

Translate this page into:
Early Intervention in Skeletal Class II and dental Class II division I malocclusion
Address for correspondence: Dr. Zeeshan Iqbal Bhat, Consultant Orthodontist and Dentofacial Orthopedics. Dahim Hospital, Dammam, Saudi Arabia. E-mail: drzeeshanbhat@hotmail.com
This article was originally published by Wolters Kluwer and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Bhat ZI, Naik CR, Rahalkar JS. Early Intervention in Skeletal Class II and dental Class II division I malocclusion. APOS Trends Orthod 2013;3:121-7.
Abstract
A Class II malocclusion may occur as a result of mandibular deficiency, maxillary excess, or a combination of both. However, the most common finding is mandibular skeletal retrusion. The use of functional jaw orthopedics, at the right time during growth, can ultimately result in malocclusion patients achieving an excellent functional occlusion, a broad beautiful smile, a full face with a beautiful jaw line, and profile. Functional jaw orthopedic (FJO) appliances are designed to encourage adaptive skeletal growth by maintaining the mandible in a corrected forward position. The activator developed by Andresen is one of the most widely used for this purpose. A 12-year-old boy with skeletal Class II malocclusion and dental Class II div I malocclusion, a low mandibular plane angle was treated with growth modulation using an activator followed by molar distalization using fixed orthodontics for detailing of the occlusion. The major effects of the activator treatment in this case have been due to increase in condylar growth and also an increase in mandibular base length. Further, non-extraction fixed orthodontic treatment for proper interdigitation of the dentition also helped to maintain the stability of the satisfactory results achieved.
Keywords
Activator
class II malocclusion
functional jaw orthopedics
molar distalization

INTRODUCTION
No one would deny that good occlusion in the first dentition with the jaws in a class I relation and the face well-developed is a favorable precursor to the same desirable condition in the permanent dentition. It is also true that some temporary disharmonies of the early mixed dentition are self-correcting or correctable by simple means if properly timed. The class II and class III malocclusions, however, do not correct themselves and it is these cases that are of concern to parents and pediatricians. They question why, if other deformities are more easily corrected at an early age, the same should not hold true for the face. The early correction of occlusion is the greatest aid to the promotion of the health of the denture through development of normal masticatory and facial habits as well as the beauty of the face.
There is a lack of consensus regarding the degree of success of different treatment modalities applied during the early to late mixed dentition stages.[1-3] The concept of ‘‘early treatment’’ is controversial. Some define it as removable or fixed appliance intervention in the primary, early mixed (permanent first molars and incisors present), or mid-mixed (inter-transitional period, before the emergence of first premolars and permanent mandibular canines). Others define early treatment as late-mixed dentition stage treatment (before the emergence of second premolars and permanent maxillary canines).[4] Clinical research has focused on two prominent strategies for the timing of treatment for Class II malocclusion.[5,6] The first intervention is considered during the pre-adolescent years (ages 8-11 years)[7] and includes correction of the molar distocclusion, incisor alignment, improvement of the overjet/overbite relationships, and skeletal correction. This “Stage 1” treatment is usually followed by a more definitive intervention during adolescence (ages 12-15 years)[7,8] in order to finish and detail the occlusion. Despite controversies on the effectiveness of functional jaw orthopedics (FJO), it has been shown that in the short term, FJO produces different dentoskeletal results based on timing of treatment.[9-18] A significant supplementary elongation of the mandible can be achieved only when FJO is performed at pubertal or immediately post-pubertal periods of skeletal development.[10-14]
Recently, it has been suggested that FJO at the pubertal spurt followed by the use of fixed appliances is a feasible therapeutic option in patients with unfavorable Class II malocclusions.[18] As for the long-term outcomes of FJO, data available in the literature is much more scarce.[12,14,19-23] While Freeman et al.[22] and Malta et al.[23] have described a long-term statistically significant increase in mandibular length in patients treated with FJO over untreated Class II controls of about 3 to 3.5 mm. DeVincenzo[19] and Hansen and Pancherz[20] have reported a lack of significant changes for the mandible of treated Class II subjects in the long term. However, in both latter studies, the controls were not ideal, with DeVincenzo[19] using a mixed group of Class II and Class I subjects (some of whom had been treated before or were still in treatment), while Hansen and Pancherz[20] used values derived from the ‘‘Bolton Standards,’’ a group of subjects highly selected on the basis of ideal occlusions and well-balanced faces.[24] Few studies[12,14] have described the long-term effects of FJO at different stages of dentoskeletal development.
Here, we are presenting a case of a Class II skeletal malocclusion treated by using an activator appliance. In spite of its simple design, an activator can be used to change dental relationship in all three planes of space with proper adjustments.[25]
DIAGNOSIS AND ETIOLOGY
A boy, aged 12 years, came with his father with a chief complaint of being continuously bullied in school because of his facial appearance due to proclined maxillary anterior teeth and an increased overjet. He was diagnosed with a skeletal Class II and dental Class II Division 1 malocclusion with a retrognathic mandible, horizontal growth pattern, proclination of maxillary incisors, deep overbite, spacing in upper and lower anterior teeth, midline diastema, and peg-shaped lower left central incisor. Psychologically he possessed a low self esteem.
His medical history was not contributory. The pretreatment facial photographs showed a mesoprosopic face, a convex soft-tissue profile, acute nasolabial angle, potentially competent lips, deep mentolabial sulcus, lower lip trap and everted upper lip caused by a retrognathic mandible. Upon smiling, 7 mm (90%) of occluso gingival length of the maxillary central incisors was visible [Figure 1]. The pretreatment intraoral photographs and dental casts showed that the patient was in the mixed dentition. The UR1, UR2, UR6, UL1, UL2, UL4, UL5, UL6, LR4, LR5, LR6, LL6, deciduous canines, first and second upper right deciduous premolars were erupted in the oral cavity. Lower right and left root pieces of deciduous first molar were present. He had maxillary and mandibular dental midlines shifted towards the left side with his facial midline. The overbite was deep at 100%, with the mandibular incisors touching the palatal mucosa. Overjet was 12 mm. The molar relationship was end-on (Class II) on both the sides [Figure 2]. The pretreatment lateral cephalogram and orthopantomogram [Figure 3] showed that all canines and unerupted premolars are in erupting phase. The cephalometric analysis showed he was in between 2-3 stage of Cervical vertebrae maturation indicator (CVMI), a skeletal Class II relationship (ANB angle-50, Ao-Bo 5 mm) with a flat mandibular plane angle (SN-GoGn angle 270, FMA 200), a retrognathic mandible (SNB angle 740, SAr.Go angle 1350), proclined maxillary incisors (U1-NA, 12 mm and 420), and retroclined mandibular incisors (L1-NB, 3 mm and 170).

