

Translate this page into:
Current status of dental and orthodontic education in European and American countries

*Corresponding author: Kazuo Tanne, Department of Orthodontics and Craniofacial Developmental Biology, Hiroshima University Graduate School of Medical Sciences, Hiroshima 734-8553, Japan. tanne@hiroshima-u.ac.jp
-
Received: ,
Accepted: ,
How to cite this article: Tanne K. Current status of dental and orthodontic education in European and American countries. APOS Trends Orthod 2019;9(4):211-22.
Abstract
This article was designed to elucidate the current status of dental and orthodontic education in the European and American countries by a questionnaire survey through internet. In Europe, the size of orthodontic society and the number of orthodontic department or dental school are small when compared to those in USA. In Europe and South America, it takes 5 to 6 years to complete undergraduate dental education for dentist. Meanwhile, in Canada and USA, dental school system has been developed, requiring 8-year education to become dentist. For orthodontic specialists, in general, it takes 3 years on average in European and American countries with an exception of 4-year training in Switzerland. Most societies in European and American countries have two important issues such as inappropriate orthodontic treatment and incorrect use of aligners by general practitioners. The most important strategy is to appeal the public that orthodontic treatment should be executed by orthodontic specialists. In conclusion, it is shown that the educational systems for dentist and orthodontist have well been developed in every country in the world, although the strength is somewhat different from country to country.
Keywords
Dental education
Post-graduate orthodontic program
Europe and America
Important issue for orthodontists

INTRODUCTION
Orthodontic treatment has been distributed widely according to the development of technology in the field of mechanical engineering, material science, and informatics. However, the current status of dental and orthodontic education in many countries is unclear and beyond our understanding. From these considerations, I have conducted an internet interview survey to elucidate the current status of dental and/or orthodontic professionals, including education in the Asian Pacific region and already published an article on this subject.[1]
Thus, this article was designed to elucidate a useful information about the current status of dental and orthodontic education in the European and American countries and compare the outcome with that in the Asian-Pacific countries.
MATERIALS AND METHODS
Internet interview
A questionnaire was sent to very important persons in the European and American countries and collected through internet.
The interviewees are shown below [Figure 1].

- A list of interviewees in the European and American countries.
Dr. Rainer-Reginald Miethke (Germany)
Dr. Allahyar Geramy (Iran)
Dr. Moschos A. Papadopoulos (Greece)
Dr. Hans-Peter Bantleon (Austria)
Dr. Birte Melsen (Denmark)
Dr. Allan R. Thom (United Kingdom)
Dr. Stavros Kiliaridis (Switzerland)
Dr. Abbas R. Zaher (Egypt)
Dr. Ravindra Nanda (Connecticut, USA)
Dr. Steven Lindauer (Virginia, USA)
Dr. Peter Ngan (West Virginia, USA)
Drs. Kang Ting and Won Moon (California, USA)
Dr. Greg Huang (Washington, USA)
Dr. Glenn Sameshima (California, USA)
Dr. Jae Hyun Park (Arizona, USA)
Drs. Claude Remise, Jack Turkewicz and Clarice Nishio (Canada)
Dr. Roberto Justus (Mexico)
Dr. Rodrigo Iván del Pozo Ayabaca (Columbia)
Dr. Jorge Faber (Brazil).
The interview was designed to ask the following questions through the internet.
Current status of orthodontics in each country in terms of the number of orthodontists or members in the orthodontic society, and the number of dental schools or orthodontic departments
Educational process to become dentist and orthodontist in each country
Academic careers of professors and their departments in terms of the history, the faculty or teaching members, the number of residents, the tuition fee required for postgraduate orthodontic courses, and so on. This question was sent to a limited number of interviewees.
Important issues for orthodontic specialists
All the information and comments replied by each interviewee were shown in the text. In addition, numerical data were summarized in tables for a better understanding of readers.
RESULTS
Current status of orthodontics in each country in terms of the numbers of orthodontists or members in the orthodontic society and dental schools or orthodontic departments
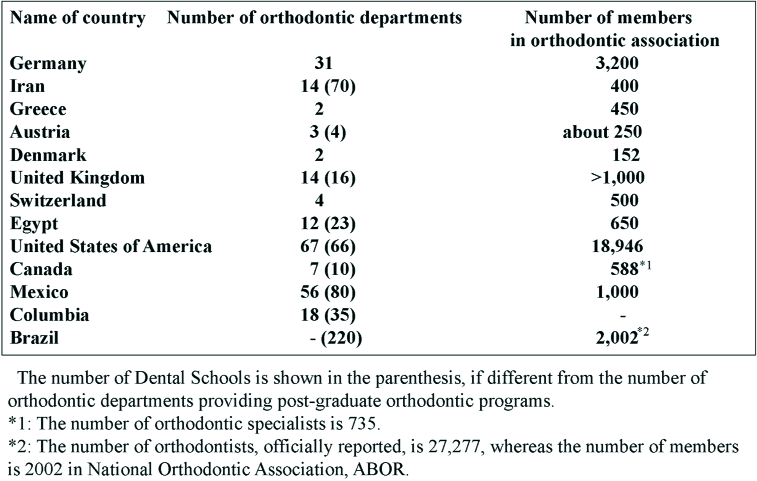
The numbers of orthodontic departments and members are shown in Table 1. The replies or comments from each interviewee are shown below.
