by 1 Orthodontist and 1 General Dental Practitioner using the selected keywords on YouTube (https://www.youtube.com) website with the settings “Private”/“Worldwide” enabled to avoid restrictions based on user history and ensure the widest search results. In many studies carried out to evaluate the quality of the videos on the internet platform, the video search was performed using the filter “view count,” and in these studies, about thirty videos, mostly featured on the first three pages, were evaluated.[10,20,21] Each video was viewed by one of the researchers, taking into account the information content about the clear aligner. Video contents
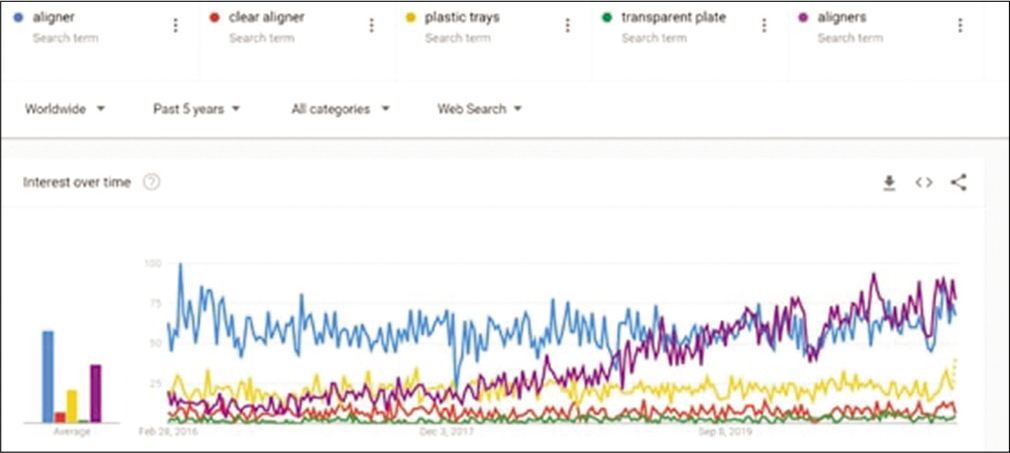
- Google trends application image used to identify keywords.
Definition of appliance: Defined in the current video as orthodontic appliances that patients can put on and remove on their own
Period of application: Talking about mixed dentition and skeletal developmental stages
Application procedure: Mentioning how the appliance is worn throughout the day, except for eating.
Benefits: Pointing out benefits such as how it is easier to clean and use and less likely to cause tissue irritation compared to fixed appliances
Types and mechanism: Mentioning the effects of the appliance depending on the types, for example, the relationship of expansion devices with and their effects on the teeth and jaw
Side effects: Pointing out the side effects such as how it affects speech and cause unwanted tooth movement
Factors to be considered: Discussing factors such as psychological effects, systemic diseases and allergic conditions related to patients.