- Pre-treatment extra-oral photographs

- Pre-treatment intraoral photographs

- Pre-treatment OPG and lateral cephalogram
VTO was positive. It was felt that cooperation would be good in this case, as the patient and family were concerned about the lack of facial harmony and anxious for this to be improved. This case almost fully met the recommended case selection criteria.
TREATMENT OBJECTIVES
The treatment objectives for this patient were as follows: (1) Sagittal advancement of the mandible to acheive Class I skeletal relation, (2) Correct the deep overbite and the increased overjet, (3) Close the spaces in the maxillary arch, (4) Correct the malalignment of the mandibular and maxillary anterior teeth, (5) Maintain the space for canine to erupt and later bring them into alignment, (6) Improve the facial balance.
TREATMENT PLAN
Phase I: A removable functional appliance Activator was constructed using a wax bite with 6 mm of sagittal advancement and 4 mm of vertical opening, to encourage an increase in lower facial height. The labial bow was passive and positioned half way up the labial surface of the maxillary incisors. Incisal capping was made on lower incisors. The initial treatment plan was for a second Andresen appliance to be used, but this was not required, as it proved possible to reduce the overjet fully using the original one [Figure 4].

- Activator with lower incisal capping and labial bow
Phase II: Full size metal maxillary and mandibular fixed appliance to correct incisor protrusion, spacing, and bring the canines into alignment.
Long-term retention with canine to canine lingual- bonded retainers on both arches. Hawley’s retainer during the day time. Night time to wear activator with 2 mm of vertical and 0 mm of sagittal advancement.
TREATMENT PROGRESS
After 5 months of good compliance with the activator, extraction of upper left deciduous molars was done and trimming of activator for eruption of upper left premolars and lower right second premolars was done. The overjet was reduced from 12 mm to 5 mm using only the one Andresen appliance for 11 months [Figure 5]. The molars and premolars were in Class I relationship with the upper incisors under lip control [Figures 6], and the patient was reminded of the need to maintain a lip seal. The activator successfully resolved the problem of the retrognathic mandible with favourable mandibular growth.