Germany
The number of practicing orthodontic specialists in Germany is around 3,000. The most relevant orthodontic society (Deutsche Gesellschaft für Kieferorthopädie) has roughly 3200 members. This includes retired practitioners and a good number of international members. Germany has 31 dental schools, and all of these have smaller or bigger orthodontic departments.
Iran
In Iran, we have <70 dental schools. We need to explain that the number of dental schools was <20 in the past 20 years. The increase was accelerated in the past two decades to give a proper answer to the demand of young students seeking continuing education in dentistry in foreign countries. Theoretically, all dental schools have orthodontic departments. Of course, we cannot have the same strength in all the departments. We are about 400 in Iran and 14 departments are training postgraduate students.
Greece
Greece is a country located in the southeast part of Europe, a member of the European Union, and has almost 11,000,000 citizens. Dental health is provided by 14,000 dentists, while orthodontic health is provided by almost 450 orthodontic specialists. Orthodontics is the only one specialty in dentistry that is officially recognized by the Greek state. There is another one specialty related to dentistry, Oral and Maxillofacial Surgery, this is a medical specialty, although it demands from the practitioners to obtain both the medical and dental degrees.
In Greece, there are only two Schools of Dentistry, one at the National University of Athens (capital of Greece) and the other one at the Aristotle University of Thessaloniki (the second largest city in Greece, but with the biggest University in the country). Consequently, there are two department of orthodontics in our country, each corresponding to either School of Dentistry in Athens and Thessaloniki.
Austria
There are three public (Medical Universities of Vienna, Innsbruck, and Graz) and one private dental school (Danube Private University) in Austria. Every public university has its orthodontic department, where postgraduate students can attend a 3-year orthodontic education.
In Austria, there are about 250 orthodontists, who are a member of the orthodontic society (ÖGKFO, VÖK 333). Because of the missing state of recognition in Austria, there does not exist an official number of orthodontists.
Denmark
There are two dental schools that educate dentists and specialists. Every year seven orthodontic specialists graduate after the completion of the official program. The number of active specialists in the Danish Society of Orthodontics is 152.
United Kingdom
Orthodontic treatment in the UK can be either private or funded by the state called the National Health Service (NHS). To be funded by the NHS, the patient must be under the age of 18, and the malocclusion within the categories of index of treatment need 4 or 5.
Orthodontic treatment is generally provided by orthodontists in their offices/practices. Specialized orthodontics such as cleft lip and palate and orthognathic is provided by consultant orthodontists who are hospital based.
There are over 1000 registered orthodontists in the UK. There are 16 dental schools and 14 postgraduate orthodontic programs of 3 years full-time duration.
Switzerland
Switzerland is a country of 8.2 million people, 6.2 million Swiss, and 2 million foreigners. Approximately 300 Swiss- educated orthodontists and 200 orthodontists from other European countries are working in Switzerland. Nevertheless, some of the orthodontic patients are treated by non-specialized dentists.
The specialist education in Orthodontics in Switzerland is provided in the four dental schools of the following universities: University of Geneva in the French-speaking part, and Universities of Basel, Bern, and Zurich in the German-speaking part of the country.
Egypt
I am happy to brief the readers about the status of the Egyptian Orthodontic Society. It was established in 1986 and is the only society representing all and only the specialists in orthodontics in Egypt. The specialist in Egypt is a dentist who has a minimum of 2 years of full-time graduate education in a formal academic institution accredited in Egypt and leading to a master’s degree in orthodontics, or any equivalent certificate from outside the country that is recognized by the High Council of the Egyptian Universities.
The Egyptian Orthodontic Society currently comprises about 650 members, and the numbers are increasing quickly every year. The membership categories include active, student, affiliate, and honorary members. Most orthodontists in Egypt are members of the society with very few exceptions.
There are 23 dental schools in Egypt among which 12 are governmental, and the rest are private schools. In these, there are 12 graduate orthodontic programs contributing to the graduation of around 35 new orthodontists every year.
USA
Orthodontics as a profession is at the top of all professions in USA. American Association of Orthodontists (AAO) is doing a wonderful job as ever representing orthodontists and orthodontic programs.
As of 2016, the number of AAO members is 18,946. Among these, the numbers of AAO and international members are 15,754 and 3192, respectively.
In the USA, we have 66 Accredited Dental Schools and 73 Accredited Orthodontic Programs including six programs in Canada.
Canada
Currently, in Canada, there are ten dental schools, seven of which offer orthodontic postgraduate programs. All of them consist of a 3-year full-time Masters of Science in Orthodontics program (MSc). The University of Alberta, University of Toronto, and University of British Colombia also provide Doctorate Programs in Orthodontics (PhD). The Canadian chairmen of the orthodontic graduate programs are as follows:
Dr. Claude Remise (Université de Montréal)
Dr. Jean Marc Retrouvey (McGill University)
Dr. William Wiltshire (University of Manitoba)
Dr. Sunjay Suri (University of Toronto)
Dr. Antonio Mamandras (University of Western Ontario)
Dr. Carlos Flores-Mir (University of Alberta)
Dr. Edwin Yen (University of British Colombia).