Each video was scored based on these parameters, and the “total content score” of the video ranging from 1 to 7 was calculated. According to the resulting total content points, videos with 4 or more points were considered high-quality content videos and videos with 3 or less points were considered low-quality content videos. In addition, video information and quality index (VIQI) were used to evaluate the overall quality of a given video. Using a 5-point Likert scale ranging from 1 (low quality) to 5 (high quality) in VIQI, the flow of information, accuracy of information, quality (use of photos, animated video titles, and summary), and precision (level of consistency between the video title and content) were evaluated. After all videos have been fully watched, the following general parameters were recorded for each: (1) View count (2) time since uploaded; (3) total number of likes, (4) total number of dislikes, and (5) video duration/quality were evaluated based on the inclusion of the following parameters:
In the present study, the first thirty videos were evaluated for each keyword using the filter “view count” (from high to low). All of the first 30 videos for each keyword were carefully reviewed by a single researcher to determine which video would/would not be included in the study. Study exclusion criteria were determined as follows;
The language of the video not being in English
Repetitive video
Lack of audio content and/or title information in the video
Being irrelevant to the topic
Featuring advertising content only
Longer than 15 min
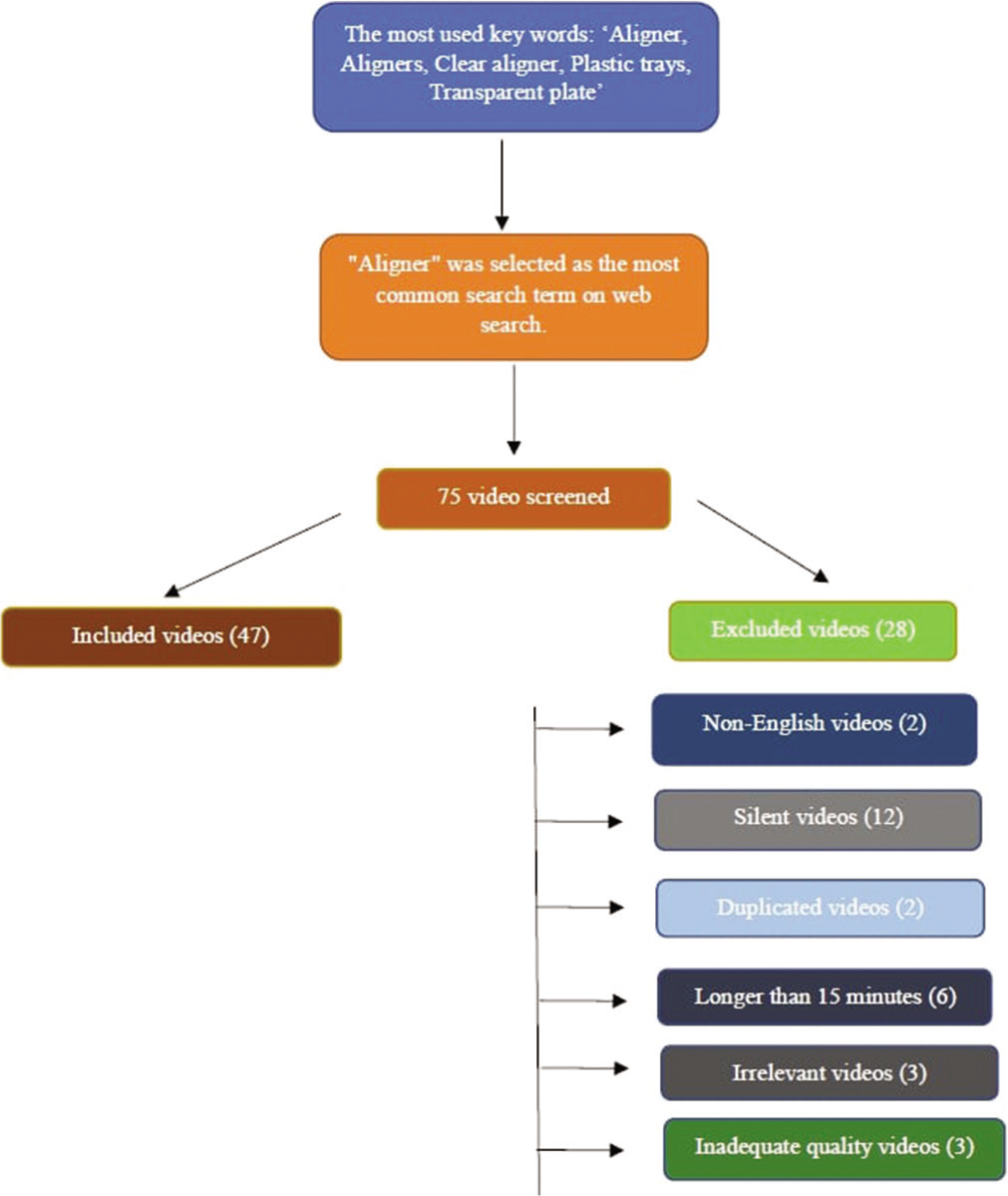
- Video selection flowchart based on exclusion criteria.
The following parameters were recorded for each video:
Header information and URL information
Video duration (in minutes)
Upload date
Time since uploaded (in days)
Poster’s number of subscribers
Source of upload (patient, doctor, and commercial)
Source of narration (patient, doctor, and voice only)
View count
Number of likes and dislikes
Number of comments.[20]
The interaction index and view rate were calculated based on the obtained data [Figure 3].