- Post-functional intraoral photographs

- Post-functional extra-oral photographs
After achieving the functional correction of skeletal discrepancy, Full-size metal maxillary and mandibular arches were bonded excluding the lower left canine with a 0.018-inch Roth preadjusted appliance (American orthodontics) at age 12 years 11 months. The opening archwires were 0.014-in NiTI, 0.016-in NiTi, 16 × 22 NiTi with light Class II elastics of 75 Gm, worn 12 hours a day. Two months later, the lower left canine was bonded and included into the arch wire. The wires were changed every 4-5 weeks. Four months after the fixed appliance therapy; 16 × 22 SS with open coil spring between UR2-UR4 and UL2-UL4 were placed to maintain the space for canines to erupt.
Later it was observed that space for canine eruption and incisor retraction was not sufficient. Distalization of molars was decided as the choice of treatment. After 6 months from the start of the phase II, 0.016 SS A.J. Wilcock with reverse curve of spee in lower arch and 0.016 SS A.J. Wilcock with mesial stops on molar, helix distal to UR2, UL2, and buccal flaring of wire to distalize the molars in upper arch was made. Molar stops were made in such a way that the wire should stay 2 mm away from the incisors. Premolars were kept disengaged. At this stage, light Class II elastics were being worn throughout the day and night to helix made into the upper archwire [Figure 7]. Elastics were changed every 24 hours. Two months later, activation was done by compressing the helix on both the sides. Three months after the start of distalization, molars were in super class I. 0.014 NiTi was placed over 0.016 A.J. Wilcock for one month engaging premolars and upper canines. After alignment of premolars and canines, retraction and intrusion utility arch was given in upper arch for a period of 3 months. Finally, 16 × 22 SS upper and lower arch wire was placed for 2 months before debonding.

- Molar distalization
At the end of treatment at age 14 years 2 months, the patient had a much improved facial harmony [Figures 8 and 9, his bullying was stopped and self- esteem was high which had been the primary reason for seeking treatment. The total treatment time was 26 months.

- Post-fixed appliance therapy (extraoral)

- Post-fixed appliance therapy (intraoral)
Canine to-canine lingual bonded retainers were placed in both arches along with day time wear Hawley’s retainer with inclined plane and night time wear activator with 2 mm of vertical and 0 mm of sagittal advancement to maintain the achieved sagittal correction. Cephalometrically, the measurements were close to ideal. Overall superimpositions showed favorable growth of the mandible and improvement of overjet [Figure 10].
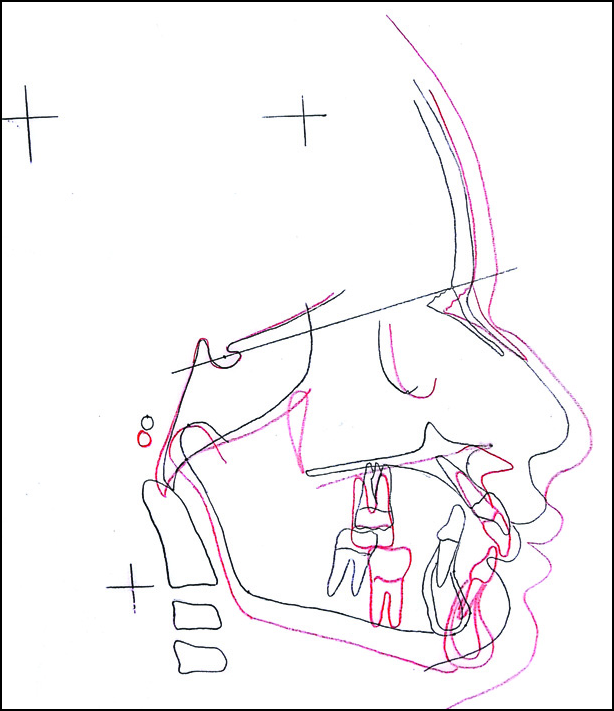
- Superimposition, Pretreatment black and Post treatment red
After 1 year in retention, the occlusion was well maintained [Figures 11 and 12].