According to the most recent report “Dental Health Services in Canada,” published in 2010 by the Canadian Dental Association,[2] the specialty with the highest number of dentists is orthodontics, with approximately 735 orthodontists. The Canadian Association of Orthodontists (CAO-ACO) has reported 588 active members in 2000 (https://cao-aco.org).
Mexico
The Asociacion Mexicana de Ortodoncia has approximately 1500 members. The Academia Mexicana de Ortodoncia has approximately 1000 members. The total number of orthodontists in Mexico is probably 10,000, You can observe that the majority of orthodontists do not belong to any orthodontic society.
There are 80 schools of dentistry and 56 orthodontic departments.
Columbia
The population of Colombia is approximately 50,000,000 people. In Colombia, officially, there are 35 faculties of dentistry and 18 postgraduate courses of orthodontics (including a new one). All of them are for “clinical specialties” and there are no Masters and PhD degrees.
Of those 18, four are in public universities and 14 in private universities. Six of them are in the capitol Bogotá, five in Medellín (Second biggest city in Colombia), and the rest distributed in different small cities in the county.
Brazil
Currently, the number of dentists is 118,006 (female; 65,203, male; 52,803). The number of orthodontists is 27,277 (female; 15,982, male; 11,295).
http://cfo.org.br/website/estatisticas/
As of 2017, the number of dental schools is 220, whereas the number of the orthodontic department could not be found.
In Brazil, we have the specialization course. Many courses are not part of a university. Ministry of Education allows private courses without any university association.
https://doi.org/10.30979/rev.abeno.v18i1.399
In Brazil, there are two associations of orthodontists. In ABOR (National association), there are 2002 members, whereas no information in the other association, Sao Paulo State Association.
Educational process to become dentist and orthodontist in each country
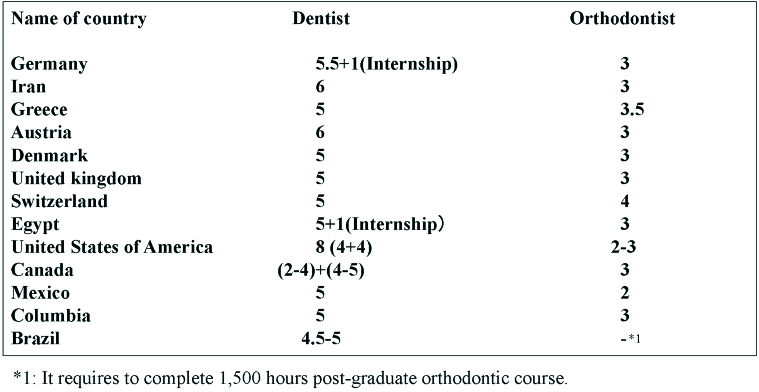
Table 2 shows the duration of educational systems for dentists and orthodontic specialists in each country.
The replies and the relevant comments are shown below for a better understanding of the readers.
Germany
Principally, a student in dentistry needs minimally 5.5 years to complete academic education. After this, she/he has to work for 1 year as an employed general dentist in a general dental office. Following, she/he needs 3 years of orthodontic specialist training. The basic regulation of this training is that she/he has to study at a university orthodontic department for at least one year but she/he can spend two or all three years there. On the other side, the trainee can spend 1 or even 2 years in a private office which is acknowledged for its training capacity. Two of the 3 years have to be continuous. In any case, there is an oral and/or written final examination. It has to be remembered, however, that Germany is a federal state and the dental chambers of each state are independent, i.e., their rules vary, though only slightly.
Iran
Our curriculum consists of 12 semesters. Our dental students start with a four-semester course to learn basic sciences. After passing a national exam they will start their preclinic course which is a 1-year course to learn the basic points of operative dentistry and prosthodontics on dental models. After this course, they start to treat patients under the direct supervision of their instructors. In the 6th year, they choose a topic and a professor to conduct research and write a report as their dissertation, which will be explained and defended before a jury of five, and if accepted he/she is called “doctor….”
If he/she is allowed to register for the postgraduate course, he/she will take a national exam to get the permission to enter one of the departments to spend a 3-year course in orthodontics. We have 14 departments to spend this course. Our postgraduate students treat patients under the supervision of their instructors, and at the same time, they conduct a research as the partial fulfillment of their qualification. They explain the research before a 7-member jury, and then if accepted, they will be graduated. They should pass a national board exam which has oral section. At this time, they can start their services as assistant professors of different departments or treating patients.
Greece
The duration of the undergraduate studies in dentistry in Greece as – in all European countries – up until now is 5 years. After that period, one is allowed to go to private practice or to continue with postgraduate studies. Both universities in Athens and Thessaloniki offer a great variety of postgraduate studies, including orthodontics, pediatric dentistry, periodontology, endodontics, conservative dentistry, prosthetics, implantology, and oral surgery. These studies usually last in total 3 years, with one or two exceptions related to dental fields that are not so broad, such as community dentistry.
Postgraduate studies in orthodontics last 3.5 years (7 semesters). They are provided only either at the Department of Orthodontics of the National University of Athens or at the Department of Orthodontics of the Aristotle University of Thessaloniki. After completion of a minimum of a 3 years full-time period of postgraduate studies in Greece or abroad, a dentist is eligible to participate in the examinations organized by the Ministry of Health, to receive the official title of the orthodontic specialty from the Greek state.
