

Translate this page into:
Contrary to an old belief, four corner curing does not provide more bond strength or polymerization in bonding of orthodontic metal brackets

-
Received: ,
Accepted: ,
How to cite this article: Behroozian A, Rezaei Y, Abdulkarim BA, Moghaddam SF. Contrary to an old belief, four corner curing does not provide more bond strength or polymerization in bonding of orthodontic metal brackets. APOS Trends Orthod 2022;12:157-61.
Abstract
Objectives:
The study aimed to investigate the effect of the direction of light curing on bond strength and adhesive polymerization of orthodontic metal brackets.
Material and Methods:
In this in vitro investigation, 75 extracted human upper premolars were randomly divided into three groups according to the curing direction: Group A (20 s curing from the occlusal side of the bracket), Group B (10 s from occlusal and 10 s from gingival), and Group C (5 s from four corners of the bracket). After bonding, the brackets were subjected to a shear bond strength (SBS) test performed with a universal testing machine. Moreover, Fourier transform infrared spectroscopy (FTIR) analysis was used to find the polymerization ratio of the adhesives in each group. Kruskal–Wallis test was to statistical analysis of SBS and FTIR data, respectively, at the 0.05 level of significance.
Results:
The difference in SBS of metal brackets was not statistically significant between the groups (P > 0.05). However, the difference in polymerization ratio was significant between all groups where the highest and lowest ratio belonged to Groups A and B, respectively (P < 0.05).
Conclusion:
Curing metal brackets from four corners do not increase their bond strength and/or polymerization.
Keywords
Bond strength
Polymerization
Light cure
Metal brackets
Orthodontics

INTRODUCTION
Using of light-polymerizing composite has become increasingly popular in the bonding of fixed appliances since its introduction for orthodontics by Newman.[1] Light curing adhesives have many advantages such as controlled working time, extended time for bracket repositioning, and easier removal of residual composite.[2]
Bond strength to the enamel which can be measured by shear bond strength (SBS) is of importance in fixed orthodontics to achieve treatment goals.[3] Adequate bond strength is achieved by ensuring that photons of light curing units reach the composite and polymerize it.[4,5] The prevalence of orthodontic bond failure varies from 6% to 17.6%[6,7] and both clinicians and manufacturers are trying to reduce bond failure. Since metal brackets inhibit light photons to reach the underlying composite, some studies have tested transillumination but the results were not encouraging unless with increasing curing time and intensity.[5,8]
On the other hand, the polymerization of bisphenol A-glycidyl methacrylate (Bis-GMA) which is known as the monomer material of dental composite takes place with the conversion of carbon double bonds to single bond in bisGMA monomers.[9] Conversion of carbon double bonds to single bond during curing of the composite can reflect the degree of conversion which can affect the properties of final polymer.[10] The degree of conversion is determined by the proportion of remaining double bonds to the total number of double carbon bonds in the uncured composite.[11]
There is an old belief that four corner light curing of bracket composite results in higher bond strength compared to one-sided curing. The philosophy behind it is that the intensity of the light cure photons decreases by increasing the distance between curing tip and composite[2,12] so it is necessary to bracket adhesives to be cured from all four directions. However, to date, no study has challenged this allegation whether it is true or not.
In this study, we aimed to investigate the effect of three different modes (four corners, two-sided, and one-sided) of curing orthodontic metal brackets on SBS and polymerization using Fourier Transform Infrared Spectroscopy (FTIR).
MATERIAL AND METHODS
Sampling
Seventy-five extracted human upper premolars were collected and divided randomly into three groups each 25 teeth. The inclusion criteria of selected teeth were intact buccal enamel, no history of the application of chemical adhesives, no visible cracks, and no restorations and caries extended to the buccal surface. We washed the teeth with water to remove contaminations and then stored them in a bottle containing distilled water at 4°C. The time between extraction and the tests was no longer than 3 months.