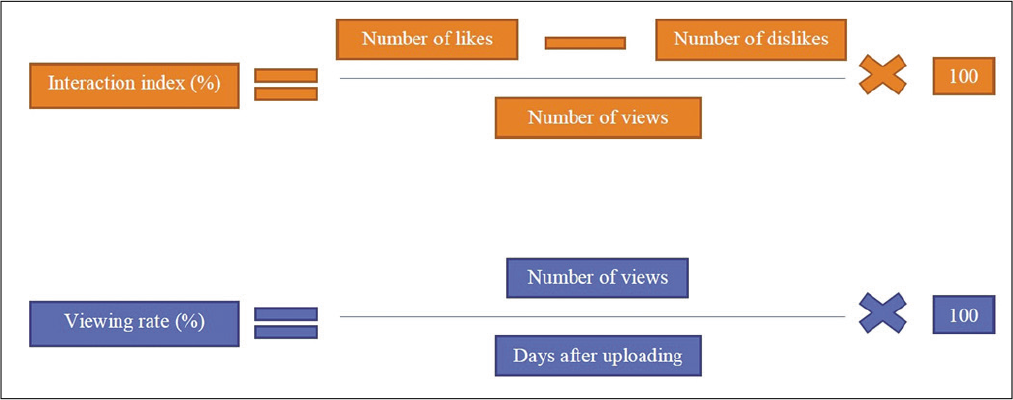
- Formulas used to calculate engagement index and viewership parameters.
The level of information regarding clear align procedure provided on the videos included in the study was evaluated using a standard scoring scale. Each video was scored in eight items in total, with the score sheet given in [Table 1]. As stated in the study by Ayrancı et al., videos with a score between 0 and 2 were considered to have “terrible-quality information content,” videos with a score between 3 and 4 to have “poor-quality information content,” videos with a score between 5 and 6 to have “good-quality information content,” and videos with a score of 7–8 to have “excellent-quality information content.” The videos were also separately categorized by upload source as upload by individual, upload by doctor, and upload by commercial organization.[20] The audio-visual quality of the videos was rated as good, moderate, and poor, as defined in the study by Sorensen et al.[21] The interaction index and viewership parameters of the videos were determined using the number of likes, dislikes, total likes and dislikes, total views, and days since uploaded, as shown by Hassona et al. [Figure 3].[22]
| Variables | n | Minimum | Maximum | Mean | Mean±SD |
|---|---|---|---|---|---|
| Video characteristics No. of views | 47 | 182 | 616563 | 7661 | 35814.87±97058.11 |
| No. of likes | 47 | 0 | 6300 | 30 | 281.26±971.57 |
| No. of dislikes | 47 | 0 | 424 | 2 | 16.17±62.62 |
| No. of comments | 47 | 0 | 958 | 2 | 46.81±156.16 |
| Duration in minutes | 47 | 42 | 880 | 186 | 245.96±178.09 |
| Days since upload | 47 | 39 | 2801 | 697 | 941.3±676.28 |
| Interaction index (%) | 47 | -0.18 | 2.3 | 0.4 | 0.49±0.46 |
| Viewing rate (%) | 47 | 87.92 | 137934 | 970.46 | 5420.69±20246.52 |
| Reliability score (orthodontist) | 47 | 0 | 5 | 2 | 1.89±1.01 |
| Global quality scale (orthodontist) | 47 | 0 | 4 | 2 | 1.72±0.93 |
| Video information and quality index (orthodontist) | 47 | 5 | 20 | 13 | 13.3±3.01 |
| Quality of video content (orthodontist) | 47 | 1 | 8 | 2 | 2.64±1.98 |
Ethics committee approval was not required for this study as it was conducted using a public website.