Austria
The minimum duration of study in dentistry is 6 years. During dental education, students acquire the theoretical basics of orthodontics. To become an orthodontist, postgraduate education is necessary. Because of missing state recognition, there is no officially regulated education in Austria (as well as in Spain) for orthodontists until today, but there are enough possibilities to undergo a voluntary education. Since 2014 Vienna Medical University is part of the Network of Erasmus Based European Orthodontic (NEBEOP) Programmes. It comprises a group of orthodontic postgraduate training programs in Europe represented by program directors or orthodontists assigned by institutes, which deliver a structured program in orthodontics equivalent to a minimum of 3 years full time. The primary concern of the network is education, specific to the specialty of orthodontics, and the main purpose is the advancement of orthodontic postgraduate training in Europe. At the moment, there are eight postgraduate students in education at the University Clinic of Vienna.
Denmark
The dental education is a 5-year full-time program. To become a specialist in orthodontics in Denmark, you have to finish the above-mentioned dental degree and work a minimum of 2 years with general dentistry. Of these, 2 years or a minimum of 1440 h have to be with pedodontics. Hereafter, the specialty education which is 3 years full-time at one of the two dental schools can be initiated. The education is finished with an oral examination based on a master’s degree and a presentation of ten finished cases.
United Kingdom
The undergraduate program is 5 years full time. The postgraduate orthodontic program is 3 years full time. To specialize as a consultant in a hospital setting, an additional 2 years of orthodontic training is necessary.
Switzerland
To become dentist in Switzerland demands 5 years full-time education in one of the following universities; University of Geneva in the French-speaking part, and Universities of Basel, Bern, and Zurich in the German-speaking part of the country.
The annual number of new educated dentists from all the four Swiss Universities is about 150. The applicants for specialist education in orthodontics should have at least 1 year of experience in general dentistry. Then, they have to go through a tough selection procedure to become postgraduate students (one out of ten Swiss or foreign candidates). The postgraduate students follow a 4-year full-time program, according to the guidelines of the NEBEOP, as published by Huggare et al.[3] in the Eur. J. Orthod. In my University in Geneva as well as in Bern, specialist education is combined with a Master of Science program.
Egypt
To become a dentist, one needs to complete 5 years in a recognized Dental School in addition to a 1 year of internship, rotating in the various clinical departments.
All graduate programs in orthodontics are leading to a master’s degree in orthodontics. Graduate orthodontic programs are 3 years of clinical and didactic training as well as the preparation of a thesis.
USA
To become a dentist in the USA, you need 4 years of college degree after high school and then 4 years of dental school education. The majority of the orthodontic programs are of 30–36 month duration. Five or six programs are only 24-month duration.
Canada
Entrance to dental school requires completing at least 2 years of undergraduate university pre-requisites, although most students entering dental programs in Canada have a bachelor’s degree. Most dental school curriculums cover 4 years of study, although, in some schools, such as the Université de Montreal (UdeM), it is 5 years. On completion of the accredited 3-year Masters orthodontic program, the resident needs to successfully pass the national specialty examination conducted by the Royal College of Dentists of Canada. This step is required to obtain recognition and designation as a dental specialist by the professional licensing bodies of each province.
Mexico
It takes 5 years for dental students to graduate. Most orthodontic programs are 2-year programs.
Columbia
To become dentist, 5-year education is required in dental school. The postgraduate program for the orthodontic specialist is of 3 years or six semesters.
Brazil
Time for graduation is 4.5–5 years for dentists. It requires 1500 h to become orthodontic specialists.
Academic career as a Professor and the Department of Orthodontics in terms of the history, the faculty or teaching members, the number of residents, the tuition fee required, and so on
Dr. Moschos Papadopoulos (Aristotle University of Thessaloniki, Greece)
The postgraduate program in orthodontics we have at the School of Dentistry of the Aristotle University of Thessaloniki, of which I (Prof. Moschos Papadopoulos) am happy to serve as Director, is in function since 1994. It was organized from the very beginning according to the European Union’s standards for specialization in orthodontics, and since last year after a positive assessment is full member of the NEBEOP. The NEBEOP is a network of European Postgraduate Programs of Orthodontics, which function according to the national legislation but, at the same time, meet high guidelines regarding their structure and their content, set by the Erasmus Program of the European Union. The main purpose of the NEBEOP is the quality of postgraduate training in orthodontics and its advancement in European countries. The number of the Networks’ full members is limited and to become one, requires a thorough and on-site evaluation of the postgraduate program. The status of «full member» of the NEBEOP verifies the quality of the postgraduate training provided by the Department of Orthodontics of the Aristotle University of Thessaloniki in international level, and reflects to the long term and the strenuous efforts of the faculty members, as well as of the students who participate in the postgraduate program.
Dr. Abbas Zaher (Alexandria University, Egypt)
The sschool of dentistry including a Department of Orthodontics in Alexandria University was first founded in 1944 and was a school under the auspices of the Faculty of Medicine. It then became the independent Faculty of Dentistry in 1970. At first, the number of accepted residents in the graduate program of orthodontics was variable. Some years, it accepted three, and some years, only one student was accepted. Nowadays, we regularly accept five students per year. Education is free for Egyptian students, including graduate studies. However, recently, because of the lack of resources, the Faculty started to charge a minimal fee for the usage of the clinics and equipment. This nominal fee is around $1,500/year.