Specimen preparation
The buccal surfaces of all teeth were cleaned with oil-free, non-fluoride pumice, and then rinsed with water and dried with moisture-free Airstream for 20 s. Then, the enamel was etched with a conventional 35% phosphoric acid (Ultra Etch, Ultradent Products Inc, South Jordan, USA) for 20 s. Then, the etched surface was rinsed for 20 s until the etchant was completely removed and then dried with oil and moisture-free air source to achieve a frosted appearance. A thin uniform coat of Transbond XT primer (3 M Unitek, Monrovia, CA, USA) was applied to the etched enamel surfaces and Transbond XT (3 M Unitek, Monrovia, CA, USA) adhesive was applied to the bracket bases. The brackets used in this study were stainless steel mesh base premolar with a 0.022-in slot (Master Series Brackets, American Orthodontics, WI, USA). Immediately, the brackets were placed on the tooth surface in their standard position and then pressed firmly. Excess resin material was carefully removed from around the bracket with a dental probe without disturbing it before polymerization.
Before light curing, the teeth were randomly divided into three groups each containing 25 teeth based on the mode of curing [Figure 1]:

- (a-c) Three groups based on the mode of irradiation; Group A: One-sided, Group B: Two-sides, and Group C: Four corners curing.
Group A: 20 s curing from the occlusal aspect of the bracket.
Group B: 10 s from the occlusal and 10 s from the cervical aspect.
Group C: 5 s from four corners of the bracket.
The brackets were light-cured with a conventional QTH curing light (Litex 680A, Dentamerica Inc., California, USA) for 20 s. Irradiation was performed from the bracket edges at an angle of 45° to the surface. All bonding procedures were performed by an orthodontist. For keeping blindness, the remaining process of the study was done by another orthodontist who was not aware of the types of curing. For this, the first clinician placed the samples in three different boxes with the codes unrelated to the type of bonding and the study proceeded with these codes. After finishing the tests and statistical analyzes, the codes were translated to group names by the first clinician.
After bonding, the teeth were embedded in self-curing acrylic resin using a standard plastic cylinder which was prepared in the size to be fitted in the universal testing machine (Hounsfield Test Equipment: H5K Model, England). We used a jig to position the buccal surface of the premolars perpendicular to the base of the cylindrical specimen holder ring with the help of the slot of the bracket. Therefore, the buccal surface of the teeth will be parallel to the arm of the universal testing machine. Then, the embedded teeth were stored in distilled water at 37°C for 24 h.
Tastings
SBS
The universal testing machine (Hounsfield Test Equipment: H5K Model, England) was used to measure SBS. The acrylic cylindrical specimens were located in the holder rings in such a way that the occlusogingival force applied to the bracket was parallel to the facial surface of the teeth. The load required to debond the bracket was recorded in Newton (N) at a speed of 0.5 mm/min. To blindness, the operator who did the debonding procedures was unaware of the content of the groups and the teeth were given numbers that were unrelated to their group codes.
FTIR spectroscopy
Immediately after debonding, the remnant composite was collected and composite particles were ground into a fine powder. Then, the powder was stored in a dark box until the onset of the FTIR test. Ten milligrams of the fine ground powder were mixed with 100 mg of KBr powder. This mixture was placed into a pelleting device and then pressed for 1 min to obtain a pellet. Then, the pellet was placed into a holder attached to the spectrophotometer.
The polymerization ratio was monitored by the FTIR spectroscopic analysis in transmission mode and it can be convertible to absorbance mode, using the device’s software. The FTIR spectrometer (Bruker Tensor 27 IR, Bruker, Germany) ran under the following conditions: Spectral range: 7500–370 cm−1, wavenumber range accuracy: 0.01 cm−1, resolution: Better than 1 cm–1, and scan speed: 20 kHz (12.7 mm/s opd, from 32 scans). The percentage of unreacted carbon-carbon double bonds (C=C) was determined from the ratio of absorbance intensities of aliphatic C=C. The transmission ratio of the aliphatic C=C peak at 1638 cm−1 can be determined with this test.
Statistical analysis
We use a one-sample Kolmogorov–Smirnov test for checking the normality. The data were not normal. Hence, we used Kruskal–Wallis test for assessing the significance between the groups. All statistical analysis was done with SPSS (version 24.0, Chicago, IL) and P < 0.05 was considered significant.