Statistical analysis
All statistical analyses were performed with Stata/IC (StataCorp. 2017, Stata Statistical Software: Release 15.1 College Station, TX: StataCorp LLC, Chicago, USA). The normality test was performed using the Shapiro–Wilks test for view count, likes, dislikes, video duration, time since uploaded, uploader subscriber interaction index, view rate, and number of comments. And median, minimum and maximum values were used for descriptive statistics. In linear regression analysis, backward method was used to include independent variables in the model. The Kruskal–Wallis test was used to compare the information content quality of the videos as terrible, poor, good or excellent, and the video source as individual, doctor, and commercial organization. Mann–Whitney U-test was used for between-groups pairwise comparisons. Statistical significance value was set at P < 0.05.
RESULTS
In the present study, a total of 75 videos were analyzed including the first 30 videos for each keyword. After the evaluation performed based on the exclusion criteria, a total of 47 videos were included in and 28 videos were excluded from the study [Figure 2]. Following the evaluation of all the videos, view count was found as 35814.87 ± 97058.11, number of likes as 281.26 ± 971.57, number of dislikes as 16.17 ± 62.62, interaction index as 00.49 ± 0.46, and view rate as 5420.69 ± 20246.52 [Table 1]. According to the video source, it was found that 12 videos had been uploaded by individuals, 8 videos by doctors, and 27 videos by commercial sources [Table 2]. A statistically significant difference was only found in the number of comments on the source between the groups (P ≤ 0.001). Accordingly, the highest number of comments was detected in doctor (median: 82; min: 1.00, max: 958) and commercial upload sources (median: 1; min: 0, max: 71), while the lowest number of comments was seen in individual upload sources (median: 2; min: 0 max: 34). When the videos were evaluated according to the quality level of information content, 32 videos were qualified as terrible, ten videos as poor, and five videos as good in terms of information content quality [Table 3]. With regard to the quality level of information content, a statistically significant difference was only found in video duration between the groups (P ≤ 0.043). Accordingly, the shortest video durations were seen in videos with terrible-quality information content (median: 174; min: 42 max: 880), while the longest video durations were seen in videos with good-quality information content (median: 300; min: 294 max: 676). Of the 47 videos in total included in the study, 36% featured a description of the treatment, while 20% made mention of the treatment procedure and 41% of the treatment costs [Figure 4]. Contraindications were not mentioned in any of the videos [Figure 4]. When the independent variables affecting the view count were examined using linear regression analysis, the built regression model was found to be statistically significant (F = 104.440; P < 0.001). The number of video likes increases in parallel with the view count, and a one unit increase in the number of likes boosts the view count by 221.876 views (P < 0.001). There was no significant relationship between the view count and the video duration and interaction index [Table 4].

- Graphical representation of the distribution of the scoring categories used in determining the information content category of the videos.
| Variables | Doctor (n:8) | Individual (n:12) | Commercial (n:27) | P-value | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Median | Min | Max | Median | Min | Max | Median | Min | Max | ||
| Days since upload | 924.5 | 271 | 2801 | 466 | 39 | 1686 | 702 | 207 | 2649 | 0.305 |
| Number of views | 23588 | 191 | 616563 | 5146.5 | 185 | 69688 | 4929 | 182 | 138758 | 0.201 |
| Number of likes | 138.5 | 0 | 6300 | 26 | 1 | 410 | 14 | 0 | 413 | 0.140 |
| Number of dislikes | 8.5 | 0 | 424 | 4 | 0 | 35 | 1 | 0 | 55 | 0.490 |
| Number of comments | 82 | 1 | 958 | 2 | 0 | 34 | 1 | 0 | 71 | 0.001** |