Dr. Peter Ngan (West Virginia University, USA)
I actually graduated from high school in Hong Kong and came over to the United States for my college education. I was accepted into a combined Pediatric Dentistry and Orthodontics specialty program at the University of Pennsylvania.
West Virginia University School of Dentistry is the only dental school in the state of West Virginia. The Department of Orthodontics started in 1968, graduated its first class in 1970. Since its inception, over 150 orthodontists in various parts of the country can call themselves Alumni of WVU Department of Orthodontics. All have been dedicated to delivering the highest quality of orthodontic care possible.
The orthodontic program leading to a Master of Orthodontics degree and certificate is a 3 years program, and we accepted three residents each year.
The program currently has one full-time Chair, one program director, and eight part-time clinical instructors. Each resident starts around 50 new cases during the 1st year of training and inherits the same number of cases from the previous residents. In general, they complete around 80% of their started cases on graduation.
The tuition and supplies for out of state students are approximately $22,000 for the 1st and 2nd years of education. Tuition is waived for the 3rd year, and students receive a stipend of $13,777.
Dr. Ting Kang (University of California Los Angeles [UCLA], USA)
UCLA was founded in 1919, and the school of dentistry was founded in 1964. In 1970, Dr. Spiro Chaconas developed the orthodontic program, the first post-doctoral program at UCLA. It was a 2-year program with two residents per year. Now, we have grown into a substantially larger and more comprehensive program, one that is 3 years in duration.
We have five full-time, four half-time, and about 30 part- time faculty members; eight post-doctoral residents (3-year program) per year (four domestic and four international), and 6–8 international Advanced Clinical Training program (1-year program) students. The 3-year post-doctoral orthodontic program grants Commission on Dental Accreditation (CODA)-approved orthodontic certificates and MS degrees in Oral Biology.
Our international tuition for a 3-year CODA approved post-doctoral orthodontic program is $70,000/year, plus the tuition for the Oral Biology MS Program. The 1-year ACT program has $55,000 tuition.
Dr. Greg Huang (University of Washington, USA)
My dental education was at the University of Florida (UF), and my orthodontic education was at the University of Washington (UW). I also obtained an Master of Public Health (MPH) (major in epidemiology) from the UW.
After obtaining my certificate in orthodontics and Master of Science in Dentistry from UW, I moved back to my hometown in central Florida, where I practiced for 10 years. During that time, I taught 1 day each month in the graduate clinic at UF. After I had been in practice for about 7 years, I started thinking seriously about a full-time academic career, and began looking for opportunities. Eventually, that decision led me to an offer for a full-time position at UW, with concurrent enrollment in the MPH program (focusing on epidemiology). This additional training has been invaluable in my endeavors with clinical research and evidence-based orthodontics. When I first joined the faculty in 1999, I held the title of Acting Assistant Professor. After 3 years, I became an Assistant Professor. I was promoted to Associate Professor in 2005, and I became Chair of the Department in 2008. In 2011, I achieved the rank of full professor.
Dr. Alton Moore founded our department around 1949, and the second faculty member at UW was Richard Riedel. Over the years, we have had four other chairs – Don Joondeph, Peter Shapiro, Greg King, and me. We have also had some very influential faculty members, including David Turpin, Robert Little, and Vincent Kokich. We also have some very well-known alumni, including William Proffit, Arthur Dugoni, Peter Sinclair, Roberto Justus, and Patrick Turley.
Currently, we have four full-time and four half-time faculty members. We also have more than 30 affiliate faculty members who teach in the graduate clinic and various courses. Each year, we admit five students into our 33-month program. Our students earn a Certificate in Orthodontics, as well as a Masters of Science in Dentistry. Out-of-state tuition is about $37,000 USD each year.
Dr. Glenn Sameshima (University of Southern California [USC], USA)
On graduation from the University of California San Francisco, I served as a general dentist in the US Air Force. I was stationed at Yokota Air Base outside Tokyo for 4 years. I did my orthodontic training and PhD in craniofacial biology at USC; when I finished both, my instructors Professors Harry L. Dougherty and Sakae Tanaka hired me to teach part-time. When Peter Sinclair became chair a few years later, I was hired full time. I was appointed clinic director in 2003, the year I was promoted to Associate Professor with Tenure. In 2006, I became chair and program director.
The USC Orthodontic Program started in 1934, the first formal program on the West Coast. The Angle School was a few miles away, so the first faculty members were all trained by Angle. We currently accept six residents per year, with no geographic restrictions. We have had students from many countries. Clinical faculty must be board certified with experience in private practice. Most are Angle Society members and active in organized orthodontics. Board certification is a primary goal for the students. Tuition is the same regardless of nationality. The program is 34 months long.
Dr. Jae Park (Arizona A.T. Still University, USA)
The postgraduate orthodontic program at the Arizona School of Dentistry and Oral Health opened its doors in 2007. We look forward to graduating our 10th class in December 2018. We are currently a 30-month program with over 20 adjunct faculty members, and we accept five residents per year. We also offer a 1-year fellowship program to international and domestic dentists. More information about the program, admissions, and tuition can be found at https://www.atsu.edu/asdoh/programs/orthodontics/
Dr. Claude Remise (Université de Montréal [UdeM], Canada)
At the UdeM, we annually accept a maximum of five residents for the orthodontic master’s program. Depending on whether we have filled our quota of residents, we may also be able to offer one or two positions for the Dental Specialty Assessment and Training Programs (DSATP, Gap training). This program is intended to assess the clinical knowledge, skill, and judgment of internationally-trained dental specialists or graduates of non-accredited dental specialty programs.