RESULTS
The result of SBS measurement is reported in [Table 1]. The difference between the groups was not significant (P > 0.05).
| Bond strength (n) | |||||
|---|---|---|---|---|---|
| Mean | Minimum | Maximum | SD |
P value |
|
| Group A (occlusal) | 80.85 | 23 | 202.20 | 39.45 | 0.419 |
| Group B (occlusal and gingival) | 99.88 | 37 | 273.5 | 58.08 | 0.419 |
| Group C (four corner) | 100.57 | 25.70 | 240 | 55.50 | 0.419 |
P<0.05 shows significant difference
[Table 2] represents the result of FTIR test where the transmission ratio of the groups is reported in 1638 cm-1 wavelength. Statistical analysis showed that the difference between the groups was significant (P = 0.001). Group A had the highest transmission ratio and Group B had the lowest value. [Figure 2] shows the graph representing the transmission of photons in different wavelengths in three groups.
| Transmission ratio |
P value |
||||
|---|---|---|---|---|---|
| Mean | Minimum | Maximum | SD | ||
| Group A (occlusal) | 0.91128 | 0.91104 | 0.91689 | 0.01048 | 0.001* |
| Group B (occlusal and gingival) | 0.83738 | 0.83707 | 0.84629 | 0.00883 | 0.001* |
| Group C (four corner) | 0.89089 | 0.89081 | 0.90195 | 0.00468 | 0.001* |
*P<0.05 shows significant difference
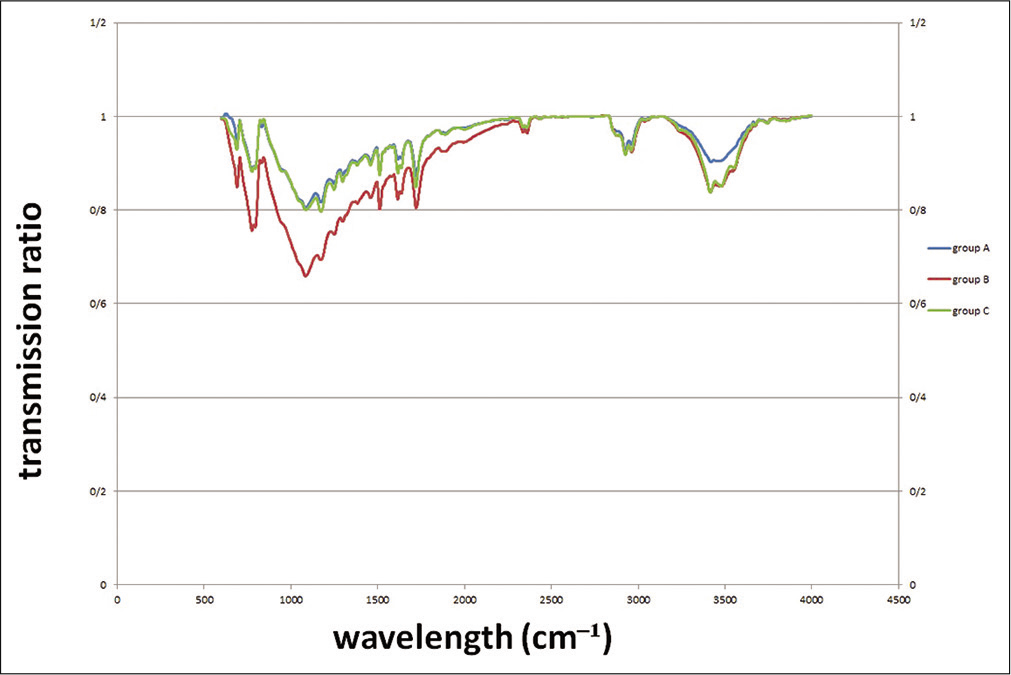
- Transmission ratio of photons in different groups at 1638 cm−1 wavelength.
DISCUSSION
Using of light cure for polymerization of adhesive of orthodontic brackets is a routine process that each orthodontist may encounter in the office every day. Finding the best protocol and direction of curing is of importance and interest to increase the bond strength and efficiency of the treatment. In this in vitro study, we found no significant difference in bond strength between one-sided, two-sided, and four corner curing groups. However, FTIR test result showed that the polymerization was significantly higher in the one-sided group compared to the other groups.