| Duration in minutes | 281 | 114 | 880 | 149.5 | 84 | 506 | 178 | 42 | 655 | 0.15 |
| Interaction index (%) | 0.76 | 0 | 1.83 | 0.47 | 0.25 | 0.66 | 0.37 | -0.18 | 2.3 | 0.149 |
| Viewing rate (%) | 2385 | 474.2 | 137934 | 1924.25 | 394.42 | 15486.22 | 1490 | 187.92 | 12718.1 | 0.118 |
| Variables | High Quality (n:5) | Moderate Quality (n:10) | Low Quality (n:32) | P-value | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Median | Min | Max | Median | Min | Max | Median | Min | Max | ||
| Days since upload | 1026 | 625 | 1686 | 1542.5 | 39 | 2801 | 511.5 | 121 | 2649 | 0.11 |
| Number of views | 22519 | 6650 | 251995 | 11016.5 | 185 | 138758 | 4417.5 | 182 | 616563 | 0.104 |
| Number of likes | 40 | 0 | 2400 | 34.5 | 1 | 413 | 17 | 0 | 6300 | 0.457 |
| Number of dislikes | 5 | 0 | 77 | 4.5 | 0 | 17 | 1 | 0 | 424 | 0.116 |
| Number of comments | 7 | 2 | 297 | 2 | 0 | 419 | 1.5 | 0 | 958 | 0.095 |
| Duration in minutes | 300 | 294 | 676 | 179.5 | 100 | 506 | 174 | 42 | 880 | 0.043* |
| Interaction index (%) | 0.4 | 0 | 1.54 | 0.37 | 0.16 | 0.66 | 0.41 | -0.18 | 2.3 | 0.873 |
| Viewing rate (%) | 2194.83 | 394.42 | 23550.93 | 914.31 | 115.08 | 6825.28 | 777.64 | 87.92 | 137933.6 | 0.246 |
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | |
|---|---|---|---|---|---|---|---|---|
| 1. Days since upload | ||||||||
| r | 1.000 | |||||||
| p | ||||||||
| 2. Number of views | ||||||||
| r | 0,440** | 1 | ||||||
| p | 0.002 | |||||||
| 3. Number of likes | ||||||||
| r | 0.331* | 0.900** | 1 | |||||
| p | 0.023 | 0.000 | ||||||
| 4. Number of dislikes | ||||||||
| r | 0.357* | 0.837** | 0.782** | 1.000 | ||||
| p | 0.014 | 0.000 | 0.000 | |||||
| 5. Number of comments | ||||||||
| r | 0 | 0.705** | 0.698** | 0.629** | 1 | |||
| p | 0.131 | 0.000 | 0.000 | 0.000 | ||||
| 6. Duration in minutes | ||||||||
| r | –0.03 | 0 | 0.053 | –0.151 | 0.169 | 1 | ||
| p | 0.843 | 0.992 | 0.724 | 0.311 | 0.256 | |||
| 7. Interaction index (%) | ||||||||
| r | –0.209 | 0.215 | 0.535** | 0.191 | 0.284 | 0.167 | 1.000 | |
| p | 0.159 | 0.146 | 0 | 0.197 | 0.053 | 0.263 | ||
| 8. Viewing rate (%) | ||||||||
| r | 0.005 | 0.876** | 0.809** | 0.736** | 0.649** | –0.014 | 0.332* | 1 |
| P | 0.974 | 0.000 | 0.000 | 0 | 0.000 | 0.924 | 0.022 |
DISCUSSION
Since the quality of the videos uploaded to YouTube™ was poor in terms of orthodontics, with an average of 2.82 points, the authors accepted the null hypothesis, which proposes that the content quality of the videos is not consistent with the number of likes and view count. This is because, in the correlation index, the video content quality score and like index showed weak positive correlation (+0.331), while the view percentage (–0.110) did not. The authors rejected the second hypothesis, which proposes that the videos uploaded by a dentist or a specialist are of higher quality compared to other uploaders, as there was no statistically significant difference between the groups (P = 0.226).
Today, many patients and parents use social media tools to learn more about their treatments. With the advancements in technology, the internet has become one of the main sources utilized in obtaining information on any health-related subject. About 81% of people use the internet for health-related research. YouTube video sharing site is an internet platform frequently used for obtaining information on any subject. Although some of the studies measuring the quality of information accessed through social media tools have evaluated other platforms, YouTube™ has been the one mostly examined in such studies.[14,20,23] As one of the social media tools, YouTube™ is frequently used by patients for its rich visual content and easy access to information, unlike professional scientific platforms. However, the validity of the information on YouTube™ is questioned due to the ease of video sharing and the lack of standardization for the content of the uploaded videos.[24] It is for this reason that the present study chose to evaluate YouTube™ among other social media platform and the quality of the content on dental orthodontics uploaded to this platform.