The tuition fees for the postgraduate orthodontic program at UdeM vary according to the status of the student. The fees per trimester is in Canadian dollars; $1,227.75 for Quebec residents, $3,815.85 for Canadian non-residents in Quebec, and $8,407.73 for foreign students.
The orthodontic graduate program at UdeM started in 1947 and remained a 2-year certificate program until 1996 when it became a 3-year masters orthodontic program. To date, 283 orthodontic residents have graduated from our orthodontic program.
Dr. Rodrigo del Pozo (Universidad Cooperativa de Columbia, Columbia)
After I graduated in the Department of Orthodontics Hiroshima University Graduate School of Biomedical and Health Sciences in March 2002, I returned to my home city in Caracas-Venezuela. I started working in my private practice and as a Cathedratical Professor in the postgraduate course of Orthodontics, Faculty of Dentistry, Universidad Central de Venezuela, Caracas-Venezuela. Due to the political and economic turmoil of my home country, I decided to search for new opportunities in another country. That is how, after searching, the Department of Orthodontics, Faculty of Dentistry, Universidad de Antioquia in the city of Medellín- Colombia offered me a position as a full-time visiting Professor. I accepted and moved to Medellín-Colombia. I have been living in Medellín with my family for the past 10 years. Currently, I am a Cathedratical Professor in the postgraduate course of Orthodontics, Faculty of Dentistry, Universidad Cooperativa de Colombia in charge of the clinic of MBT Philosophy and the seminars of TMJ and TMD. I am in charge every semester of eight residents.
The tuition fee is approximately US$ 3,000 each semester, and the postgraduate program is of 3 years (6 Semesters).
Dr. Jorge Faber (Federal University of Rio de Janeiro, Brazil)
I got my master’s degree in orthodontics from the Federal University of Rio de Janeiro in 1994. This program completes 60 years of foundation in 2018 and is the oldest in Brazil. Subsequently, I did my PhD at the University of Brasilia (UnB) in Animal Biology, Morphology, in 2003. My primary research during my PhD was on periodontal distraction, a still promising technique for periodontal regeneration.[4]
Today I work in my private practice – which is focused on adult patients and in the postgraduate program of the UnB, where I am the advisor of three masters and one PhD student at this moment. UnB’s postgraduate program is new; it was created in 2017. All Federal universities in Brazil are public. This means students do not pay tuition fees for undergraduate and postgraduate programs.
Important issues for orthodontic specialists
Various problems specified to each country or district are shown below.
Germany
There are some general dentists who do orthodontics. However, their number is commonly not a real problem for orthodontic specialists. The only existing problem to some degree is prophylactic service which is offered by both parties. Hence, there is an overlap of interest. If this latent conflict is clarified, both can coexist well.
Iran
When I decided to become an orthodontist, general dentists were not involved in this field. We do not have fixed orthodontic courses in the undergraduate curriculum. Logically, they did not treat complicated patients. Now, we have several general dentists who think they are able to treat patients. Currently, there are private clinics and institutes where orthodontics and some other fields like implant are taught. Based on my experience in orthodontic education, it is not an accepted method to teach how to treat orthodontic patients. I, as the coordinator of post-graduate studies in our department, try to provide a full-time program for our post- graduate students and one of the classes which is a constant part of this program is the case presentation. It is not so easy for me to say all of them are qualified in this field after 1 or 2 years. In their 3rd year, they can be considered as dentists able to manage a case according to standards. How could this ability be transferred to general dentists in a not-so-long period in a private clinic or office?
Greece
This is an actual problem in whole Europe but not in only Greece. According to the European guidelines, a general dentist is eligible to provide his/her patients with any kind of dental treatment including orthodontics. Thus, although there are strict rules that these colleagues cannot use the official title of “specialist in orthodontics” they can still provide orthodontic treatment.
Another phenomenon, which is also increased during the last years along with the financial crisis, is that some general dentists with well-known and/or big offices, hire young orthodontists as employees to work part-time for 1–2 days a week in their offices to provide orthodontic services to their patients.
Austria
For example, aplasia, orthodontists favor space closure to prevent prosthetic treatment. Dentists often prefer a quick and less extensive way of treatment by providing the gap with implants. However, this can lead to future problems like vertical bone deficiency. A good cooperation between dentist and orthodontist is important to choose the best solution, which differs from case to case.
Denmark
It is still relatively seldom that the general dentist performs orthodontics, but the internet advertisement is starting to have an influence, and aligners, and small fixed appliance treatments are becoming more popular by the public. I personally feel that the so-called “fast food orthodontics” may have the capacity to destroy our profession and this is not specially aligners that may deliver custom made treatments but the “fast and easy treatments” many of which can be detrimental both for the patients and for the image of our profession.
United Kingdom
The British Orthodontic Society has a number of generalists in the society. While these generalists have not received formal specialty training, many have undergone additional part-time orthodontic training and are keen to continue to learn.