- 1 year in retention (extraoral)

- 1 year in retention (intraoral)
TREATMENT RESULTS
At the end of the treatment, The cephalometric analysis showed a significant change in skeletal Class II to Class I relationship [Table 1] (ANB angle 50 - 20, Ao-Bo 5 mm-1 mm), a significant increase in the inclination of the mandibular plane to the Frankfort plane, a significant opening of the gonial angle (Ar-Go-Me) and a significant repositioning of articular angle (S-Ar-Go).
| Pre- treatment | Post- functional | Post- treatment | |
|---|---|---|---|
| Pt A to Nasion Perp | -1 | -1.5 | -6 |
| SNA | 79 | 79 | 79 |
| SNB | 74 | 78 | 77 |
| ANB | 5 | 1 | 2 |
| AO-BO | 5 mm | 2 mm | 1 mm |
| CO-A | 75 mm | 82 mm | 82 mm |
| CO-GN | 92 mm | 103 mm | 103 mm |
| SN-GoGn | 27 | 27 | 26 |
| Occ-SN | 16 | 16 | 16 |
| CO-GO | 47 mm | 49 mm | 53 mm |
| GO-GN | 59 mm | 67 mm | 67 mm |
| N S.Ar | 128 | 127 | 132 |
| S Ar.Go | 135 | 140 | 140 |
| Ar.Go.Me | 128 | 130 | 130 |
| FMA | 20 | 23 | 26 |
| Y-axis | 57 | 55 | 55 |
| U1-SN | 120 | 108 | 102 |
| U1-NA | 12 mm, 40 | 7 mm, 28 | 5 mm, 26 |
| U1-A-Pg | 12 mm, 42 | 10 mm, 34 | 5 mm, 25 |
| L1-NB | 3 mm, 17 | 6 mm, 30 | 5 mm, 31 |
| IMPA | 93 | 105 | 103 |
| L1-APog | 0 mm | 2 mm | 3 mm |
| Ul-L1 | 125 | 116 | 122 |
| SnG Pg | 25 | 21 | 20 |
| Nasolabial angle | 91 | 106 | 102 |
| Lip strain | 3 mm | 1 mm | 0 mm |
| S line-LL1 | -2 mm | 0 mm | 0 mm |
| PFH/AFH | 63/93 | 68/104 | 68/105 |
As for the occlusal changes, a well-aligned dentition with Class I molar and canine relationship was achieved. The patient had a consonant smile arc, the teeth had good interdigitation, and both overjet and overbite were significantly reduced (2 mm and 2.5 mm, respectively), the proclination of the maxillary incisors was decreased (400 to 260), there was no significant reduction in the inter-incisal angulation (1220) due to a significant increase in the projection of the lower incisors (L1 to APg- 3 mm). The molar relation improved significantly. The maxillary and mandibular midlines were coincident with the facial midline. The post-treatment panoramic radiograph showed no apparent root resorption of the teeth [Figure 13].