The platform contains a huge number of videos on a wide variety of health-related topics. Dentistry studies conducted using the YouTube™ video sharing platform investigate numerous topics including orthognathic surgery, genioplasty, cleft lip and palate, acceleration of orthodontic tooth movement, toothache, root canal treatment, and early childhood caries. However, there is no available study in the literature that examines the quality and accuracy of the information on the clear aligner treatment procedure provided by the videos on YouTube.[25]
There are quite a number of search terms available on clear align on the YouTube™ platform. However, to be able to make an objective selection of the most searched terms, the Google Trends application, which was used in the previous studies as well, was used and the top three most searched terms were selected as keywords. The view counts, number of likes, number of dislikes, and other similar parameters can allow a video to be evaluated as ‘useful’ or “not useful.” Although the evaluation of such videos is subjective, the video content is very effective for the viewer to obtain information on the subject.[25] The present study found the quality level of information provided by YouTube videos on clear aligner plaque to be quite insufficient. Similarly, in a study evaluating the quality of the YouTube™ video platform in terms of offering information on surgical-assisted clear aligner, the quality and reliability of information offered to patients by relevant videos were found to be low. Furthermore, according to the results of the aforementioned study, it was stated that only 25% of the videos provided information of moderate quality. The present study, on the other hand, found that only 12 (13.3%) of the 90 videos provided information of moderate-good quality.[26]
Clear aligner is an orthodontic issue that remains difficult for patients and their parents to understand and for physicians to explain. Because individuals are often unable to fully comprehend the three-dimensional design as well as different designs of removable plates, they are worried about their difficulty of use and side effects. In such cases today, physicians or patients usually refer to visual content providers such as YouTube™. Al-Silwadi et al.[9] investigated the importance of social media in raising the knowledge level of patients undergoing fixed orthodontic treatment and found that social media tools such as YouTube™, which convey audiovisual information, improve the level of knowledge of orthodontic patients. However, as shown in [Table 1], 47 (62.7%) of the 75 videos that appeared when the term clear aligner was searched were irrelevant, repetitive and did not feature sound or visuals. In a study by Elkarmi et al.[14] examining the quality of the YouTube™ videos on early childhood carries, this rate was found to be 50%. This is a clear indication of the fact that individuals and physicians have difficulty in accessing information due to redundant videos, even if they type the right search terms. The authors examined the content quality of the remaining 47 YouTube™ videos after excluding the redundant ones that did not meet the ideal criteria. Knosel and Jung[27] conducted a study to measure the knowledge level of orthodontic content on YouTube™ and concluded that although YouTube™ is a platform for sharing patient experiences, the related videos are insufficient in terms of content. When the authors evaluated the quality of the videos based on the combination of the criteria established by “American Association of Orthodontists’ Clinical Practice Guidelines for Orthodontics and Dentofacial Orthopedics American Association of Orthodontists” 25 and the authors’ clinical observations, the results were found to be insufficient, with an average of 2.64 ± 1.98 out of 7. In addition, the number of videos with terrible content with a score between 1 and 3 points and lower is 32 (42.3%), while the number of videos with poor content with a score between 4 and 6 points is 11 (39.4%) and the number of videos with good content with a score between 7 and 9 points was 4 (14.3%). When the videos with high, moderate, and low quality content are compared, the videos with rich content were more competent in terms of clear aligner definition, application time, side effects, and factors to be considered (P < 0.05), while no difference was found in terms of application procedures, benefits, and types (P > 0.05). Based on these results, the reason the definition and purpose of the appliance also refer frequently to the application procedures may be to provide an answer to the questions that first comes to mind such as; “What is this plate?” and “What happens if I wear it?” The reason the plaque types factor, the other result with no difference, was mentioned less frequently in both groups may be due to the existence of numerous plate types and avoiding excessive technical information not to tire out the viewer. When the two groups were compared in terms of likes, duration and views, no significant difference was found between videos with high-quality content and videos with low-quality content (P > 0.05). Considering the VIQI, a universal index for evaluating video quality in visual, auditory, and informative terms, no significant difference was found between the two groups (P > 0.05). This indicates that the VIQI proves insufficient in terms of evaluating the medical content and that not enough attention is paid to the visual quality of the video. The reason why there is no difference between the view percentages may be due to the disadvantages of videos with rich content such as long duration, incompatibility with the VIQI, lack of emphasis on visual quality and featuring excessive information. Lena et al.