SBS
The overall average of SBS in the present study was 93.81 N. The area of the bracket base was calculated at 10.31 mm2. Hence, the mean pressure for debonding was 9.09 MPa which is comparable with the results of Endo et al.[13] and Bishara et al.[3] who reported 11.94 MPa and 7.0–12.2 MPa, respectively, for permanent teeth. They also used a universal testing machine for debonding. In the present study, SBS of all groups was well beyond the acceptable range of bond strength for successful clinical performance which is 6–8 MPa.[14] This shows that all three directions of light curing can be acceptable. Hobson et al. emphasized that, at this range of bond strength, < 14% of bonds would fail in the worst scenario.[15]
The theory behind the suggestion of four corner curing is that metal brackets are not translucent and the light cannot pass through them, so some authors propose curing from different directions to achieve adequate bond strength by ensuring that photons of light cure reach all layers of composite and completely polymerize it.[16,17] However, our study showed that this theory is not true. A possible explanation is that the diameter of light tube (8 mm) is completely larger compared to the width of the bracket (3.5 mm); therefore, with curing from one aspect, other aspects receive a degree of curing automatically and changing the direction of the tube may not be necessary.
Polymerization ratio
By polymerization of the Bis-GMA, double carbon-carbon bonds of monomers change into single bonds.[18] A single carbon-carbon bond absorbs fewer photons in wavelengths of 1638 cm–1 compared to double carbon-carbon bonds; therefore, the amount of transmitted or absorbed photons can reflect the degree of polymerization.[19,20] In the present study, we found that one-sided curing results in a higher polymerization ratio compared to other groups.
The question is why SBS did not increase significantly despite higher polymerization in one-sided curing group? Can it be related to other types of polymerization like circular or crosslinking reaction rather than linear propagation that increase the transmission but do not necessarily increase the bond strength?[20] It seems that for bonding of metal brackets with continuous unidirectional 20 s curing results in more polymerization compared to interrupt multidirectional curing.
Some researchers investigated the effect of transillumination curing from the lingual aspect of the tooth on bond strength.[4] Their theory was that since the composite polymerizes toward the source of energy so the resin tags will penetrate deeply into enamel rods and this, in turn, will result in a stronger bond.[21] The other theory was that because the tooth structure is partially transparent light photons that can reach the adhesive through the tooth. However, a lot of studies showed that transillumination on itself cannot increase the bond strength of orthodontic brackets unless there was increased curing time and light intensity.[4,22] However, this increases chair time and the risk of pulpal damage and reduces the efficiency of the procedure.[23,24]
On the other hand, a higher polymerization ratio which was seen in one-sided curing has other potential advantages rather than SBS. It has been demonstrated that higher DC decreases the age-dependent discoloration of composite.[25] Furthermore, the release of uncured Bis-GMA may be hazardous for the patient[9] and higher DC can prevent these side effects.[26] A high degree of monomer convergence is vital to enhance color stability and biocompatibility.[27]
Limitations and suggestions
We suggest repeating the study with attachments with smaller or larger bonding bases like lingual buttons and buccal tubes. Needless to say that we cannot overgeneralize the results of the present study to porcelain brackets because of their transparency. Furthermore, the question, why the increase in the degree of conversion does not guarantee higher bond strength, remained unanswered and more investigations are needed to answer that. Furthermore, we suggest repeating the study by adding the aging process. We suggest adding thermocycling of the samples before debonding and use of LED units in future studies.
CONCLUSION
One-sided curing had the highest polymerization whereas the bond strength did not change significantly.
Acknowledgments
We would like to acknowledge the staff of the dental biomaterial laboratory of the faculty of dentistry who warmly helped us during data collection.
Authors’ contributions
AB and BAA initiated, conceptualized, and supervised the research work. SFM and YR prepared samples and collect the data with the collaboration of AB. All authors have contributed to analyzing the data and writing the manuscript.
References
- Epoxy adhesives for orthodontic attachments: Progress report. Am J Orthod. 1965;51:901-12.
- [CrossRef] [Google Scholar]
- An ex vivo investigation into the bond strength of orthodontic brackets and adhesive systems. Br J Orthod. 1999;26:47-50.
- [CrossRef] [PubMed] [Google Scholar]
- Effect of changing a test parameter on the shear bond strength of orthodontic brackets. Angle Orthod. 2005;75:832-5.