- Post-fixed appliance therapy (OPG, Lateral cephalogram)
DISCUSSION
Teeth have been reported as the fourth most common feature to provoke unfavourable social responses, including bullying. Increased overjet is linked with teasing[26] and reduced self-concept. Some improvement in self-concept has been demonstrated in subjects undergoing early overjet reduction.[27] An increased overjet can have negative psychosocial implications and is also associated with an increased risk of trauma to the upper labial segment, particularly in children, both of which are indications for treatment.[28]
The main aim of the functional phase is to achieve skeletal correction, reduce the overjet and overbite, and also to achieve a near-normal incisor relationship. Correction of the overjet allows a lip seal to establish, so that normal function and development can resume. Function determines how the skeletal development will be, and: “If you can change the function, you can change the development.”[29]
It is necessary to select a functional appliance that will achieve these goals and that is easy for the patient to wear. Noro et al.,[30] suggested that Patients generally find appliances easier to wear with a modest construction bite of 2-4 mm at the incisors. This produces 80-100 Grams of force and clinicians may feel this is adequate for successful treatment. Ruf et al.,[31] concluded that effective condylar growth and the chin position can be affected by activator treatment. Antonarakis GS[32] concluded, Anteroposterior treatment response following the use of activator in growing class II malocclusion patients is most evident in the mandible.
Functional appliances are thus effective in treating skeletal Class II malocclusion. Particularly in cases with retrognathic mandible, functional appliances are of greatest clinical benefit in actively growing patients with good compliance. In our patient, response to the activator was overwhelming and so was his cooperation. The muscular force generated by the forward mandibular positioning was transferred to the maxillary and the mandibular teeth through the acrylic body and labial bow. These forces which were transmitted through the teeth to the periosteum and bone were responsible in producing a restraining effect on the forward growth of maxilla, while stimulating the mandibular growth and causing maxilla-mandibular dentoalveolar adaptation. The major effects of the activator treatment in this case has been due to an increase in condylar growth and in mandibular base length. The combination of these effects resulted in the permanent anterior displacement of the mandible. The activator also had an influence on the dentition. By inhibiting the maxillary dentoalveolar vertical growth and encouraging the mandibular dentoalveolar mesial and vertical development, the activator resolved the Class II malocclusion to Class I malocclusion. The possible mechanisms for the activator in correcting a Class II malocclusion in this patient include Stimulation of the mandibular growth,[31] Redirection of the anterior and Vertical dentoalveolar growth of maxilla and mandible,[33] and remodelling changes in TMJ.[34]
Upper incisors became retroclined and lower incisors proclined during overjet correction with a functional appliance. Soon after the start of leveling and aligning, it is therefore helpful to ask the patient to wear very light Class II elastics of 75 Gm during the evenings and when sleeping. These support anchorage, and help to prevent an increase in overjet as the crown tip is corrected. During leveling and aligning Class II elastics can be carried to Kobayashi hooks. As the case moves into rectangular wires, it is therefore normally necessary to ask the patient to continue wearing light Class II elastics, of 100 Gm or less, during the evenings and when sleeping. Full-time elastic wear is not normally needed at first, but may be indicated later if there is a tendency for the overjet to reappear. Predictably, there is often a need for more anchorage support from Class II elastics in cases with an underlying Class II skeletal pattern, or for cases which had a large starting overjet.
For the case under study, 0.016 A.J. Wilcock with reverse curve of spee was placed in both the arches. In the maxillary arch, molar stops were given mesial to both the molars in such a way that wire would stay 2 mm away from incisors and buccal flaring was given in the buccal segment, it was thought that the cheek would exert pressure on the flared wire that would in turn exert pressure on the stops on molars and this would distalize the molars, but that would have a counter effect on insiors, it would procline them. To counter act this effect a Helix was made in the wire distal to lateral incisors on which light class II elastics were given. This would not only help in maintaining overjet but also helps in maintaining the class I skeletal correction achieved during phase I. Case was later finished with 16 × 22 ss wire for two months in both the arches to express sufficient torque.
Long-term retention with Canine to canine lingual- bonded retainers were placed on both arches to prevent spaces from opening up. Hawley’s retainer with labial bows canine to canine were given during the day time, at night time he was asked to wear activator with 2 mm of vertical and 0 mm of sagittal advancement. This was to maintain the class II correction.
CONCLUSION
Treatment of Class II malocclusion with functional appliances followed by fixed appliances produced a significant long-term elongation of the mandible over the controls associated with improvements in the skeletal sagittal intermaxillary relationship, the overjet, and sagittal molar relationship. A significant reduction of the overbite is associated with an increase in lower anterior facial height and mandibular ramus height.