[28] reported no difference in VIQI when comparing videos with rich and poor content in individuals undergoing lingual orthodontic treatment, which is also consistent with the present study. In some other studies, views and video ratings were similar among videos found to be helpful or misleading.[29] Due to ongoing controversy about medical information available online, the vast majority of patients continue to rely on their physicians over online information.[30] However, given the popularity of YouTube™ and its potential use as an important source of medical information in the future, patients need to be referred to appropriate sources. Videos uploaded by the public serve a social purpose, in that, they enable the public to share their own experiences, but videos produced by health institutions often feature more educational content.[31] In the present study, no statistical difference was found when comparing the uploaders of clear aligner videos (P > 0.05). The lack of videos uploaded by the public, which are expected to have low video content quality, may have prevented the authors from making an ideal comparison. Considering the videos reviewed by the authors, it was seen that an average of 3–4 years have passed since some of them were uploaded. The possibility that experience, technology and visual effects will pave the way for the emergence of better quality video content on clear aligner in the near future was ignored in the present study. On the other hand, it should also be noted that YouTube™ variables such as view rate, likes, and dislikes are prone to manipulation.
There were several limitations of this study. One of the limitations was that the evaluation is done by a single investigator.
CONCLUSION
A wide range of information on clear aligner is available on the YouTube™ platform. The platform is not a reliable and useful source of information on clear aligner. However, the content of the YouTube™ videos about clear aligner was mostly insufficient. The majority of the videos talked about application procedures and basic information, while only a few mentioned use, factors to consider, timing of administration, and side effects. Therefore, patients seek to use YouTube™ to learn about clear aligner may have difficulty finding high-quality content videos. According to the content analysis used in this study, it was seen that the number of videos with good-quality information content is quite low. This fact indicates that the YouTube video platform is an insufficient source of information on clear aligner. In the light of these findings, the authors think that it is highly crucial for dentists, specialists, and dental healthcare providers to stay informed about the information available on the internet rather than the information made available by commercial organizations, and to conduct studies on this issue so that patients can have easier access to accurate and reliable information.
Acknowledgments
The authors would like to thank the Vice Chancellor for research, Istanbul Aydin University for supporting the research. In addition, we express our gratitude to Dr. Cansu G. Koca (Assist.Prof) for her valuable contribution to the article interpretation.
Declaration of patient consent
Patient’s consent not required as patient’s identity is not disclosed or compromised.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Health information quality of websites on periodontology. J Clin Periodontol. 2017;44:308-14.
- [CrossRef] [PubMed] [Google Scholar]
- Does YouTube™ offer high quality information? Evaluation of accelerated orthodontics videos. Ir J Med Sci. 2020;189:505-9.
- [CrossRef] [PubMed] [Google Scholar]
- YouTube as a patient-ınformation source for cleft lip and palate. Cleft Palate Craniofac J. 2020;57:327-32.
- [CrossRef] [PubMed] [Google Scholar]
- Patients using the ınternet to obtain health information: How this affects the patient-health professional relationship. Patient Educ Couns. 2006;63:24-8.
- [CrossRef] [PubMed] [Google Scholar]
- Twitter analysis of the orthodontic patient experience with braces vs ınvisalign. Angle Orthod. 2016;87:377-83.
- [CrossRef] [PubMed] [Google Scholar]
- Healthcare information on YouTube: A systematic review. Health Informatics J. 2015;21:173-94.
- [CrossRef] [PubMed] [Google Scholar]
- Online social networking by patients with diabetes: A qualitative evaluation of communication with Facebook. J Gen Intern Med. 2011;26:287-92.