- [Google Scholar]
- Evaluation of shear bond strength of orthodontic brackets using trans-illumination technique with different curing profiles of LED light-curing unit in posterior teeth. Prog Orthod. 2013;14:49.
- [CrossRef] [PubMed] [Google Scholar]
- Bracket bond strength with transillumination of a light-activated orthodontic adhesive. Angle Orthod. 2001;71:307-11.
- [Google Scholar]
- A 5-year clinical review of bond failure with a light-cured resin adhesive. Angle Orthod. 1998;68:351-6.
- [Google Scholar]
- Eighteen-month bracket survival rate: conventional versus self-etch adhesive. Eur J Orthod. 2008;30:94-9.
- [CrossRef] [PubMed] [Google Scholar]
- In vitro evaluation of shear bond strength of orthodontic stainless steel brackets using transillumination. J Clin Exp Dent. 2018;10:e450-7.
- [CrossRef] [PubMed] [Google Scholar]
- Changes on degree of conversion of dualcure luting light-cured with blue LED. Laser Phys. 2009;19:1050-5.
- [CrossRef] [Google Scholar]
- Degree of polymerization of resin composites by different light sources. J Oral Rehabil. 2002;29:1165-73.
- [CrossRef] [PubMed] [Google Scholar]
- Bond strength and clinical efficiency for two light guide sizes in orthodontic bracket bonding. Br J Orthod. 1997;24:35-40.
- [CrossRef] [PubMed] [Google Scholar]
- Comparison of shear bond strengths of orthodontic brackets bonded to deciduous and permanent teeth. Am J Orthod Dentofacial Orthop. 2008;134:198-202.
- [CrossRef] [PubMed] [Google Scholar]
- The effect of moisture and blood contamination on bond strength of a new orthodontic bonding material. Am J Orthod Dentofacial Orthop. 2001;120:54-7.
- [CrossRef] [PubMed] [Google Scholar]
- Effect of light-tip distance on the shear bond strengths of composite resin. Angle Orthod. 2005;75:386-91.
- [Google Scholar]
- Human prismless enamel and its influence on sealant penetration. Arch Oral Biol. 1973;18:441-4.
- [CrossRef] [Google Scholar]
- Primary cyclization in the polymerization of bis-GMA and TEGDMA: A modeling approach to understanding the cure of dental resins. Dent Mater. 2001;17:221-9.
- [CrossRef] [Google Scholar]
- Evaluation of polymerization efficacy in composite resins via FT-IR spectroscopy and vickers microhardness test. J Dent Res Dent Clin Dent Prospects. 2015;9:226-32.
- [CrossRef] [PubMed] [Google Scholar]
- Modelling ATR-FTIR spectra of dental bonding systems to investigate composition and polymerisation kinetics. Materials (Basel). 2021;14:760.
- [CrossRef] [PubMed] [Google Scholar]
- Bracket bond strength with transillumination of a light activated orthodontic adhesive and the effect of curing time and tooth thickness on it: An in vitro study. J Ind Orthod Soc. 2013;47:148-53.
- [CrossRef] [Google Scholar]
- Bond strengths of lingual orthodontic brackets bonded with light-cured composite resins cured by transillumination. Am J Orthod Dentofacial Orthop. 1987;91:312-5.
- [CrossRef] [Google Scholar]
- Pulp temperature rise induced by light-emitting diode light-curing units using an ex vivo model. Materials (Basel). 2019;12:411.
- [CrossRef] [PubMed] [Google Scholar]
- Light-curing units used in dentistry: Factors associated with heat development-potential risk for patients. Clin Oral Investig. 2017;21:1687-96.
- [CrossRef] [PubMed] [Google Scholar]
- Effect of exponential polymerization on color stability of resin-based filling materials. Dent Mater. 2007;23:696-704.
- [CrossRef] [PubMed] [Google Scholar]
- Effect of the degree of conversion of resin-based composites on cytotoxicity, cell attachment, and gene expression. Dent Mater. 2019;35:1173-93.
- [CrossRef] [PubMed] [Google Scholar]
- Oxidative stress and cytotoxicity generated by dental composites in human pulp cells. Clin Oral Investig. 2012;16:215-24.
- [CrossRef] [PubMed] [Google Scholar]