Unfortunately, there are generalists who attempt to carry out orthodontic treatment with little or no training often relying on 3rd party diagnosis and treatment planning from remote laboratories. Unfortunately, many of these cases are poorly treated.
Switzerland
The overall relation between orthodontists and general dentists is very good, aiming to the best of their common patients. The orthodontist is an essential member of the multidisciplinary team and leads often the discussions for the treatment planning of difficult cases. However, there are some general dentists who are not convinced that the collaboration between the different disciplines is to the benefit of the patient, so they try to do everything by themselves, ending some times to tragic results. Problems may also appear in the treatment of malocclusions by general dentists who are not educated to intervene with comprehensive orthodontic means. Unfortunately, for the patients they need often to repeat the treatment. Nevertheless, these events of orthodontic treatment by nonorthodontists are not the rule but rather the exception in the treatment of malocclusions.
Egypt
This is a sensitive issue! The law in Egypt does not recognize orthodontics as a specialty yet. We have made some progress to have the Ministry of Health and the Dental Syndicate recognize the specialty of orthodontics, but these efforts were fruitless so far due to the change of government several times in the past few years. The Egyptian Orthodontic Society is taking the lead to lobby a change in the laws of medical practice to obtain recognition.
Hence, the current law permits the general dentist to provide orthodontic treatment. Many dentists target the short orthodontic courses that claim it will be enough to teach and train them to become proficient in a short period of time. They advertise that they only concentrate on the essentials and skip the “unnecessary” basic science and “dry knowledge.” The fact is that these courses are mostly given by unqualified practitioners and lead the participants to believe that they have become capable of managing various types of orthodontic cases. Many patients who are not aware of the specialty and are attracted by the lower prices, end up suffering mediocre service and poor treatment results and in most of the cases seek re-treatment with a specialist.
The Egyptian Orthodontic Society is in the process of fighting these misleading courses by developing a national awareness campaign that targets the end-users, i.e., the patients. The main messages in this campaign are: Orthodontics is the specialty of dentistry that is concerned with the correction of teeth alignment, bite correction, as well as jaw discrepancies; an orthodontist requires extra training in an academic institution for an average of 3 years after being a dentist; and all the members of the Egyptian orthodontic society are qualified specialists.
We are faced with two major obstacles or concerns; the campaign should not dismay the general dentist population and should reach a large sector of the population and run for an extended period of time. In a large country like Egypt, such a campaign will incur a very high cost.
USA
Dr. Ravindra Nanda
Few years back it was a big issue, but in recent years all is quite on this front. A significant number of general dentists use aligner therapy. AAO has taken an active role in educating general public regarding training and expertise of orthodontists.
Dr. Steven Lindauer
Orthodontists in my area, and all over the US, definitely complain that more general dentists are doing orthodontics and therefore decreasing the number of patients that they refer for treatment by specialists. This may be due to the increase in the availability of aligners to straighten teeth, which is claimed by many specialists to be the cause. On the other hand, a lot of the complaining I used to hear has decreased dramatically now that the economy has improved again. Orthodontists have changed their own marketing techniques to attract patients directly rather than relying on general dentists to refer patients to them.
I believe that orthodontists, rather than general dentists, will win whatever “battle” there is over the patients seeking orthodontic treatment. Orthodontists are better educated to perform orthodontic treatment of higher quality, with greater efficiency, better diagnostic skills, and using the latest technology.
Dr. Peter Hgan
A small percentage of general dentists in West Virginia include orthodontic treatment as part of their service. This is in contrast to big cities such as Chicago, San Francisco, Los Angeles, and New York that most of the general dentists provide orthodontic treatment or multidisciplinary treatment service.
The reason why more and more general dentists are engaged in orthodontics is because the tools and technology such as straight wire appliance, clear aligners, and indirect bonding allow general dentists to practice orthodontic tooth movement with little or no training.
Most of the dental graduates in North America have little to no training in orthodontics and yet they can provide orthodontic service with minimal training by taking courses after graduation. Orthodontists have 3 years of additional training, so they should be engaged in treating more complicated cases.
Dr. Greg Huang
I don’t know if it is really a problem. General dentists are allowed to provide orthodontic treatment, and many elects to offer orthodontic care, especially in patients whose malocclusions are less severe. The advent of clear aligners has certainly made this easier for general dentists.
Dr. Glenn Sameshima
The percentage of orthodontic services done in America by general dentists and pediatric dentists continues to rise. The impact thus far has been restricted to certain metropolitan areas such as Southern California, but orthodontists are generally still busy. This may change in the next decade, and the profession here as in many other countries must confront the issue of reducing the number of residents.
Dr. Jae Park
General dentists can treat orthodontic patients, but to be an orthodontist, we typically spend 2–3 more years in orthodontic training. To protect the public and provide them with better orthodontic service, we feel that orthodontists are best equipped to treat patients.
Canada
There is a significant increase in general dentists providing orthodontic treatment to their patients, especially because of the development of the aligners. While general dentists can treat some orthodontic cases, they are ethically required to work within their competencies and experience and be honest about their abilities to deliver proper results. However, some general dentists go beyond their competencies, which may lead to compromised treatment. It is likely that with competitiveness in the dental marketplace and with the influence of digital aligner therapy, this trend of general dentists providing orthodontic treatment will only increase.