- [CrossRef] [PubMed] [Google Scholar]
- Patients' use of the Internet for pain-related medical information. Patient Educ Couns. 2007;68:86-97.
- [CrossRef] [PubMed] [Google Scholar]
- Effect of social media in improving knowledge among patients having fixed appliance orthodontic treatment: A single-center randomized controlled trial. Am J Orthod Dentofacial Orthop. 2015;148:231-7.
- [CrossRef] [PubMed] [Google Scholar]
- YouTube™ as an information resource for orthognathic surgery. J Orthod. 2017;44:90-6.
- [CrossRef] [PubMed] [Google Scholar]
- YouTube as a source for parents' education on early childhood caries. Int J Paediatr Dent. 2017;27:437-43.
- [CrossRef] [PubMed] [Google Scholar]
- An analysis of widely viewed youtube videos on anal cancer. Int J Prev Med. 2017;8:74.
- [Google Scholar]
- Social perceptions of adults wearing orthodontic appliances: A cross-sectional study. Eur J Orthod. 2010;33:476-82.
- [CrossRef] [PubMed] [Google Scholar]
- Automated custom-manufacturing technology in orthodontics. Am J Orthod Dentofacial Orthop. 2003;123:578-81.
- [CrossRef] [Google Scholar]
- Clear aligner appliances: Fabrication and clinical application. Turk J Orthod. 2009;22:256-66.
- [CrossRef] [Google Scholar]
- Clear aligner: An efficient, esthetic, and comfortable option for an adult patient. World J Orthod. 2007;8:13-8.
- [Google Scholar]
- Invisalign A to Z. Am J Orthod Dentofacial Orthop. 2002;121:540-1.
- [CrossRef] [PubMed] [Google Scholar]
- Is ınformation for surgically assisted rapid palatal expansion available on YouTube reliable? J Oral Maxillofac Surg. 2020;78:1017.e1-10.
- [CrossRef] [PubMed] [Google Scholar]
- Are YouTube™ videos a reliable source of information about genioplasty? J Stomatol Oral Maxillofac Surg. 2021;122:39-42.
- [CrossRef] [PubMed] [Google Scholar]
- YouTube as an information source for pediatric adenotonsillectomy and ear tube surgery. Int J Pediatr Otorhinolaryngol. 2014;78:65-70.
- [CrossRef] [PubMed] [Google Scholar]
- YouTube as a source of information on mouth (oral) cancer. Oral Dis. 2016;22:202-8.
- [CrossRef] [PubMed] [Google Scholar]
- YouTube video analysis as a source of information for patients on impacted canine. Int Orthod. 2019;17:769-75.
- [CrossRef] [PubMed] [Google Scholar]
- Using the internet for health-related activities: Findings from a national probability sample. J Med Internet Res. 2009;11:e4.
- [CrossRef] [PubMed] [Google Scholar]
- Are video sharing web sites a useful source of information on hypertension? J Am Soc Hypertens. 2014;8:481-90.
- [CrossRef] [PubMed] [Google Scholar]
- Cleft lip and palate YouTube videos: Content usefulness and sentiment analysis. Cleft Palate Craniofac J. 2020;58:362-8.
- [CrossRef] [PubMed] [Google Scholar]
- Informational value and bias of videos related to orthodontics screened on a video-sharing Web site. Angle Orthod. 2011;81:532-9.
- [CrossRef] [PubMed] [Google Scholar]
- Lingual orthodontic treatment: A YouTube™ video analysis. Angle Orthod. 2018;88:208-14.
- [CrossRef] [PubMed] [Google Scholar]
- Levels of toothache-related interests of Google and YouTube users from developed and developing countries over time. PeerJ. 2019;7:e7706.
- [CrossRef] [PubMed] [Google Scholar]
- YouTube as a patient-information source for root canal treatment. Int Endod J. 2016;49:1194-200.
- [CrossRef] [PubMed] [Google Scholar]
- The accuracy of ınformation about orthodontics available on the ınternet. Turk J Orthod. 2018;31:127-32.
- [CrossRef] [PubMed] [Google Scholar]