Source of Support:
Nil.
Conflict of Interest:
None declared.
References
- Class II treatment: A comparison of one and two stage non-extraction alternatives In: McNamara JA Jr, ed. Orthodontic treatment outcome and effectiveness (2nd ed). Ann Arbor, Mich: Center for Growth and Development, University of Michigan; 1995. p. :163-93.
- [Google Scholar]
- Timing of Class II treatment: Rationale, methods and early results of an ongoing randomized clinical trial In: McNamara JA Jr, ed. Orthodontic Treatment: Outcome and Effectiveness. Ann Arbor, Mich: Center for Growth and Development, University of Michigan; 1995. p. :81-112.
- [Google Scholar]
- Early versus late treatment of Class II malocclusion: Preliminary results from the University of North Carolina clinical trial In: McNamara JA Jr, ed. Orthodontic Treatment: Outcome and Effectiveness. Ann Arbor, Mich: Center for Growth and Development, University of Michigan; 1995. p. :113-38.
- [Google Scholar]
- Headgear versus function regulator in the early treatment of Class II, division 1 malocclusion: A randomized clinical trial. Am J Orthod Dentofacial Orthop. 1998;113:51-61.
- [Google Scholar]
- Treatment objectives in the deciduous dentition. Am J Orthod Dentofacial Orthop. 1969;55:617-32.
- [Google Scholar]
- The early treatment of Angle’s Class II, division 1 malocclusion. Dent Pract Dent Rec. 1968;19:137-44.
- [Google Scholar]
- Comprehensive mixed dentition treatment. Am J Orthod Dentofacial Orthop. 1998;113:75-84.
- [Google Scholar]
- Skeletal and dental changes following functional regulator therapy on Class II patients. Am J Orthod Dentofacial Orthop. 1985;88:91-110.
- [Google Scholar]
- Dentofacial orthopaedics in relation to chronological age, growth period and skeletal development: An analysis of 72 male patients with Class II, division 1 malocclusion treated with the Herbst appliance. Eur J Orthod. 1988;10:169-76.
- [Google Scholar]
- Mechanism of craniofacial growth and modus operandi of functional appliances: A cell-level and cybernetic approach to orthodontic decision making In: Carlson DS, ed. Craniofacial Growth Theory and Orthodontic Treatment. Ann Arbor, Mich: Center for Human Growth and Development, The University of Michigan; 1990.
- [Google Scholar]
- Long-term effects of the Herbst appliance in relation to the treatment growth period: A cephalometric study. Eur J Orthod. 1991;13:471-81.
- [Google Scholar]
- Treatment timing for twin block therapy. Am J Orthod Dentofacial Orthop. 2000;118:159-70.
- [Google Scholar]
- Long-term effectiveness and treatment timing for Bionator therapy. Angle Orthod. 2003;73:221-30.
- [Google Scholar]
- The effect of early intervention on skeletal pattern in Class II malocclusion: A randomized clinical trial. Am J Orthod Dentofacial Orthop. 1997;111:391-400.
- [Google Scholar]
- Effectiveness of early orthodontic treatment with the Twin-block appliance: A multicenter, randomized, controlled trial. Part 1: Dental and skeletal effects. Am J Orthod Dentofacial Orthop. 2003;124:234-43.
- [Google Scholar]
- Effectiveness of orthodontic treatment with functional appliances on mandibular growth in the short-term. Am J Orthod Dentofacial Orthop. 2011;139:24-36.
- [Google Scholar]
- The impact of functional jaw orthopedics in subjects with unfavorable Class II skeletal patterns. Prog Orthod. 2010;11:118-26.
- [Google Scholar]
- Changes in mandibular length before, during, and after successful orthopedic correction of Class II malocclusions, using a functional appliance. Am J Orthod Dentofacial Orthop. 1991;99:241-57.
- [Google Scholar]
- Long-term effects of Herbst treatment in relation to normal growth development: A cephalometric study. Eur J Orthod. 1992;14:285-95.
- [Google Scholar]
- Long-term treatment effects of the FR-2 appliance of Frankel. Am J Orthod Dentofacial Orthop. 2009;135:570.e1-6.
- [Google Scholar]
- Long-term dentoskeletal effects and facial profile changes induced by Bionator therapy. Angle Orthod. 2010;80:10-7.
- [Google Scholar]
- Bolton Standards of Dentofacial Developmental Growth. St Louis, Mo: CV Mosby; 1975.
- Predicting functional appliance treatment outcome in class II malocclusions-review. Am J Orthod Dentofacial Orthop. 1998;112:282-6.
- [Google Scholar]
- Nicknames, teasing, harassment and the salience of dental features among school children. Br J Orthod. 1980;7:75-80.
- [Google Scholar]
- Effectiveness of treatment for Class II malocclusion with the Herbst or twin-block appliances: A randomized, controlled trial. Am J Orthod Dentofacial Orthop. 2003;124:128-37.
- [Google Scholar]
- A systematic review of the relationship between overjet size and traumatic dental injuries. Eur J Orthod. 1999;21:503-515.
- [Google Scholar]
- Funktions- Kieferorthopadie. Die Grundlagen des ‘norwegischen Systems.’ Leipzig: H. Meusser; 1936.
- Orthodontic forces exerted by activators with varying construction heights. Am J Orthod Dentofacial Orthop. 1994;105:169-79.
- [Google Scholar]
- Effective condylar growth and chin position changes in activator treatment: A cephalometric roentgenographic study. Angle Orthod. 2001;71:4-11.
- [Google Scholar]
- Short-term anteroposterior treatment effects of functional appliances and extraoral traction on class II malocclusion. A meta-analysis. Angle Orthod. 2008;77:907-14.
- [Google Scholar]
- Class II: A comparison of activator and activator headgear combination appliances. Eur J Orthod. 1994;16:149-57.
- [Google Scholar]
- Changes in the TMJ disc-condyle-fossa relationship following functional treatment of skeletal Class II division I malocclusion: A Magnetic Resonance Imaging study. Am J Orthod Dentofacial Orthop. 2001;119:316-9.
- [Google Scholar]