Recently, some of our orthodontic societies have carried out advertising campaigns to educate the public about the differences in training between orthodontists and general dentists and the advantages of being treated by a specialist.
Mexico
Just like in countries around the world, Mexico is no different; over 50% of the general dental practitioners do orthodontics or have someone come to their offices to do orthodontics for them.
Columbia
The Colombian Legislation and law do not prohibit the general practitioner (GP) to do orthodontic treatment; therefore, there is always confrontation between GPs and orthodontists.
Brazil
The fixed orthodontic appliance with brackets was developed by Angle seeking treatment effectiveness. Trying to increase the efficiency of treatment, the straight-wire and self-ligating brackets were developed. However, all of these advances were focused on the orthodontist, not on the patient.
The great advantage of aligners is that they are focused on the patient’s experience. The use of aligners has grown exponentially. In fact, there is an important demand from the population for the use of aligners. In addition to internationally known brands, many local Brazilian companies have begun to produce aligners, since 3D printing technology has become very accessible, as do intraoral scanners. In addition, some patents that protected components of some alignment companies fell, giving rise to the improvement of competing companies.
However, aligners have technical limitations. In my opinion, we need to go back to the drawing board to conceive something new in terms of design. The bracket is not an unchangeable icon. The aligners are a beginning, but they are still not the solution. We will probably need to throw away the orthodontic appliance design used today and possibly develop a hybrid device, with fixed and removable components. Whatever the future appliance is, it needs to be more esthetically appealing and less traumatic than fixed appliances, but still mechanically efficient.
DISCUSSION
It should be noted that the number of dental schools or orthodontic departments is zero in Macau and only one in Singapore, Hong Kong, New Zealand, and Sri Lanka.[1] The total number of members in APOS affiliate societies is approximately 18,000. Among these, the members in four big societies, Chinese Orthodontic Society, Indian Orthodontic Society, Japanese Orthodontic Society, and Korean Association of Orthodontist, are more than 80% of the total number.[1]
Meanwhile, in Europe, the size of orthodontic society and the number of orthodontic departments or dental schools are small when compared to those in USA and Asian countries such as China, India, Japan, and Korea. In fact, these numbers are greatest in USA, demonstrating a fact that orthodontist in USA is recognized as the most popular profession among all.
In most countries in Asian Pacific region, it takes 5–6 years to complete dental education for BDS or DDS.[1] It should be noted that dental school system for 8 years has recently been started in Korea. Thus, Korea has two kinds of educational systems to become a dentist. Some dental colleges have traditional system of 2-year pre-dental course plus 4-year dental course. Meanwhile, six dental colleges have changed their educational systems to 4+4 systems since 2005, which means 4 years of bachelor’s degree plus 4-year dental school program.[1] In Europe and South America, it also takes 5–6 years to complete undergraduate dental education for qualified dentists. Meanwhile, in Canada and USA, dental school system has been developed, requiring 8-year education to become dentist.
For orthodontic specialists, in general, it takes 3–6 years as either resident or Master or PhD student. It should be noted that, in Hong Kong, it takes at least 6 years after graduation from dental school to become an orthodontic specialist, which seems one of the most difficult post- graduate orthodontic programs in the world.[1] Such system of postgraduate orthodontic courses is almost the same in European and American countries with an exception of 4-year training in Switzerland. Meanwhile, official postgraduate orthodontic program is for 5 and 6 years in Japan and Hong Kong,[1] respectively.
Most societies have two important issues, such as orthodontic treatment and inappropriate use of aligners by GPs.[1] The most important strategy is to appeal the public that orthodontic treatment should be executed by orthodontic specialists because the treatment quality is quite different from that of GPs. These problems are similarly observed in European and American countries; however, the status seems less serious than in developing Asian countries. It is of a great interest to know such comments of Dr. Lindauer that orthodontists, rather than general dentists, will win whatever “battle” there is over the patients seeking orthodontic treatment and that orthodontists are better educated to perform orthodontic treatment of higher quality, with greater efficiency, better diagnostic skills, and using the latest technology. It is thus confirmed that we orthodontists have to perform a national awareness campaign to the public that orthodontic treatment should be carried out by orthodontic specialists, who are essentially different from GPs in terms of the training period, clinical skills, and quality of treatment outcomes.
In addition, the Orthodontic Society or Association in each country has to take action to educate the general public in terms of the appropriate use of aligners and the effectiveness.
CONCLUSION
It is shown that the educational system for dentists and orthodontists has well been developed in every country in the world, although the strength is somewhat different from country to country.
Acknowledgment
I would like to express a sincere appreciation to all the interviewees for their kindest help and cooperation extended to the publication of this article.
Declaration of patient consent
The author certifies that appropriate consent was obtained from all the interviewees.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Current status of orthodontic professionals in the Asian Pacific region. APOS Trends Orthod. 2016;6:111-30.
- [CrossRef] [Google Scholar]
- Dental Health Services in Canada. Facts and Figures 2010. Canadian Dental Association.
- [Google Scholar]
- The Erasmus programme for postgraduate education in orthodontics in Europe: An update of the guidelines. Eur J Orthod. 2014;36:340-9.
- [CrossRef] [PubMed] [Google Scholar]
- Distraction osteogenesis may promote periodontal bone regeneration. J Dent Res. 2005;84:757-61.
- [CrossRef] [PubMed] [Google Scholar]




